
Abstract
Upper eyelid blepharoplasty in the Asian patient incorporates the basic techniques and principles of standard blepharoplasty surgery, although it is important to understand the anatomic differences in the Asian lids, as well as the cultural significances that may play a part in achieving optimal results. Even among the various Asian ethnicities, there are subtle anatomic differences and diverse cultural concepts of beauty that should not be overlooked. Eyelid surgery for visually obstructing dermatochalasis has become more popular over recent years in the Asian population, and cosmetic blepharoplasty surgery is also gaining momentum for cosmetic creation of “double eyelids.”
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Upper lid blepharoplasty
- Asian patient
- Standard blepharoplasty surgery
- Anatomic differences
- Asian lids
- Cultural concepts of beauty
- Eyelid surgery
- Dermatochalasis
- Double eyelids
Upper eyelid blepharoplasty in the Asian patient incorporates the basic techniques and principles of standard blepharoplasty surgery, although it is important to understand the anatomic differences in the Asian lids, as well as the cultural significances that may play a part in achieving optimal results. Even among the various Asian ethnicities, there are subtle anatomic differences and diverse cultural concepts of beauty that should not be overlooked. Eyelid surgery for visually obstructing dermatochalasis has become more popular over recent years in the Asian population, and cosmetic blepharoplasty surgery is also gaining momentum for cosmetic creation of “double eyelids.” As mentioned previously, the preoperative evaluation should include a thorough discussion with the patient regarding their ideal outcome from surgery, using photos for illustration, as well as demonstrating the result to the patient with a mirror. Using a cotton tip applicator or other small instrument to simulate the eyelid crease height and contour of the skinfold during the evaluation can be very helpful for the patient to visualize the expected outcome. Careful planning with the patient should include discussion of the eyelid crease placement and shape, the desired type of lid fold or absence of fold, and epicanthal fold considerations.
Preoperative office examination should document in detail the following:
-
1.
Presence of eyelid crease, contour, and height on both sides
-
2.
Eyelid skinfold
-
3.
Brow position
-
4.
Measurement of eyelid skin from lid margin to the thicker brow skin
-
5.
Fullness of the upper lid fat
-
6.
Pretarsal fullness (subcutaneous fat) – not normally seen in Caucasian eyelids
-
7.
Epicanthal fold and shape
-
8.
Eyelash ptosis and trichiasis
-
9.
Asymmetries
With the above findings in mind, some important pearls for upper eyelid blepharoplasty in the Asian patient are as follows:
-
1.
Determine the desired height and shape for the lid crease preoperatively – does the patient wish to create a lid crease or prefer to maintain the single-lid appearance?
-
2.
Skin marking:
-
(a)
Keep the height of the eyelid crease low, approximately 4–6 mm above the lid margin (Fig. 39.1).
Fig. 39.1 
External photo displaying the suggested lid crease height for the Asian upper lid
-
(b)
Blend the eyelid crease into the epicanthal fold:
-
(i)
With the patient supine, gently push up on the lid margin to see where the epicanthal fold is most prominent, and place the markings directly on the edge of the skinfold. Ask the patient to open the eyes to confirm that the medial apex of the blepharoplasty marking blends into the epicanthal fold without creating a second fold or crease.
-
(i)
-
(c)
Avoid creating a semilunar skin incision, which is more characteristic of the Caucasian eyelid. The crease contour should be relatively flat or mildly rounded.
-
(d)
Make the lateral extent of the lid crease parallel or slightly higher than central portion (Fig. 39.2).
Fig. 39.2 
Schematic illustration of the intraoperative marking for the Asian upper lid, noting the higher lateral extent of lid crease
-
(e)
Generally 15–18 mm of skin (rather than the average 19–20 mm in Caucasian eyelids) from the lid margin to brow skin should be preserved, due to smaller orbital spaces. The pinch technique should confirm that there is no tightness of the skin or eyelid margin eversion that would result in lagophthalmos. Inferior brow margins are sometimes fuller and indistinct and sit slightly lower in the Asian population.
-
(a)
-
3.
Incision and excision:
-
(a)
Remove the skin or skin-orbicularis muscle flap.
-
(b)
If upper blepharoplasty is performed in a young patient primarily for creation of an eyelid crease, the excised flap should not exceed 3 mm in height (Fig. 39.3).
Fig. 39.3 
External photo of preoperative (a) and postoperative (b) low lid crease of an Asian patient
-
(c)
Avoid aggressive excision of preaponeurotic and medial fat pads, as a hollow upper lid sulcus would be uncharacteristic of the naturally fuller Asian eyelid appearance.
-
(d)
Further excise a 2–3 mm strip of pretarsal orbicularis muscle and subcutaneous tissue along the length of the inferior skin incision to facilitate lid crease formation (Fig. 39.4).
Fig. 39.4 
Schematic illustration demonstrating excision of pretarsal orbicularis muscle and subcutaneous fat tissue from the inferior crease edge to facilitate lid crease formation (shaded orange area)
-
(a)
-
4.
Eyelid crease formation
-
(a)
Pass a 6.0 Vicryl suture through the inferior edge subcutaneous tissue, then gently lift the lid skin up to its normal height without causing eyelash eversion or tightness of the skin. Pass the suture into corresponding levator aponeurosis or tarsus directly behind the edge of the lifted lid skin, and then pass the suture through the superior edge orbicularis muscle. Multiple interrupted sutures should be placed along the entire incision as these posterior tacking bites to the underlying tarsus or aponeurosis secure the placement of the eyelid crease (Fig. 39.5). Slightly superior placement of the deeper pass into tarsus can also help evert the lashes to minimize eyelash ptosis, which is often seen in Asian eyelids. The sutures can also be placed in buried fashion to minimize palpable knots.
Fig. 39.5 
Cross-sectional diagram of eyelid crease formation using posterior tacking sutures to the underlying levator aponeurosis or tarsus
-
(a)
-
5.
Closure
-
(a)
Close the skin with running or interrupted 6–0 fast gut suture or nonabsorbable suture. Sutures should be removed by 10 days if present to avoid post-inflammatory hyperpigmentation in this population (Fig. 39.6).
Fig. 39.6 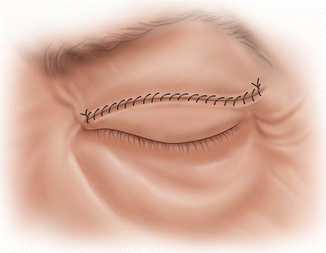
Schematic illustration of upper eyelid skin closure with running suture after lid crease formation
-
(a)






Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Burkat, C.N., Jaru-Ampornpan, P. (2015). Upper Lid Blepharoplasty in the Asian Patient. In: Hartstein, MD, FACS, M., Massry, MD, FACS, G., Holds, MD, FACS, J. (eds) Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1544-6_39
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1544-6_39
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1543-9
Online ISBN: 978-1-4939-1544-6
eBook Packages: MedicineMedicine (R0)