
Abstract
Placement of the skin incision is crucial to the perceived success of blepharoplasty surgery as the eyelid crease is the most distinguishing feature of the upper lid. The heights of the creases are compared on both sides. If they are symmetric and appropriate for gender (approximately 8–11 mm for women, 6–8 mm for men), the creases are delineated with a fine-tip skin marking pen. Occasionally, the crease heights are asymmetric, contain double lines, or are discontinuous. In these cases, careful comparison between the two sides will help guide the proper placement.
Gender and ethnic considerations should be incorporated into placement of the skin marking, with the crease incision rounder and more arched in women, as opposed to a flatter and lower crease incision in men. In Asian eyelids, the medial end of the blepharoplasty markings should blend precisely into the epicanthal fold. The height of the eyelid crease in Asians will also be lower and flatter at 4–6 mm in order to avoid a westernized appearance.
The upper eyelid skin should measure 18–20 mm from eyelid margin to the transition to eyebrow skin to eliminate the risk of postoperative lagophthalmos from aggressive tissue excision. The height of the eyelid crease is first subtracted from the total 18–20 mm. This amount is then measured from the inferior edge of brow skin, which will thus represent the superior border of the skin flap to be excised. Laterally, an extra several millimeters may be removed as there is usually some degree of lateral eyebrow ptosis, although a browpexy should be performed if significant brow ptosis exists. The pinch technique confirms that adequate skin is preserved. The inner aspect of the skin marking also should not extend further medially than the upper punctum in order to avoid webbing postoperatively.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Blepharoplasty
- Incision
- Eyelid/lid crease height
- Asian eyelid
- Epicanthal fold
- Pinch technique
- Eyelid/lid crease shape/contour
- Burow’s triangle
- Scarring
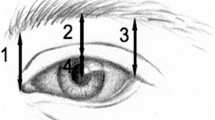
During blepharoplasty surgery, marking the skin is probably one of the most important steps and therefore warrants careful attention to detail. The placement of the skin incision is crucial to the perceived success of the surgery postoperatively as the eyelid crease is the most distinguishing feature of the upper lid. Preferably, the incisions should be marked prior to injection of local anesthetic, in order to avoid tissue distortion from anesthetic infiltration. The height of the eyelid creases are first measured and compared on both upper eyelids. If they are symmetric and appropriate for gender (approximately 8–11 mm for women, 6–8 mm for men), the creases are gently delineated with a fine-tip skin marking pen (Fig. 24.1). Occasionally, the crease heights are asymmetric, contain double lines, or are discontinuous. In these cases, careful comparison between the two sides will help guide the proper placement. If the surgical incision is placed lower on the side with the higher crease (to match the height of the contralateral side), the previous asymmetric crease will therefore be excised in the blepharoplasty flap, and the resultant creases will be symmetric without risk of multiple lines.

Measuring and marking the eyelid crease incision from the eyelid margin
If involutional ptosis is also present, the eyelid crease may be anatomically elevated up to 15–20 mm from the eyelid margin, due to dehiscence of the anterior fibers of the levator aponeurosis that attach to the dermis and skin at the level of the lid crease. Placement of the incision at these elevated crease levels would result in a suboptimal and unnatural appearance to the eyelids.
Gender and ethnic considerations should be incorporated into placement of the skin marking, with the crease incision rounder and more arched in women, as opposed to a flatter and lower crease incision in men. In eyelids of patients with Asian descent, the medial ends of the blepharoplasty markings should blend precisely into the epicanthal fold. Pushing the eyelid margin gently upward with a finger, or asking the patient to open his or her eyes, can confirm that the skin marking tapers into the medial fold. In addition, the height of the eyelid crease in Asians will be much lower at 4–6 mm, with a flat or softly rounded contour. Placing the incision at the normal 8–11-mm height, or creating a semilunar shape, would result in a westernized Caucasian eyelid that would be undesirable to the Asian patient.
In general, the upper eyelid skin should measure 18–20 mm from eyelid margin to the transition to eyebrow skin. This measurement eliminates the risk of postoperative lagophthalmos from aggressive tissue excision (Fig. 24.2). In addition, it is a useful guideline for teaching residents in training. The height of the eyelid crease is first subtracted from a total of 18–20 mm (Fig. 24.3). This amount is then measured from the inferior edge of brow skin, which will thus represent the superior border of the skin flap to be removed (Fig. 24.3). This is measured at the central lid first and then medially. Avoid excising too much skin medially, which may cause medial lagophthalmos or webbing (Fig. 24.4). Laterally, an extra 2–3 mm may be removed as there is usually some degree of lateral eyebrow ptosis, although a lateral browpexy should be performed if significant brow ptosis exists. Additional skin excision can always be judiciously performed if there still appears to be excess tissue, particularly in those with a smaller orbital space. Care should be taken to avoid confusing the true junction of the inferior brow (where the thin eyelid skin transitions to thicker, larger porous brow skin with a different color) in women who pluck their eyebrows to a higher height (Fig. 24.5). Measuring the upper incision to the plucked eyebrow level would result in erroneous excess skin removal.

Postoperative lagophthalmos following aggressive skin incision

(a, b ) Marking the superior incision from the thick eyebrow skin

Webbing of skin medially due to extension of incision past the superior punctum

Arrows demarcate the transition from thin eyelid skin to thick eyebrow skin, which may be considerably below the level of plucked eyebrows
The pinch technique is then performed to confirm that an adequate amount of skin is preserved, done by pinching together the skin between the inferior and superior markings and measuring the remaining skin from the eyelid margin to the brow skin. If the skin pinch results in tightness to the thin eyelid skin, vertical striae to the skin, or retraction or eversion of the eyelid margin, too much skin is being excised (Fig. 24.6).

The pinch technique confirms that 20 mm of skin has been retained
The inner aspect of the skin marking also should not extend further medially than the upper punctum. Incisions that extend medial to the punctum increase the risk of webbing in the nasal eyelid region (Fig. 24.4). In the event that there still remains an excess of skin medially, a Burow’s triangle directed superomedially is helpful while still avoiding webbing.
The lateral extent of the skin marking should also be measured from the lateral canthal angle with a caliper. This ensures that the incisions extend for the same length bilaterally, which is often noticeable to the patient. In addition, the lateral extent should not extend into the horizontal lateral raphe or the thicker temporal skin, as this may also result in unsightly scars.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Burkat, C.N. (2015). Skin Marking in Upper Blepharoplasty: Avoiding Pitfalls. In: Hartstein, MD, FACS, M., Massry, MD, FACS, G., Holds, MD, FACS, J. (eds) Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1544-6_24
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1544-6_24
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1543-9
Online ISBN: 978-1-4939-1544-6
eBook Packages: MedicineMedicine (R0)