
Abstract
When marking the upper lids, the inferior incision is placed in the location of the desired postoperative eyelid crease. Many patients have a well-defined, ideally positioned preoperative crease that can be used. Otherwise, the surgeon must determine the location for the desired crease. This location should be individualized, realizing that excessive high or low creases may have an abnormal appearance and can occasionally adversely affect eyelid function.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Prep and Drape: Perform a full-face prep. Ensure the drape does not place traction on the lids or brows.
Marking Incision: The inferior incision is placed in the location of the desired postoperative eyelid crease. Many patients have a well-defined, ideally positioned preoperative crease that can be used. Otherwise, the surgeon must determine the location for the desired crease. This location should be individualized, realizing that excessive high or low creases may have an abnormal appearance and can occasionally adversely affect eyelid function. A higher crease usually results in more visible pretarsal skin. General guidelines are (see Table 19.1)
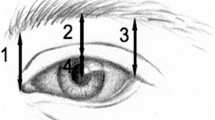
This distance from the superior border of the lashes to the crease in the central lid is usually 9–10 mm in females and 8–9 mm males (Fig. 19.1).

Skin markings for upper blepharoplasty incisions. The lower incision can be aligned with the natural crease if desired
To minimize web formation, the medial and lateral extensions of the lower incision angle upward, starting before the lacrimal punctum medially and near the canthal angle laterally. With the patient gently closing his or her eyes, forceps are used to measure the amount of redundant skin across the lid, ensuring sufficient tissue is left in place to allow full eyelid closure. More conservative skin excision is indicated in patients with dry eyes or at risk for lagophthalmos. The two sides are examined for symmetry. Asymmetric skin excision may be needed in patients with uneven skin redundancy or orbital asymmetry.


Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Custer, P.L. (2015). Orbit Size and Lid Marking in Upper Blepharoplasty. In: Hartstein, MD, FACS, M., Massry, MD, FACS, G., Holds, MD, FACS, J. (eds) Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1544-6_19
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1544-6_19
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1543-9
Online ISBN: 978-1-4939-1544-6
eBook Packages: MedicineMedicine (R0)