
Abstract
The direct browlift is often reviled as a cosmetically unacceptable or inappropriate procedure. Nonetheless, this procedure may be employed alone or as an adjunct to blepharoplasty surgery with excellent functional and cosmetic results. The direct browlift provides the most predictable and effective (on a millimeter-for-millimeter basis) lift available.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Described by Passot in 1919, the direct browlift is often reviled as a cosmetically unacceptable or inappropriate procedure. Nonetheless, this procedure may be employed alone or as an adjunct to blepharoplasty surgery with excellent functional and cosmetic results. The direct browlift provides the most predictable and effective (on a millimeter-for-millimeter basis) lift available.
The direct browlift employs a suprabrow incision, which may extend variably across the brow. When extended medially over the head of the brow, the incision is more visible, with questionable value as a cosmetic procedure.
Over the years, I have shortened the incision and avoid the head of the brow. With age, the tail of the brow tends to become more ptotic, lending an antimongoloid slant to the brow. Often, the medial brow has little of no involutional descent. The absence of the frontalis muscle as an elevating structure in the temporal brow and deflational descent due to soft tissue thinning in the temporal fossa area contribute to this change.
If a direct browlift incision is limited to 3 cm or less in overall length and the incision is beveled medially paralleling the brow cilia, it will heal almost imperceptibly. It is important to utilize a meticulous layered skin closure to achieve ideal wound construction and avoid a permanently visible scar.
Patient Selection
-
Temporal brow ptosis with limited medial brow ptosis
-
Temporal hairline sufficient distance from brow to allow lift
-
Patient without history of scarring problems (keloid, etc.)
-
More acceptable in older patients with bushy brow and prominent forehead rhytids
-
Patient willing to accept possibility of visible surgical scar (incision readily apparent long term in 5 % of patients)
Procedure
-
Mark temporal brow over area of expected lift.
-
In upright position, lift brow to determine amount of excision (Fig. 101.1).
Fig. 101.1 
Demonstration of brow marking in the upright position to determine amount of temporal suprabrow tissue for excision
-
After anesthesia, incise skin, beveling medially to parallel brow cilia.
-
Excise skin and subcutaneous fat, stopping at frontalis muscle.
After hemostasis, layered closure:
-
1.
Subcutaneous layer inverted 5-0 Vicryl
-
2.
Deep dermis inverted 5-0 Vicryl
-
3.
Skin 5-0 nylon (prefer running vertical mattress medially, simple running laterally) (Fig. 101.2)
Fig. 101.2 
Vertical running closure that provides excellent eversion while breaking up line of closure
-
1.


Postoperative
-
Antibiotic ointment three times daily
-
Suture removal 6 days
-
Incision generally imperceptible once erythema fades at 3–6 months (Fig. 101.3)
Fig. 101.3 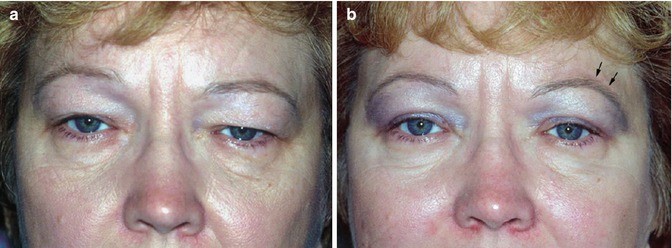
Patient (a) preoperatively and (b) 3 months postoperatively after limited upper blepharoplasty bilaterally with left direct browlift to correct congenital brow asymmetry. Note barely visible incision line

Complications
Cosmetically objectionable scar or contour abnormality usually responds to waiting 3–6 months for scar maturation. Occasional incisional revision required.
Medial undercorrection suggests the selection of an inappropriate procedure and may be improved with botulinum toxin therapy or further surgery.
Forehead hypesthesia may result from damage to the supraorbital or supratrochlear neurovascular bundles from inappropriate deep medial excision.
Conclusion
The direct browlift is an effective cosmetic technique for the limited correction of temporal brow ptosis. Patient selection and appropriate surgical technique are key in achieving an adequate surgical result.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Holds, J.B. (2015). The Direct Browlift: Focus on the Tail. In: Hartstein, MD, FACS, M., Massry, MD, FACS, G., Holds, MD, FACS, J. (eds) Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1544-6_101
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1544-6_101
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1543-9
Online ISBN: 978-1-4939-1544-6
eBook Packages: MedicineMedicine (R0)