
Abstract
Postmortem studies of schizophrenia have historically been focused on abnormalities of neurons, with only a small but growing body of work focused on astroglia. The limitations of this approach are reflected by the recent failed efficacy of several neuron-centric pharmacological treatments. In this chapter, we will review glutamate neurochemistry and present a novel hypothesis related to astrocyte dysfunction in schizophrenia. We posit that plasma membrane glutamate transporters expressed on astrocytes help partition extrasynaptic regions, where pools of extracellular glutamate may be tightly regulated. These so-called “glutamate microdomains” may impact excitatory neurotransmission via modulation of extrasynaptic glutamate receptors. This hypothesis is supported by structural, biochemical and electrophysiological evidence, which suggests that the fidelity of these domains could be altered in severe mental illness.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
16.1 Introduction
The study of severe mental illness includes materials/data obtained from living patients, animal models, and postmortem studies using brain tissues from afflicted patients. This review will primarily focus on postmortem studies that inform the hypothesis that remodeling of astroglial processes leads to glutamate spillover in glutamate circuits. We also argue that there are specialized extracellular regions, or microdomains, where glutamate levels are tightly regulated and contribute to astrocyte-neuron interactions via modulation of extrasynaptic glutamate receptors. We will present data that argue for an abnormality of extracellular glutamate microdomains secondary to astroglial deficits found in the brain in schizophrenia.
The focus of this chapter on astrocyte-associated changes in schizophrenia represents an important extension of the glutamate hypothesis of schizophrenia beyond the N-methyl-D-aspartate (NMDA) receptor signaling complex. For decades, the prevailing hypotheses of schizophrenia were centered on neurotransmitter receptor dysfunction, first with D2 dopamine receptors , and more recently NMDA subtype of glutamate receptors. Studies focused on these hypotheses explored how changes in neurotransmitter receptors localized to the postsynaptic density (PSD) or presynaptic structures on neurons contributed to the pathophysiology of severe mental illness (reviewed in (McCullumsmith et al. 2004a)) . In general, the interpretation of the data in these studies is biased towards the view that observed changes in variables such as measures of receptor subunit gene expression reflect a primary deficit in pre- or postsynaptic neurons. In the sections below, we seek to develop a more balanced view of the role(s) of astroglia in the pathophysiology of this often devastating illness.
16.2 Glutamate Neurotransmission
Glutamate Release and Reuptake
The process of release, activity as a ligand, and reuptake of glutamate involves three distinct cell types: the astrocyte, the presynaptic neuron and the postsynaptic neuron (Salt et al. 1996) . In the presynaptic neuron, glutamine can be converted to glutamate by the enzyme glutaminase, and packaged into vesicles by a family of vesicular glutamate transporters (VGLUT1–3) for release into the synapse (Bellocchio et al. 2000; Takamori et al. 2000) . Glutamate is released into the synapse and may occupy and activate ionotropic [NMDA, α-amino-3-hydroxy-5-methyl-isoxazole propionate (AMPA), and (kainate) or metabotropic (mGluR1-8) glutamate receptors on both neurons and astrocytes (Hollmann and Heinemann 1994; Hollmann et al. 1994; Salt et al. 1996) . Glutamate is rapidly removed from the synapse by a family of plasma membrane excitatory amino acid transporters, localized to postsynaptic neurons and astrocytes (Masson et al. 1999b) . Recovered glutamate may enter the tricarboxylic acid cycle via conversion to alpha-ketoglutarate by glutamate dehydrogenase, be converted to glutamine by glutamine synthetase and transported back into the synapse, or be released into the extracellular space by a variety of mechanisms (Malarkey and Parpura 2008) , including the cystine/glutamate antiporter . In astrocytes, glutamate may also be added to this cycle via de novo synthesis of glutamate in a pathway involving pyruvate carboxylase and transaminases (Brainard et al. 1989; Patel et al. 2001; McKenna 2011) . Recovered glutamate can also contribute to formation of lactic acid. Lactate production is favored in astrocytes, while lactate breakdown is favored in neurons (Stobart and Anderson 2013) . Lactate may be efficiently shuttled from astrocytes to neurons, suggesting that lactic acid may be a preferred energy source for neuronal structures enveloped by astrocytic processes (Stobart and Anderson 2013). Finally, several families of novel glutamate receptor and transporter associated molecules regulate glutamate release and reuptake through intracellular signaling mechanisms (Jackson et al. 2001; Lin and Maiese 2001; Marie et al. 2002; Watanabe et al. 2003) .
Glial Plasma Membrane Glutamate Transporters
The excitatory amino acid transporters (called EAATs in human) are expressed in the plasma membranes of neurons and glia throughout the brain in a region and cell specific manner (Arriza et al. 1993; Utsunomiya-Tate et al. 1996) . EAATs mediate glutamate transport by an electrogenic exchange of 3 Na+, 1 H+, and 1 glutamate (monovalent anion at conditions in the brain) molecule into the cell and 1 K+ ion out of the cell, with the net inward movement of positive charges (Zerangue and Kavanaugh 1996; Levy et al. 1998) . EAATs are likely homomers comprised of 2–3 non-covalently linked subunits that have 6–10 transmembrane domains (Danbolt 2001). The transporters have specific patterns of cellular localization: EAAT1 and EAAT2 have primarily been localized to astroglia. EAAT3–4 and EAAT5 are primarily localized to neurons and the retina, respectively (Arriza et al. 1997; Danbolt 2001). In the prefrontal cortex, glial transporters (EAAT1 and EAAT2) are predominately expressed in discrete subsets of astrocytes which account for approximately 90 % of synaptic glutamate reuptake (Regan et al. 2007) . The glial transporters are localized to perisynaptic processes facing the synaptic cleft (Tzingounis and Wadiche 2007) . In the rodent, activation of the promoters and expression of EAAT1 (called GLAST in the rodent) and EAAT2 (GLT-1 in rodent) is generally nonoverlapping (Regan et al. 2007) . In addition, the GLAST, but not GLT-1, promoter was activated and EAAT1 expressed in oligodendrocytes, suggesting that EAAT1 has a role in myelination and CNS connectivity (Regan et al. 2007) . The functional importance, perisynaptic localization, and heterogeneity of expression of the glial glutamate transporters suggests that examination of the expression and function of these molecules may be a high yield target for studies of neuropsychiatric illnesses that involve alterations in glutamate transmission .
EAAT Expression, Processing, and Trafficking
EAATs are synthesized in the endoplasmic reticulum and have extensive posttranslational modification in the Golgi, including N-linked glycosidation of at least two sites which are important for homomultimer formation (Kalandadze et al. 2004) . EAATs are then trafficked to the plasma membrane where localization and clustering are regulated by protein-protein interactions and phosphorylation (Conradt and Stoffel 1997; Figiel and Engele 2000; Gamboa and Ortega 2002; Schluter et al. 2002; Figiel et al. 2003) . Ultrastructural studies indicate that most EAAT1-2 expression is in the plasma membrane (Chaudhry et al. 1995) . EAATs may be removed from the plasma membrane via endocytosis and shuttle back to the cell surface via recycling endosomes, or be targeted for degradation in lysosomes (Nakagawa et al. 2008) .
Extracellular Glutamate
Glutamate released at the presynaptic terminal diffuses out of the synaptic cleft and may be transported into the astrocyte by EAATs or spillover to extrasynaptic areas (Masson et al. 1999a; Bridges et al. 2012) . Extrasynaptic glutamate may also originate from astrocytes via vesicular release, the cystine/glutamate antiporter (also known as the system Xc − ) , or other less prominent mechanisms (Montana et al. 2004; Haydon and Carmignoto 2006; Bridges et al. 2012) . The cystine/glutamate antiporter releases glutamate and transports cystine into the astrocyte for glutathione synthesis. Glutamate levels in the extracellular milieu are postulated to be tightly regulated, as activation of extrasynaptic glutamate receptors has potent effects. For example, activation of extrasynaptic NMDA receptors promotes initiation of NMDA spikes, while long-term potentiation (LTP) and long-term depression (LTD)can be readily induced in the adult cortex by activation of extrasynaptic GluN2B containing NMDA receptors (Massie et al. 2008; Chalifoux and Carter 2011) .
Removal of glutamate from the synaptic cleft may be conceptualized as a two-step process, involving first the high affinity binding of glutamate by perisynaptic transporters, and second the transport of bound glutamate by the transporter across the plasma membrane (Tong and Jahr 1994; Tzingounis and Wadiche 2007) . Once bound, glutamate may be “unbound” or released, or alternatively, transported across the plasma membrane (Tong and Jahr 1994; Tzingounis and Wadiche 2007). The “capture efficiency” of the EAATs is defined as the ratio of the rate of unbinding of glutamate to rate of transport, which is reported to be about 0.5 (Tzingounis and Wadiche 2007). The relatively low rate of transport of bound glutamate compared to the capture efficiency suggests that the EAATs first act as buffers for released glutamate (Tzingounis and Wadiche 2007). Thus, glutamate molecules may bounce from one transporter binding site to another, until transported, limiting glutamate spillover from the synaptic cleft
Glutamate Spillover
The density of perisynaptic glutamate transporter protein, the amount of glutamate released, and the rate of glutamate transport determine, in part, the kinetics of glutamate diffusion away from the synaptic cleft. While several regions have well characterized glutamate spillover between excitatory synapses (such as the cerebellum and hippocampus), there is ongoing debate regarding the extent of glutamate diffusion in other regions, including the frontal cortex, where spillover of glutamate may detrimentally lead to loss of input specificity and activation of cell death pathways (Kullmann and Asztely 1998; Hardingham and Bading 2002; Hardingham et al. 2002; Lozovaya et al. 2004a; Tsvetkov et al. 2004; Marcaggi and Attwell 2007; Leveille et al. 2008) . Under physiologic conditions, release of glutamate may exceed the capacity of cortical synapses to remove glutamate from the cleft (Weng et al. 2007; Drew et al. 2008) . Mathematical models suggest that glutamate may diffuse and activate NMDA receptors within a radius of 0.5 µm from the release point (Rusakov and Kullmann 1998) . Thus, the spatial arrangement of glutamate synapses, their glutamate transporter buffering zones, and extrasynaptic glutamate receptors will determine the extent and effect of glutamate spillover (Lehre and Danbolt 1998; Sem’yanov 2005; Weng et al. 2007) .
Glutamate Microdomains
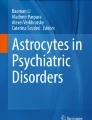
We posit that glutamate microdomains are formed by specialized protein clusters on the membranes of astrocytic processes apposed to extrasynaptic glutamate receptors expressed on specialized regions of neuronal membranes (Fig. 16.1) (Grosche et al. 1999; Genda et al. 2011) . Diffusion of glutamate between domains or domains and synapses would be limited by the dense expression of glutamate transporters between these specialized structures (Lehre and Danbolt 1998) .

Glutamate microdomains may be formed by specialized protein complexes found on plasma membranes in extrasynaptic regions where astrocytic and neuronal membranes are opposed to one another. Glutamate is released into the synapse (red shading) where it may bind and activate glutamate receptors. Plasma membrane glutamate transporters localized to perisynaptic astroglial processes bind and transport glutamate (green shading). Glutamate levels in extrasynaptic regions (yellow shading) may be regulated by glutamate spillover from synapses, release of glutamate from astrocytes, as well as reuptake of glutamate by glutamate transporters
Extrasynaptic Glutamate Receptors
The G-protein linked mGluRs have a central role in regulating synaptic glutamate. mGluRs are expressed perisynaptically, and activation of mGluR2/3 receptors decreases presynaptic glutamate release (Schoepp 2001) . Thus, activation of mGluRs may serve as a brake on glutamate spillover, preserving input specificity by diminishing synaptic glutamate levels (Huang and Bergles 2004) . This mechanism has recently been exploited to develop a highly selective mGluR2 agonist that decreases glutamate release (Patil et al. 2007) . This development suggests a role for the pharmacological modulation of glutamate spillover as a treatment for schizophrenia and other illnesses where psychosis is a central feature .
16.3 The Schizophrenia Syndrome
Schizophrenia is most properly considered to be a syndrome, as its specific causes are unknown, and the diagnosis is based on the presence of a heterogeneous collection of signs and symptoms. There is no blood test, specific genetic marker, or cognitive battery that can predict who will develop this illness. The schizophrenia phenotype is characterized by the presence of specific clinical findings, often divided into positive, negative, and cognitive symptoms (Buchanan et al. 2000) .Positive symptoms include hallucinations, which are often auditory. Patients report that they hear voices that are clearly located outside of their heads, most often engaged in a running commentary on their thoughts and behaviors (Kay 1990; Badcock 2010) . Other common positive symptoms include paranoid delusions and disorders of thought processes (Kay 1990; Badcock 2010) . Much more debilitating are the negative symptoms, which are associated with the diminution of normal social behaviors, and include withdrawal, decreased speech, diminished eye contact, decreased or muted facial expression and vocal inflection, and diminished spontaneous movement (Buchanan et al. 2000; Fleischhacker 2000) . Cognitive impairments in this illness include, but are not limited to, deficits in verbal fluency, executive function, and working memory (Rajji and Mulsant 2008; Szoke et al. 2008; Wobrock et al. 2008; Potkin et al. 2009; Zanello et al. 2009) . Few individuals suffering from schizophrenia have all of these symptoms, but the persistence of several characteristic symptoms, like auditory hallucinations, must be present in order for someone to be diagnosed with this disorder (Buchanan et al. 2000) .
16.4 Prevailing Hypotheses of Schizophrenia
For decades, scientists have focused on the dopamine hypothesis of schizophrenia, which postulates that dysregulated dopaminergic neurotransmission is a key feature of the pathophysiology of the illness. The dopamine hypothesis is based on the observation that antipsychotics block D2 receptors, and antipsychotic affinity for these receptors correlates with the ability to attenuate psychotic symptoms. Although numerous studies point to dopaminergic abnormalities in schizophrenia, dopamine dysfunction cannot completely account for all of the symptoms observed, since neuroleptics typically are effective only for the positive symptoms of the illness while negative symptoms and cognitive deficits are relatively refractory to treatment with typical antipsychotics (Joyce and Meador-Woodruff 1997; Laruelle et al. 1999) . Consequently, alternative hypotheses that may help explain the pathophysiology of schizophrenia have been sought.
While the dopaminergic neurotransmitter system was implicated due to the effects of antipsychotic drugs, this system does of course not act in isolation. Dopamine receptors are found throughout the brain where they modulate excitatory and inhibitory neurotransmission via G-protein signaling pathways. Blockade of dopamine receptors in corticolimbic circuits directly alters release of other neurotransmitters including glutamate and γ-aminobutyric acid (GABA). Not surprisingly, extensive postmortem studies have found changes in glutamatergic and GABAergic systems in this illness (Alda et al. 1996; Lewis et al. 2004; Deep-Soboslay et al. 2011; McCullumsmith and Meador-Woodruff 2011) . However, evidence for involvement of glutamate receptor dysfunction, in particular the NMDA-subtype glutamate receptor, suggests a prominent role for glutamatergic abnormalities. NMDA receptor antagonists (but not GABA receptor antagonists) can induce both the positive and negative symptoms of schizophrenia, including cognitive deficits (Javitt and Zukin 1991; Tamminga 1999) . Moreover, these compounds can exacerbate both positive and negative symptoms in schizophrenia (Lahti and Tamminga 1995) . Chronic administration of phencyclidine (PCP)-like compounds induces a persistent psychotic symptomatology (Tsai and Coyle 2002) and reduces frontal lobe blood flow and glucose utilization, which is remarkably similar to the “hypofrontality” described in schizophrenia (Hertzmann et al. 1990) .
Despite these observations, the complexity of schizophrenia is not readily explained by a static neurochemical model. The onset of schizophrenia is typically in late adolescence or early adulthood (Alda et al. 1996) . The onset of positive and negative symptoms in a previously normally functioning person, coupled with a lifetime of waxing and waning symptoms, accompanied by the possibility of a steady decline in social, occupational, and cognitive functioning, has led to longitudinal neurodevelopmental models that take into account genetic and environmental factors (Marenco and Weinberger 2000) . Data supporting the neurodevelopmental hypothesis includes studies suggesting that schizophrenia is associated with late winter births in urban environments, as well as a number of other prenatal, perinatal, and postnatal events (Marenco and Weinberger 2000; Lewis and Levitt 2002) . Schizophrenia is perhaps best considered a disorder of neuroplasticity (McCullumsmith et al. 2004a). Plasticity refers to the ability of a system to effect reversible, long term changes in response to stimuli. Molecular correlates of learning and memory, including LTP and LTD, likely facilitate neuroplasticity in the brain; these processes are significantly impaired in severe mental illnesses, including schizophrenia (Malenka and Nicoll 1999; McCullumsmith et al. 2004b; Talbot et al. 2009) . Glutamate transmission is a central component of LTP and LTD, and hence has a central role in plasticity.
16.5 Glutamatergic Abnormalities in Schizophrenia
A number of studies have evaluated glutamate neurotransmission is schizophrenia using different approaches. In this section we first discuss data from magnetic resonance spectroscopy (MRS), a technique which is largely focused on measuring glutamate, glutamine, and associated metabolites in specific brain regions of living patients. A strength of these studies is that the data are collected from afflicted individuals relatively close in time to the onset of the illness, while postmortem studies are examining brain tissues from more aged individuals who have had a lifetime of psychiatric illness. Next, we will briefly discuss data from postmortem studies, with a particular focus on extrasynaptic glutamate receptors and astroglial transporters.
Magnetic Resonance Spectroscopy Findings in schizophrenia
The balance of studies using MRS to examine glutamate, glutamine, N-acetylaspartate (NAA), and other metabolic intermediates have yielded mixed results (Bartha et al. 1997; Deicken et al. 1997; Theberge et al. 2002; Hutcheson et al. 2012; Kraguljac et al. 2012b) . While a couple of studies have found changes in glutamate in schizophrenia, one large meta-analysis found decreases in the glutamate metabolite NAA in the basal ganglia and frontal lobe (Kraguljac et al. 2012a, 2012b) . Changes in NAA levels suggest abnormalities of glutamate synthesis and/or cycling in schizophrenia (Clark et al. 2006) . A different meta-analysis found decreased glutamate and decreased glutamine in the medial frontal cortex in schizophrenia, suggesting that glutamate neurotransmission is diminished in this illness (Marsman et al. 2011) . One interesting finding from these studies is the loss of correlation between NAA and glutamate levels in subjects with schizophrenia, compared to disease-free control subjects (Hutcheson et al. 2012; Kraguljac et al. 2012a). Taken together with the meta-analyses, these data suggest a significant abnormality in the glutamate/glutamine cycle in limbic circuits in schizophrenia. One limitation of the MRS approach is that it measures all glutamate, glutamine or NAA without regard for it/them being intra or extracellular. For example, there may be a global increase in glutamine in the anterior cingulate cortex, with a large increase in intracellular pools, and a small decrease in extracellular levels.
Abnormalities of Glutamatergic Enzymes in Schizophrenia
There are several key enzymes involved in the glutamate/glutamine cycle as well as the synthesis or break-down of glutamate. Changes in enzymes levels may impact the amount of glutamate available for release from neurons and glial cells. Several studies have found decreased expression of carboxypeptidase II (binding and activity), glutaminase (mRNA), and glutamaine synthetase (mRNA and protein) in limbic regions in schizophrenia (Burbaeva et al. 1999; Goff and Coyle 2001; Laruelle et al. 2003; Bruneau et al. 2005) . Other studies have found increases in glutaminase (mRNA and activity) (Gluck et al. 2002; Bruneau et al. 2005) . While these data support the hypothesis that glutamate synthesis and cycling may be impaired in schizophrenia, all of these studies were done at the regional level, and thus fail to capture the complexity of glutamate synapses at the cellular or subcellular level. For example, there may be diminished expression of glutamate enzymes in astrocytes, but increased expression in pyramidal neurons. Finally, one of the most interesting findings is a decrease in the dipeptidase glutamate carboxypeptidase II (GCP II; also known as NAALADase) activity in the frontal cortex and hippocampus in schizophrenia. GCPII catabolizes N-acetylaspartyl glutamate (NAAG) to glutamate and NAA (Ghose et al. 2004) . These findings are consistent with the MRS data discussed above which found decreased levels of NAA. NAAG antagonizes NMDA receptors, and increased levels (secondary to diminished GCP II activity) might contribute to NMDA receptor hypofunction. One strength of this study is that the authors measured enzyme activity, and not just transcript or protein levels, a technically demanding approach (Tsai and Coyle 2002) .
Glutamate Receptor Abnormalities in Schizophrenia
The observation that PCP may cause a schizophreniform psychosis in persons without a prior diagnosis of schizophrenia led to investigation of ionotropic glutamate receptor expression in schizophrenia. Initial hypotheses were focused on the idea that a loss or hypofunction of NMDA receptor activity would be reflected by diminished expression of NMDA receptor subunits as well as NMDA receptor binding sites. However, on balance, studies of NMDA receptor expression in the postmortem brain in schizophrenia have no clear or consistent pattern of findings (McCullumsmith et al. 2012). For example, there are over 18 studies of NMDA receptor subunit expression in the frontal cortex alone, and other than some changes in binding site expression, the hypothesis that there is deficient NMDA receptor expression stands largely unproven (McCullumsmith et al. 2012) . Similar to NMDA receptors, AMPA and kainate receptor studies generally do not have a consistent pattern of abnormalities other than perhaps changes in AMPA receptor GluA2 subunit expression in the hippocampus (Tamminga 1999; Meador-Woodruff et al. 2001a; Harrison 2004) . Interestingly, administration of PCP, which blocks the NMDA receptor channel, leads to increased glutamate release, which may lead to spillover of glutamate from the synaptic cleft to extrasynaptic areas, activating extrasynaptic (non-NMDA) glutamate receptors. This mechanism may simulate/reflect the condition in schizophrenia where impaired astrocyte function leads to diminished glutamate buffering and reuptake.
Metabotropic Receptor Expression in Schizophrenia
While there are fewer postmortem studies of mGluRs, compared to ionotropic receptors , the data are no less contradictory. For example, mGluR3 protein expression has been reported as increased, decreased and unchanged in the frontal cortex (Gupta et al. 2005; Corti et al. 2007; Ghose et al. 2009; Shan et al. 2012) . Genetic linkage studies suggest that mGluR5 is involved in schizophrenia, and increased mGluR5 and mGluR1 transcript, and mGluR1 protein expression have been found in prefrontal cortex in this illness (Ohnuma et al. 1998; Devon et al. 2001; Gupta et al. 2005; Volk et al. 2010) .
Abnormalities of Glutamate Transporters in Schizophrenia
Several studies have reported region-level changes in the expression of the glial glutamate transporters EAAT1 and EAAT2 in schizophrenia. EAAT1 protein expression was decreased and EAAT1 glycosylation altered in the dorsolateral prefrontal cortex (DLPFC) (Bauer et al. 2008, 2010) . Decreased EAAT1 and EAAT2 protein was found in the superior temporal gyrus, while only EAAT2 protein was decreased in the hippocampus (Shan et al. 2013) . In contrast to these protein studies, increased levels of EAAT1 mRNA were found in the anterior cingulate cortex and thalamus (Smith et al. 2001; Bauer et al. 2008; Rao et al. 2012) , suggesting a compensatory response to diminished glutamate reuptake capacity. Alterations in EAAT2 mRNA have also been reported in the hippocampus (decreased) and neocortex (increased, decreased and unchanged) in schizophrenia (Ohnuma et al. 1998, 2000; Matute et al. 2005; Lauriat et al. 2006; Bauer et al. 2008; Rao et al. 2012) .
The neuronal transporters have also been studied. We have previously reported increased expression of EAAT3 protein and mRNA in the anterior cingulate cortex, while other studies have measured EAAT3 mRNA expression in the frontal cortex (increased), DLPFC (no change) and striatum (decreased) (McCullumsmith and Meador-Woodruff 2002; Lauriat et al. 2006; Nudmamud-Thanoi et al. 2007; Bauer et al. 2008; Horiuchi et al. 2012; Rao et al. 2012) . No changes in EAAT3 protein levels were detected in the superior temporal gyrus or hippocampus (Shan et al. 2013) . These conflicting data for neuronal glutamate transporters mirror the findings of glutamate receptor subunit expression, and are limited by the likelihood that glutamate transporter expression changes may be cell-specific, and change in different directions in different populations of cells. These findings have contributed to reformulation of the glutamate hypothesis of schizophrenia, with the idea that changes in glutamate receptor and/or transporter expression in schizophrenia is not a problem of too much or too little protein expression, but a problem with protein trafficking or signaling. Localization and activity of astroglial-localized glutamate transporters is mediated, in part, by protein-protein interactions. Expression of some of these EAAT interacting proteins has been assessed in severe mental illness.
EAAT Interacting Proteins in Schizophrenia
Several glutamate transporter interacting molecules have been identified, including G-protein suppressor pathway 1 (GPS1), JWA, ARHGEF11, and KIAA0302 (also called beta III spectrin). These molecules can affect glutamate transport function through trafficking , anchoring, phosphorylation, glycosylation, and degradation of transporters in the brain. For example, GPS1 decreases EAAT2 mediated glutamate reuptake through a direct protein-protein interaction, and levels of GPS1 protein were elevated in the frontal cortex in schizophrenia. These data suggest that there may be normal levels, but decreased activity, of a specific transporter due to modulation of transporter function or localization to the plasma membrane (Bauer et al. 2008).
In summary, changes in glutamate neurotransmission in schizophrenia point towards complex abnormalities of protein localization and function, contributing to the molecular neuropathology that underlies the schizophrenia phenotype.
16.6 Glutamate Spillover in Schizophrenia
Glutamate Spillover in Schizophrenia
As outlined above, several postmortem studies have found changes in EAAT expression in schizophrenia, as well as changes in the molecules that regulate EAAT localization and activity (Ohnuma et al. 1998, 2000; Smith et al. 2001; McCullumsmith and Meador-Woodruff 2002; Lauriat et al. 2006; Bauer et al. 2008) . In general, these changes in gene expression are consistent with diminished regional expression of astroglial (but not neuronal) glutamate transporter expression and activity. Further, a recent genetic study analyzing copy number variants reported a subject with schizophrenia with a deletion of several EAAT1 exons (Cook and Scherer 2008) . Finally, characterization of the complete GLAST (EAAT1) knockout found changes consistent with behavioral endophenotypes associated with schizophrenia, including locomotor hyperactivity and abnormal social behavior (Karlsson et al. 2008, 2009) . Several of these abnormal behavioral findings were reversed by administration of antipsychotic medication or mGluR2/3 receptor agonist administration, which decreases presynaptic glutamate release. These data suggest that there are region specific deficits in EAAT reuptake capacity in schizophrenia which could lead to glutamate spillover.
Chronic Glutamate Spillover May Lead to Remodeling of Synapses
In the prefrontal cortex (PFC) in schizophrenia, there are changes in the structure, composition, and numbers of excitatory synapses (Broadbelt et al. 2002; Lewis et al. 2003, 2008) . Increased packing density, decreased numbers of dendritic spines and diminished expression of structural proteins suggest significant alterations of synapses in this region (Selemon et al. 1995; Rajkowska et al. 1998, 2002) . Several reports have found specific alterations in layers III and IV of the PFC, including abnormalities of pyramidal cells and interneurons (Hashimoto et al. 2003; Dong et al. 2005; Huang and Akbarian 2007; Huang et al. 2007; Lewis et al. 2008) . One well replicated finding is a decrease in parvalbumin positive interneurons in the middle cortical layers (Lewis et al. 2001; Hashimoto et al. 2003) . A lamina specific deficit in inhibitory tone could lead to increased release of glutamate, which combined with diminished reuptake capacity could lead to increased glutamate spillover.
Accumulating evidence from postmortem gene expression studies suggests neurochemical alterations consistent with spillover. We have found increased mGluR2/3 protein in the PFC (Gupta et al. 2005) , which may be interpreted as an attempt by synapses to decrease spillover by decreasing presynaptic release. Expression of the cystine/glutamate antiportercatalytic subunit (xCT) was also increased in the DLPFC (Baker et al. 2008) . This molecule is expressed on glia and releases glutamate into the extrasynaptic space in exchange for uptake of cystine, which is required for glutathione synthesis. The effect of increased xCT protein expression on glutamate release is not known, because it is the activity, and not expression level, of this molecule that determines the rate of glutamate release. However, changes in the expression of xCT minimally suggest abnormalities of the regulation of extracellular glutamate levels (Baker et al. 2008) . Finally, anumber of studies have also described changes in ionotropic glutamate receptor binding site expression, suggesting a change in NMDA and AMPA receptor stoichiometry in the frontal cortex in schizophrenia (Akbarian et al. 1996; Healy et al. 1998; Ibrahim et al. 2000; Meador-Woodruff et al. 2001b; Beneyto and Meador-Woodruff 2006; Beneyto et al. 2007; Harney et al. 2008) . Interestingly, preclinical studies have shown that glutamate spillover is associated with alterations in ionotropic receptor subunit composition and function (Lozovaya et al. 2004b; Harney et al. 2008) .
We propose that there is remodeling of glutamate synapses in schizophrenia secondary to glutamate spillover (Fig. 16.2). Glutamate spillover may be secondary to increased release (in a misguided attempt to activate “sick” NMDA receptors), as well as deficits in glutamate reuptake capacity. In this setting, we would predict that perisynaptic localization of glutamate transporters on the plasma membrane of astrocytes is diminished, either as a primary deficit in transporter localization, as a compensation for increased extrasynaptic glutamate release, or both. Redistribution of glutamate transporters on astrocytes would lead or contribute to increased spillover, causing excitotoxicity and loss of input specificity. Further, we postulate that these deficits are initially relatively subtle, but chronic in nature, leading to inappropriate remodeling of excitatory synapses which do not function normally. This idea is supported by the phenotype of the GLAST/EAAT1 knockout mice, which have moderate cognitive and behavioral impairment, but no morbidity or mortality associated with seizures (Watase et al. 1998; Karlsson et al. 2008, 2009) .

There are likely a number of primary causes which yield the constellations of symptoms found in schizophrenia. Proximate causes might include NMDA receptor dysfunction or abnormalities of glutamate microdomains. The red boxes may be a final common pathway that contributes to the phenotype of this syndrome
16.7 A Role for Glutamate Microdomains
Glutamate Microdomains
Critical to cellular function of proteins is subcellular locality or microenvironment, in which proteins cluster and interact with numerous others . These biologically and morphologically discrete microdomains require tightly regulated trafficking of component proteins and thus organize the intermolecular environment for proteins and their interactions (Grosche et al. 1999; Hemler 2003; Füllekrug and Simons 2004; Tzingounis and Wadiche 2007; Farr et al. 2009; Newpher and Ehlers 2009) . Evidence for cortical glutamate microdomains is based on several observations: (1) extracellular glutamate levels may vary between 0.2–7 µM in the extrasynaptic space in a region- and milieu- dependent manner; (2) a large body of work has described localization of functional glutamate receptors outside of synapses; (3) the localization and buffering/transport properties of glutamate transporters strongly suggests partitioning of non-synaptic extracellular spaces; (4) several recent studies have characterized the functional coupling of protein complexes, structural proteins, organelles, and signaling pathways that converge on cellular processes involving glutamate and finally; (5) glial cells may form electronically-independent morphological structures that ensheath neuronal structures of unknown function (Grosche et al. 1999, 2002; Szabadkai and Rizzuto 2007; Spat et al. 2009; Genda et al. 2011) . Taken together, these data suggest that glutamate microdomains are formed by specialized regions of astrocytic processes and neuronal membranes (Fig. 16.1) (Grosche et al. 1999; Genda et al. 2011) . Glutamate levels within these domains may be determined by spillover from synapses or release from astrocytes (Fig. 16.1) (Lehre and Danbolt 1998) .
The composition and function of specialized protein clusters in astrocytes has recently been investigated in rodent brain tissues. Using immunoisolation, one study found a complex comprised of GLT-1 (the rodent isoform of EAAT2), Na+/K+-ATPase, hexokinase, and mitochondria (Genda et al. 2011) , while another found Na+/K+-ATPase, the water channel aquaporin 4, and mGluR5 (Fig. 16.2) (Illarionova et al. 2010) . Other studies have found functional coupling of glutamate reuptake, cytosolic and mitochondrial sodium exchange, and glucose utilization in astrocytes (Hertz 2011; Skytt et al. 2012) . Interacting partners and ultrastructural localization have not been determined for the cystine/glutamate antiporter .
Evidence for Abnormalities of Glutamate Microdomains in Schizophrenia: Structural Abnormalities
In the frontal cortex in schizophrenia there are changes in volume and cell density suggesting significant alterations in the spatial arrangement of synapses and microdomains in this illness (Selemon et al. 1995; Rajkowska et al. 1998, 2002; Broadbelt et al. 2002; Lewis et al. 2003; Lewis and Gonzalez-Burgos 2008) . Specifically, there is thinning of cortical gray matter accompanied by decreased density of astrocytes as well as a loss of neuropil, while the balance of studies has typically found no changes in the number of neurons (Selemon et al. 1995; Rajkowska et al. 1998, 2002; Broadbelt et al. 2002; Lewis et al. 2003; Lewis and Gonzalez-Burgos 2008) . These findings suggest a marked abnormality in the ultrastructural elements that account for the large volume of gray matter not occupied by cell bodies or synapses.
Abnormalities of Mitochondria
A few studies have assessed the density of mitochondria in schizophrenia . One study found a decrease in the number of mitochondria per synapse in the striatum in treatment responsive subjects with schizophrenia, while another found decreased volume fraction and area density of mitochondria in subjects with duration of disease more than 21 years (Uranova et al. 2001; Somerville et al. 2011, 2012) . In addition, decreased expression of transcripts for a mitochondrial proton transporter were found in the frontal cortex in schizophrenia, and association of the glycolytic enzyme hexokinase 1 with mitochondria was decreased in the parietal cortex in this illness (Gigante et al. 2011; Regenold et al. 2012) . These data suggest an abnormality of mitochondrial coupling in schizophrenia, which may reflect an alteration in the association of mitochondria with proteins that comprise these domains .
Changes in Glutamate Receptor and Transporter Expression
The changes in glutamate receptor and transporter expression detailed above are consistent with diminished glutamate reuptake capacity, indicating increased diffusion of glutamate between synapses and microdomains. In addition, changes in extrasynaptic expression of the cystine/glutamate antiporter (which releases glutamate from astrocytes) indicate an increased capacity for extrasynaptic release of glutamate (Kristiansen and Meador-Woodruff 2005; Baker et al. 2008) . Both of these mechanisms could lead to increased activation of extrasynaptic glutamate receptors in extracellular glutamate microdomains.
16.8 Conclusions
We propose that there is increased activity of extrasynaptic glutamate receptors in schizophrenia secondary to increased levels of extrasynaptic glutamate (Fig. 16.2). Increased extrasynaptic glutamate may be due to increased presynaptic release and spillover (in a misguided attempt to activate sick NMDA receptors in the PSD), increased diffusion of glutamate out of the cleft secondary to deficits in glutamate buffering and reuptake capacity, and/or increased release of glutamate from astrocytes. In this setting, we would predict that integrity of glutamate microdomains is disrupted, either as a primary deficit in the assembly and localization of these domains, as a compensation for increased synaptic glutamate release and spillover, or both. Regardless of the mechanism, we hypothesize that the composition and localization of astrocytic proteins in glutamate microdomains is abnormal in schizophrenia, leading to pathological neuroplastic changes in the structure and function of glutamate circuits in schizophrenia.
Interestingly, several promising trials of various glutamate receptor modulators have failed to yield new pharmacological treatments for schizophrenia, including NMDA receptor glycine-site agonists (targeting NMDA receptors in the PSD), AMPA receptor modulators, called AMPAkines (targeting AMPA receptors in the PSD), and more recently mGluR2 modulators (targeting presynaptic release of glutamate). The challenges of developing effective glutamatergic drugs may be harder to surmount because the pathosphysiology of excitatory neurotransmission in schizophrenia has generally been viewed in a neuron-centric manner. Viewing abnormalities of glutamate transmission as a problem of astrocyte dysfunction may yield fresh insights for developing pharmacological targets to treat this devastating illness.
References
Akbarian S, Sucher NJ, Bradley D, Tafazzoli A, Trinh D, Hetrick WP, Potkin SG, Sandman CA, Bunney WE Jr, Jones EG (1996) Selective alterations in gene expression for NMDA receptor subunits in prefrontal cortex of schizophrenics. J Neurosci 16:19–30
Alda M, Ahrens B, Lit W, Dvorakova M, Labelle A, Zvolsky P, Jones B (1996) Age of onset in familial and sporadic schizophrenia. Acta Psychiatr Scand 93:447–450
Arriza JL, Kavanaugh MP, Fairman WA, Wu YN, Murdoch GH, North RA, Amara SG (1993) Cloning and expression of a human neutral amino acid transporter with structural similarity to the glutamate transporter gene family. J Biol Chem 268:15329–15332
Arriza JL, Eliasof S, Kavanaugh MP, Amara SG (1997) Excitatory amino acid transporter 5, a retinal glutamate transporter coupled to a chloride conductance. Proc Natl Acad Sci U S A 94:4155–4160
Badcock JC (2010) The cognitive neuropsychology of auditory hallucinations: a parallel auditory pathways framework. Schizophr Bull 36:576–584
Baker DA, Madayag A, Kristiansen LV, Meador-Woodruff JH, Haroutunian V, Raju I (2008) Contribution of cystine-glutamate antiporters to the psychotomimetic effects of phencyclidine. Neuropsychopharmacology 33:1760–1772
Bartha R, Williamson PC, Drost DJ, Malla A, Carr TJ, Cortese L, Canaran G, Rylett RJ, Neufeld RW (1997) Measurement of glutamate and glutamine in the medial prefrontal cortex of never-treated schizophrenic patients and healthy controls by proton magnetic resonance spectroscopy. Arch Gen Psychiatry 54:959–965
Bauer D, Gupta D, Harotunian V, Meador-Woodruff JH, McCullumsmith RE (2008) Abnormal expression of glutamate transporter and transporter interacting molecules in prefrontal cortex in elderly patients with schizophrenia. Schizophr Res 104:108–120
Bauer D, Haroutunian V, Meador-Woodruff JH, McCullumsmith RE (2010) Abnormal glycosylation of EAAT1 and EAAT2 in prefrontal cortex of elderly patients with schizophrenia. Schizophr Res 117:92–98
Bellocchio EE, Reimer RJ, Fremeau RT Jr, Edwards RH (2000) Uptake of glutamate into synaptic vesicles by an inorganic phosphate transporter. Science 289:957–960
Beneyto M, Meador-Woodruff JH (2006) Lamina-specific abnormalities of AMPA receptor trafficking and signaling molecule transcripts in the prefrontal cortex in schizophrenia. Synapse 60:585–598
Beneyto M, Kristiansen LV, Oni-Orisan A, McCullumsmith RE, Meador-Woodruff JH (2007) Abnormal glutamate receptor expression in the medial temporal lobe in schizophrenia and mood disorders. Neuropsychopharmacology 32:1888–1902
Brainard JR, Kyner E, Rosenberg GA (1989) 13C nuclear magnetic resonance evidence for gamma-aminobutyric acid formation via pyruvate carboxylase in rat brain: a metabolic basis for compartmentation. J Neurochem 53:1285–1292
Bridges R, Lutgen V, Lobner D, Baker AM (2012) Thinking outside the cleft to understand synaptic activity: contribution of the cystine-glutamate antiporter (system xc-) to normal and pathological glutamatergic signaling. Pharmacol Rev 64
Broadbelt K, Byne W, Jones LB (2002) Evidence for a decrease in basilar dendrites of pyramidal cells in schizophrenic medial prefrontal cortex. Schizophr Res 58:75–81
Bruneau EG, McCullumsmith RE, Haroutunian V, Davis KL, Meador-Woodruff JH (2005) Increased expression of glutaminase and glutamine synthetase mRNA in the thalamus in schizophrenia. Schizophr Res 75:27–34
Buchanan RW, Carpenter WT, Sadock Be, Sadock Ve (2000) Schizophrenia: introduction and overview. Comprehensive textbook of psychiatry. Lippincott, Williams, and Wilkins, Philadelphia, pp 1096–1110
Burbaeva G, Savushkina OK, Dmitriev AD (1999) Brain isoforms of creatine kinase in health and mental diseases: Alzheimer’s disease and schizophrenia. Vestnik Rossiiskoi akademii meditsinskikh nauk/Rossiiskaia akademiia meditsinskikh nauk, pp 20–24
Chalifoux JR, Carter AG (2011) Glutamate spillover promotes the generation of NMDA spikes. J Neurosci 31:16435–16446
Chaudhry FA, Lehre KP, van Lookeren Campagne M, Ottersen OP, Danbolt NC, Storm-Mathisen J (1995) Glutamate transporters in glial plasma membranes: highly differentiated localizations revealed by quantitative ultrastructural immunocytochemistry. Neuron 15:711–720
Clark JF, Doepke A, Filosa JA, Wardle RL, Lu A, Meeker TJ, Pyne-Geithman GJ (2006) N-acetylaspartate as a reservoir for glutamate. Med Hypotheses 67:506–512
Conradt M, Stoffel W (1997) Inhibition of the high-affinity brain glutamate transporter GLAST-1 via direct phosphorylation. J Neurochem 68:1244–1251
Cook EH Jr, Scherer SW (2008) Copy-number variations associated with neuropsychiatric conditions. Nature 455:919–923
Corti C, Crepaldi L, Mion S, Roth AL, Xuereb JH, Ferraguti F (2007) Altered dimerization of metabotropic glutamate receptor 3 in schizophrenia. Biol Psychiatry 62:747–755
Danbolt NC (2001) Glutamate uptake. Prog Neurobiol 65:1–105
Deep-Soboslay A, Benes FM, Haroutunian V, Ellis JK, Kleinman JE, Hyde TM (2011) Psychiatric brain banking: three perspectives on current trends and future directions. Biol Psychiatry 69:104–112
Deicken RF, Zhou L, Schuff N, Weiner MW (1997) Proton magnetic resonance spectroscopy of the anterior cingulate region in schizophrenia. Schizophr Res 27:65–71
Devon RS, Anderson S, Teague PW, Muir WJ, Murray V, Pelosi AJ, Blackwood DH, Porteous DJ (2001) The genomic organisation of the metabotropic glutamate receptor subtype 5 gene, and its association with schizophrenia. Mol Psychiatry 6:311–314
Dong E, Agis-Balboa RC, Simonini MV, Grayson DR, Costa E, Guidotti A (2005) Reelin and glutamic acid decarboxylase67 promoter remodeling in an epigenetic methionine-induced mouse model of schizophrenia. Proc Natl Acad Sci U S A 102:12578–12583
Drew GM, Mitchell VA, Vaughan CW (2008) Glutamate spillover modulates GABAergic synaptic transmission in the rat midbrain periaqueductal grey via metabotropic glutamate receptors and endocannabinoid signaling. J Neurosci 28:808–815
Farr GA, Hull M, Mellman I, Caplan MJ (2009) Membrane proteins follow multiple pathways to the basolateral cell surface in polarized epithelial cells. J Cell Biology 186:269–282
Figiel M, Engele J (2000) Pituitary adenylate cyclase-activating polypeptide (PACAP), a neuron-derived peptide regulating glial glutamate transport and metabolism. J Neurosci 20:3596–3605
Figiel M, Maucher T, Rozyczka J, Bayatti N, Engele J (2003) Regulation of glial glutamate transporter expression by growth factors. Exp Neurol 183:124–135
Fleischhacker W (2000) Negative symptoms in patients with schizophrenia with special reference to the primary versus secondary distinction. Encephale 26(Spec No 1):12–14
Füllekrug J, Simons KAI (2004) Lipid rafts and apical membrane traffic. Ann N Y Acad Sci 1014:164–169
Gamboa C, Ortega A (2002) Insulin-like growth factor-1 increases activity and surface levels of the GLAST subtype of glutamate transporter. Neurochem Int 40:397–403
Genda EN, Jackson JG, Sheldon AL, Locke SF, Greco TM, O’Donnell JC, Spruce LA, Xiao R, Guo W, Putt M, Seeholzer S, Ischiropoulos H, Robinson MB (2011) Co-compartmentalization of the astroglial glutamate transporter, GLT-1, with glycolytic enzymes and mitochondria. J Neurosci 31:18275–18288
Ghose S, Weickert CS, Colvin SM, Coyle JT, Herman MM, Hyde TM, Kleinman JE (2004) Glutamate carboxypeptidase II gene expression in the human frontal and temporal lobe in schizophrenia. Neuropsychopharmacology 29:117–125
Ghose S, Gleason KA, Potts BW, Lewis-Amezcua K, Tamminga CA (2009) Differential expression of metabotropic glutamate receptors 2 and 3 in schizophrenia: a mechanism for antipsychotic drug action? Am J Psychiatry 166:812–820
Gigante AD, Andreazza AC, Lafer B, Yatham LN, Beasley CL, Young LT (2011) Decreased mRNA expression of uncoupling protein 2, a mitochondrial proton transporter, in post-mortem prefrontal cortex from patients with bipolar disorder and schizophrenia. Neurosci Lett 505:47–51
Gluck MR, Thomas RG, Davis KL, Haroutunian V (2002) Implications for altered glutamate and GABA metabolism in the dorsolateral prefrontal cortex of aged schizophrenic patients. Am J Psychiatry 159:1165–1173
Goff DC, Coyle JT (2001) The emerging role of glutamate in the pathophysiology and treatment of schizophrenia. Am J Psychiatry 158:1367–1377
Grosche J, Matyash V, Moller T, Verkhratsky A, Reichenbach A, Kettenmann H (1999) Microdomains for neuron-glia interaction: parallel fiber signaling to Bergmann glial cells. Nat Neurosci 2:139–143
Grosche J, Kettenmann H, Reichenbach A (2002) Bergmann glial cells form distinct morphological structures to interact with cerebellar neurons. J Neurosci Res 68:138–149
Gupta DS, McCullumsmith RE, Beneyto M, Haroutunian V, Davis KL, Meador-Woodruff JH (2005) Metabotropic glutamate receptor protein expression in the prefrontal cortex and striatum in schizophrenia. Synapse 57:123–131
Hardingham GE, Bading H (2002) Coupling of extrasynaptic NMDA receptors to a CREB shut-off pathway is developmentally regulated. Biochim Biophys Acta 1600:148–153
Hardingham GE, Fukunaga Y, Bading H (2002) Extrasynaptic NMDARs oppose synaptic NMDARs by triggering CREB shut-off and cell death pathways. Nat Neurosci 5:405–414
Harney SC, Jane DE, Anwyl R (2008) Extrasynaptic NR2D-containing NMDARs are recruited to the synapse during LTP of NMDAR-EPSCs. J Neurosci 28:11685–11694
Harrison PJ (2004) The hippocampus in schizophrenia: a review of the neuropathological evidence and its pathophysiological implications. Psychopharmacology 174:151–162
Hashimoto T, Volk DW, Eggan SM, Mirnics K, Pierri JN, Sun Z, Sampson AR, Lewis DA (2003) Gene expression deficits in a subclass of GABA neurons in the prefrontal cortex of subjects with schizophrenia. J Neurosci 23:6315–6326
Haydon PG, Carmignoto G (2006) Astrocyte control of synaptic transmission and neurovascular coupling. Physiol Rev 86:1009–1031
Healy DJ, Haroutunian V, Powchik P, Davidson M, Davis KL, Watson SJ, Meador-Woodruff JH (1998) AMPA receptor binding and subunit mRNA expression in prefrontal cortex and striatum of elderly schizophrenics. Neuropsychopharmacology 19:278–286
Hemler ME (2003) Tetraspanin proteins mediate cellular penetration, invasion, and fusion events and define a novel type of membrane microdomain. Ann Rev Cell Dev Biol 19:397–422
Hertz L (2011) Astrocytic energy metabolism and glutamate formation-relevance for 13C-NMR spectroscopy and importance of cytosolic/mitochondrial trafficking. Magn Reson Imaging 29:1319–1329
Hertzmann M, Reba RC, Kotlyarov EV (1990) Single photon emission computed tomography in phencyclidine and related drug abuse. Am J Psychiatry 147:255–256
Hollmann M, Heinemann S (1994) Cloned glutamate receptors. Annu Rev Neurosci 17:31–108
Hollmann M, Maron C, Heinemann S (1994) N-glycosylation site tagging suggests a three transmembrane domain topology for the glutamate receptor GluR1. Neuron 13:1331–1343
Horiuchi Y et al. (2012) Association of SNPs linked to increased expression of SLC1A1 with schizophrenia. American journal of medical genetics Part B. Neuropsychiatr Genet 159B:30–37
Huang HS, Akbarian S (2007) GAD1 mRNA expression and DNA methylation in prefrontal cortex of subjects with schizophrenia. PloS ONE 2:e809
Huang YH, Bergles DE (2004) Glutamate transporters bring competition to the synapse. Curr Opin Neurobiol 14:346–352
Huang HS, Matevossian A, Whittle C, Kim SY, Schumacher A, Baker SP, Akbarian S (2007) Prefrontal dysfunction in schizophrenia involves mixed-lineage leukemia 1-regulated histone methylation at GABAergic gene promoters. J Neurosci 27:11254–11262
Hutcheson NL, Reid MA, White DM, Kraguljac NV, Avsar KB, Bolding MS, Knowlton RC, den Hollander JA, Lahti AC (2012) Multimodal analysis of the hippocampus in schizophrenia using proton magnetic resonance spectroscopy and functional magnetic resonance imaging. Schizophr Res 140:136–142
Ibrahim HM, Hogg AJ Jr, Healy DJ, Haroutunian V, Davis KL, Meador-Woodruff JH (2000) Ionotropic glutamate receptor binding and subunit mRNA expression in thalamic nuclei in schizophrenia. Am J Psychiatry 157:1811–1823
Illarionova NB, Gunnarson E, Li Y, Brismar H, Bondar A, Zelenin S, Aperia A (2010) Functional and molecular interactions between aquaporins and Na, K-ATPase. Neuroscience 168:915–925
Jackson M, Song W, Liu MY, Jin L, Dykes-Hoberg M, Lin CI, Bowers WJ, Federoff HJ, Sternweis PC, Rothstein JD (2001) Modulation of the neuronal glutamate transporter EAAT4 by two interacting proteins. Nature 410:89–93
Javitt DC, Zukin SR (1991) Recent advances in the phencyclidine model of schizophrenia. Am J Psychiatry 148:1301–1308
Joyce JN, Meador-Woodruff JH (1997) Linking the family of D2 receptors to neuronal circuits in human brain: insights into schizophrenia. Neuropsychopharmacology 16:375–384
Kalandadze A, Wu Y, Fournier K, Robinson MB (2004) Identification of motifs involved in endoplasmic reticulum retention-forward trafficking of the GLT-1 subtype of glutamate transporter. J Neurosci 24:5183–5192
Karlsson RM, Tanaka K, Heilig M, Holmes A (2008) Loss of glial glutamate and aspartate transporter (excitatory amino acid transporter 1) causes locomotor hyperactivity and exaggerated responses to psychotomimetics: rescue by haloperidol and metabotropic glutamate 2/3 agonist. Biol Psychiatry 64:810–814
Karlsson RM, Tanaka K, Saksida LM, Bussey TJ, Heilig M, Holmes A (2009) Assessment of glutamate transporter GLAST (EAAT1)-deficient mice for phenotypes relevant to the negative and executive/cognitive symptoms of schizophrenia. Neuropsychopharmacology 34:1578–1589
Kay SR (1990) Significance of the positive-negative distinction in schizophrenia. Schizophr Bull 16:635–652
Kraguljac NV, Reid MA, White DM, den Hollander J, Lahti AC (2012a) Regional decoupling of N-acetyl-aspartate and glutamate in schizophrenia. Neuropsychopharmacology 37:2635–2642
Kraguljac NV, Reid M, White D, Jones R, den Hollander J, Lowman D, Lahti AC (2012b) Neurometabolites in schizophrenia and bipolar disorder-a systematic review and meta-analysis. Psychiatry Res 203:111–125
Kristiansen LV, Meador-Woodruff JH (2005) Abnormal striatal expression of transcripts encoding NMDA interacting PSD proteins in schizophrenia, bipolar disorder and major depression. Schizophr Res 78:87–93
Kullmann DM, Asztely F (1998) Extrasynaptic glutamate spillover in the hippocampus: evidence and implications. Trends Neurosci 21:8–14
Lahti AC, Tamminga CA (1995) Recent developments in the neuropharmacology of schizophrenia. Am J Health Syst Pharm 52:S5–S8
Laruelle M, Abi-Dargham A, Gil R, Kegeles L, Innis R (1999) Increased dopamine transmission in schizophrenia: relationship to illness phases. Biol Psychiatry 46:56–72
Laruelle M, Slifstein M, Huang Y (2003) Relationships between radiotracer properties and image quality in molecular imaging of the brain with positron emission tomography. Mol Imag Biol 5:363–375
Lauriat TL, Dracheva S, Chin B, Schmeidler J, McInnes LA, Haroutunian V (2006) Quantitative analysis of glutamate transporter mRNA expression in prefrontal and primary visual cortex in normal and schizophrenic brain. Neuroscience 137:843–851
Lehre KP, Danbolt NC (1998) The number of glutamate transporter subtype molecules at glutamatergic synapses: chemical and stereological quantification in young adult rat brain. J Neurosci 18:8751–8757
Leveille F, El Gaamouch F, Gouix E, Lecocq M, Lobner D, Nicole O, Buisson A (2008) Neuronal viability is controlled by a functional relation between synaptic and extrasynaptic NMDA receptors. FASEB J 22:4258–4271
Levy LM, Warr O, Attwell D (1998) Stoichiometry of the glial glutamate transporter GLT-1 expressed inducibly in a Chinese hamster ovary cell line selected for low endogenous Na+-dependent glutamate uptake. J Neurosci 18:9620–9628
Lewis DA, Gonzalez-Burgos G (2008) Neuroplasticity of neocortical circuits in schizophrenia. Neuropsychopharmacology 33:141–165
Lewis DA, Levitt P (2002) Schizophrenia as a disorder of neurodevelopment. Annu Rev Neurosci 25:409–432
Lewis DA, Cruz DA, Melchitzky DS, Pierri JN (2001) Lamina-specific deficits in parvalbumin-immunoreactive varicosities in the prefrontal cortex of subjects with schizophrenia: evidence for fewer projections from the thalamus. Am J Psychiatry 158:1411–1422
Lewis DA, Glantz LA, Pierri JN, Sweet RA (2003) Altered cortical glutamate neurotransmission in schizophrenia: evidence from morphological studies of pyramidal neurons. Ann N Y Acad Sci 1003:102–112
Lewis DA, Volk DW, Hashimoto T (2004) Selective alterations in prefrontal cortical GABA neurotransmission in schizophrenia: a novel target for the treatment of working memory dysfunction. Psychopharmacology 174:143–150
Lewis DA, Hashimoto T, Morris HM (2008) Cell and receptor type-specific alterations in markers of GABA neurotransmission in the prefrontal cortex of subjects with schizophrenia. Neurotox Res 14:237–248
Lin SH, Maiese K (2001) The metabotropic glutamate receptor system protects against ischemic free radical programmed cell death in rat brain endothelial cells. J Cereb Blood Flow Metab 21:262–275
Lozovaya N, Melnik S, Tsintsadze T, Grebenyuk S, Kirichok Y, Krishtal O (2004a) Protective cap over CA1 synapses: extrasynaptic glutamate does not reach the postsynaptic density. Brain Res 1011:195–205
Lozovaya NA, Grebenyuk SE, Tsintsadze T, Feng B, Monaghan DT, Krishtal OA (2004b) Extrasynaptic NR2B and NR2D subunits of NMDA receptors shape ‘superslow’ afterburst EPSC in rat hippocampus. J Physiol 558:451–463
Malarkey EB, Parpura V (2008) Mechanisms of glutamate release from astrocytes. Neurochem Int 52:142–154
Malenka RC, Nicoll RA (1999) Long-term potentiation-a decade of progress? Science 285:1870–1874
Marcaggi P, Attwell D (2007) Short- and long-term depression of rat cerebellar parallel fibre synaptic transmission mediated by synaptic crosstalk. J Physiol 578:545–550
Marenco S, Weinberger DR (2000) The neurodevelopmental hypothesis of schizophrenia: following a trail of evidence from cradle to grave. Dev Psychopathol 12:501–527
Marie H, Billups D, Bedford FK, Dumoulin A, Goyal RK, Longmore GD, Moss SJ, Attwell D (2002) The amino terminus of the glial glutamate transporter GLT-1 interacts with the LIM protein Ajuba. Mol Cell Neurosci 19:152–164
Marsman A, van den Heuvel MP, Klomp DW, Kahn RS, Luijten PR, Hulshoff Pol HE (2011) Glutamate in schizophrenia: a focused review and meta-analysis of 1H-MRS studies. Schizophr Bull 39:120–129
Massie A, Cnops L, Smolders I, McCullumsmith R, Kooijman R, Kwak S, Arckens L, Michotte Y (2008) High-affinity Na+/K+-dependent glutamate transporter EAAT4 is expressed throughout the rat fore- and midbrain. J Com Neurol 511:155–172
Masson J, Sagne C, Hamon M, El Mestikawy S (1999a) Neurotransmitter transporters in the central nervous system. Pharmacol Rev 51:439–464
Masson J, Cervera P, Cote S, Morisette J, Aidouni Z, Giros B, Hamon M, Falardeau P, Mestikawy SE (1999b) Characterization and distribution of Hxt1, a Na(+)/Cl(-)-dependent orphan transporter, in the human brain. J Neurosci Res 56:146–159
Matute C, Melone M, Vallejo-Illarramendi A, Conti F (2005) Increased expression of the astrocytic glutamate transporter GLT-1 in the prefrontal cortex of schizophrenics. Glia 49:451–455
McCullumsmith RE, Meador-Woodruff JH (2002) Striatal excitatory amino acid transporter transcript expression in schizophrenia, bipolar disorder, and major depressive disorder. Neuropsychopharmacology 26:368–375
McCullumsmith RE, Meador-Woodruff JH (2011) Novel approaches to the study of postmortem brain in psychiatric illness: old limitations and new challenges. Biol Psychiatry 69:127–133
McCullumsmith R, Clinton S, Meador-Woodruff J (2004a) Schizophrenia as a disorder of neuroplasticity. Int Rev Neurobiol 59:19–45
McCullumsmith RE, Clinton SM, Meador-Woodruff JH (2004b) Schizophrenia as a disorder of neuroplasticity. Int Rev Neurobiol 59:19–45
McCullumsmith RE, Hammond J, Funk A, Meador-Woodruff JH (2012) Recent advances in targeting the Ionotropic glutamate receptors in treating schizophrenia. Curr Pharm Biotechnol 13:1535–1542
McKenna MC (2011) Glutamate dehydrogenase in brain mitochondria: do lipid modifications and transient metabolon formation influence enzyme activity? Neurochem Int 59:525–533
Meador-Woodruff JH, Hogg AJ Jr, Smith RE (2001a) Striatal ionotropic glutamate receptor expression in schizophrenia, bipolar disorder, and major depressive disorder. Brain Res Bull 55:631–640
Meador-Woodruff JH, Davis KL, Haroutunian V (2001b) Abnormal kainate receptor expression in prefrontal cortex in schizophrenia. Neuropsychopharmacology 24:545–552
Montana V, Ni Y, Sunjara V, Hua X, Parpura V (2004) Vesicular glutamate transporter-dependent glutamate release from astrocytes. J Neurosci 24:2633–2642
Nakagawa T, Otsubo Y, Yatani Y, Shirakawa H, Kaneko S (2008) Mechanisms of substrate transport-induced clustering of a glial glutamate transporter GLT-1 in astroglial-neuronal cultures. Eur J Neurosci 28:1719–1730
Newpher TM, Ehlers MD (2009) Spine microdomains for postsynaptic signaling and plasticity. Trends Cell Biol 19:218–227
Nudmamud-Thanoi S, Piyabhan P, Harte MK, Cahir M, Reynolds GP (2007) Deficits of neuronal glutamatergic markers in the caudate nucleus in schizophrenia. J Neural Transm Suppl 2007:281–285
Ohnuma T, Augood SJ, Arai H, McKenna PJ, Emson PC (1998) Expression of the human excitatory amino acid transporter 2 and metabotropic glutamate receptors 3 and 5 in the prefrontal cortex from normal individuals and patients with schizophrenia. Brain Res Mol Brain Res 56:207–217
Ohnuma T, Tessler S, Arai H, Faull RL, McKenna PJ, Emson PC (2000) Gene expression of metabotropic glutamate receptor 5 and excitatory amino acid transporter 2 in the schizophrenic hippocampus. Brain Res Mol Brain Res 85:24–31
Patel DR, Young AM, Croucher MJ (2001) Presynaptic alpha-amino-3-hydroxy-5-methyl-4-isoxazole propionate receptor-mediated stimulation of glutamate and GABA release in the rat striatum in vivo: a dual-label microdialysis study. Neuroscience 102:101–111
Patil ST, Zhang L, Martenyi F, Lowe SL, Jackson KA, Andreev BV, Avedisova AS, Bardenstein LM, Gurovich IY, Morozova MA, Mosolov SN, Neznanov NG, Reznik AM, Smulevich AB, Tochilov VA, Johnson BG, Monn JA, Schoepp DD (2007) Activation of mGlu2/3 receptors as a new approach to treat schizophrenia: a randomized phase 2 clinical trial. Nat Med 13:1102–1107
Potkin SG, Turner JA, Brown GG, McCarthy G, Greve DN, Glover GH, Manoach DS, Belger A, Diaz M, Wible CG, Ford JM, Mathalon DH, Gollub R, Lauriello J, O’Leary D, van Erp TG, Toga AW, Preda A, Lim KO, Fbirn (2009) Working memory and DLPFC inefficiency in schizophrenia: the FBIRN study. Schizophr Bull 35:19–31
Rajji TK, Mulsant BH (2008) Nature and course of cognitive function in late-life schizophrenia: a systematic review. Schizophr Res 102:122–140
Rajkowska G, Selemon LD, Goldman-Rakic PS (1998) Neuronal and glial somal size in the prefrontal cortex: a postmortem morphometric study of schizophrenia and Huntington disease. Arch Gen Psychiatry 55:215–224
Rajkowska G, Miguel-Hidalgo JJ, Makkos Z, Meltzer H, Overholser J, Stockmeier C (2002) Layer-specific reductions in GFAP-reactive astroglia in the dorsolateral prefrontal cortex in schizophrenia. Schizophr Res 57:127–138
Rao JS, Kellom M, Reese EA, Rapoport SI, Kim HW (2012) Dysregulated glutamate and dopamine transporters in postmortem frontal cortex from bipolar and schizophrenic patients. J Affect Disord 136:63–71
Regan MR, Huang YH, Kim YS, Dykes-Hoberg MI, Jin L, Watkins AM, Bergles DE, Rothstein JD (2007) Variations in promoter activity reveal a differential expression and physiology of glutamate transporters by glia in the developing and mature CNS. J Neurosci 27:6607–6619
Regenold WT, Pratt M, Nekkalapu S, Shapiro PS, Kristian T, Fiskum G (2012) Mitochondrial detachment of hexokinase 1 in mood and psychotic disorders: implications for brain energy metabolism and neurotrophic signaling. J Psychiatr Res 46:95–104
Rusakov DA, Kullmann DM (1998) Extrasynaptic glutamate diffusion in the hippocampus: ultrastructural constraints, uptake, and receptor activation. J Neurosci 18:3158–3170
Salt TE, Eaton SA, Turner JP (1996) Characterization of the metabotropic glutamate receptors (mGluRs) which modulate GABA-mediated inhibition in the ventrobasal thalamus. Neurochem Int 29:317–322
Schluter K, Figiel M, Rozyczka J, Engele J (2002) CNS region-specific regulation of glial glutamate transporter expression. Eur J Neurosci 16:836–842
Schoepp DD (2001) Unveiling the functions of presynaptic metabotropic glutamate receptors in the central nervous system. J Pharmacol Exp Ther 299:12–20
Selemon LD, Rajkowska G, Goldman-Rakic PS (1995) Abnormally high neuronal density in the schizophrenic cortex. A morphometric analysis of prefrontal area 9 and occipital area 17. Arch Gen Psychiatry 52:805–818 (discussion 819–820)
Sem’yanov AV (2005) Diffusional extrasynaptic neurotransmission via glutamate and GABA. Neurosci Behav Physiol 35:253–266
Shan D, Haroutunian V, Meador-Woodruff JH, McCullumsmith RE (2012) Expression of equilibrative nucleoside transporter type 1 protein in elderly patients with schizophrenia. Neuroreport 23:224–227
Shan D, Lucas EK, Drummond JB, Haroutunian V, Meador-Woodruff JH, McCullumsmith RE (2013) Abnormal expression of glutamate transporters in temporal lobe areas in elderly patients with schizophrenia. Schizophr Res 144:1–8
Skytt DM, Klawonn AM, Stridh MH, Pajecka K, Patruss Y, Quintana-Cabrera R, Bolanos JP, Schousboe A, Waagepetersen HS (2012) siRNA knock down of glutamate dehydrogenase in astrocytes affects glutamate metabolism leading to extensive accumulation of the neuroactive amino acids glutamate and aspartate. Neurochem Int 61:490–497
Smith RE, Haroutunian V, Davis KL, Meador-Woodruff JH (2001) Expression of excitatory amino acid transporter transcripts in the thalamus of subjects with schizophrenia. Am J Psychiatry 158:1393–1399
Somerville SM, Lahti AC, Conley RR, Roberts RC (2011) Mitochondria in the striatum of subjects with schizophrenia: relationship to treatment response. Synapse 65:215–224
Somerville SM, Conley RR, Roberts RC (2012) Striatal mitochondria in subjects with chronic undifferentiated vs. chronic paranoid schizophrenia. Synapse 66:29–41
Spat A, Fulop L, Koncz P, Szanda G (2009) When is high-Ca+ microdomain required for mitochondrial Ca+ uptake? Acta physiologica 195:139–147
Stobart JL, Anderson CM (2013) Multifunctional role of astrocytes as gatekeepers of neuronal energy supply. Front Cell Neurosci 7:38
Szabadkai G, Rizzuto R (2007) Chaperones as parts of organelle networks. Adv Exp Med Biol 594:64–77
Szoke A, Meary A, Trandafir A, Bellivier F, Roy I, Schurhoff F, Leboyer M (2008) Executive deficits in psychotic and bipolar disorders-implications for our understanding of schizoaffective disorder. Eur Psychiatry 23:20–25
Takamori S, Riedel D, Jahn R (2000) Immunoisolation of GABA-specific synaptic vesicles defines a functionally distinct subset of synaptic vesicles. J Neurosci 20:4904–4911
Talbot K, Ong WY, Blake DJ, Tang J, Louneva N, Carlson GC, Arnold SE (2009) Dysbindin-1 and its protein family. In: Lajtha A, Javitt D, Kantrowitz J (eds) Handbook of neurochemistry and molecular neurobiology. Springer, New York, pp 107–241
Tamminga C (1999) Glutamatergic aspects of schizophrenia. Br J Psychiatry Suppl 1999:12–15
Theberge J, Bartha R, Drost DJ, Menon RS, Malla A, Takhar J, Neufeld RW, Rogers J, Pavlosky W, Schaefer B, Densmore M, Al-Semaan Y, Williamson PC (2002) Glutamate and glutamine measured with 4.0 T proton MRS in never-treated patients with schizophrenia and healthy volunteers. Am J Psychiatry 159:1944–1946
Tong G, Jahr CE (1994) Block of glutamate transporters potentiates postsynaptic excitation. Neuron 13:1195–1203
Tsai G, Coyle J (2002) Glutamatergic mechanisms in schizophrenia. Annu Rev Pharmacol Toxicol 42:165–179
Tsvetkov E, Shin RM, Bolshakov VY (2004) Glutamate uptake determines pathway specificity of long-term potentiation in the neural circuitry of fear conditioning. Neuron 41:139–151
Tzingounis AV, Wadiche JI (2007) Glutamate transporters: confining runaway excitation by shaping synaptic transmission. Nat Rev Neurosci 8:935–947
Uranova N, Orlovskaya D, Vikhreva O, Zimina I, Kolomeets N, Vostrikov V, Rachmanova V (2001) Electron microscopy of oligodendroglia in severe mental illness. Brain Res Bull 55:597–610
Utsunomiya-Tate N, Endou H, Kanai Y (1996) Cloning and functional characterization of a system ASC-like Na+-dependent neutral amino acid transporter. J Biol Chem 271:14883–14890
Volk DW, Eggan SM, Lewis DA (2010) Alterations in metabotropic glutamate receptor 1alpha and regulator of G protein signaling 4 in the prefrontal cortex in schizophrenia. Am J Psychiatry 167:1489–1498
Watanabe C, Sakurada T, Okuda K, Sakurada C, Ando R, Sakurada S (2003) The role of spinal nitric oxide and glutamate in nociceptive behaviour evoked by high-dose intrathecal morphine in rats. Pain 106:269–283
Watase K, Hashimoto K, Kano M, Yamada K, Watanabe M, Inoue Y, Okuyama S, Sakagawa T, Ogawa S, Kawashima N, Hori S, Takimoto M, Wada K, Tanaka K (1998) Motor discoordination and increased susceptibility to cerebellar injury in GLAST mutant mice. Eur J Neurosci 10:976–988
Weng HR, Chen JH, Pan ZZ, Nie H (2007) Glial glutamate transporter 1 regulates the spatial and temporal coding of glutamatergic synaptic transmission in spinal lamina II neurons. Neurosci 149:898–907
Wobrock T, Schneider M, Kadovic D, Schneider-Axmann T, Ecker UK, Retz W, Rosler M, Falkai P (2008) Reduced cortical inhibition in first-episode schizophrenia. Schizophr Res 105:252–261
Zanello A, Curtis L, Badan Ba M, Merlo MC (2009) Working memory impairments in first-episode psychosis and chronic schizophrenia. Psychiatry Res 165:10–18
Zerangue N, Kavanaugh MP (1996) Flux coupling in a neuronal glutamate transporter. Nature 383:634–637
Acknowledgements
We thank the Alabama Brain Collection for providing postmortem brain tissue. This work was supported by MH074016, MH094445 and Doris Duke Clinical Scientist Award (REM).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
McCullumsmith, R., Shan, D., Yates, S., Roberts, R. (2014). Astroglia and Severe Mental Illness: A Role for Glutamate Microdomains. In: Parpura, V., Verkhratsky, A. (eds) Pathological Potential of Neuroglia. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0974-2_16
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0974-2_16
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0973-5
Online ISBN: 978-1-4939-0974-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)