
Abstract
Two men working in the same factory report the onset of back pain after the same type of incident—lifting a heavy object at the end of a long work day. One man, Mr. A, misses 2 days of work and then returns although, for the first few days back at work, he avoids the heavier tasks. Mr. Z, destined never to return to work, experiences increasing pain and limitations in his ability to function. He undergoes ever-more expensive and invasive treatments until, perhaps inevitably, he ends up having spine surgery. Even so, his pain does not remit. Eventually, he loses his job, his motivation and his self-esteem. He is declared to have failed back surgery syndrome (FBSS), and another surgery is proposed. He goes on to become, essentially, a ward of the State, on Social Security Disability, with almost no hope of resuming productive activity.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Two men working in the same factory report the onset of back pain after the same type of incident—lifting a heavy object at the end of a long work day. One man, Mr. A, misses 2 days of work and then returns although, for the first few days back at work, he avoids the heavier tasks. Mr. Z, destined never to return to work, experiences increasing pain and limitations in his ability to function. He undergoes ever-more expensive and invasive treatments until, perhaps inevitably, he ends up having spine surgery. Even so, his pain does not remit. Eventually, he loses his job, his motivation and his self-esteem. He is declared to have failed back surgery syndrome (FBSS), and another surgery is proposed. He goes on to become, essentially, a ward of the State, on Social Security Disability, with almost no hope of resuming productive activity.
Are there signs that could have foretold the divergent course of these two men? What treatment options exist for those with spine injuries? Could something have been done to forestall the downward spiral of Mr. Z? In the present chapter, we explore the answers to these questions. First, we present data on the incidence rates of, and costs associated with, back injuries in general, emphasizing industrial injuries specifically. Next, we review physical causes of back pain. Psychosocial influences on the experience and course of back pain are subsequently reviewed. We then discuss the range of treatment options available for back pain. Finally, we discuss how multidisciplinary approaches to the assessment and treatment of back injuries can provide for cost-effective intervention, maximizing the opportunities for treatment success while reducing the likelihood of failure.
Epidemiology of Back Pain
Back pain is a nearly ubiquitous problem. Generally, research shows that 70–85 % of all individuals in the United States experience back pain at some point in their lives (Andersson, 1999). Several studies have shown that, each year, approximately 25–27 % of all US residents experience an episode of back pain (Deyo, Mirza, & Martin, 2006; Pleis & Lethbridge-Cejku, 2007). According to the Agency for Healthcare Research and Quality, about 70 % of these individuals seek medical treatment, so that, as reported by Katz (2006), there are 19 million office visits each year for low back pain (for a total cost of $3 billion in office visits alone). This represents 2 % of all office visits, exceeded only in quantity by routine examinations, hypertension and diabetes (Martin et al., 2008). Thus, the costs associated with back pain are tremendous. The total incremental costs for healthcare associated with spine pain were estimated in 2005 to be $85.9 billion, with only heart disease and stroke responsible for greater cost (Martin et al., 2008). These costs have been rising rapidly, as the total cost of spine pain treatment in 1997 was only about $26.3 billion. If one includes the indirect costs of back pain, including lost wages, the economic impact rises as high as $200 billion per year (Katz, 2006).
Given the overall incidence of back pain, it should not be surprising that occupational spine injuries are frequent and expensive and may have problematic outcomes. Five percent of all American workers miss at least 1 day annually due to low back pain, and the most common occupational injury in most States is to the spine. For example, 2011 data on occupational injuries in the State of Washington reveal a far greater number of claims for back injury (14,112) than for any other body part, with the next most common being finger injuries (11,679 claims). In the same year, the total incurred costs for back injury in Washington ($114,379,462) far exceeded the costs for the next most costly injury—multiple body parts ($92,034,875). In 2001, it was estimated that, nationally, annual workers’ compensation expenditures on treatment for low back pain was approximately $20 billion (National Research Council and Institute of Medicine, 2001). Fortunately, job-related back injuries mostly resolve quickly and with minimal treatment—80 % of those injured on the job return to work within 1 month, and greater than 90 % return in 3 months. However, for a small percentage of patients, the pain becomes protracted, leading to extended disability and tremendous medical costs, as only 5 % of those with back injuries are responsible for the 75 % of the total costs of work-related low back pain (Frank et al., 1996).
Structure of the Spine
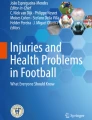
An understanding of the causes and treatment options for occupational back pain is informed by an overview of the spine itself. The spinal column typically consists of 33 vertebrae: 7 cervical, 12 thoracic, and 5 lumbar vertebrae compose the mobile portion of the spine, with an additional 5 segments fused to form the sacrum, and 4 joined bones which compose the coccyx, or tailbone. The spinal column anatomy must be flexible enough to allow for effective motion of the trunk and yet rigid enough to serve as a protective structure for the spinal cord and nerve roots contained within its center. In general, an individual vertebra consists of an anterior (ventral) mass of predominantly cancellous bone (referred to as the vertebral body) and a posterior (dorsal) vertebral arch consisting mainly of denser cortical bone. The vertebral arch is the confluence of paired pedicles, laminae and a central spinous process from each level. The space between the dorsal arch and ventral body is the spinal canal, within which the spinal cord and spinal nerves are enclosed (Figs. 2.1, 2.2, and 2.3).

Lateral view of entire spinal column

Lateral view of a spinal segment, consisting of two vertebrae and an intervertebral disc

Axial view of a lumbar vertebra, showing spinal nerves within the thecal sac
Each vertebral body in the cervical, thoracic and lumbar spine is effectively “linked” to the bodies above and below through intervertebral discs anteriorly, through paired facet joints posteriorly, and through numerous ligamentous attachments. The facet joints are diarthrodial (i.e., freely mobile) synovial joints formed from a more ventrally-located superior articular process originating from the inferior vertebral level and a dorsally located inferior articular process originating from the superior vertebral level. At the level of the sacrum, although there is no mobility between the individual segments, there is the sacroiliac joint (SI joint), which functions to transmit loads from the trunk to the lower extremities. The SI joint is also a diarthrodial synovial joint, with stability imparted to it through a number of extremely strong ligamentous attachments.
Major Physical Sources of LBP
There are a number of potential anatomic sources of low back pain. The paraspinal musculature, intervertebral disc, facet joints, vertebral bodies and SI joints are the most common structures cited as “pain generators” in the spine. In many cases, more than one of these structures is ultimately responsible for the overall clinical presentation. Fortunately, the astute clinician is often able to determine the dominant source(s) of pain in a given patient and direct appropriate treatment.
Paraspinal Musculature
Low back pain resulting primarily from the paraspinal musculature is referred to as a myofascial pain syndrome. Spasm and overcontraction of injured muscles are the root cause for this syndrome, which was originally described by Simons, Travell, and Simons (1999) as a condition characterized by muscles that are shortened or contracted, with increased tone and stiffness, and that contain numerous trigger points (tender, firm nodules identified with muscular palpation). Usually there is an aggravating factor or history of direct or indirect trauma, but triggers can also include postural dysfunction and physical deconditioning (Panjabi, 2006).
Facet Joint Pain
The facet joints are paired diarthrodial synovial joints between the posterior elements of adjacent vertebrae, and have been implicated as a source of chronic low back pain since the early 1900s. The term facet syndrome was first coined by Ghormley (1933) when he described lumbosacral pain that often occurred after a twisting injury to the lumbar spine and that was accompanied by local paraspinal muscular tenderness, exacerbation of symptoms with hyperextension, and radiation of pain into the hips and buttocks without neurologic deficits. The innervation to the lumbar facet joints is derived from medial branches of the dorsal rami of the spinal nerves. With trauma to the joints, inflammation leading to pain, stiffness and secondary muscle spasm occurs. There is also an important correlation between degenerative changes and aging of the intervertebral disc and resultant increased transfer of stress to the facet joints, subsequently leading to accelerated degenerative changes there as well.
Intervertebral Disc
The outer annulus fibrosis of the intervertebral disc is innervated by the sinuvertebral nerves, first described by Luschka (1850). These nerves are derived primarily from the spinal nerves, with additional contributions from the sympathetic plexus. Only the outer third of the annulus is innervated; the inner two-thirds of the annulus and the nucleus pulposus are devoid of any nerve fibers. Thus, for the disc itself to be a pain generator, the presumption is that the outer third of the annulus must be exposed to a painful stimulus. Over time, as the disc succumbs to the physiology of aging, dehydration can result in annular tears or fissures (Vernon-Roberts & Pirie, 1977).
The disc can also play a role in back pain in the setting of an acute herniation. In this case, compression of an exiting nerve root or the collection of nerve roots contained within the dura from bulging disc material will result in lower extremity radicular pain—the classic sciatica. A large central disc herniation can present with predominantly low back pain in the setting of minimal or no lower extremity symptoms.
Vertebral Body
The vertebral body itself can be a source of low back pain in the setting of trauma, infection, or tumor. Compression fractures can be a source of significant acute and chronic back pain after trauma, especially in the elderly population where osteopenia (defined by WHO as a T-score on a bone density study of −1.0 to −2.5) or osteoporosis (defined by WHO as a T-score on bone density study below −2.5) is a predisposing factor for fracture even with minimal trauma (i.e., a fall from standing height). In the case of infection, osteomyelitis can cause bony destruction, leading to pain. Primary or metastatic spinal tumors can also lead to bony destruction and pain. A patient history of unintentional weight loss, fevers, chills or severe unremitting pain (i.e., the so-called red flags) should alert the physician to consider these possible differential diagnoses.
Sacroiliac Joint
The SI joint is an often unrecognized source of pain in many patients. It can be injured with minimal trauma in the setting of a combined axial loading and abrupt rotational force, such as in falls, motor vehicle accidents and athletic injuries (Chou et al., 2004). Despite the existence of numerous physical examination tests to help evaluate for SI joint dysfunction, history and exam findings alone are not consistently reliable in making the diagnosis (Dreyfuss, Michaelsen, Pauza, McLarty, & Bogduk, 1996; Slipman, Sterenfeld, Chou, Herzog, & Vresilovic, 1998). If clinical suspicion is strongly in favor of SI joint pain, a diagnostic block with an appropriate response during the anesthetic phase of the injection can help in supporting the diagnosis.
Psychosocial Influences on Back Pain
The experience of back pain can be traumatic, protracted, and life altering—or it can be merely an adversity which one learns to control or manage. Obviously, the physical basis of the pain is one of the factors that determines the impact of the pain. Patients whose back pain is sufficiently intense that surgery is considered based on an identifiable physical cause will, on average, experience pain for a greater duration and undergo more intense treatment than the 54 % of patients for whom no cause can be specified (Martin et al., 2008). However, regardless of its cause, the course of back pain can be strongly influenced by emotional and personality factors, which we now briefly review.
Depression
Back pain and depression are intimately linked—several general population studies have shown their relationship. Currie and Wang (2004), for example, analyzed data from the Canadian Community Health Survey to explore the relationship of depression (as assessed by a structured diagnostic interview) to back pain in over 110,000 household residents. Overall, 9 % of those interviewed experienced back pain, but the incidence rate of depression in those with back pain was 19.8 %, whereas depression was experienced by only 5.9 % of those with no back pain (see also Gureje et al., 2008). Among patients with chronic low back pain, lifetime rates of depression are much higher, ranging from 45 to 65 % (Polatin, Kinney, Gatchel, Lillo, & Mayer, 1993). The direction of causation between depression and back pain is uncertain. Clearly, the onset of pain can lead to many adverse consequences—loss of income, decreased function, loss of enjoyment, etc.—all of which may lead to the onset of depression. In fact, a number of cross-sectional and prospective studies have shown that emotional distress worsens as back pain becomes more protracted. However, several studies have found that individuals who are depressed are more likely to develop chronic pain (see Fishbain, Cutler, Rosomoff, & Rosomoff, 1997, for a review). Many of the symptoms of major depression and chronic pain overlap, including sleep disturbance, loss of enjoyment, social withdrawal, memory and concentration difficulties. Thus, while depression may place individuals at risk for the development of chronic low back pain, it is certainly the case that pain can create or exacerbate depression, leading to a quite recalcitrant chronic pain syndrome.
Anxiety and Fear
The experience of back pain, especially if it is protracted, is one that almost inevitably produces anxiety. Worries about the basis of the pain, ability to work and function, dependence on narcotics, worsening of the pain, and concerns about the possibility of spine surgery, are common and intense. In fact, data from Gureje et al. (2008), who analyzed results from the World Mental Health Survey, found that community members in the United States who reported pain in multiple body areas were at greatly increased risk of having diagnosable anxiety disorders (generalized anxiety, panic disorder, social phobia or post-traumatic stress disorder), compared to respondents who did not report any pain. In a similar vein, McWilliams, Goodwin, and Cox (2004), analyzing data from the Midlife Development in the United States Survey (MIDUS), found that, compared to those without back pain, individuals with back pain were at risk for diagnosable panic attacks (odds ratio 2.69) and generalized anxiety disorder (odds ratio 2.54). Again, the question of whether the anxiety precedes or results from the back pain remains an open one. However, what is clear is that patients who experience significant anxiety do not respond as well to treatments for back pain as those who are less anxious.
Pain Sensitivity
Back pain cannot be measured directly. It can only be assessed through the patient’s self-report of the pain experienced, as well as changes in functional ability and usage of pain medication. Even when an underlying physiological cause of the pain can be identified, it is difficult to tell whether an individual’s experience of pain is appropriate. The concept of pain sensitivity revolves around whether the patient experiences pain of an intensity, and in a physical distribution, consistent with an identified cause. To the extent that inconsistency is found, the patient can be deemed as excessively pain sensitive.
Pain sensitivity can be assessed in several ways. The most widely researched of these utilizes the MMPI and MMPI-2, in which Scales 1 and 3, reflecting somatic preoccupation, are frequently found to be elevated in patients with chronic back pain (Keller & Butcher, 1991). Classic research by Bigos et al. (1991), who prospectively studied over 3,000 aircraft employees, demonstrated that elevations on MMPI Scale 3 were strongly associated (along with low levels of vocational satisfaction) with the development of back pain over a 4-year period. Recent research by Block, Ben-Porath, and Marek (2013), using a newer version of the MMPI, the MMPI-2-RF (Ben-Porath & Tellegen, 2008), found that patients who are candidates for spine surgery have elevations on Scale Rc1 (somatic complaints), relative to the general population, and that elevations on Rc1 are associated with reduced outcome of spine surgery (Block, Ben-Porath, Ohnmeiss, Guyer, & Marek, 2012).
Pain sensitivity that is more specific to back pain can be assessed by providing the patient with a body outline and having the patient shade in areas where pain is experienced. To the extent that such “pain drawings” are not consistent with the underlying physical pathology, the patient can be seen to be excessively pain sensitive. Such inconsistent pain drawings are associated with elevations on MMPI Scales 1 and 3 (Dennis, Rocchio, & Wiltse, 1981) and are associated with reduced effectiveness of conservative treatment for back pain (Takata & Hirotani, 1995) as well as spine surgery (Block, Ohnmeiss, Guyer, Rashbaum, & Hochschuler, 2001).
Anger
Of the panoply of negative emotions experienced by back pain patients, perhaps the most significant one is anger. Fernandez, Clark, and Ruddick-Davis (1999) asked chronic pain patients to rate the frequency with which they had experienced six emotions during the previous 30 days. Although guilt, shame, fear, sadness, shame, and envy were all commonly experienced, anger was the most frequently reported—about 70 % of the time. Several intriguing studies have shown that anger may actually increase pain awareness through physiological mechanisms. In one study, chronic back pain patients and non-pain control subjects were asked to recall experiences of both anger and sadness while activity of the lumbar paraspinal muscles was monitored (Burns, 2006). While both the pain patients and controls had elevations in paraspinal muscle tension in both emotional recall conditions, the pain patients (but not the controls) showed greater muscle tension elevations in the anger recall condition than in the sadness recall condition. The author concluded that excessive lumbar paraspinal reactivity may increase pain awareness in chronic low back pain patients. In a separate study, Bruehl, Chung, Burns, and Diedrich (2007) found that a particular type of anger, in which patients tend to directly express anger rather than suppress it (termed “anger out”), is associated with dysfunction in endogenous opioid release during painful conditions, leading individuals with “anger out” traits to experience heightened pain sensations.
The results reported above indicate that anger appears to be the most commonly experienced emotion associated with chronic back pain, and also may increase the pain experience through association with heightened physiological responses to pain. Fernandez and Turk (1995) suggested another way in which anger may adversely affect the course of chronic low back pain. They posit that anger may lead to maladaptive lifestyle changes, such as excessive use of drugs or alcohol, poor health habits, and lack of physical exercise, all of which may compound the adverse impact of back pain. Furthermore, if the patient is angry at a particular person or event, such anger may drive the patient to continue experiencing pain as a means of vindication. Such a notion receives support from recent research showing that those chronic back pain patients, who report an inability to forgive others, experience higher pain and psychological distress than do patients who are more forgiving, and that this appears to be mediated by relatively higher levels of state anger (Carlson et al., 2005).
Physical and Sexual Abuse
Chronic back pain patients often have been the victims of abuse or abandonment as either adults or as children. In one study, more than half of the patients evaluated at a multidisciplinary pain clinic reported a history of at least one form of such abuse, with 90 % of the cases the abuse occurring during adulthood (Haber & Roos, 1985; see also Green, Flowe-Valencia, Rosenblum, & Tait, 1999). A number of other studies have shown that early experiences of abuse or abandonment may leave individuals particularly prone to the development of pain disorders, as well as general health problems. For example, Linton (1997) surveyed a sample of the general population in Sweden, as well as chronic pain patients, about their histories of physical and sexual abuse. All subjects, whether patients or not, were also questioned about any chronic pain symptoms they might have had. Analyses of the results revealed that the chances of women developing chronic pain were increased fivefold by physical abuse and fourfold by sexual abuse. In this study, there appeared to be little association of abuse with pain for the men. A different community-based study (Walsh, Jamieson, MacMillian, & Boyle, 2007) found that physical abuse, but not sexual abuse, predisposed woman toward chronic pain (see Davis, Luecken, & Zaruta, 2005, for a review). More generally, childhood physical abuse, parental instability and sexual abuse have been linked with poorer adult health outcomes (Irish, Kobayashi, & Delhanty, 2010) and with significantly increased likelihood of early disability retirement (Harkonmaki et al., 2008).
Opioid Medication Abuse/Misuse
Opioid medication abuse is an increasingly problematic issue in the United States. The National Survey on Drug Use and Health (NSDUH, 2007) found that among individuals over the age of 12, 4.8 % had used a prescription pain reliever nonmedically in the previous 12 months. Despite such obvious indications that pain medications are frequently diverted for recreational purposes, they are still widely prescribed for individuals with low back pain. For example, Nyiendo, Haas, Goldberg, and Lloyd (2001) found that 31 % of patients with chronic non-malignant back pain who were referred to multispecialty clinics in Oregon were prescribed with opioid medications. Even more dramatically, Mahowald, Singh, and Majeski (2005) found a 61 % prescription rate among patients in a specialty spine clinic. These medications are frequently not used as prescribed, as exemplified by research conducted by Wunsch, Cropsey, Campbell, and Nicely (2008), who found that 61 % of chronic pain patients met the criteria for opioid abuse.
The use of narcotic medications in chronic back pain is controversial, with many expressing the view that chronic opioid therapy can be effective and cannot lead to abuse or addiction (c.f., Rosenblum, Marsch, Portenoy, & Jospeh, 2008). However, it appears that even when taken as prescribed, chronic opioid therapy is associated with poorer outcomes of both conservative treatment for spine pain (Dersh et al., 2008) and spine surgery. For example, Lawrence, London, Bohlman, and Chin (2008) found that 50 % of patients had been using narcotics on a daily basis for greater than 6 months prior to spine surgery, and such patients were much less likely to achieve excellent or good surgical results, compared to the patients who had not been on such a long-term opioid regimen. There is also evidence that opioid medications are not effective for relief of back pain nor are associated with improved functioning when prescribed for longer than 16 weeks (Martell et al., 2007). To the extent that back pain patients use opioids excessively, in a manner not prescribed, or for protracted periods, they are less likely to be responsive to any treatment.
Workers’ Compensation
In the setting of an occupational injury, it is critical to be aware of the large body of research demonstrating that back pain patients covered by workers’ compensation fare more poorly than do those who are covered by other insurance types. Workers’ compensation patients report more severe pain, greater disability, more emotional distress and greater life interference than non-compensation patients (Turk & Okifuji, 1996). A number of studies have shown that spine surgery outcome is reduced in patients receiving workers’ compensation payment (e.g., Atlas et al., 2009; Klekamp, McCarty, & Spengler, 1998). In fact, a meta-analysis by Harris, Mulford, Solomon, van Gelder, and Young (2005) found that workers’ compensation significantly increases the odds ratio for worse outcome of lumbar spinal fusion (odds = 4.33) and lumbar spinal discectomy (odds = 4.77).
Poor treatment results among workers’ compensation patients may not arise solely from economic considerations. Rather, workers’ compensation patients have a number of additional issues that may lead to reports of high pain levels and poor treatment outcome. First, these patients have frequently been unable to work for extended periods at the time of surgery. Research on chronic pain has clearly shown that the length of time a patient has been nonfunctional strongly influences treatment outcome. Dworkin, Handlin, Richlin, Brand, and Vannucci (1985) using multiple regression to examine the relationships among compensation, litigation, and employment status (time off work) in 454 patients undergoing treatment for chronic pain found that only time off work (and not workers’ compensation or litigation) predicted treatment outcome. In similar and even more dramatic fashion, Anderson, Schwaegler, Cizek, and Leverson (2006) found that patients who were working up to the time that they went in for anterior lumbar interbody fusion (ALIF) were 10.5 times more likely to have returned to work by 1-year post-op than were individuals who had not been working prior to surgery. Interestingly, this association was independent of workers’ compensation status and number of spinal levels treated.
Responses to treatment by patients receiving workers’ compensation may be influenced by a number of other work-related factors, including job dissatisfaction (Bigos et al., 1991) and high levels of anger or blame toward the employer (DeGood & Kiernan, 1996). Regardless of the cause, workers’ compensation is so widely recognized as a risk factor that Frymoyer and Cats-Baril (1987) have proposed that compensability is one of the strongest predictors of excessive disability among back injury patients.
Treatments
Conservative Treatment
The natural history for patients suffering from an episode of back pain is actually quite positive. In the majority of patients (approximately 90 %), symptoms will resolve with or without treatment in a period of 6–12 weeks (Andersson, 1999). Therefore, in the absence of a progressive neurological deficit, spinal instability, infection, or tumor, conservative efforts toward managing back pain are the preferred initial approach.
Physical Therapy and Chiropractic Treatments
Physical therapy is one of the most commonly initiated rehabilitation programs for patients with low back pain. The goal of the various exercise regimens is to promote strengthening of the key postural muscles and thereby reduce stress or strain on the structures acting as pain generators. Numerous philosophies exist regarding the “best” technique for rehabilitation. “McKenzie exercises,” which are extension-based exercises, are believed to reduce discogenic pain by alleviating pressure on the posterior annulus (Melzack & Wall, 1965; Nachemson & Elfström, 1970). Flexion-based regimens, or “Williams exercises,” focus on decreasing compressive forces across the facet joints in an effort to decrease compressive loads at the posterior aspect of the disc, decompress the intervertebral foramen, and strengthen the core-stabilizing musculature (Williams, 1974). A study directly comparing both methods showed no significant difference between the two groups, except that sagittal mobility improved faster with flexion exercises (Elnaggar, Nordin, Sheikhzadeh, Parnianpour, & Kahanovitz, 1991).
Fitness programs including pilates and yoga are additional options targeting core strengthening for patients who are able to participate in them. The muscular conditioning afforded by these types of programs helps with maintaining appropriate posture and reducing low back strain. As well, it has been shown that exercise alone can improve function and decrease pain in adult patients suffering from chronic low back pain (Hayden, van Tulder, Malmivaara, & Koes, 2005). Chiropractic treatment, or spinal manipulation, is yet another option for the treatment of acute low back pain, and it has shown benefit equivalent to that from physical therapy in this group of patients (Cherkin, Deyo, Battie, Street, & Barlow, 1998).
Regardless of the specific type of rehabilitation program implemented, a key component for long-term success is patient education regarding appropriate biomechanics for proper lifting and bending techniques in order to avoid further injury and pain.
Injections
Various types of spinal injections can be employed as conservative treatment options. Depending on the presumed source of pain, facet injections, epidural injections, or even trigger point injections can play a role in conservative efforts. A goal of injection therapy is always to decrease or eliminate pain. However, in many cases, the diagnostic information obtained from a patient’s response to an injection can also help direct the physician toward additional treatment options should conservative efforts fail.
Epidural Steroid Injections
Epidural Steroid Injections (ESIs) are commonly performed as a treatment for low back or leg pain resulting from a number of spinal etiologies. The administration of a potent anti-inflammatory agent, usually combined with an anesthetic agent, acts to reduce local inflammation that can be caused from chemical mediators at the site of injury or nerve irritation. Studies have shown very mixed results with epidural injections and, considering that there are a number of techniques for administration of the steroid, this should come as no surprise. There is some evidence to suggest that caudal ESIs can provide short- and long-term improvement for chronic, axial low back pain and for radicular pain (Abdi et al., 2007).
Facet Injections
Facet-mediated pain has been implicated in up to 20 % of low back pain complaints, although the diagnosis itself is often quite difficult to accurately make. In the suspected case of pain stemming from the facets, the physician will often order a diagnostic injection. Under image guidance, a needle is inserted into the facet joint being evaluated, and a low volume of anesthetic, often coupled with a small amount of steroid, is injected. The “diagnostic phase” of the first 6–8 h following the injection can provide clinical information as to whether the facet joints are a chief contributing cause to the pain. Unfortunately, there is a high false-positive rate for a single set of diagnostic injections (Manchukonda, Manckikanti, Cash, Pampati, & Manchikanti, 2007), so the treating physician might consider a second set of injections as a “confirmatory” block.
Surgery
Surgical treatment of low back pain is a last resort, but in appropriately selected patients who have failed extensive conservative management and continue to have unremitting pain or functional disability, it can provide symptomatic improvement.
Discectomy
For patients with a herniated disc and resulting leg and/or back pain, surgical treatment is aimed toward decompressing the affected nerve(s) by removing the herniated fragment of disc. In one study designed to evaluate the long-term success of the procedure, successful outcomes at 6 months for 91 % of patients only declined slightly to 83 % at 10 years (Findlay, Hall, Musa, Olivreia, & Fear, 1998). Surgically treated patients were shown to have more complete relief of leg pain and improved function and satisfaction compared with nonsurgically treated patients in another large study over a 10-year follow-up period (Atlas, Keller, Wu, Deyo, & Singer, 2005).
Fusion
Lumbar fusion surgery as a treatment for low back pain, particularly for discogenic pain, remains quite controversial. Results in the literature are variable, but evidence does suggest that in an appropriately selected group of patients with severe low back pain, fusion can diminish pain and decrease disability more effectively than nonsurgical treatment (Fritzell, Hagg, Wessberg, & Nordwall, 2001). It should also be noted that there are many different techniques for spinal fusion, ranging from posterior intertransverse process fusions, posterior lumbar interbody fusions (PLIF), transforaminal lumbar interbody fusions (TLIF), lateral interbody fusions (XLIF or DLIF), ALIF, and combined anterior–posterior approaches (360° fusion). Application of spinal instrumentation, typically pedicle screws and connecting rods, usually accompanies the fusion in order to provide a more stable construct to facilitate bone healing.
Arthroplasty
Total disc replacement (TDR) technology emerged as an alternative treatment option to fusion, beginning in Europe over 20 years ago, and migrating to the United States in 2000 with the first Food and Drug Administration (FDA) Investigational Device Exemption (IDE) trial of the Charite III disc. There are various implant designs, but the key feature they all have in common is preservation of motion at the surgical level. The established indication for TDR is chronic low back pain from single-level degenerative disc disease that has failed extensive conservative treatment. A large driving force for development of disc replacement technology has been the concern over symptomatic adjacent segment disease seen after lumbar fusion. In a systematic review analyzing the association of symptomatic adjacent segment disease (as distinguished from asymptomatic adjacent segment degeneration) in lumbar disc replacement compared to fusion, Harrop et al. (2008) reported that 14 % of fusion patients developed adjacent segment disease, compared with 1 % of disc replacement patients.
Absolute contraindications to TDR include osteopenia and osteoporosis, history of previous disc infection or ongoing infection, prior fusion at the level of consideration, severe posterior element pathology, instability at the operative segment, vertebral fracture, malignancy, scoliotic curve greater than 11°, metal allergy, or a psychosocial state that places a given patient at increased risk for a poor surgical outcome. Relative contraindications include prior abdominal surgery and obesity (Guyer & Shellock 2011)
Spinal Cord Stimulation
Spinal cord stimulation (SCS) is a treatment option for patients with chronic back and/or leg pain who have failed prior surgical treatment (often referred to as FBSS) or who have pain that is predominantly neuropathic, such as from complex regional pain syndrome or from diabetic neuropathy. The first SCS device was implanted in 1967 by Shealy, who placed a subdural electrode over the dorsal columns of the spinal cord and connected it to an external power source (Shealy, Mortimer, & Reswick, 1967). Although the exact mechanism of action is still debatable, it is generally held that the “gate control theory” of pain, originally described by Melzack and Wall (1965), is the foundation for SCS technology. According to their theory, the central transmission of pain could be blocked by electrically stimulating afferent (i.e., sensory) nerve fibers. In other words, the stimulator can act as a “signal jammer” so the brain does not interpret a stimulus as painful.
Patients who are candidates for SCS should have exhausted reasonable medical and therapy approaches for their symptoms prior to undergoing the procedure. SCS is better able to reduce leg pain as opposed to back pain, which should be considered in evaluating a given patient for the procedure. Additionally, patients generally undergo placement of a trial stimulator, done with percutaneously placed electrodes, in order to ascertain the type of benefit they can receive with an implant. If the trial period is deemed successful, a patient can undergo permanent implantation of the device. Turner, Loeser, Deyo, and Sanders (2004), reviewing the literature on SCS for FBSS, found that pain was reduced by about one-half for 50–60 % of patients undergoing this procedure.
Presurgical Psychological Screening
There is clearly strong evidence that spine surgery can be effective in providing pain relief and improved functional ability. For example, a study by Malter, Larson, Urban, and Deyo (1996) found that patients who underwent discectomy for lumbar disc herniation, even at 5-year postsurgery, had significantly better quality of life than those who were treated conservatively. Similarly, Atlas, Keller, Robson, Deyo, and Singer (2000) compared the 4-year outcomes of surgery vs. unstructured conservative care for lumbar stenosis. They found that those treated surgically had significantly greater relief of pain and higher levels of satisfaction than those treated conservatively. However, spine surgery is not universally effective, and not-infrequently leads to worsening disability and the need for additional surgical intervention. For example, Sherman et al. (2010) found unfavorable outcomes in 28 % of lumbar discectomy patients, with 80 % of such patients undergoing repeat discectomy (average cost $6,907) and 20 % undergoing spinal fusion (average cost $24,375).
Beginning about 20 years ago, a growing body of research began to demonstrate that spine surgery failures can be predicted through the process of presurgical psychological screening (PPS). PPS is a procedure increasingly used in connection with a wide variety of surgical procedures, including bariatric surgery, organ transplantation, deep brain stimulation and reconstructive plastic surgery (Block & Sarwer, 2013). As applied to spine surgery, PPS utilizes a psychosocial diagnostic interview, psychometric testing and review of the medical records to identify empirically-determined psychosocial risk factors for reduced surgery outcome (Block, Gatchel, Deardorff, & Guyer, 2003). Many of these risk factors are those associated with back pain in general and reviewed above. These risk factors are weighted and combined to determine the patient’s level of psychosocial risk for poor surgery results. Research on PPS indicates that unfavorable surgery results are obtained by approximately 84 % of patients who fall into the highest risk category, while 20 % of those with low levels of psychosocial risk obtain poor results (Block et al., 2001).
Chronic Pain Management Programs
For many patients with persistent back pain, there exists a viable, effective alternative to spine surgery—the interdisciplinary chronic pain management program (CPMP). Such programs teach patients to manage and cope with pain and its impacts, through a combination of physical conditioning, education, psychosocial treatment, relaxation training, and vocational counseling. The CPMP approach can be as effective in treating spine pain patients as is spine surgery. Brox et al. (2003), for example, assessed 64 Swedish patients with evidence of severe disc degeneration lasting more than 1 year. These patients were randomly assigned to undergo either (1) a modified CPMP involving cognitive-behavioral intervention with 3 daily physical exercise sessions for 3 weeks, or (2) a lumbar fusion with posterior transpedicular screws and postoperative physical therapy. At 1-year follow-up, both groups had significant improvements in function, as measured by the Oswestry Disability Index (ODI). However, there was no significant difference found in functional improvement between those treated surgically and those treated nonsurgically. Additionally, there were no significant differences in pain, use of analgesics, emotional distress, and return to work. Fear-avoidance beliefs were reduced significantly more in the nonsurgically treated group (see Brox et al., 2006, for similar results). The early complication rate for the surgically treated group was 18 %.
Further support for the use of CPMP has been obtained by Fairbank et al. (2005) who examined 349 patients uncertain about whether they should undergo spine surgery. These patients were randomly assigned to an “intensive rehabilitation program” (essentially a CPMP) or to spinal fusion. Subjects were followed for 24 months. The fusion patients showed a slightly greater improvement in function as measured by the ODI, but no other comparisons between the two groups reached significance. An additional study of these same patients (Rivero-Arias et al., 2005) found that the cost of fusion far exceeded that of CPMP (£7,830 vs. £4,256). The percentage of patients returning to work at 2 years were equivalent, indicating CPMP was much more cost-effective than spinal fusion. Turk and Burwinkle (2005), in a separate review of the literature extending such findings, determined that the CPMP approach can be approximately 26-times more cost-effective in patients returning to work than is spine surgery.
It appears, then, that CPMP is a viable alternative for some spine surgery candidates. This is particularly the case for those whose psychosocial risk profiles place them in the high-risk category for reduced spine surgery outcome, or those who are uncertain about whether to undergo spine surgery. However, there are many other potential candidates for spine surgery who could benefit by consideration of CPMP. For example, many patients may have expectations of poor outcome, or may be overly optimistic in their hopes. Iverson, Daltroy, Fossel, and Katz (1998) found that expectations of great pain relief by patients who underwent surgery for spinal stenosis were associated with more pain and less satisfaction at 6 months than were lower expectations of pain relief (however, in this study, higher expectations of improvement in functioning as a result of the surgery were associated with greater improvement in functioning and greater satisfaction). Thus, for patients expecting to have “no pain” as a result of spine surgery, CPMP may be a valuable alternative. Such is also the case for patients who have failed previous spine surgeries because, as noted by a number of authors including North, Campbell, James, and Conover-Walker et al., 1991), the success rate for repeat spine surgery is quite low (see also Franklin et al., 1994). Similarly, since substance abuse or overuse is associated with reduced spine surgery outcome (Spengler, Freeman, Westbrook, & Miller, 1980), patients with such problems would likely be better served by participation in a CPMP than by spine surgery.
Summary and Conclusions
Back pain is the most problematic complaint associated with occupational injuries. Fortunately, most patients, like Mr. A in the introduction to this chapter, recover rapidly and without much, if any, medical treatment. On the other hand, Mr. Z represents the relatively small percentage of patients whose pain continues unabated, consuming large economic and medical resources, devolving into increasing disability and emotional distress. This chapter provides strong evidence that, with appropriate medical or surgical treatment, even most of those with protracted back pain can experience significant improvement. However, many psychosocial factors are associated with the development and maintenance of back pain. These same factors are associated with reduced outcomes of conservative and surgical treatment. Costs to the insurer and employer, as well as frustration and emotional distress to the patient, can be reduced when medical providers are aware of, and address, such psychosocial issues, and avoid worsening them, by being cautious in the use of opioid therapy, spine surgery, or other high-risk procedures.
References
Abdi, S., Datta, S., Trescott, A., Schultz, D. M., Adlaka, R., Atluri, S. L., et al. (2007). Epidural steroids in the management of chronic spinal pain: A systematic review. Pain Physician, 10, 185–212.
Anderson, P. A., Schwaegler, P. E., Cizek, D., & Leverson, G. (2006). Work status as a predictor of surgical outcome of discogenic low back pain. Spine, 31, 2510–2515.
Andersson, G. B. J. (1999). Epidemiological features of chronic low-back pain. Lancet, 354, 581–585.
Atlas, S. J., Keller, R. B., Robson, D., Deyo, R. A., & Singer, D. E. (2000). Surgical and nonsurgical management of lumbar spinal stenosis: Four-year outcomes from the Maine lumbar spine study. The Spine Journal, 35(5), 556–562.
Atlas, S. J., Keller, R. B., Wu, Y. A., Deyo, R. A., & Singer, D. E. (2005). Long-term outcomes of surgical and non-surgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine Lumbar Spine Study. Spine, 30, 936–943.
Atlas, S. J., Tosteson, T. D., Blood, E. A., Skinner, J. S., Pransky, G. S., & Weinstein, J. N. (2009). The impact of workers compensation on outcomes of surgical and nonoperative therapy for patients with lumbar disc herniation: Sport. Spine, 2009, 89–97.
Ben-Porath, Y. S., & Tellegen, A. (2008). The Minnesota multiphasic personality inventory-2 restructured form (MMPI-2-RF): Manual for administration, scoring, and interpretation. Minneapolis, MN: University of Minnesota Press.
Bigos, S. J., Battie, M. C., Spengler, D. M., Fisher, L. D., Fordyce, W. E., Hansson, T., et al. (1991). A prospective study of work perceptions and psychosocial factors affecting the report of back injury. Spine, 16, 1–6.
Block, A. R., Ben-Porath, Y. S., & Marek, R. J. (2013). Psychological risk factors for poor outcome of spine surgery and spinal cord stimulator implant: A review of the literature and their assessment with the MMPI-2-RF. The Clinical Neuropsychologist, 27, 81–107. doi: 10.1080/13854046.2012.721007.
Block, A.R., Ben-Porath, Y.S., Ohnmeiss, D., Guyer, R.D., & Marek, R. (2012). Psychosocial factors and expectancy contribute separately to spine surgery outcome. Paper Presented at North American Spine Society Annual Convention, Dallas, TX.
Block, A. R., Gatchel, R., Deardorff, W., & Guyer, R. (2003). The psychology of spine surgery. Washington, DC: American Psychological Association.
Block, A. R., Ohnmeiss, D. D., Guyer, R. D., Rashbaum, R., & Hochschuler, S. H. (2001). The use of presurgical psychological screening to predict the outcome of spine surgery. The Spine Journal, 1, 274–282.
Block, A. R., & Sarwer, D. B. (Eds.). (2013). Presurgical psychological screening: Understanding patients, improving outcomes. Washington, DC: American Psychological Association.
Brox, J. I., Reikeras, O., Nygaard, O., Sørensen, R., Indahl, A., Holm, I., et al. (2006). Lumbar instrumented fusion compared with cognitive intervention and exercises in patients with chronic back pain after previous surgery for disc herniation: A prospective randomized controlled study. Pain, 122, 145–155.
Brox, J. I., Sorensen, R., Friis, A., Nygaard, Ø., Indahl, A., Keller, A., et al. (2003). Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine, 28, 1913–1921.
Bruehl, S., Chung, O. Y., Burns, J. W., & Diedrich, L. (2007). Trait anger expressiveness and pain-induced beta-endorphin release: Support for the opioid dysfunction hypothesis. Pain, 130, 208–215.
Burns, J. W. (2006). Arousal of negative emotions and symptom-specific reactivity in chronic low back pain patients. Emotion, 6, 309–319.
Carlson, J. W., Keefe, F. J., Goli, V., Fras, A. M., Lynch, T. R., Thorp, S. R., et al. (2005). Forgiveness and chronic low back pain: A preliminary study examining the relationship of forgiveness to pain, anger and psychological distress. The Journal of Pain, 6, 84–91.
Cherkin, D. C., Deyo, R. A., Battie, M., Street, J., & Barlow, W. (1998). A comparison of physical therapy, chiropractic manipulation, and provision of an educational booklet for the treatment of patients with low back pain. New England Journal of Medicine, 339, 1021–1029.
Chou, L. H., Slipman, C. W., Bhagia, S. M., Tsaur, L., Bhat, A. L., Isaac, Z., et al. (2004). Inciting events initiating injection-proven sacroiliac joint syndrome. Pain Medicine, 5, 26–32.
Currie, S. R., & Wang, J. L. (2004). Chronic back pain and major depression in the general Canadian population. Pain, 107, 54–60.
Davis, D. A., Luecken, L. J., & Zaruta, A. J. (2005). Are reports of childhood abuse related to the experience of chronic pain in adulthood? A meta-analytic review of the literature. Clinical Journal of Pain, 21, 398–405.
DeGood, D. E., & Kiernan, B. (1996). Perception of fault in patient with chronic pain. Pain, 64, 153–159.
Dennis, M. D., Rocchio, P. O., & Wiltse, L. L. (1981). The topographical pain representation and its correlation with MMPI scores. Orthopedics, 5, 432–434.
Dersh, J. D., Mayer, T. G., Gatchel, R. J., Polatin, P. B., Theodore, B. R., & Mayer, E. A. K. (2008). Prescription opioid dependence is associated with poorer outcomes in disabling spinal disorders. The Spine Journal, 20, 2219–2227.
Deyo, R. A., Mirza, S. K., & Martin, B. I. (2006). Back pain prevalence and visit rates: Estimates from U.S. national surveys. Spine, 21, 1957–1963.
Dreyfuss, P., Michaelsen, M., Pauza, K., McLarty, J., & Bogduk, N. (1996). The value of medical history and physical examination in diagnosing sacroiliac joint pain. Spine, 21, 2594–2602.
Dworkin, R. H., Handlin, D. S., Richlin, D. M., Brand, L., & Vannucci, C. (1985). Unraveling the effects of compensation, litigation and employment on treatment response in chronic pain. Pain, 23, 49–59.
Elnaggar, I. M., Nordin, M., Sheikhzadeh, A., Parnianpour, M., & Kahanovitz, N. (1991). Effects of spinal flexion and extension exercises on low-back pain and spinal mobility in chronic mechanical low-back pain patients. Spine, 16, 967–972.
Fairbank, J., Frost, H., Wilson-MacDonald, J., Yu, L. M., Barker, K., & Collins, R. (2005). Randomised controlled trial to compare surgical stabilisation of the lumbar spine with an intensive rehabilitation programme for patients with chronic low back pain: The MRC spine stabilisation trial. British Medical Journal, 330, 1233–1239.
Fernandez, E., Clark, T. S., & Ruddick-Davis, D. (1999). A framework for conceptualization and assessment of affective disturbance in pain. In A. R. Block, E. F. Kremer, & E. Fernandez (Eds.), Handbook of pain syndromes: Biopsychosocial perspectives. Mahwah, NJ: Lawrence Erlbaum.
Fernandez, E., & Turk, D. C. (1995). The scope and significance of anger in the experience of chronic pain. Pain, 61, 165–175.
Findlay, G. F., Hall, B. I., Musa, B. S., Olivreia, M. D., & Fear, S. C. (1998). A 10-year follow-up of the outcome of lumbar discectomy. Spine, 10, 1168–1171.
Fishbain, D., Cutler, R., Rosomoff, H., & Rosomoff, R. (1997). Chronic-pain associated depression: Antecedent or consequence of chronic pain? A review. Clinical Journal of Pain, 13, 116–137.
Frank, J. W., Brooker, A. S., DeMaio, S. E., Kerr, M. S., Maetzel, A., Shannon, H. S., et al. (1996). Disability resulting from occupational low back pain. Part II: What do we know about secondary prevention? A review of the scientific evidence on prevention after disability begins. Spine, 21, 2918–2929.
Franklin, G. M., Haug, J., Heyer, N. J., McKeefrey, S. P., & Picciano, J. F. (1994). Outcome of lumbar fusion in Washington state workers’ compensation. Spine, 19(17), 1897–1904.
Fritzell, P., Hagg, O., Wessberg, P., & Nordwall, A. (2001). Volvo award winner in clinical studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish lumbar spine study group. Spine, 26, 2521–2532.
Frymoyer, J. W., & Cats-Baril, W. L. (1987). An overview of the incidences and cost of low back pain. Orthopedic Clinics of North America, 22, 263–271.
Ghormley, R. (1933). Low back pain with special reference to the articular facets with presentation of an operative procedure. Journal of the American Medical Association, 101, 1773–1777.
Green, C. R., Flowe-Valencia, H., Rosenblum, L., & Tait, A. R. (1999). Do physical and sexual abuse differentially affect chronic pain states in women? Journal of Pain and Symptom Management, 18, 420–426.
Gureje, O., Von Korff, M., Kola, L., Demyttenaere, K., He, Y., Posada-Villa, J., et al. (2008). The relation between multiple pains and mental disorders: Results for the World Mental Health Survey. Pain, 135, 82–91.
Guyer, R. D., & Shellock, J. (2011). Lumbar disc arthroplasty: Indications and contra-indications. In J. J. Yue, R. D. Guyer, J. P. Johnson, T. L. Khoo, & S. H. Hochschuler (Eds.), Comprehensive treatment of the aging spine: Minimally invasive and advanced techniques. Philadelphia: Saunders.
Haber, J., & Roos, C. (1985). Effects of spouse abuse and/or sexual abuse in the development and maintenance of chronic pain in women. Advances in Pain Research and Therapy, 9, 889–895.
Harkonmaki, K., Korkeila, K., Vahtera, J., Kivimaki, M., Suominen, S., Silanmaki, L., et al. (2008). Childhood adversities as a predictor of disability retirement. Journal of Epidemiology and Community Health, 61, 479–484.
Harris, I., Mulford, J., Solomon, M., van Gelder, J. M., & Young, J. (2005). Association between compensation status and outcome after surgery. Journal of the American Medical Association, 293, 1644–1652.
Harrop, J. S., Youssef, J. A., Maltenfort, M., Vorwald, P., Jabbour, P., Bono, C. M., et al. (2008). Lumbar adjacent segment degeneration and disease after arthrodesis and total disc arthroplasty. Spine, 33, 1701–1707.
Hayden, J. A., van Tulder, M. W., Malmivaara, A., & Koes, B. W. (2005). Exercise therapy for the treatment of non-specific low back pain. Cochrane Database Systems Review, 3, CD000335.
Irish, L., Kobayashi, I., & Delhanty, D. L. (2010). Long-term health consequences of childhood sexual abuse: A meta-analytic review. Journal of Pediatric Psychology, 35, 450–461.
Iverson, M. D., Daltroy, L. H., Fossel, A. H., & Katz, J. N. (1998). The prognostic importance of patient pre-operative expectations for surgery for lumbar spinal stenosis. Patient Education and Counseling, 34, 169–178.
Katz, J. N. (2006). Lumbar disc disorders and low-back pain: Socioeconomic factors and consequences. Journal of Bone and Joint Surgery, 88(Suppl. 2), 21–24.
Keller, L. S., & Butcher, J. N. (1991). Assessment of chronic pain patients with the MMPI-2. Minneapolis, MN: University of Minnesota Press.
Klekamp, J., McCarty, E., & Spengler, D. (1998). Results of elective lumbar discectomy for patients involved in the workers’ compensation system. Journal of Spinal Disorders, 11, 277–282.
Lawrence, J. T., London, N., Bohlman, H. H., & Chin, K. R. (2008). Preoperative narcotic use as a predictor of clinical outcome: Results following anterior cervical arthrodesis. Spine, 33(19), 2074–2078.
Linton, S. J. (1997). A population-based study of the relationship between sexual abuse and back pain: Establishing a link. The Journal of Pain, 73, 47–53.
Luschka, H. V. (1850). Die Nerven des menshlichen Wirbelkanales. Tubingen, Germany: Laub.
Mahowald, M. L., Singh, J. A., & Majeski, P. (2005). Opioid use by patients in an orthopedic spine clinic. Arthritis and Rheumatism, 52, 312–321.
Malter, A. D., Larson, E. B., Urban, N., & Deyo, R. A. (1996). Cost-effectiveness of lumbar discectomy for the treatment of herniated intervertebral disc. The Spine Journal, 21, 1048–1054.
Manchukonda, R., Manckikanti, K. N., Cash, K. A., Pampati, V., & Manchikanti, L. (2007). Facet joint pain in chronic spinal pain: An evaluation of prevalence and false-positive rate of diagnostic blocks. Journal of Spinal Disorders & Techniques, 20, 539–545.
Martell, B. A., O’Connor, P. R., Kerns, R. D., Becker, W. C., Morales, K. H., Kosten, T. R., et al. (2007). Systematic review: Opioid treatment for chronic back pain: Prevalence, efficacy and association with addiction. Annals of Internal Medicine, 146, 16–127.
Martin, B. I., Deyo, R. A., Mirza, S. K., Turner, H. A., Comstock, B. A., Hollingworth, W., et al. (2008). Expenditures and health status among adults with back and neck problems. Journal of the American Medical Association, 299, 656–664.
McWilliams, L. A., Goodwin, R. D., & Cox, B. J. (2004). Depression and anxiety associated with three pain conditions: Results from a nationally-representative sample. Pain, 111, 77–83.
Melzack, R., & Wall, P. D. (1965). Pain mechanism: A new theory. Science, 150, 971–979.
Nachemson, A., & Elfström, G. (1970). Intravital dynamic pressure measurements in lumbar discs: A study of common movements, maneuvers and exercises. Scandinavian Journal of Rehabilitation Medicine, 1(Suppl. 1), 1–40.
National Research Council and Institute of Medicine. (2001). Musculoskeletal disorders and the workplace: low back and upper extremities (Panel on Musculoskeletal disorders and the work place. Commission on Behavioral and Social Science and education). Washington, DC: National Academy Press.
North, R. B., Campbell, J. N., James, C. S., Conover-Walker, M. K., Wang, H., Piantadosi, S., et al. (1991). Failed back surgery syndrome: 5-year follow up in 102 patients undergoing repeated operation. Neurosurgery, 28(5), 685–691.
Nyiendo, J., Haas, M., Goldberg, B., & Lloyd, C. (2001). A descriptive study of medical and chiropractic patients with chronic low back pain and sciatica: management by physicians (practice activities) and patients (self-management). Journal of Manipulative and Physiological Therapeutics, 24, 5423–5551.
Panjabi, M. M. (2006). A hypothesis of chronic back pain: Ligament subfailure injuries lead to muscle control dysfunction. European Spine Journal, 5, 668–676.
Pleis, J. R., & Lethbridge-Cejku, M. (2007). Summary health statistics for U.S. adults: National Health Interview Survey, 2006. National Center for Health Statistics. Vital and Health Statistics, 10(235), 1–153.
Polatin, P. R., Kinney, R. K., Gatchel, R. J., Lillo, E., & Mayer, T. G. (1993). Psychiatric illness and chronic low-back pain. The mind and the spine—which goes first? Spine, 12, 66–71.
Rivero-Arias, O., Campbell, H., Gray, A., Fairbank, J., Frost, H., & Wilson-MacDonald, J. (2005). Surgical stabilisation of the spine compared with a programme of intensive rehabilitation for the management of patients with chronic low back pain: Cost utility analysis based on a randomised controlled trial. British Medical Journal, 330, 1239–1243.
Rosenblum, A., Marsch, L. A., Portenoy, R. K., & Jospeh, H. (2008). Opioids and the treatment of chronic pain: Controversies, current status and future directions. Experimental and Clinical Psychopharmacology, 16, 405–416.
Shealy, C. N., Mortimer, J. T., & Reswick, J. B. (1967). Electrical inhibition of pain by stimulation of the dorsal columns: preliminary clinical report. Anesthesia and Analgesia, 46, 489–491.
Sherman, J., Cauthen, J., Schoenberg, D., Burns, M., Reaven, N. L., & Griffith, S. L. (2010). Economic impact of improving outcomes of lumbar discectomy. The Spine Journal, 10, 108–116.
Simons, D. G., Travell, J. G., & Simons, L. S. (1999). Myofascial pain and dysfunction. The trigger point manual (2nd ed.). Baltimore: Williams & Wilkins.
Slipman, C. W., Sterenfeld, E. B., Chou, L. H., Herzog, R., & Vresilovic, E. (1998). The predictive value of provocative sacroiliac joint stress maneuvers in the diagnosis of sacroiliac joint syndrome. Archives of Physical Medicine and Rehabilitation, 79, 288–292.
Spengler, D. M., Freeman, C., Westbrook, R., & Miller, J. W. (1980). Low-back pain following multiple lumbar spine procedures: Failure of initial selection? Spine, 5(4), 356–360.
Substance Abuse and Mental Health Services Administration. (2008). Results from the 2007 national survey on drug use and health: National findings (Office of Applied Studies, NSDUH Series H-34, DHS publication No. SMA 08-4343), Rockville, MD.
Takata, K., & Hirotani, H. (1995). Pain drawings in the evaluation of low back pain. International Orthopaedics, 19, 361–366.
Turk, D. C., & Burwinkle, T. M. (2005). Assessment of chronic pain in rehabilitation: Outcomes measures in clinical trials and clinical practice. Rehabilitation Psychology, 50, 56–64.
Turk, D. C., & Okifuji, A. (1996). Perception of traumatic onset, compensation status, and physical findings: Impact on pain severity, emotional distress, and disability in chronic pain patients. Journal of Behavioral Medicine, 19, 435–453.
Turner, J. A., Loeser, J. D., Deyo, R. A., & Sanders, S. B. (2004). Spinal cord stimulation for patients with failed back surgery syndrome or complex regional pain syndrome: A systematic review of effectiveness and complications. The Journal of Pain, 108, 137–147.
Vernon-Roberts, B., & Pirie, C. J. (1977). Degenerative changes in the intervertebral discs of the lumbar spine and their sequelae. Rheumatology Rehabilitation, 16, 13–21.
Walsh, C. A., Jamieson, E. L., MacMillian, H., & Boyle, M. (2007). Child abuse and chronic pain in a community survey of women. Journal of Interpersonal Violence, 22, 1536–1554.
Williams, P. (1974). Low back and neck pain: Causes and conservative treatment (3rd ed.). Springfield, IL: Charles C. Thomas.
Wunsch, M. J., Cropsey, K. L., Campbell, E. D., & Nicely, J. S. (2008). Oxycontin abuse and overuse. Journal of Opioid Management, 4, 73–79.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Block, A.R., Shellock, J. (2014). Back Pain. In: Gatchel, R., Schultz, I. (eds) Handbook of Musculoskeletal Pain and Disability Disorders in the Workplace. Handbooks in Health, Work, and Disability. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-0612-3_2
Download citation
DOI: https://doi.org/10.1007/978-1-4939-0612-3_2
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-0611-6
Online ISBN: 978-1-4939-0612-3
eBook Packages: Behavioral ScienceBehavioral Science and Psychology (R0)