
Abstract
This chapter will review three genetically determined diseases: alpha-1 antitrypsin deficiency, Wilson disease, and hereditary hemochromatosis. Liver disease associated with cystic fibrosis and other disorders of iron storage are also reviewed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Alpha-One Antitrypsin Deficiency
Background
Alpha-1 antitrypsin deficiency (A1-ATD) is the most common genetic cause of liver disease in children, with a prevalence of 1:1,600–1:2,000 per live birth [1–3]. One in 5,000 North Americans has severe A1-ATD [4]. It is an autosomal codominant condition resulting in an 85–90 % reduction in serum alpha-1 antitrypsin (A1-AT). A1-AT is a member of the serine protease inhibitor (serpin) family that inhibits destructive neutrophil proteases, elastase, cathepsin G, and proteinases. The protein is produced in the liver and increases in response to injury and inflammation [5–7].
Deficiency of the A1-AT protein results in both liver and lung injury. Adults develop chronic lung disease felt to be due to unregulated elastolytic attack of the connective tissue due to decreased circulating levels of A1-AT [2]. Lung injury is accelerated by smoke and pollution exposure [8–10]. In adults the disease is also associated with a variety of liver disorders, including chronic hepatitis, cirrhosis, and hepatocellular carcinoma. Children also demonstrate a broad spectrum of liver involvement. A1-AT deficiency is the most common metabolic disease causing neonatal hepatitis syndrome. The presentation is easily confused with biliary atresia and cystic fibrosis; however, the pathology can differ. The pathophysiology of liver disease is not clearly understood. The current belief is that liver injury results from retention of misfolded A1-AT molecules in the endoplasmic reticulum (ER) of hepatocytes [11].
Structure of Alpha-1 Antitrypsin
The normal A1-AT molecule is designated by its electrophoretic migration pattern as M (middle). The various structural variants of A1-AT are identified by agarose electrophoresis or isoelectric focusing of plasma in polyacrylamide gel at acid pH [12]. Letters are assigned to variants based on distance of migration using alphabetical assignments from low to high isoelectric points [12]. The most common severe deficiency, PiZZ, has a A1-AT variant that moves the slowest [2]. PiZZ is responsible for 95 % of cases of severe A1-ATD [13].
Function of Alpha-1 Antitrypsin
The major physiologic function of A1-AT is inhibition of the serine proteases, released by activated neutrophils, to include elastase, cathepsin G, and proteinase 3 [14].
Biosynthesis and Regulation
The primary site of A1-AT production is the liver. This is demonstrated by synthesis of the donor A1-AT phenotype in patients following an orthotopic liver transplant and the basis for correction with liver transplantation [2]. A1-AT is synthesized and secreted to a lesser degree from human blood monocytes and bronchoalveolar and breast milk macrophages [2].
Plasma concentration of A1-AT increases three- to fivefold in response to inflammation and/or tissue injury mediated by IL 6 and lipopolysaccharide (LPS) stimulation [2, 3, 15]. Levels of A1-AT also rise during pregnancy and with oral contraceptive therapy [2].
Variants
There are more than 120 identified allelic variants. The majority of variants are associated with a reduction in serum A1-AT protein levels. There is a null variant, with no measurable A1-AT in the serum, associated with emphysema, but not liver disease [16]. PiMM (protease inhibitor), the normal variant, is the phenotype in 95 % of the population and is associated with normal serum levels of A1-AT. The S and Z variants are the most common. Some of the variants, such as S, are not associated with disease in homozygous state. Other familial variants result in a deficiency of serum A1-AT and demonstrate variable presentations, including emphysema and liver disease.
PiZZ has less elastase inhibition capability and is cleared sooner due to its instability [17]. The mutation is due to a single AA nucleotide change (lysine for glutamic acid) resulting in decreased secretion and accumulation of the mutated form in the endoplasmic reticulum (ER). The protein becomes trapped due to increased folding and decreased stability [18]. PiSS has no decrease in function or duration of function [19, 20].
Liver Disease
Liver involvement and disease, first reported in 1968 by Freir et al. and in 1969 by Sharp, is quite variable in affected individuals [21]. Data and animal models are most consistent with accumulation of abnormal A1-AT in ER resulting in hepatocyte damage. Interestingly not all patients with ER accumulation of the mutant protein develop injury. This suggests a role for inherited traits and environmental factors [2, 3].
Liver disease develops in PiZZ and PiSZ variants and very rarely in PiMZ. Liver disease does not occur with the other variants (e.g., PiSS). The PiMZ state, which has a 50 % reduction in serum A1-AT, may predispose to more severe liver disease in other hepatic disorders such as hepatitis B and C, alcoholic liver disease, cystic fibrosis-associated liver disease, and NAFLD [22, 23]. The clinical spectrum of liver disorders is shown in Table 9.1.
The natural history of liver disease has been described in a longitudinal follow-up study from Sweden [6, 7, 24]. Of the 176 with A1-ATD after screening of 200,000 infants in 1972–1974, 125 were PiZZ, 48 PiSZ, 2 PiZnull, and 1 PiSnull. Forty-five percent of the PiZZ infants were small for gestational age. Only 11 % of the affected infants had obstructive jaundice in infancy. Of the 14 PiZZ infants with cholestasis, 9 demonstrated severe clinical and laboratory evidences and 5 had only laboratory evidence of liver disease. Four of these infants went on to develop cirrhosis by 2 years of age. Eighty-three percent demonstrated no clinical signs of liver disease, but 50 % still had abnormal LFTs at 6 months of age. Two thirds of those with hepatic anomalies were male. Only 25 % of the PISZ infants had abnormal LFTs. By 18 years of age, 85 % had normal aminotransferases and no signs of liver disease [6]. Three children died before age eight of liver disease. Further follow-up of the same population identified that only 5–10 % of all PiZZ children develop significant liver disease [6, 24].
Other studies have screened all infants with liver disease for A1-ATD [25, 26]. In 43 infants with A1-ATD identified over 10 years, 24 were PiZZ [25]. Liver pathology was available on 14 of the PiZZ infants in whom 57 % had periodic acid-Schiff (PAS) inclusion bodies at less than 3 months of age. Of the PiZZ infants, 10 % were born premature, 37 % were SGA, and 31 % had failure to thrive with 83 % identified and diagnosed by 3 months of age. Laboratory studies showed elevated transaminases in 59 and 91 % were cholestatic. Physical findings demonstrated hepatomegaly in 87 % and splenomegaly in 43 % with only 5 % having a normal physical exam. Heterozygotes were more likely to have normal laboratory values, with only 23 % having elevated transaminases and 39 % with cholestasis. Hepatomegaly was present in only 43 % and splenomegaly in 7 % of heterozygotes. In a large pediatric liver practice, 36 children with A1-ATD were identified from 424 with liver disease [26]. Nineteen were PiZZ, all of whom had prolonged cholestasis. All demonstrated PAS inclusions on liver biopsy. All demonstrated hepatomegaly and elevated LFTs, and all but one had resolution of cholestasis by 7 months of age. Three developed cirrhosis by 3 years of age. Cirrhosis and portal hypertension may have been present in 5 others with hepatosplenomegaly and fibrosis. The 16 affected with heterozygous disease (MS, MZ, SZ) demonstrated less severe liver involvement with cholestasis in 5. Interestingly, many were found to have other liver disease including biliary atresia. One sibling was identified as PiZZ with no evidence of liver disease, again showing the variability in disease course.
Lung Disease
Lung injury in A1-ATD is due to multiple factors. Due to low levels of A1-AT in the lungs, the elastase created by neutrophils is not neutralized, and proteolytic activity goes unchecked. Cigarette smoke and pollution exposure along with pulmonary infections significantly affect the elastase levels and therefore the severity of lung damage [27].
Lung disease is commonly associated with A1-AT deficiency with 60–70 % of PiZZ subjects developing lung injury as adults. The typical presentation is insidious development of dyspnea in the 30–40s. Lung disease peaks in the fourth and fifth decades [22, 28]. One half will have a cough and history of recurrent infections with progression to decreasing FEV (forced expiratory volume) and increasing total lung capacity [8]. Chest X-ray demonstrates hyperinflation with base atelectasis [29]. The correlation between cigarette smoking and decreasing survival is clear [13]. The National Heart Lung and Blood Institute reports a mortality of 3 % per year in A1-ATD with 72 % dying from lung disease and only 10 % from liver disease [13].
Diagnosis
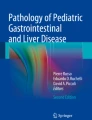
A1-ATD is diagnosed by both serology and histology. Screening with serum levels is acceptable, but levels can be elevated in acute infection. PiZZ phenotypes rarely have serum levels over 50–60 mg/dL [30]. Serum A1-AT phenotyping (Pi phenotyping) should be performed in children with low levels (<1.1 g/L) or those with a high suspicion despite low normal levels [30]. Genotyping is available, but rarely needed. Histology can be useful for diagnosis, but is not necessary. PAS-positive diastase-resistant eosinophilic globules can be visualized in the endoplasmic reticulum in the periportal hepatocytes (Fig. 9.1) [31, 32].

PAS-positive diastase-resistant eosinophilic globules (black arrow) in a liver biopsy from a child with A1-ATD (40×)
Similar findings are seen in other liver diseases and therefore are not diagnostic [32]. In addition, the histology may demonstrate necrosis, inflammation, fibrosis, cirrhosis, bile duct proliferation, bile duct destruction, and possible bile duct paucity [32]. Individuals where screening for A1-ATD is appropriate are shown in Table 9.2.
Treatment
Treatment of patients with A1-ATD is primarily supportive care and aggressive prevention and treatment of lung disease. At this time there are no specific therapies for A1-ATD liver disease. Infants with cholestasis may benefit from fat-soluble vitamin supplementation. Ursodeoxycholic acid is often used to improve bile flow, but no study has shown benefit. There has been a suggestion that breastfeeding provides some protection. It has been postulated that breast milk contains active A1-AT [33]. However, no difference was found between breast- and formula-fed babies in another report [34]. Avoidance of cigarette smoke (primary and secondary) and environmental pollution is vital as this accelerates lung disease and has a clear association with shortened life.
Liver transplantation is appropriate for individuals with end-stage liver disease. The recipient assumes the donor’s Pi phenotype. A1-ATD accounts for 3.5 % of all pediatric and 1.1 % adult liver transplants [35]. More males were transplanted than females. One-year survival in children and adults was 89 and 92 % and 5-year survival 83 and 90 %. In addition to improvement in liver disease, there is a decrease in the risk of lung disease.
Gene therapy has also been evaluated and may hold hope for lung disease [36]. Pluripotent stem cell therapy is also currently being evaluated with promising early results [37].
Recombinant A1-AT administered by inhalation or infusion is used in A1-ATD-associated lung disease but not the liver disease. Many other drugs and therapies are currently being evaluated. Of these, carbamazepine is in clinical safety and efficacy trials [38].
A1-AT and Other Organs
There have been some reports and small studies that have suggested a role of A1-AT deficiency in the development of other disease to include inflammatory bowel disease, glomerulonephritis, and pancreatitis, but no definitive study has been completed. Further study is needed to confirm associations and understand mechanisms.
A1-AT Summary
A1-ATD should be considered in all adults and children with liver disease of unclear etiology. Most affected individuals develop liver disease. A1-AT deficiency is associated with both liver and lung injury and possible other organ involvement. Liver damage is due to retained A1-AT in the endoplasmic reticulum. There is currently no accepted medical therapy for liver disease, but gene and stem cell therapy continue to be investigated. Liver transplant does resolve the liver disease and improve lung function.
Wilson Disease
Background
Wilson disease (WD) is a rare autosomal recessive disorder of copper metabolism. Mutations of the copper-transporting P-type ATPase, ATP7B, impair the biliary excretion of copper and cellular utilization resulting in copper overload and copper accumulation in tissue. First described in 1912 as a central nervous system disease (CNS) with asymptomatic liver involvement [39], it is now understood that WD affects many organ systems with CNS and liver being the most significant. The prevalence is estimated at 1 in 30,000 persons worldwide with a carrier frequency of 1 in 90 [40, 41]. Symptoms often begin in childhood and adolescence. WD is universally fatal if not treated.
Genetics
The gene for WD, located on chromosome 13, encodes a transmembrane copper-transporting P-type ATPase, ATP7B [42, 43]. There are more than 500 identified polymorphisms in the ATP7B gene, with more than 250 confirmed as disease-causing mutations [44]. Newer studies show a correlation between genotype and phenotype. Patients with nonsense or frameshift mutations have earlier and more severe disease [45]. A database of the polymorphisms can be found at www.wilsondisease.med.ualberta.ca/database.asp [46]. The variability in timing of onset and severity of symptoms suggests involvement of modifier genes and environmental factors. One example is the MURR1 gene, which has been associated with earlier onset of disease [47].
Pathophysiology
Copper is an essential trace element functioning as a coenzyme for many key enzymes [47]. Following ingestion, copper diffuses across the intestinal mucosa and is carried across the enterocyte by the copper-transporting enzyme, ATP7A, into the portal circulation where it binds to albumin allowing transport into the hepatocytes by transporter HCTR1. Inside the hepatocyte it is chaperoned to the Golgi network where ATP7B, an ATPase transporter, transports copper for incorporation into ceruloplasmin. It is then exported in the bile [47]. In WD, ceruloplasmin secretion is decreased due to decreased copper delivery, but apoceruloplasmin, which has a shorter half-life, is normal.
The resultant inadequate excretion in WD results in excessive copper accumulation in the brain, liver, kidney, and other organs [48]. The exact mechanisms of copper toxicity are not fully understood. It has been suggested that copper accumulation induces cellular damage via oxidative stress, increased apoptosis, or mitochondrial damage [44, 47].
Clinical Manifestations
The initial presentation can occur between 5 and 35 years of age (See Table 9.3). The youngest reported new diagnosis was at 3 years and the oldest in their 80s [47]. Typically, manifestations are related to liver and CNS copper deposition. The frequency of the primary presentations were hepatic in 42 %, CNS in 44 % (neurologic 34 % and psychiatric 10 %), and hematologic and endocrine in 12 % [48–50]. One fourth of patients have multiorgan involvement [48]. In children it is common for hepatic involvement to precede neurologic manifestations. After the age of 20 years, the neurologic (75 %) presentation is more common than hepatic (25 %) [51]. In children evaluation is often triggered by elevated transaminases, hepatomegaly, or family history of WD [51]. Syriopoulou’s study of 57 pediatric patients showed 1/3 to have hepatic symptoms triggering evaluation [51].
Hepatic Manifestations
Liver involvement can vary from a self-limited acute hepatitis through a chronic hepatitis to acute liver failure. Younger children may present with acute liver failure with jaundice, coagulopathy, ascites, and hepatic encephalopathy commonly with massive hemolysis. Acute liver failure due to WD accounts for approximately 4 % of all acute liver failure in children over 3 years of age [52] and occurs in up to 12 % of all cases [47]. Children with liver failure demonstrate a female predominance, likely related to hormonal influences [41]. Children and adolescents may also present with evidence of chronic liver disease with cirrhosis, portal hypertension, and ascites. Hepatomegaly is found in many children with WD with one study identifying hepatomegaly in 77 % of WD children [51]. Cholelithiasis is another complication of WD and warrants a WD evaluation in the undiagnosed. The stones are mixed pigment and cholesterol [48].
Central Nervous System Manifestations
Central nervous system (CNS) involvement results in a spectrum of neurologic sequelae. Typically neurologic issues present in the second and third decade but have presented as early as 6 years of age [40]. Kaiser Fleischer rings are typically found in patients with CNS symptoms, but not always. Onset of symptoms is gradual and progressive. Typical presentation includes tremors and difficulty with fine motor tasks. As the disease progresses, patients may develop masklike facies, rigidity, and gait disturbances. Cognitive decline is also documented. Psychiatric disturbances occur in up to 25 % of patients. Many patients are given a psychiatric diagnosis prior to identification of WD. Manifestations can include anxiety, affective disorders, depression, compulsive behaviors, phobias, aggression, poor school performance, and even psychosis [47, 48].
Ophthalmologic Manifestations
Kayser-Fleischer (KF) rings are associated with WD, but are not limited to WD. KF rings are described as golden brown, brownish green, bronze, tannish green, and greenish yellow in the zone of Descemet’s membrane in the limbic region of the cornea (Fig. 9.2). KF rings can be appreciated on gross exam, but slit-lamp examination is required for confirmation. The rings represent deposited copper granules throughout the layers of the cornea. They may be found in asymptomatic patients [48] and fade with treatment. Sunflower cataracts can be seen in WD [53]. These are a greenish gray or golden disk in the anterior capsule of the lens with spokes radiating to the lens periphery and resolve with therapy [48].

Kayser-Fleischer ring indicated by the solid black arrow
Renal Manifestations
Renal involvement is characterized by proximal tubular dysfunction and is common in WD. This results in aminoaciduria, glycosuria, and increased excretion of uric acid (with resultant low serum uric acid levels) and calcium, as well as a decrease in filtration rate. Many WD patients are unable to acidify their urine resulting in potassium loses and hypokalemia [54]. The combination of inadequate acidification and hypercalciuria results in the common occurrence of renal stones [48]. Renal function improves with therapy [48].
Cardiac Manifestations
In a study of 53 WD patients [55], 34 % percent demonstrated electrocardiographic (ECG) abnormalities to include left ventricle hypertrophy, ST depression, premature ventricular contractions, sink atrial block, T-wave inversion, and atrial fibrillation. Compared to a control population, there was an increased rate of arrhythmia, which may be associated with sudden death [50, 55].
Other Manifestations
Bone, hemolytic, endocrine, reproductive, and biliary abnormalities are also found. The skeletal changes include osteoporosis, rickets, osteomalacia, spontaneous fractures, and osteoarthritis [48]. Demineralization is the most common abnormality resulting from hypocalcemia and hyperphosphatemia [48]. Hemolysis is another common issue which can be transient or progress to chronic anemia [48]. Endocrine dysfunction presents as hypothyroidism and hypoparathyroidism [47]. Reproductive issues include infertility and increased frequency of miscarriage [47].
Diagnosis
The diagnosis can be made in the face of the classic triad of hepatic disease, neurologic symptoms, and KF rings (see Table 9.4). If this triad does not exist, there is no single test that is 100 % sensitive and specific, especially in children. A high index of suspicion, combined with a complete history and physical exam, as well as laboratory and genetics studies is used in diagnosis. Physical exam may demonstrate findings of chronic liver disease including fluid retention, ascites, jaundice, hepatic encephalopathy, and hepatosplenomegaly.
Ferenci incorporated comments on the Leipzig score to create a scoring system for diagnosis that includes clinical symptoms, laboratory findings, and mutational analysis [46, 57]. Points are assigned for presence of KF rings, neurologic symptoms, low serum ceruloplasmin levels, anemia, liver copper, urine copper, and presence of mutations. A score of greater than 4 establishes diagnosis and greater than 3 requires mutation analysis for confirmation (Table 9.4) [46]. Two recent studies in pediatric patients retrospectively identified 53/54 and 55/57 WD patients with this tool [51, 58]. Another retrospective study identified 28/30 asymptomatic WD patients [59].
The score is not needed in straightforward cases. This would include a patient with extrapyramidal symptoms, KF rings, and typical labs (low ceruloplasmin, high urine copper excretion) and, similarly, a patient with evidence of hepatic disease with KF rings and typical labs (low ceruloplasmin, high urine copper excretion). However, clinical symptoms and KF rings are not always present. It is in these cases the scoring system assists with diagnosis.
Laboratory Testing
Serum ceruloplasmin is decreased (<20 mg/dL) in 95 % of patients presenting with WD [47]. Decreased levels are not specific for WD and may represent other conditions associated with decreased hepatic synthetic function, protein loss, and hereditary hypoceruloplasmin [48]. Ceruloplasmin is an acute phase reactant and may be normal in patients with WD at times of hepatic inflammation [47].
Evaluation of urinary copper excretion, which is normally less than 100 μg/24 h, is also used in diagnosis. In WD urine copper excretion is typically greater than 100 μg/24 h and can increase into the thousands but may be normal in asymptomatic patients. Using a level of 40 μg/24 h increases the sensitivity in children [47]. Elevation of urinary copper excretion may also be found in other causes of cholestasis [49]. Urinary copper excretion is also used to document effectiveness of chelation treatment, with increasing levels identifying successful therapy. One retrospective study found that a ceruloplasmin less than 20 mg/dL and urinary copper greater than 40 μg/24 h in an asymptomatic child diagnosed WD with a sensitivity of 95 % and a specificity of 84.5 %. The positive predictive value was 93 % and the negative predictive value was 91.6 % [59]. Children with normal urinary copper excretion in whom there is still suspicion of WD may require a d-penicillamine challenge.
Serum copper concentrations are useful in the diagnosis. Serum copper levels can be used to follow therapy with a goal level of 5–15 μg/dL during chelation.
Liver functions are also helpful in identifying patients with possible hepatic WD, but are generally not specific enough for diagnosis. Typically serum transaminases remain elevated and the alkaline phosphatase is low, and some authors have suggested a high specificity for WD with an elevated AST:ALT ratio and alkaline phosphatase elevation to total bilirubin ratio in acute liver failure [47, 60].
Genetic testing can be very useful in the confirmation of diagnosis. Molecular genetic testing is utilized in asymptomatic siblings where the mutation(s) in the affected sibling is known. Testing for common mutations is recommended in cases of nonfamilial WD, as direct sequencing is costly and time consuming.
Liver Pathology
Liver biopsy for quantification of hepatic copper is included in the scoring system. Hepatic copper measurement of >250 μg/g dry weight is consistent with WD, while <50 μg/g dry weight excludes WD [48]. Some experts recommend using levels of greater than 75 μg/g of dry liver tissue for diagnosis to increase sensitivity. Elevated hepatic copper may be seen in normal healthy infants less than 6 months of age, cholestasis, cirrhosis, and cholangitis [48].
Liver histology is also helpful in diagnosis with changes seen even in the very young. Cirrhosis has been identified as early as 5 years of age [61]. Fat deposition is seen early in the disease with progression to steatosis. Evidence of chronic active hepatitis is seen with fibrosis leading to cirrhosis. Periportal glycogenated nuclei are found in liver biopsies in WD (Fig. 9.3a). Copper stores are seen in less than 10 % of patients, despite special stains (rhodanine, Fig. 9.3b) [44]. Positive staining is a factor in the scoring system.

(a) Periportal glycogenated nuclei (solid black arrows) in a liver biopsy from a patient with Wilson disease. (b) Rhodanine stain of a liver biopsy from a patient with Wilson disease demonstrating positive staining (black arrows)
Ophthalmologic Evaluation
Slit-lamp examination for KF rings is supportive of a diagnosis, but not pathognomonic. KF rings are seen in approximately 50 % of patients with hepatic involvement and 95 % of those with neurologic and psychiatric presentations. KF may also be seen in chronic hepatitis, primary biliary cirrhosis, and intrahepatic cholestasis [53, 56]. KF rings are rarely seen in children younger than 7 years [51].
Neurologic Examination
A thorough neurologic exam and imaging of the brain (CT or MRI) should be considered in all patients with suspected or confirmed WD. A baseline neurologic assessment is helpful while following response to therapy. MRI and CT may identify changes in the basal ganglia, pons, or thalamus suggesting the diagnosis [47].
Screening of Asymptomatic Relatives
Siblings have a 1 in 4 chance and children of a WD parent have a 1 in 180 chance of inheriting the disease [47]. It is recommended that asymptomatic relatives have a thorough screening at 3 years of age [52]. This includes a complete history and physical exam and ophthalmologic slit-lamp exam along with measurement of serum ceruloplasmin, serum copper, and 24-h urinary copper excretion and evaluation of transaminases. The likelihood of diagnosis with all the testing returning normal is exceedingly small. If any of the testing returns abnormal, further testing with a liver biopsy for quantification of copper and histology is prudent. Genetic testing is recommended to confirm diagnosis.
Treatment
Therapy for WD is lifelong (See Table 9.5). Treatment may vary between initial therapy and maintenance therapy following successful de-coppering. Foods high in copper (shellfish, grains, nuts, mushrooms, legumes, chocolate, and organ meats) should be avoided. The three therapies are d-penicillamine, trientine, and zinc salts [47, 48]. d-penicillamine and trientine chelate copper allowing urinary excretion. Dosage is slowly increased to maximize chelation and then reduced to a maintenance therapy. Significant improvement is seen within weeks of starting therapy. Neurologic symptoms may initially worsen with treatment of d-penicillamine, due to mobilization of large amounts of copper and subsequent deposition in the brain. d-penicillamine has more side effects that lead to therapy changes (Table 9.5). Trientine is typically better tolerated and may have a lower risk of neurologic worsening. Zinc functions as an antagonist to intestinal copper absorption [48]. Zinc increases intestinal metallothionein, leading to copper binding and retention in the intestinal cell which is sloughed with the stool. It takes 2 weeks to increase intestinal metallothionein levels, and thus zinc is not a good option in symptomatic patients. To be most effective, zinc should be taken at least 1 h away from meals at least three times a day. The newest experimental therapy is ammonium tetrathiomolybdate with two anti-copper mechanisms, reduced absorption and decreasing availability due to binding. The complications and side effects are significantly less than d-penicillamine.
Long-term and comparative studies of the various available therapies are lacking, making the selection of therapy challenging despite the safety profiles. Weiss did directly compare zinc to chelators in patients with neurologic disease and found zinc to have a higher rate of worsening liver function tests and decreased urinary copper excretion [44]. Future prospective trials are needed to determine the best therapies for patients with neurologic and hepatic predominant disease.
Urine copper levels can be used to monitor success in all three therapies. With chelation therapy, urinary copper excretion should rise. Tapering the dose of the chelator to maintenance levels or converting to zinc should only be considered when the urinary copper excretion subsequently declines. With zinc therapy, copper removal is slower and will not rise but should eventually decline. Spot urine zinc can be used to assess compliance. A small study of 16 children with WD who received trientine found that 10/16 had improvement in LFTs. Thirteen of 16 continued on trientine with 1 stopping for allergic reaction, 1 with low copper excretion, and 1 going to transplant [62].
Liver transplantation is indicated in WD patients who have (1) acute liver failure and (2) severe hepatic decompensation not responding to therapy and (3) responded to d-penicillamine but have developed severe progressive hepatic insufficiency with therapy discontinuation [35, 58, 63]. Transplantation changes the hepatic genotype and improves copper excretion. The role of transplant in severe neurologic disease is unclear. Survival following transplant is good. Patients will experience normalization in serum copper and ceruloplasmin as well as 24-h urinary copper excretion 1–2 months following transplant [48].
Natural History and Clinical Outcome
The prognosis is excellent for patients with early diagnosis who are compliant with therapy. Similarly, patients with mild symptoms will likely experience improvement with therapy. Patients with neurologic symptoms may have initial worsening in the first 4 weeks of therapy due to initial increases in serum copper levels. In patients with significant neurologic and psychiatric manifestation, studies show a slow progressive benefit over 3 years or longer. Two recent studies with long follow-up found that on therapy, 61–76 % of subjects remained clinically stable and 2–18 % progressed, with few deaths associated with WD [43, 44, 64]. Patients are more likely to have progression associated with neuropsychiatric involvement than liver involvement [43, 44, 64]. King’s College studied 74 children with WD including 57 with liver disease and 17 asymptomatic siblings. Of this group 32 remained on long-term chelation, 10 had liver transplants, and 15 died from acute liver failure (10 days or less from symptoms to death) [58]. There is a revised prognostic index score that is used to predict response to treatment. The score is based on serum bilirubin, INR, AST, white blood cell count, and albumin (scores 0–20). A pediatric evaluation predicted favorable response to chelation in children with a score of less than 11. Those with scores of greater than 11 died without transplant [58].
Summary
Wilson disease is an autosomal recessive disease of copper metabolism with dysfunction of the P-type ATPase, ATP7B, copper transporter. This results in copper overload and injury to multiple organ system but most notable the CNS and liver. Presentation varies significantly in both time course and severity. Diagnosis is complex and based on several laboratory studies. Liver biopsy adds both copper content and histology to assist with the diagnosis. There is a scoring system that is showing increasing promise for the diagnosis of WD. There are currently three main medical therapies with few large studies or comparative studies to direct therapy selection. A revised scoring system can assist with selection of medical therapy versus transplantation and has been shown to be predictive in children. Liver transplant is curative.
Cystic Fibrosis Liver Disease
Cystic fibrosis (CF) is a common lethal genetic disease in the North American population, affecting 1:2,500 births. There are about 30,000 individuals in the USA with CF and approximately 1,000 new cases annually. Although pulmonary-related factors are the most common cause of death in CF [65–67], liver disease is the third leading cause of death, accounting for 2.5 % of overall mortality [68, 69].
The liver is likely involved to some degree in all individuals with CF; however, clinically significant liver disease (multilobular cirrhosis with or without portal hypertension) only occurs in 5–10 % of individuals.
The term cystic fibrosis liver disease has been commonly used. However, there have been variable definitions of this entity, and this has led to confusion about the natural history, clinical impact, and outcome of liver disease in CF. We prefer to use the following classification of liver involvement in CF put forth at a CF Foundation Williamsburg conference. In this scheme, advanced liver disease is reserved for CF-related liver disease with cirrhosis with or without portal hypertension, based on clinical examination, imaging, or histology. Other liver disease is classified as liver involvement without cirrhosis/portal hypertension. The various indications of this could include one or any combination of persistent or intermittent AST, ALT, or GGT >2 times upper limit of normal; hepatic steatosis as determined by liver biopsy or imaging; hepatic fibrosis as determined by liver biopsy; cholangiopathy demonstrated by MRCP or ERCP; and other ultrasound abnormalities not consistent with cirrhosis.
The definitions, clinical presentations, and prevalence data for each of the categories are described below.
Cystic Fibrosis-Related Cirrhosis with and Without Portal Hypertension
Multilobular Cirrhosis
Multilobular cirrhosis is indicated by the presence of multiple regenerative nodules and diffuse involvement of the liver. On physical exam a hard nodular liver that may or may not be enlarged detects multilobular cirrhosis. On imaging, there is an irregular nodular liver edge and coarse heterogeneous parenchyma. Prior to the development of portal hypertension, there are often no other clinical features. Once portal hypertension is present, splenomegaly, esophageal or gastric varices, or ascites may be the first suggestion of previously unsuspected cirrhosis. Liver biopsy can show features consistent with cirrhosis but may not be sensitive due to the patchy nature of the nodular involvement and the large regenerative nodules that can be mistaken for normal hepatic parenchyma. Multilobular cirrhosis in CF is a pediatric disorder. The median age of discovery is 10 years with very few new cases identified after 20 years of age, and no increased prevalence with increased life span. The prevalence of cirrhosis and its complications have been reported in multiple studies that include 4,446 subjects from Europe, Canada, Australia, and Israel in the last 20 years. In total, there was an average prevalence of multilobular cirrhosis of 5.6 % portal hypertension 4.2 % and varices 2.4 % [68, 70–80].
Portal Hypertension Without Cirrhosis
Non-cirrhotic portal hypertension has been reported in CF [78, 81, 82].
Complications of Cirrhosis with Portal Hypertension
The primary complications of CFLD are restricted to individuals with multilobular cirrhosis with portal hypertension and include the complications expected in portal hypertension with hypersplenism and esophageal or gastric variceal hemorrhage the predominant issues. Variceal hemorrhage occurs in 40–50 % of patients and may occur even more frequently as survival with CF continues to improve. Hepatic decompensation is rare and appears much more slowly than in primarily hepatocellular diseases. Ascites is a late and ominous complication, and synthetic liver failure with coagulopathy is very rare. While liver disease is listed as the third leading cause of death among CF patients, some studies report no increase in mortality among patients with multilobular cirrhosis [70, 76, 77]. Two recent studies report a trend towards younger age of death in those with cirrhosis [80, 83]. In a large 18-year retrospective review of 1,108 patients with CF, 53 developed cirrhosis, 23 with portal hypertension, 14 with varices, 8 with coagulopathy, and 6 with overt liver failure resulting in 3 liver transplants, but only one reported liver-related death [73]. The incidence rate of major complications of cirrhosis (bleeding, ascites, encephalopathy) among a cohort of 177 CF patients (17 who developed cirrhosis) followed longitudinally was 0.4 %, with an all-cause mortality rate of 1.6 % among cirrhotic patients [70]. This is in contrast to older reports that showed 11–19 % mortality from variceal bleeding or liver failure in CF cirrhosis [84]. Once portal hypertension develops in CFLD, some studies report an increased risk of malnutrition, osteoporosis/hepatic osteodystrophy, and decline in lung function. However, a recent retrospective study of 59 CF patients with cirrhosis and portal hypertension found no decline in lung function associated with portal hypertension as compared to age- and gender-matched CF-specific reference values for lung function [85]. Malnutrition associated with portal hypertension is likely multifactorial with decreased nutrient absorption, increased resting energy expenditure, anorexia, and decreased caloric intake. There may be a link between CFLD and increased insulin resistance leading to a higher incidence of CF-related diabetes [86]. A single-center retrospective case-control study showed an odds ratio of 4.8 (95 % CI 2.49, 9.17) for CF-related diabetes in those with cirrhosis and portal hypertension, using a surrogate marker (thrombocytopenia) for cirrhosis with portal hypertension [87]. A case-control study of CF patients with and without CFLD found lower weight, height, and mid-upper arm circumference and lower FEV1 scores in CFLD patients [88].
Liver Involvement Without Cirrhosis or Portal Hypertension
There are a variety of other forms of liver involvement in CF. Some of these may occur together in individual patients.
Focal Biliary Cirrhosis
FBC is primarily a histologic diagnosis. Autopsy data has demonstrated liver involvement in 25–72 % of adults with CF, with the majority showing focal biliary cirrhosis [89, 90]. FBC has been found on postmortem exam in 11 % of infants, 27 % at 1 year, and 25–70 % of adults [89, 90]. It is the pathognomonic histopathologic liver lesion in CF and is often clinically silent without abnormalities in AST, ALT, or GGT. On ultrasound, there are thickened (>2 mm), hyperechoic periportal tissues. On MRI, there is high-intensity signal in the periportal area on T1-weighted imaging [91]. On liver biopsy, FBC is characterized by focal portal fibrosis and inflammation, cholestasis, and bile duct proliferation. It has been suggested that FBC is part of the progression to multilobular cirrhosis, but given the much lower frequency of multilobular cirrhosis compared to FBC, the progression is very rare [68, 70–72, 74–79].
Elevations in AST, ALT, and/or GGT
Forty to 50 % of CF patients have intermittent elevations in AST, ALT, or GGT that are not predictive of the development or presence of significant fibrosis. In a longitudinal study of over 250 children identified by newborn screen in Colorado, followed for up to 20 years, 90 % had at least one abnormal ALT and 30 % had persistently (>6 months) elevated ALT. Persistent elevations of AST, ALT, or GGT more than 3 times the upper limit of normal were very rare [92]. In a study of 376 children in 3 clinical trials with frequent determination of biochemistries, 25 % had emergence of at least one abnormal AST, ALT, or GGT over an average of 8 months of follow-up [93]. Persistently elevated ALT or GGT (for more than 6 months) are common and warrant further investigation but are not diagnostic of any particular disorder [94].
Hepatic Steatosis
Steatosis is likely the most common hepatic finding in CF with a prevalence of 23–75 % of CF patients in all age categories [95]. Steatosis was present in 70 % of children undergoing liver biopsy for suspected liver disease [76, 81]. Hepatic steatosis has been associated with malnutrition and deficiencies of essential fatty acid, carnitine, and choline. However, steatosis is also found in CF patients with adequate nutritional status [69]. It presents as smooth mild hepatomegaly without signs of portal hypertension. The appearance on ultrasound is typically uniform hyperechogenicity, but it may also have a heterogeneous appearance on ultrasound or as one or several “pseudomasses,” which are lobulated fatty structures 1–2 cm in size [96, 97]. In one study, 57 % of cases of steatosis detected on ultrasound were associated with elevation in aminotransferases [98].
Biliary Tract Disease
Cholangiopathy
Magnetic resonance cholangiography (MRC) demonstrates abnormalities in the intrahepatic bile ducts in a significant number of CF patients, with stricturing, beading, and areas of narrowing and dilatation similar to primary sclerosing cholangitis [96]. MRC-detected intrahepatic biliary anomalies were reported in 69 % of CF patients regardless of laboratory or clinical evidence of liver disease, with isolated or multiple dilations in the biliary tree noted [99].
Cholestasis
This is the earliest manifestation of liver involvement in CF and may mimic biliary atresia. Less than 2 % of infants with CF present with neonatal cholestasis. In a large study of infants with cholestasis, only 9 of 1,474 (0.6 %) had CF as their etiology, so it is an uncommon cause of neonatal cholestasis [100]. Liver biopsy can mimic findings seen in biliary obstruction and can be confused with biliary atresia. Meconium ileus is a known risk factor for the development of cholestasis [69, 95, 97]. While cholestasis generally resolves within 3 months with no sequelae, some studies have suggested an increased risk for cirrhosis in children with meconium ileus [68, 70, 71].
Gallbladder Involvement
Gallbladder abnormalities are found in 24–50 % of CF patients by US, MRI, or MRC. Microgallbladder is reported in 5–45 % of CF patients and 3–20 % have gallbladder distention and evidence of gallbladder dysfunction. Older studies reported that gallstones develop in 3–25 % of pediatric CF patients [95, 96, 101]. These stones are more commonly calcium bilirubinate stones [102]. Coinheritance of the Gilbert syndrome-associated UGT1A1 mutation appears to increase the risk for gallstones in CF [103]. Cholecystectomy is indicated for the management of symptomatic cholelithiasis. Calcium bilirubinate stones do not respond to ursodeoxycholic acid treatment. No treatment is required for microgallbladder.
Pathogenesis
The pathogenesis of CF liver disease is largely unknown. In the liver, CFTR is localized to the apical surface of bile duct epithelium and is not found in hepatocytes [104]. CFTR in biliary epithelium increases apical biliary chloride secretion primarily increasing bile acid-independent bile flow. In the pancreas and lung, CFTR is similarly located in the apical epithelium. These organ systems are affected to varying degrees by a dysfunctional or absent chloride channel leading to thickened mucus secretions and plugging. A similar pathologic mechanism has been suggested in the liver, with inspissated bile leading to obstruction of small intrahepatic bile ducts, subsequent inflammation, and progression to fibrosis.
Screening for Liver Disease
The goals of screening for liver disease in CF are twofold. The first would be to identify individuals at risk for cirrhosis prior to its development in order to institute therapy to prevent or reduce progression to cirrhosis. The second would be to detect patients who have developed clinically silent cirrhosis to allow monitoring and interventions to reduce or mitigate complications.
No tests reliably identify individuals with CF who are at high risk for the development of cirrhosis. In contrast, several methods have shown promise for the detection of clinically silent cirrhosis. A combination of physical examination for hepatomegaly, annual testing of AST/ALT and GGT, and abdominal imaging (ultrasound, CT, or MRI/MRC) has been thought to hold the best promise for detecting clinically relevant liver disease in CF (cirrhosis with or without portal hypertension or advanced hepatic fibrosis). However, these tests are not sensitive for early stages of hepatic fibrosis or the identification of individuals who are at high risk for cirrhosis. In a prospective cohort study of CF patients with suspected CFLD, dual-pass core-needle liver biopsy increased the sensitivity of the detection of hepatic fibrosis by 22 % compared to a single-pass liver biopsy. In that study, the finding of more advanced hepatic fibrosis was the only factor independently associated with the future development of portal hypertension. Clinical exam, ultrasound, and ALT were not predictive of development of portal hypertension. Clinical hepatomegaly and ultrasound abnormalities were found to be sensitive, but not specific, and ALT elevation specific but not sensitive for the detection of advanced fibrosis on biopsy [81].
The CF guidelines from 1999 recommend an annual physical exam for liver span and texture, spleen size, and annual AST, ALT, and GGT determination but contained no definitive recommendations on screening imaging or liver biopsy. A recent best practice guideline paper from the European Cystic Fibrosis Society recommends hepatic ultrasound for patients with persistent elevation of AST, ALT, or GGT on three consecutive occasions over 12 months and/or clinical hepatomegaly or splenomegaly. They proposed that abnormalities in ultrasound could be followed by liver biopsy [94].
Liver biopsy remains the “gold standard” for the detection and staging of hepatic fibrosis and the diagnosis of cirrhosis. The risks, cost, and lack of ability to perform serial measurements with liver biopsy in large part explain the emphasis on developing reliable and validated noninvasive tests for liver disease in CF.
Routine liver biochemistries are unreliable as indicators of cirrhosis or the risk of development of cirrhosis. Several studies have suggested the use of serum markers of hepatic fibrogenesis for early detection of CF liver disease, such as TIMP-1, collagen type IV, prolyl hydroxylase, and glutathione s-transferase [105–108].
Radiologic Imaging
The three main imaging modalities: ultrasound, CT, and MRI can detect cirrhosis with or without findings of portal hypertension [109]. Ultrasound can demonstrate multilobular nodularity indicative of cirrhosis but is unreliable at detecting earlier stages of hepatic fibrosis. Steatosis and hepatic fibrosis may be indistinguishable. Children with normal hepatic ultrasounds can have advanced fibrosis [76]. In a single-center study, the ultrasound finding of hyperechogenicity was associated with an increased risk for the development of multilobular cirrhosis [75]. However, ultrasound heterogenicity can be intermittent [75], and consistency in interpretation of echogenicity and homogeneity may be center dependent leading to increased interobserver variability [75, 98, 110]. However some centers perform serial routine abdominal ultrasound to detect early imaging abnormalities such as parenchymal heterogeneity that may indicate an increased risk for progression to cirrhosis [75].
Acoustic Transient Elastography
Acoustic transient elastography uses a low-frequency acoustic wave transmitted through the liver via a probe placed on the skin over the liver. The velocity of the wave propagation is directly proportional to the stiffness of the liver due to its collagen fiber content. There are limited studies of elastography in CF. Two studies of children and adults with CF found increased liver stiffness in clinical and biochemical CFLD and elastography compared favorably to ultrasound for the detection of advanced fibrosis [108, 111]. Two studies in CF found a good correlation between transient elastography values and the presence of esophageal varices [108, 112].
Acoustic Radiation Forced Impulse Imaging
Acoustic radiation forced impulse imaging (ARFI) uses ultrasound to measure liver stiffness and shear wave velocities. A potential advantage is that ARFI may not be influenced by hepatic steatosis [113, 114]. Initial studies show a good correlation with transient elastography. One report in a small cohort of CF subjects suggests that ARFI is similar to transient elastography [115].
Treatment and Outcome
To date, there is no effective therapy in CF to prevent or treat fibrosis. Thus, most efforts are directed at supportive care and management of complications.
Infants
Infants with cholestasis and prolonged jaundice are at risk for malnutrition, fat-soluble vitamin deficiency, and growth failure. This risk is higher in those infants who have undergone bowel resection. Close monitoring of growth and fat-soluble vitamin status with institution of higher-calorie feedings and fat-soluble vitamin supplementation is often required. Ursodeoxycholic acid (UCDA) increases bile flow and has been used in this setting despite the lack of published evidence in this age group.
Children and Adults
In older children and adults with CF and cirrhosis, the main issues in care are screening for and management of complications of portal hypertension (splenomegaly, ascites, varices) and optimization of their nutritional status and lung function.
Ursodeoxycholic Acid
UDCA at present is the only therapy available that may possibly prevent or delay progression of CFLD. It increases bile flow, may replace potentially toxic bile acids, acts as a cytoprotective agent, and possibly stimulates bicarbonate secretion in the biliary tract [116–118]. UDCA at 15–20 mg/kg/day has been shown to improve AST and ALT, bile drainage, liver histology, and nutritional and essential fatty acid status in CF liver disease. However, a 2000 Cochrane review on the use of UCDA in CF found few suitable randomized trials assessing UDCA efficacy, and there have not been any randomized studies conducted since that review [119]. They concluded data are insufficient to justify routine use in CF, and no data on impact of UCDA on death or liver transplant are available. In summary, there is significant disagreement about the use of UDCA in CF [94, 118, 120]. There is no well-controlled randomized study of UDCA in CF and no strong evidence for benefit or harm in CF. Further study is needed to clarify the potential role of UDCA in CF. Other potential therapies such as essential fatty acid supplementation and antioxidants have not been sufficiently investigated to provide any recommendations.
Management of CF Cirrhosis with Portal Hypertension
Screening
Standard follow-up for sequelae of cirrhosis is appropriate in CF. There is some evidence for an increased risk of GI cancers in CF [121], but not hepatocellular carcinoma (HCC), although there are isolated case reports of HCC [122].
Esophageal and Gastric Varices
In CF patients with cirrhosis, varices have been reported to be present in anywhere from 30 to 100 % [68, 70–73, 77]. In total these studies reported on 3,057 patients with CF with 111 patients (3.6 %) with cirrhosis identified of whom 54 (48 %) had varices. The risk of variceal bleeding in CF cirrhosis has not been well studied. In two studies of a total of 67 patients with CF and cirrhosis, 28 (42 %) developed variceal hemorrhage [80, 84]. There have not been any studies of primary or secondary variceal prophylaxis in CF. Transjugular intrahepatic portosystemic shunt (TIPS) has been used in CF and reported in case reports and one small case series [123]. TIPS is effective in management of variceal bleeding in CF and can stabilize patients for over 5 years. Some authors have used partial splenic embolization or partial or total splenectomy in an attempt to reduce portal venous flow and improve thrombocytopenia [124, 125]. Indeed, partial splenectomy with splenorenal shunt had favorable outcome in 15 of 19 CF patients with portal hypertension, with improvement in liver function and portal hypertensive symptoms, significantly delaying or obviating the need for liver transplantation [124].
Ascites
The development of ascites represents a poor prognostic sign and is indicative of relative hepatic decompensation and the need for evaluation for possible liver transplant. Diuretics such as furosemide or spironolactone may be utilized as first-line therapy in concert with a salt- and fluid-restricted diet in attempts to decrease the ascitic fluid load. However, care must be taken to not overly restrict salt in CF, as hypochloridia may result especially in the summer months.
Liver Transplantation
Liver Transplantation Which patients with CF and cirrhosis require liver transplant and optimal timing of transplantation remains a controversial subject. Reserving liver transplant only for those with liver synthetic failure (a relatively rare late event in CF cirrhosis) versus early transplantation following the development of portal hypertensive complications varies by center. The established indications for liver transplant in CF include cirrhosis with evidence for hepatic decompensation or uncontrollable variceal bleeding. Some authors feel that evaluation and transplantation should occur earlier in the disease course, before lung function is severely compromised when outcomes are likely to be better [126, 127]. The relatively preserved hepatic synthetic function in the CF cirrhosis population affects prioritization for liver transplant, and clear guidelines on selection of CF patients for liver transplantation are lacking, although a scoring system has been proposed [128].
Of 203 liver transplants in CF patients performed in the USA from 1987 to 2008, 148 were performed in children. There was a significant survival advantage in both adults and children with CF cirrhosis receiving liver transplant compared to those with cirrhosis who did not receive a transplant, with further survival advantage in children compared to adults [129, 130]. Outcomes of liver transplant in CF have generally been favorable with 1-year patient and graft survival (89 %/83 %, respectively), and 5-year patient survival rates (85.8 %) are not significantly different than non-CF liver transplant patients [130, 131]. However, for CF patients without liver synthetic failure or intractable GI bleeding, their 1-year survival without transplant would likely be higher. In Europe, the median age of CF liver transplant recipients was 12 years and the 3-year survival was approximately 80 % [132]. Thus pediatric CF patients in the USA and Europe who undergo liver transplant experience survival rates similar to the 5-year unadjusted survival rates of 86 % in US non-CF pediatric liver transplant recipients [130].
Relative contraindications to an isolated liver transplant in CF include infection with multidrug-resistant organisms (Pseudomonas, Burkholderia), poor pre-transplant pulmonary function (FEV1 <50 % predicted) and/or elevated resting arterial pCO2, extensive pulmonary fibrosis on imaging, and severe pulmonary hypertension [132, 133]. Short-term improvements in lung function are reported in pediatric patients following liver transplant, and poorer lung function prior to surgery is associated with mortality risk [133]. Small single-center series have reported both favorable [127] and unfavorable pulmonary function outcomes following liver transplantation [134]. A recent analysis of the CF registry found no difference in the rate of decline in FEV1 in the 3 years following liver transplant in the CF subjects who underwent liver transplant compared to CF controls without liver disease [135]. This suggests that liver transplantation does not lead to a significant long-term change in pulmonary outcome. The effect of liver transplant on the nutritional status of CF patients is also uncertain, with reports of improvements [136, 137] and reports of no improvement [135].
Combined lung and liver transplant may be considered in patients with cirrhosis and portal hypertension and extensive pulmonary fibrosis, lower FEV1, and resting hypercapnia. Eleven CF patients underwent combined liver-lung transplantation between 1987 and 2004 in the USA. The median age was 15 years, and 1-, 3-, and 5-year patient survival rates were 79, 63, and 63 %, respectively [138]. Eleven combined liver-pancreas transplants in CF patients with cirrhosis and CFRD were performed between 1987 and 2010, with 100 % 5-year survival reported in follow-up of 7 patients, with no further requirement for exogenous insulin or pancreatic enzyme replacement therapy [131].
Hemochromatosis and Hemosiderosis
Iron overload states can be classified as primary or secondary. There are many disorders that can lead to iron overload (Table 9.6). This discussion will focus on hereditary hemochromatosis (HHC), juvenile hemochromatosis (JHC), and secondary iron overload (primarily transfusion associated) in the pediatric patient. For a discussion of the rarer entities, the reader is referred to a recent review [140].
Physiology and Pathophysiology of Iron Overload
Iron is one of the more tightly regulated nutrients in the body. Humans have no significant excretory pathway for iron. Iron stores are normally controlled at the level of absorption, matching absorption to physiologic requirements. Under normal circumstances, only about 1 mg of elemental iron is absorbed per day, in balance with gastrointestinal losses. Intestinal iron absorption is increased by low body iron stores (storage regulation), increased erythropoiesis (erythropoietic regulation), anemias associated with ineffective erythropoiesis (thalassemias, congenital dyserythropoietic anemias, and sideroblastic anemia), and acute hypoxia. Both dietary iron intake (dietary regulation) and systemic inflammation can temporarily decrease iron absorption and availability, even in the presence of iron deficiency [141].
Iron is absorbed in the duodenal and proximal jejunal enterocytes via divalent metal transporter 1 (DMT-1), where it is either stored as ferritin or moved across the basolateral membrane to reach the plasma, where it is bound to transferrin. The regulation of iron status hinges on hepcidin and ferroportin. Hepcidin is produced in the liver and is elevated in iron-sufficient states. High levels of hepcidin decrease intestinal iron absorption [142, 143]. When hepcidin is low, iron absorption is increased. Mutations in both the hepcidin (juvenile hemochromatosis) and ferroportin (autosomal dominant hemochromatosis) genes have been described [144]. Hepcidin expression is regulated by the HFE protein (mutated in HHC type 1), transferrin receptor 2 (TfR2 mutated in some forms of iron overload), and hemojuvelin (mutated in juvenile hemochromatosis). In animal models and in humans with hemochromatosis, the normal increase in hepcidin expression with iron loading is lost, leading to lower hepcidin levels and continued iron absorption in the face of iron overload [139].
In humans, iron in the circulation is tightly bound to transferrin. Diferric transferrin binds to the transferrin receptor on the cellular plasma membrane. This complex is then endocytosed into the cell, where iron is released by the acid environment of the endocytic vesicle. The iron is then transported across the endosomal membrane to the cytoplasm. In iron overload states, more of transferrin is in the diferric state, or the more readily absorbable state. The uptake of iron is primarily regulated by the expression of the transferrin receptor on the cell surface. In iron deficiency, iron regulatory proteins are increased and upregulate expression of transferrin receptor 1 increasing iron uptake and decrease the synthesis of ferritin. In states of iron repletion or excess, there is a reduced level of iron-binding proteins, leading to less transferrin receptor production and an increase in ferritin and hepcidin synthesis.
A second transferrin receptor (TfR2) binds holotransferrin/diferric transferrin and mediates the uptake of transferrin-bound iron. TfR2 is predominately expressed in the liver, where, in contrast to TfR1, it is not downregulated by dietary iron overload. Hepatic TfR2 provides an explanation for the continued hepatic iron uptake in HHC despite the downregulation of TfR1. TfR2 also regulates hepcidin synthesis in the liver.
In HHC and JHC, net iron absorption is increased above endogenous losses. In addition, in both disorders, there is loss of the normal downregulation of iron absorption as iron accumulates in the body. This is directly related to inhibition hepatic hepcidin expression by the mutations in the hepcidin regulatory proteins responsible for HHC and JHC [139, 144]. The result is a gradual increase in total body iron. In HHC, the net increase in total body iron has been estimated at 4–7 mg/day. The increased iron absorption in HHC is the result of inappropriate transfer of iron in the intestine due to suppression of hepatic hepcidin secretion [144]. In JHC, iron accumulates more rapidly than in HHC, due in part to the more significant role of hemojuvelin in the regulation of hepcidin [145]. Excessive iron intake in the diet can accelerate the accumulation of iron in both HHC and JHC. In a similar manner, increased iron losses (most commonly in menstruating females) can slow the accumulation of iron. In secondary iron overload due to hemoglobinopathies, iron overload is related to both the anemia and increased iron absorption and excess iron provided by transfusions. In contrast, in aplastic anemias, iron overload is primarily related to transfusion.
Genetics of Hereditary Hemochromatosis
Hereditary hemochromatosis is an autosomal recessive disorder due to a mutation in HFE [146]. The HFE gene encodes a novel major histocompatibility (MHC) class 1-like molecule. Two principal missense mutations of HFE have been identified (C282Y and H63D). Upward of 85–90 % of patients with classic HHC are homozygous for C282Y, and another 5 % are compound heterozygotes (C282Y/H63D). The H63D mutation is quite common (15–20 % heterozygote state in the general population), but H63D homozygotes generally do not have iron loading. Ten to 15 % of patients with a clinical syndrome of typical HHC do not have either the C282Y or H63D mutation. However, 55 % of patients initially felt to have HHC who carried neither mutation were found to have previously unrecognized causes for secondary iron overload. There remains a small subgroup of HFE mutation-negative iron-overloaded patients with typical HHC. Some of these patients have mutations in other hepcidin regulatory proteins. Several new mutations in HFE have been described in patients with iron overload, suggesting that other HFE mutations may be found in “wild-type” HHC.
HFE is widely expressed throughout the body; the highest levels are found in the liver and small intestine. HFE is involved in an as yet unknown complex regulation of hepcidin secretion, with subsequent lack of hepcidin mRNA expression and secretion in the face of excessive total body iron stores [147].
Epidemiology
Hereditary hemochromatosis is one of the most common genetic diseases in the white population, with a prevalence of the C282Y homozygous state of 1 in 200 to 1 in 400 [148]. The disease is most common in individuals of northern European descent. The frequency of the C282Y mutation is highest in subjects from northwest Europe (10–20 %), less frequent in southern and eastern European populations (2–4 %), and rare in natives of Africa, Central or South America, Eastern Asia, and the Pacific Islands [149]. The H63D mutation has a distribution similar to that of C282Y, but it is more common in European groups (15–40 %). In a large population-based study of 3,011 unrelated white adults in Busselton, Australia, 14.1 % were heterozygous for the C282Y mutation and 0.5 % were homozygous [149].
About 6.8 % of the US white population is heterozygous for the C282Y mutation and 0.5 % is homozygous. This is fairly similar to the estimates of 1 in 200 incidence of iron overload in the worldwide white population [150]. HHC and the C282Y mutation are uncommon in African Americans or Asian Americans [149], the prevalence of clinically diagnosed HHC in African Americans being about 1 in 1,000 [148].
Thus, HHC remains predominately a disease of individuals of northern European descent. Although mutation analysis has assisted in defining the prevalence of the disease in this population, it has not proved useful in other selected populations. Nevertheless, HHC remains one of the more common, if not the most common, inherited disorder in humans.
Clinical Features
In adults, HHC may present with the clinical syndrome of diabetes, cirrhosis, and increased skin pigmentation as initially described in 1865. Although the genetic defect is present at birth, years of increased iron absorption and tissue accumulation (usually >5 g of excess total body iron) are required for the development of clinical symptoms. Clinical symptoms are rare before adulthood. Before the discovery of the gene for HHC, most adults were diagnosed with clinical symptoms that included liver disease (fibrosis or cirrhosis), diabetes, skin pigmentation, heart failure, arthritis, and endocrinologic disturbances. Since the discovery of the HFE gene, it is recognized that many adults who are homozygous for the C282Y mutation are asymptomatic [149]. HHC can be classified into four stages: (1) a genetic predisposition with no abnormality other than possibly an elevated serum transferrin saturation, (2) iron overload (2–5 g) without symptoms, (3) iron overload with early symptoms (lethargy, arthralgia), and (4) iron overload with organ damage. Almost all children with HHC are in the first stage and may rarely be in the second stage. For further data on the clinical manifestations in adults, the reader is referred to a recent review [151]. As iron accumulates in the tissues, there is progressive fibrosis and injury. As organ failure results, the classic clinical consequences of hemochromatosis are recognized. The organs involved and pathologic findings are listed in Table 9.7.
Disease expression is dependent not only on the mutation but on other genetic and environmental factors, such as sex, age, dietary iron, and other factors affecting iron balance. Males with HHC typically present earlier than females, presumably because of the ongoing iron losses in menstruating females. In addition, the association of symptoms with the mutations is quite variable and less common than previously thought.
Most children and adolescents with HHC are asymptomatic. Although most have abnormal transferrin saturation, a normal ferritin is the rule. Reports of elevated ferritin and death from congestive heart failure in pediatric patients have not been confirmed by genotype analysis and may represent JHC, a truly distinct disorder [152]. A study screening the children of 179 homozygotes found that even at a mean age of 37 years, most affected children of parents with HHC were asymptomatic [153].
Unless another illness is present, heterozygotes do not have clinically important iron overload. Heterozygotes do have slightly higher transferrin saturations than those in normal individuals (men 38 % vs. 30 %; women 32 % vs. 29 %). This suggests that the heterozygote state may be protective for iron deficiency in women.
Diagnosis and Screening
Prior to the discovery of HFE, the diagnosis of HHC required the documentation of iron overload or HLA linkage to an affected individual. Criteria for iron overload consistent with HHC include (a) grade 3 or 4 stainable iron on liver biopsy, (b) hepatic iron concentration greater than 4,500 μg (80 μmol)/g dry weight, (c) a hepatic iron index (iron concentration in micromoles per gram of dry weight divided by age in years) of more than 1.9, and (d) evidence of iron overload of more than 5 g. These criteria are rarely encountered in children because in the absence of confounding factors (high dietary intake, hepatitis C viral infection, etc.), children typically have not developed this degree of iron overload. These criteria are probably not acceptable for individuals identified by family screening, who may be early in the course of iron overload. Some investigators have suggested that any individual with an abnormal hepatic iron concentration (>30 μmol/g or 1,500 μg/g dry weight) who has no other reason for iron overload should be suspected of having HHC. A variety of disorders can lead to hepatic iron overload, including chronic liver diseases such as alcoholic liver disease, nonalcoholic steatohepatitis (NASH), chronic viral hepatitis, cystic fibrosis, and porphyria cutanea tarda. There is no association with an increased prevalence of the HFE mutations in either alcoholic liver disease or viral hepatitis [154]. However, in both NASH and porphyria cutanea tarda, a higher frequency of the C282Y mutation has been observed [155].
In adults, transferrin saturation is used to screen individuals, with the threshold for further investigation of 45 % in men and 42 % in premenopausal women. Abnormal transferrin saturation has been reported in children as young as 2 years. However, fasting transferrin saturation and ferritin level in affected children can be normal, even in known homozygous subjects [156]. Up to 30 % of women with HHC who are under 30 years of age have normal transferrin saturation [156]. Thus, transferrin saturation is helpful in phenotypic screening in children when it is abnormal but does not exclude HHC when normal. In contrast, ferritin may be elevated in many inflammatory liver diseases such as chronic viral hepatitis and NASH in the absence of HHC and is less helpful in phenotypic screening for HHC in children and adults.
Liver biopsy has been primarily studied in adults and should not be used for the diagnosis of HHC in children. Increased hepatic iron can be demonstrated by Prussian blue staining. Hepatic iron quantitation with the determination of the hepatic iron index (micromoles of iron per gram of dry weight divided by age in years) has been considered one of the more sensitive and specific tests for HHC. A hepatic iron index of greater than 1.9 in the absence of secondary iron overload is indicative of HHC with iron overload. However, 10–15 % of HHC patients identified by genetic testing will have a hepatic iron index of less than 1.9, calling into question the use of this test for diagnosis in children [156]. In children with HHC, an abnormal hepatic iron index has been reported in those as young as 7 years. Liver biopsy has given way to magnetic resonance imaging (MRI) quantitation of hepatic iron content. Liver biopsy should reserved for assessment of hepatic fibrosis in HHC and ruling out other causes of liver disease [157].
Genetic testing is available on a commercial basis. In 150 family members of 61 white American probands, 34 family members had an HHC phenotype. Among the family members, 92 % of the C282Y homozygotes and 34 % of the C282Y/H63D compound heterozygotes had the HHC phenotype. None of the H63D homozygotes had an HHC phenotype. A few individuals were heterozygous for one mutation and had iron overload. Thus, testing for HFE mutations should include both the C282Y and the H63D mutations. Heterozygosity may contribute to iron overload with an associated condition, but it should not be considered the sole cause of iron overload. Only C282Y/C282Y and compound heterozygosity (C282Y/H63D) should be considered indicative of HHC. However, not all compound heterozygotes will develop HHC. In most cases, these individuals will not require liver biopsy for confirmation of the diagnosis. However, C282Y homozygotes with evidence of liver disease (elevated aminotransferases or hepatomegaly) or with serum ferritin levels greater than 1,000 μg/L should undergo a liver biopsy to assess the degree of liver injury and the possible contribution of other liver disorders to the clinical picture. Liver biopsy is also recommended in suspected iron overload in non-C282Y homozygotes (C282Y heterozygotes, C282Y/H63D, or no mutations).
Approach to the Child with a Parent with HHC
The preferred clinical assessment of a child whose parent has HHC is open to debate. Because symptomatic end-stage organ disease from HHC is easily preventable with early therapy, screening of potentially affected children has been advocated. However, the majority of patients present with clinical disease after the age of 20 years. Biochemical screening requires repeated determination of transferrin saturation and ferritin. With the advent of genetic mutation testing, Adams et al. [153] have shown that it is cost-effective to screen the unaffected parent with mutation analysis. A suggested strategy is shown in Fig. 9.4. If the unaffected parent is either heterozygous or homozygous for C282Y, the potentially affected children are then screened with mutation analysis following appropriate counseling and consent [153]. Subsequently, at-risk children are followed with fasting transferrin saturation, ferritin, and liver blood tests. This strategy was found to be more cost-effective when compared with the phenotypic strategy [158]. When the ferritin is greater than 200 μg/L or aminotransferases increase, phlebotomy therapy is then initiated.

Strategy for screening for hereditary hemochromatosis in a child with a parent with hemochromatosis
Iron Overload in Children with Liver Dysfunction
In pediatric patients, iron overload should be considered in the differential diagnosis of liver disease. Testing for transferrin saturation and ferritin should be considered in the evaluation of hepatic dysfunction in children (Fig. 9.5). If liver biopsy is performed as part of the evaluation, staining for iron should be done and quantitative hepatic iron determination should be considered. There are older reports of children presenting as young as 5 years with iron overload and presumed HHC that may have been JHC, as these reports predate HFE testing. White children with evidence of iron overload (elevated transferrin saturation of >45 %, elevated ferritin, increased stainable iron or hepatic iron concentration) would be candidates for possible HFE mutation analysis. The yield of HFE analysis in African American and Asian American children should be quite low. HFE mutation analysis may be helpful in patients with other diseases that can lead to iron overload (NASH, porphyria cutanea tarda).

Strategy for screening and diagnosis of iron overload in a child with liver disease and suspected iron overload
The role of liver biopsy has not been studied in children. Data from one large adult study has shown that 50 % of HHC patients with a ferritin level greater than 1,000 μg/L, abnormal aspartate aminotransferase (AST), or hepatomegaly had significant fibrosis on liver biopsy [159]. In contrast, none of the HHC patients without those factors had significant fibrosis [159]. Even before genotyping was available, it was shown that patients diagnosed in the precirrhotic stage who were treated with venisection had a normal life expectancy. Thus, in patients homozygous for the C282Y mutation, these noninvasive measures may be used to avoid liver biopsy.
Because HHC is a common genetic disorder whose effects can be prevented by presymptomatic intervention, screening of the general population has been considered. Until the cost of the testing is reduced and the implications for insurability and management are clarified, newborn testing has not been recommended [160]. In adults, screening strategies have been suggested using a combination of transferrin saturation and confirmation with HFE testing.
Treatment
The goals of treatment are to reduce total body iron overload and prevent reaccumulation of iron. When instituted before end-organ injury, successful treatment would ideally prevent the development of cirrhosis and other end-organ disease and reduce the incidence of hepatocellular carcinoma. Current recommendations are that venisection is indicated if serum ferritin is greater than 300 μg/L in males or 200 μg/L in females [161]. The goal of therapy is to maintain a ferritin level less than 50 μg/L. There are little published data on phlebotomy therapy in children as children with HHC rarely meet the preceding criteria. Initial therapy in symptomatic children should include weekly or every-other-week phlebotomy of 5–8 mL/kg until the ferritin has decreased to <300 μg/L. Thereafter, two to four sessions per year will probably be required. In our experience, therapeutic phlebotomy may need to be less frequent in children with HHC who have asymptomatic iron overload, probably because of their lower total body iron load. Careful attention to the development of iron deficiency is required when treating children. Once identified, children with HHC should be counseled to maintain a low-iron diet and avoid ascorbic acid and vitamin supplements containing iron.
Juvenile Hemochromatosis (OMIM 602390)
Juvenile hemochromatosis, or hemochromatosis type 2, is a rare iron-loading disorder that leads to severe iron loading and organ failure, typically before 30 years of age [152]. Even though this is rarer than HHC, JHC may be a more common cause of symptomatic iron overload in children. JHC is characterized by autosomal recessive inheritance and a pattern of iron distribution and tissue injury similar to that of HHC. However, JHC is not associated with mutations in HFE. In contrast to HHC, males and females are equally affected, and hypogonadism and cardiac dysfunction are the most common symptoms at presentation. The disorder has been reported in several ethnic groups. Most patients present in the second and third decades of life, likely the result of a higher rate of iron accumulation in JHC as compared with HHC. As such, the phlebotomy requirements to maintain normal iron balance are significantly higher in JHC as compared with HHC. Most cases of JHC are due to mutations in the gene HJV which encodes hemojuvelin, a key regulatory protein for hepcidin, and accounts for about 90 % of the cases reported to date [152]. The most frequent mutation is G320V, which was reported to account for 60 % of the mutations in the original description and all individuals identified in a French Canadian study. However, many mutations have now been reported (reviewed in [152]). HAMP, which encodes hepcidin, accounts for 10 % of the reported cases [162]. Combined mutations in HFE and TFR2 may also present with a phenotype of JHC without mutations in either HJV or HAMP [140, 152].
As a consequence, this disorder should be considered when children and adolescents present with clinically significant liver disease and iron overload. A family history of iron overload and hypogonadism in the absence of HFE mutations should raise the clinical suspicion for JHC. It is likely that some of the earlier reports of children with clinically apparent liver disease and iron overload had JHC and not HHC. With the identification of candidate genes involved in JHC, genetic diagnosis is available for HJV, HAMP, and the HFE/TFR2 combination. These offer the opportunity for presymptomatic diagnosis in children from affected families. However, the overall incidence of this disorder must be small in comparison with classic HHC, as in the Australian population study, only 0.5 % of the adults with the wild-type/wild-type hemochromatosis genotype had an elevated (>45 %) fasting transferrin saturation.
A recommended approach to children with suspected iron overload and no family history of HHC is shown in Fig. 9.5.
Secondary Iron Overload
Secondary iron overload is a common problem for children with transfusion-dependent diseases such as the thalassemias, sickle cell disease, and aplastic anemias. This disorder has been referred to as hemosiderosis, primarily because the accumulation of iron begins in the reticuloendothelial cells in the liver. The pathophysiology of secondary iron overload is related to the provision of parenteral iron that bypasses the normal intestinal regulation of iron absorption. In addition, the anemias of ineffective erythropoiesis (thalassemias, congenital dyserythropoietic anemias, and sideroblastic anemias) stimulate iron absorption, resulting in an additional 2–5 g of iron absorbed from the diet per year. Tissue iron overloading of parenchymal cells is apparent after only 1 year of transfusion therapy. In patients who are receiving transfusions without chelation therapy, symptomatic heart disease has been reported within 10 years [163]. Iron-induced liver disease is a common cause of death in older patients, often aggravated by hepatitis C infection. Hepatic fibrosis is present as early as 2 years after starting transfusions, with cirrhosis reported in the first decade of life. With improved survival with iron chelation, iron loading of the anterior pituitary and associated disturbed sexual maturation are quite common.
Although the amount of excess iron that has been provided in the form of transfused iron can be calculated from the volume of red blood cells administered, the biochemical markers of iron overload may be unreliable. Some researchers advocate following ferritin levels for signs of iron overload. Under normal conditions, 1 μg/L of ferritin is equivalent to 8–10 mg of storage iron. Thus, a ferritin of 1,000 μg/L is equal to about 10,000 mg of storage iron. When ferritin is >4,000 μg/L, there is no longer a correlation between ferritin and iron stores. In addition, ferritin may be increased with hepatic inflammation that may be related to other factors, such as hepatitis C infection. This has led others to suggest that ferritin concentrations are not an accurate reflection of tissue iron accumulation [164]. More accurate estimations of tissue iron burden are obtained by liver or cardiac biopsy and iron quantitation by MRI [165] or by investigative SQUID (superconducting quantum interference device) biomagnetometry, which may be better at assessing high tissue iron concentrations.
Treatment
Treatment of transfusional iron overload centers on chelation therapy or, when possible, exchange transfusion. Deferoxamine is generally given by continuous subcutaneous administration and is capable of inducing negative iron balance. In general, ferritin should begin to decrease by the end of 1 year of treatment. The goal is to maintain a ferritin level of less than 1,000 μg/L on treatment. Deferoxamine prevents early cardiac death, arrests the progression to cirrhosis, and stabilizes or reduces total body iron load [166]. The major risks of deferoxamine are growth failure, hearing impairment, and bone abnormalities. These are more common in patients with low iron loads. Direct dose-related toxicities involve the kidneys, lungs, and visual loss. The early use of deferoxamine in an amount proportional to the transfusional iron overload reduces iron burden and the risk of the development of diabetes mellitus, cardiac disease, and early death in patients with thalassemia major [166]. When possible, such as in some cases of sickle cell disease, exchange transfusion can reduce the iron burden from transfusions [167]. Other strategies include intravenous deferoxamine, which can rapidly reduce tissue iron burden in situations of severe iron overload. Newer oral chelation agents are available. Deferiprone, used for years in Europe and now approved in the USA, seems to be more effective at removal of cardiac iron load than deferoxamine with similar or slightly less efficacy for hepatic iron reduction. The major side effects of deferiprone are bone marrow suppression, arthropathy, gastrointestinal symptoms, and zinc deficiency. Deferasirox, another oral chelation therapy approved for use in the USA and several other countries, appears to be very efficient in liver and cardiac iron removal in adults and children. Side effect includes gastrointestinal disease. Recent reports suggest a small but increased risk of renal or hepatic failure and gastrointestinal hemorrhage. Combination treatment with deferoxamine and deferiprone or other oral chelators, such as deferasirox, suggests an additive effect in the presence of adequate renal function [168].
In the past, researchers have recommended serial liver biopsy to follow iron overload in transfusion-dependent patients. MRI is the test of choice to quantitate hepatic iron overload and longitudinal determinations [165]. Liver biopsy should be reserved for assessment of hepatic injury and fibrosis and for the assessment of the relative contribution of non-iron-related disorders to the process.
References
Perlmutter DH. Alpha-1-antitrypsin deficiency. Semin Liver Dis. 1998;18(3):217–25.
Perlmutter DH. Alpha-1 antitrypsin deficiency. In: Walker WA, editor. Pediatric gastrointestinal disease. 3rd ed. Hamilton: B C Decker; 2000.
Perlmutter DH. Alpha-1 antitrypsin deficiency. In: Suchy F, Sokol R, editors. Liver disease in children. 3rd ed. Cambridge: Cambridge University Press; 2007. p. 545–71.
Marciniuk DD, et al. Alpha-1 antitrypsin deficiency targeted testing and augmentation therapy: a Canadian Thoracic Society clinical practice guideline. Can Respir J. 2012;19(2):109–16.
Silverman EK, Sandhaus RA. Clinical practice. Alpha1-antitrypsin deficiency. N Engl J Med. 2009;360(26):2749–57.
Sveger T. Liver disease in alpha1-antitrypsin deficiency detected by screening of 200,000 infants. N Engl J Med. 1976;294(24):1316–21.
Sveger T. Alpha 1-antitrypsin deficiency in early childhood. Pediatrics. 1978;62(1):22–5.
Eriksson S. Alpha 1-antitrypsin deficiency. J Hepatol. 1999;30 Suppl 1:34–9.
Gadek JE, et al. Antielastases of the human alveolar structures. Implications for the protease-antiprotease theory of emphysema. J Clin Invest. 1981;68(4):889–98.
Perlmutter DH, Pierce JA. The alpha 1-antitrypsin gene and emphysema. Am J Physiol. 1989;257(4 Pt 1):L147–62.
Teckman JH, Perlmutter DH. Retention of mutant alpha(1)-antitrypsin Z in endoplasmic reticulum is associated with an autophagic response. Am J Physiol Gastrointest Liver Physiol. 2000;279(5):G961–74.
Pierce JA, Eradio BG. Improved identification of antitrypsin phenotypes through isoelectric focusing with dithioerythritol. J Lab Clin Med. 1979;94(6):826–31.
Ranes J, Stoller JK. A review of alpha-1 antitrypsin deficiency. Semin Respir Crit Care Med. 2005;26(2):154–66.
Travis J, Salvesen GS. Human plasma proteinase inhibitors. Annu Rev Biochem. 1983;52:655–709.
Perlmutter DH. Alpha-1-antitrypsin deficiency: importance of proteasomal and autophagic degradative pathways in disposal of liver disease-associated protein aggregates. Annu Rev Med. 2011;62:333–45.
Hofker MH, et al. Cloning and characterization of an alpha 1-antitrypsin like gene 12 KB downstream of the genuine alpha 1-antitrypsin gene. Biochem Biophys Res Commun. 1988;155(2):634–42.
Laurell CB, Nosslin B, Jeppsson JO. Catabolic rate of alpha1-antitrypsin of Pi type M and Z in man. Clin Sci Mol Med. 1977;52(5):457–61.
Lomas DA, et al. The mechanism of Z alpha 1-antitrypsin accumulation in the liver. Nature. 1992;357(6379):605–7.
Bathurst IC, et al. Structural and functional characterization of the abnormal Z alpha 1-antitrypsin isolated from human liver. FEBS Lett. 1984;177(2):179–83.
Ogushi F, et al. Z-type alpha 1-antitrypsin is less competent than M1-type alpha 1-antitrypsin as an inhibitor of neutrophil elastase. J Clin Invest. 1987;80(5):1366–74.
Rosenthal P, Liebman WM, Thaler MM. Alpha 1-antitrypsin deficiency and severe infantile liver disease. Am J Dis Child. 1979;133(11):1195–6.
Waasdorp Hurtado C, Sokol R, Rosen H. Metabolic liver disease. In: Friedman’s handbook of liver disease. 3rd ed. Philadelphia, PA: Elsevier/Mosby; 2011.
Propst T, et al. High prevalence of viral infection in adults with homozygous and heterozygous alpha 1-antitrypsin deficiency and chronic liver disease. Ann Intern Med. 1992;117(8):641–5.
Sveger T, Eriksson S. The liver in adolescents with alpha 1-antitrypsin deficiency. Hepatology. 1995;22(2):514–7.
Topic A, Prokic D, Stankovic I. Alpha-1-antitrypsin deficiency in early childhood. Fetal Pediatr Pathol. 2011;30(5):312–9.
Odievre M, et al. Alpha1-antitrypsin deficiency and liver disease in children: phenotypes, manifestations, and prognosis. Pediatrics. 1976;57(2):226–31.
Larsson C. Natural history and life expectancy in severe alpha1-antitrypsin deficiency, Pi Z. Acta Med Scand. 1978;204(5):345–51.
Stoller JK, Aboussouan LS. A review of alpha1-antitrypsin deficiency. Am J Respir Crit Care Med. 2012;185(3):246–59.
Guenter CA, et al. The pattern of lung disease associated with alpha antitrypsin deficiency. Arch Intern Med. 1968;122(3):254–7.
Kalsheker NA. Alpha1-antitrypsin deficiency: best clinical practice. J Clin Pathol. 2009;62(10):865–9.
Ghishan FK, Greene HL. Liver disease in children with PiZZ alpha 1-antitrypsin deficiency. Hepatology. 1988;8(2):307–10.
Qizilbash A, Young-Pong O. Alpha 1 antitrypsin liver disease differential diagnosis of PAS-positive, diastase-resistant globules in liver cells. Am J Clin Pathol. 1983;79(6):697–702.
Udall Jr JN, et al. Liver disease in alpha 1-antitrypsin deficiency. A retrospective analysis of the influence of early breast- vs bottle-feeding. JAMA. 1985;253(18):2679–82.
Labrune P, Odievre M, Alagille D. Influence of sex and breastfeeding on liver disease in alpha 1-antitrypsin deficiency. Hepatology. 1989;10(1):122.
Kemmer N, et al. Alpha-1-antitrypsin deficiency: outcomes after liver transplantation. Transplant Proc. 2008;40(5):1492–4.
Stecenko AA, Brigham KL. Gene therapy progress and prospects: alpha-1 antitrypsin. Gene Ther. 2003;10(2):95–9.
Yusa K, et al. Targeted gene correction of alpha1-antitrypsin deficiency in induced pluripotent stem cells. Nature. 2011;478(7369):391–4.
Carbamazepine in severe liver disease due to alpha-1 antitrypsin deficiency. Clinical Trials 2012. Available from: http://www.ClinicalTrials.gov/ct2/show/NCT01379469?term=alpha-1+antitrypsin. Cited 2 Nov 2012.
Wilson SA. Progressive lenticular degeneration: a familial nervous disease associated with cirrhosis of the liver. Brain. 1912;34:295–509.
Scheinberg I, Sternleib I. Wilson’s disease. Philadelphia: WB Saunders; 1984.
Schilsky M, Scheinberg I, Sternleib I. Liver transplantation for Wilson’s disease: indications and outcomes. Hepatology. 1994;19:583–7.
Frydman M, et al. Assignment of the gene for Wilson disease to chromosome 13: linkage to the esterase D locus. Proc Natl Acad Sci U S A. 1985;82(6):1819–21.
Merle U, et al. Clinical presentation, diagnosis and long-term outcome of Wilson’s disease: a cohort study. Gut. 2007;56(1):115–20.
Weiss KH, Stremmel W. Evolving perspectives in Wilson disease: diagnosis, treatment and monitoring. Curr Gastroenterol Rep. 2012;14(1):1–7.
Lee BH, et al. Distinct clinical courses according to presenting phenotypes and their correlations to ATP7B mutations in a large Wilson’s disease cohort. Liver Int. 2011;31(6):831–9.
Wilson’s Disease Database. 2012. Available from: http://www.wilsondisease.med.ualberta.ca/database.asp. Cited 2 Nov 2012.
Rosencrantz R, Schilsky M. Wilson disease: pathogenesis and clinical considerations in diagnosis and treatment. Semin Liver Dis. 2011;31(3):245–59.
Chitkara D, Pleskow R, Grand R. Wilson disease. In: Walker WA, editor. Pediatric gastrointestinal disease. 3rd ed. Hamilton: BC Decker; 2000.
Walshe J, Briggs J. Ceruloplasmin in liver disease, a diagnostic pitfall. Lancet. 1962;ii:263–5.
Factor SM, et al. The cardiomyopathy of Wilson’s disease. Myocardial alterations in nine cases. Virchows Arch A Pathol Anat Histol. 1982;397(3):301–11.
Manolaki N, et al. Wilson disease in children: analysis of 57 cases. J Pediatr Gastroenterol Nutr. 2009;48(1):72–7.
Yamaguchi Y, et al. Mass screening for Wilson’s disease: results and recommendations. Pediatr Int. 1999;41(4):405–8.
Wiebers D, Hollenhurst R, Goldstein N. The ophthalmologic manifestations of Wilson’s disease. Mayo Clinic Proc. 1977;52:409–16.
Chu CC, Huang CC, Chu NS. Recurrent hypokalemic muscle weakness as an initial manifestation of Wilson’s disease. Nephron. 1996;73(3):477–9.
Kuan P. Cardiac Wilson’s disease. Chest. 1987;91:579–83.
Werlin SL, et al. Diagnostic dilemmas of Wilson’s disease: diagnosis and treatment. Pediatrics. 1978;62(1):47–51.
Ferenci P, et al. Diagnosis and phenotypic classification of Wilson disease. Liver Int. 2003;23(3):139–42.
Dhawan A, et al. Wilson’s disease in children: 37-year experience and revised King’s score for liver transplantation. Liver Transpl. 2005;11(4):441–8.
Nicastro E, et al. Re-evaluation of the diagnostic criteria for Wilson disease in children with mild liver disease. Hepatology. 2010;52(6):1948–56.
European Association for Study of Liver. EASL clinical practice guidelines: Wilson’s disease. J Hepatol. 2012;56(3):671–85.
Dorney SF, et al. Wilson’s disease in childhood. A plea for increased awareness. Med J Aust. 1986;145(10):538–41.
Taylor RM, Chen Y, Dhawan A. Triethylene tetramine dihydrochloride (trientine) in children with Wilson disease: experience at King’s College Hospital and review of the literature. Eur J Pediatr. 2009;168(9):1061–8.
Narumi S, et al. Liver transplantation for Wilson’s disease in pediatric patients: decision making and timing. Transplant Proc. 2012;44(2):478–80.
Bem RS, et al. Wilson’s disease in southern Brazil: a 40-year follow-up study. Clinics (Sao Paulo). 2011;66(3):411–6.
Corey M, et al. Longitudinal analysis of pulmonary function decline in patients with cystic fibrosis. J Pediatr. 1997;131(6):809–14.
Corey M, Farewell V. Determinants of mortality from cystic fibrosis in Canada, 1970–1989. Am J Epidemiol. 1996;143(10):1007–17.
Kerem E, et al. Prediction of mortality in patients with cystic fibrosis. N Engl J Med. 1992;326(18):1187–91.
Efrati O, et al. Liver cirrhosis and portal hypertension in cystic fibrosis. Eur J Gastroenterol Hepatol. 2003;15(10):1073–8.
Colombo C. Liver disease in cystic fibrosis. Curr Opin Pulm Med. 2007;13(6):529–36.
Colombo C, et al. Liver disease in cystic fibrosis: a prospective study on incidence, risk factors, and outcome. Hepatology. 2002;36(6):1374–82.
Lamireau T, et al. Epidemiology of liver disease in cystic fibrosis: a longitudinal study. J Hepatol. 2004;41(6):920–5.
Scott-Jupp R, Lama M, Tanner MS. Prevalence of liver disease in cystic fibrosis. Arch Dis Child. 1991;66(6):698–701.
Bhattacharjee R, et al. The natural history of liver disease in cystic fibrosis. J Cyst Fibros. 2006;5:S61.
Williams SM, et al. Ultrasound evaluation of liver disease in cystic fibrosis as part of an annual assessment clinic: a 9-year review. Clin Radiol. 2002;57(5):365–70.
Lenaerts C, et al. Surveillance for cystic fibrosis-associated hepatobiliary disease: early ultrasound changes and predisposing factors. J Pediatr. 2003;143(3):343–50.
Lindblad A, Glaumann H, Strandvik B. Natural history of liver disease in cystic fibrosis. Hepatology. 1999;30(5):1151–8.
Desmond CP, et al. The benign course of liver disease in adults with cystic fibrosis and the effect of ursodeoxycholic acid. Liver Int. 2007;27(10):1402–8.
Lewindon PJ, Ramm GA. Cystic fibrosis-cirrhosis, portal hypertension, and liver biopsy: reply. Hepatology. 2011;53(3):1065–6.
Feigelson J, et al. Liver cirrhosis in cystic fibrosis–therapeutic implications and long term follow up. Arch Dis Child. 1993;68(5):653–7.
Chryssostalis A, et al. Liver disease in adult patients with cystic fibrosis: a frequent and independent prognostic factor associated with death or lung transplantation. J Hepatol. 2011;55:1377–82.
Lewindon PJ, et al. Importance of hepatic fibrosis in cystic fibrosis and the predictive value of liver biopsy. Hepatology. 2011;53(1):193–201.
Witters P, et al. Noncirrhotic presinusoidal portal hypertension is common in cystic fibrosis-associated liver disease. Hepatology. 2011;53(3):1064–5.
Rowland M, et al. Outcome in cystic fibrosis liver disease. Am J Gastroenterol. 2011;106(1):104–9.
Debray D, et al. Outcome of cystic fibrosis-associated liver cirrhosis: management of portal hypertension. J Hepatol. 1999;31(1):77–83.
Polineni D, et al. Pulmonary function (FEV1) in cystic fibrosis patients with and without severe liver disease with portal hypertension (CFLD). Am J Respir Crit Care Med. 2009;A1779.
Minicucci L, et al. Liver disease as risk factor for cystic fibrosis-related diabetes development. Acta Paediatr. 2007;96(5):736–9.
Sullivan KM, Moran A, Schwarzenberg S. Cystic fibrosis related diabetes in CF patients with cirrhosis. Pediatr Pulmonol. 2009;44:414.
Corbett K, et al. Cystic fibrosis-associated liver disease: a population-based study. J Pediatr. 2004;145(3):327–32.
Blanc WA, Di Sant’Agnese PA. A distinctive type of biliary cirrhosis of the liver associated with cystic fibrosis of the pancreas; recognition through signs of portal hypertension. Pediatrics. 1956;18(3):387–409.
Vawter GF, Shwachman H. Cystic fibrosis in adults: an autopsy study. Pathol Annu. 1979;14(Pt 2):357–82.
Robertson MB, Choe KA, Joseph PM. Review of the abdominal manifestations of cystic fibrosis in the adult patient. Radiographics. 2006;26(3):679–90.
Woodruff SA, et al. Prevalence of elevated liver function tests in children with cystic fibrosis diagnosed by newborn screen. J Pediatr Gastroenterol Nutr. 2007;45:E27–8.
Mayer-Hamblett N, et al. Incidence and clinical significance of elevated liver function tests in cystic fibrosis clinical trials. Contemp Clin Trials. 2012;34(2):232–8.
Debray D, et al. Best practice guidance for the diagnosis and management of cystic fibrosis-associated liver disease. J Cyst Fibros. 2011;10 Suppl 2:S29–36.
Herrmann U, Dockter G, Lammert F. Cystic fibrosis-associated liver disease. Best Pract Res Clin Gastroenterol. 2010;24(5):585–92.
Akata D, Akhan O. Liver manifestations of cystic fibrosis. Eur J Radiol. 2007;61(1):11–7.
Diwakar V, Pearson L, Beath S. Liver disease in children with cystic fibrosis. Paediatr Respir Rev. 2001;2(4):340–9.
Patriquin H, et al. Liver disease in children with cystic fibrosis: US-biochemical comparison in 195 patients. Radiology. 1999;211(1):229–32.
Durieu I, et al. Sclerosing cholangitis in adults with cystic fibrosis: a magnetic resonance cholangiographic prospective study. J Hepatol. 1999;30(6):1052–6.
Lykavieris P, Bernard O, Hadchouel M. Neonatal cholestasis as the presenting feature in cystic fibrosis. Arch Dis Child. 1996;75(1):67–70.
Wilschanski M, Durie PR. Patterns of GI disease in adulthood associated with mutations in the CFTR gene. Gut. 2007;56(8):1153–63.
Angelico M, et al. Gallstones in cystic fibrosis: a critical reappraisal. Hepatology. 1991;14(5):768–75.
Wasmuth HE, et al. Coinheritance of Gilbert syndrome-associated UGT1A1 mutation increases gallstone risk in cystic fibrosis. Hepatology. 2006;43(4):738–41.
Cohn JA, et al. Localization of the cystic fibrosis transmembrane conductance regulator in human bile duct epithelial cells. Gastroenterology. 1993;105(6):1857–64.
Gerling B, et al. Prediction of liver fibrosis according to serum collagen VI level in children with cystic fibrosis. N Engl J Med. 1997;336(22):1611–2.
Pereira TN, et al. Serum markers of hepatic fibrogenesis in cystic fibrosis liver disease. J Hepatol. 2004;41(4):576–83.
Sidlova K, et al. Serum alpha-glutathione S-transferase as a sensitive marker of hepatocellular damage in patients with cystic fibrosis. Physiol Res. 2003;52(3):361–5.
Rath T, et al. TIMP-1/-2 and transient elastography allow non invasive diagnosis of cystic fibrosis associated liver disease. Dig Liver Dis. 2012;44(9):780–7.
Williams SG, et al. An ultrasound scoring system for the diagnosis of liver disease in cystic fibrosis. J Hepatol. 1995;22(5):513–21.
Mueller-Abt PR, et al. Comparison of ultrasound and biopsy findings in children with cystic fibrosis related liver disease. J Cyst Fibros. 2008;7(3):215–21.
Witters P, et al. Non-invasive liver elastography (Fibroscan) for detection of cystic fibrosis-associated liver disease. J Cyst Fibros. 2009;8(6):392–9.
Malbrunot-Wagner AC, et al. Transient elastography and portal hypertension in pediatric patients with cystic fibrosis Transient elastography and cystic fibrosis. J Cyst Fibros. 2011;10(5):338–42.
Boursier J, et al. Acoustic radiation force impulse: a new ultrasonographic technology for the widespread noninvasive diagnosis of liver fibrosis. Eur J Gastroenterol Hepatol. 2010;22(9):1074–84.
Baranova A, et al. Non-invasive markers for hepatic fibrosis. BMC Gastroenterol. 2011;11:91.
Manco M, et al. Pilot study on the use of acoustic radiation force impulse imaging in the staging of cystic fibrosis associated liver disease. J Cyst Fibros. 2012;11:427–32.
Colombo C, et al. Liver disease in cystic fibrosis. J Pediatr Gastroenterol Nutr. 2006;43 Suppl 1:S49–55.
Moyer K, Balistreri W. Hepatobiliary disease in patients with cystic fibrosis. Curr Opin Gastroenterol. 2009;25(3):272–8.
Sokol RJ, Durie PR. Recommendations for management of liver and biliary tract disease in cystic fibrosis. Cystic Fibrosis Foundation Hepatobiliary Disease Consensus Group. J Pediatr Gastroenterol Nutr. 1999;28 Suppl 1:S1–13.
Cheng K, Ashby D, Smyth RL. Ursodeoxycholic acid for cystic fibrosis-related liver disease. Cochrane Database Syst Rev. 2012;10:CD000222.
Ooi CY, et al. Ursodeoxycholic acid in cystic fibrosis-associated liver disease. J Cyst Fibros. 2012;11(1):72–3.
Neglia JP, et al. The risk of cancer among patients with cystic fibrosis. Cystic Fibrosis and Cancer Study Group. N Engl J Med. 1995;332(8):494–9.
O’Donnell DH, et al. Hepatocellular carcinoma complicating cystic fibrosis related liver disease. J Cyst Fibros. 2009;8(4):288–90.
Pozler O, et al. Transjugular intrahepatic portosystemic shunt in five children with cystic fibrosis: long-term results. Hepatogastroenterology. 2003;50(52):1111–4.
Louis D, et al. Partial splenectomy for portal hypertension in cystic fibrosis related liver disease. Pediatr Pulmonol. 2007;42(12):1173–80.
Harned 2nd RK, et al. Partial splenic embolization in five children with hypersplenism: effects of reduced-volume embolization on efficacy and morbidity. Radiology. 1998;209(3):803–6.
Fridell JA, et al. Liver transplantation in children with cystic fibrosis: a long-term longitudinal review of a single center’s experience. J Pediatr Surg. 2003;38(8):1152–6.
Milkiewicz P, et al. Transplantation for cystic fibrosis: outcome following early liver transplantation. J Gastroenterol Hepatol. 2002;17(2):208–13.
Noble-Jamieson G, et al. Liver transplantation for hepatic cirrhosis in cystic fibrosis. J R Soc Med. 1996;89 Suppl 27:31–7.
Gridelli B. Liver: benefit of liver transplantation in patients with cystic fibrosis. Nat Rev Gastroenterol Hepatol. 2011;8(4):187–8.
Mendizabal M, et al. Liver transplantation in patients with cystic fibrosis: analysis of United Network for Organ Sharing data. Liver Transpl. 2011;17(3):243–50.
Lu BR, Esquivel CO. A review of abdominal organ transplantation in cystic fibrosis. Pediatr Transplant. 2010;14:954–60.
Melzi ML, et al. Liver transplant in cystic fibrosis: a poll among European centers. A study from the European Liver Transplant Registry. Transpl Int. 2006;19(9):726–31.
Genyk YS, et al. Liver transplantation in cystic fibrosis. Curr Opin Pulm Med. 2001;7(6):441–7.
Nash KL, et al. Cystic fibrosis liver disease: to transplant or not to transplant? Am J Transplant. 2008;8(1):162–9.
Miller MR, et al. Pulmonary function in individuals who underwent liver transplantation: from the US cystic fibrosis foundation registry. Liver Transpl. 2012;18(5):585–93.
Bartlett JR, et al. Genetic modifiers of liver disease in cystic fibrosis. JAMA. 2009;302(10):1076–83.
Nightingale S, et al. Isolated liver transplantation in children with cystic fibrosis–an Australian experience. Pediatr Transplant. 2010;14(6):779–85.
Barshes NR, et al. Combined lung and liver transplantation: the United States experience. Transplantation. 2005;80(9):1161–7.
De Domenico I, Ward DM, Kaplan J. Hepcidin and ferroportin: the new players in iron metabolism. Semin Liver Dis. 2011;31(3):272–9.
Pietrangelo A, Caleffi A, Corradini E. Non-HFE hepatic iron overload. Semin Liver Dis. 2011;31(3):302–18.
Evstatiev R, Gasche C. Iron sensing and signalling. Gut. 2012;61:933–52.
Donovan A, et al. The iron exporter ferroportin/Slc40a1 is essential for iron homeostasis. Cell Metab. 2005;1(3):191–200.
Vaulont S, et al. Of mice and men: the iron age. J Clin Invest. 2005;115(8):2079–82.
Pietrangelo A. Hepcidin in human iron disorders: therapeutic implications. J Hepatol. 2011;54(1):173–81.
Huang FW, et al. A mouse model of juvenile hemochromatosis. J Clin Invest. 2005;115(8):2187–91.
Feder JN, et al. A novel MHC class I-like gene is mutated in patients with hereditary haemochromatosis. Nat Genet. 1996;13(4):399–408.
Babitt JL, Lin HY. The molecular pathogenesis of hereditary hemochromatosis. Semin Liver Dis. 2011;31(3):280–92.
Phatak PD, et al. Prevalence of hereditary hemochromatosis in 16031 primary care patients. Ann Intern Med. 1998;129(11):954–61.
Olynyk JK, et al. A population-based study of the clinical expression of the hemochromatosis gene. N Engl J Med. 1999;341(10):718–24.
Edwards CQ, et al. Prevalence of hemochromatosis among 11,065 presumably healthy blood donors. N Engl J Med. 1988;318(21):1355–62.
Pietrangelo A. Hereditary hemochromatosis: pathogenesis, diagnosis, and treatment. Gastroenterology. 2010;139(2):393–408, 408 e1–2.
Pietrangelo A. Juvenile hemochromatosis. J Hepatol. 2006;45(6):892–4.
Adams PC, Kertesz AE, Valberg LS. Screening for hemochromatosis in children of homozygotes: prevalence and cost-effectiveness. Hepatology. 1995;22(6):1720–7.
Grove J, et al. Heterozygotes for HFE mutations have no increased risk of advanced alcoholic liver disease. Gut. 1998;43(2):262–6.
Bonkovsky HL, et al. Non-alcoholic steatohepatitis and iron: increased prevalence of mutations of the HFE gene in non-alcoholic steatohepatitis. J Hepatol. 1999;31(3):421–9.
Kowdley KV, et al. Utility of hepatic iron index in American patients with hereditary hemochromatosis: a multicenter study. Gastroenterology. 1997;113(4):1270–7.
Martin DR, Semelka RC. Magnetic resonance imaging of the liver: review of techniques and approach to common diseases. Semin Ultrasound CT MR. 2005;26(3):116–31.
Adams PC. Implications of genotyping of spouses to limit investigation of children in genetic hemochromatosis. Clin Genet. 1998;53(3):176–8.
Guyader D, et al. Noninvasive prediction of fibrosis in C282Y homozygous hemochromatosis. Gastroenterology. 1998;115(4):929–36.
Whitlock EP, et al. Screening for hereditary hemochromatosis: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2006;145(3):209–23.
Kumpe DA, et al. Partial splenic embolization in children with hypersplenism. Radiology. 1985;155(2):357–62.
Gehrke SG, et al. HJV gene mutations in European patients with juvenile hemochromatosis. Clin Genet. 2005;67(5):425–8.
Wolfe L, et al. Prevention of cardiac disease by subcutaneous deferoxamine in patients with thalassemia major. N Engl J Med. 1985;312(25):1600–3.
Nielsen P, et al. Liver iron stores in patients with secondary haemosiderosis under iron chelation therapy with deferoxamine or deferiprone. Br J Haematol. 1995;91(4):827–33.
Carneiro AA, et al. Liver iron concentration evaluated by two magnetic methods: magnetic resonance imaging and magnetic susceptometry. Magn Reson Med. 2005;54(1):122–8.
Brittenham GM, et al. Efficacy of deferoxamine in preventing complications of iron overload in patients with thalassemia major. N Engl J Med. 1994;331(9):567–73.
Cabibbo S, et al. Chronic red blood cell exchange to prevent clinical complications in sickle cell disease. Transfus Apher Sci. 2005;32(3):315–21.
Cappellini MD, Musallam KM, Taher AT. Overview of iron chelation therapy with desferrioxamine and deferiprone. Hemoglobin. 2009;33 Suppl 1:S58–69.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Narkewicz, M.R., Hurtado, C.W. (2014). Metabolic Liver Disease: Part 2. In: Murray, K., Horslen, S. (eds) Diseases of the Liver in Children. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-9005-0_9
Download citation
DOI: https://doi.org/10.1007/978-1-4614-9005-0_9
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-9004-3
Online ISBN: 978-1-4614-9005-0
eBook Packages: MedicineMedicine (R0)