
Abstract
Ultrasound is the most common and first-line imaging study performed in the genitourinary tract in children. It is used for screening and monitoring children even before birth. We provide a primer for the reader to understand the pertinent physics of ultrasonography by reviewing the physical properties of sound waves and their ability to capture images. Artifacts created by these physical properties are sometimes of diagnostic utility. The indications for performing ultrasound studies are described followed by a discussion of the technique and expected finding of normal ultrasound studies of the kidney, bladder, and testis in children.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Ultrasound is the most common imaging modality to study the genitourinary system in the pediatric population. While advances in other technologies further the ability to image the genitourinary tract, ultrasound has remained the imaging study of choice as it is noninvasive and involves no ionizing radiation, and the images are acquired quickly, in multiple planes in real time, without the need for sedation. There are portable units also available for clinical use. Ultrasound is a very advantageous imaging modality particularly for the young child, whose potential lack of cooperation may not allow a second chance to obtain imaging of the possible abnormality. It is also a relatively more cost-efficient imaging modality, as compared to CT scan and MRI. As significant numbers of prenatal ultrasounds are performed, many genitourinary abnormalities are being incidentally identified, requiring postnatal confirmation. The postnatal ultrasound has proven invaluable in identifying those patients for which additional imaging studies such as voiding cystourethrogram (VCUG), nuclear renography, CT, and MRI are indicated. Many children may need serial studies throughout the childhood to follow an abnormality, such as hydronephrosis. Ultrasound can also help identify patients where no further imaging workup is necessary. It has been also proven to be invaluable in the assessment of the acutely ill patient, being very highly sensitive and specific for certain diagnoses and can provide image guidance for procedures.
Background of Ultrasound
Ultrasound images are obtained by the interaction of sound waves with tissues and fluid. The term ultrasound is used as the frequency of the sound waves utilized is above the level which the human ear can detect—above 20 kHz. Ultrasound has its history in the development of SONAR, which means Sound Navigation and Ranging. Sound waves were used to help localize depth, such as structure in a lake. The piezoelectric effect was discovered in the late 1880s by the Curie brothers. With the advent of SONAR, new concepts of the physics of sound waves were being explored and new uses discovered. In 1955, Dr. Ian McDonald, seeing the application of ultrasound in the military, worked with several individuals to develop this technology for obstetrical and gynecologic patients. There were handful of indications for ultrasound in medical imaging, but its use was limited by the technology of the period.
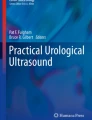
The basic ultrasound unit is composed of a transmitter, a transducer, an image display, and image storage system. There are three common types of sonographic image display used today (Fig. 2.1):

(a) An example of an A-mode scan. The received echo amplitude is plotted against time of transmission which is proportional to the depth. (b) In B-mode, the received echoes are displayed as a series of dots of varying brightness creating a two-dimensional image. (c) In M-mode, a diagram is created by graphing the received echoes on a plot of depth versus time (From Whittingham [2]. Reprinted with permission from Elsevier Limited)
A-mode (amplitude mode) ultrasound obtains echoes along a specified depth axis. After propagation through the tissues, the echoes that are returned are graphically displayed with the amplitude of the echo versus time. This appears on the screen as spikes along a horizontal line. This mode is particularly useful in situations that knowledge of the depth of the interface is desired and can be used therapeutically [1].
B-mode (brightness mode) ultrasound converts the received echoes into a series of dots of varying brightness, creating a two-dimensional grayscale image [2]. Early B-mode scanners required a patient to be placed in an immersion bath. In 1962, three men—Joseph Holmes, William Wright, and Ralph Meyerdirk—developed the compound contact B-mode scanner, revolutionizing ultrasound imaging in health care. Several more advances in B-mode scanners were developed in the 1970s.
When real-time capability was developed in B-mode, this became the dominant form of medical sonography. Real-time B-mode obtains information to create two-dimensional images that are used for the majority of medical imaging. For a given plane, multiple piezoelectric crystals are arrayed, and sound waves are sent and received and are then integrated to produce a grayscale image. The spectrum of grayscale brightness that is displayed for each received echo corresponds to the amplitude of the wave. The beam is rapidly and continuously reproduced and received to provide a dynamic, real-time image [1].
M-mode (motion mode) ultrasound obtains a series of B-mode signals, which are then displayed along a time axis, allowing for evaluation of the motion of a structure [1]. Therefore, at specific known depths from the transducer, the echoes are translated as motion of that structure. Short segments of the data can be stored digitally and played back instantly. Most common uses for this mode would be for analyzing movements of the heart or in obstetrics to isolate the beating heart of a fetus.
Basic Concept of Ultrasound
The ultrasound wave is produced by applying short burst of alternating electrical current to special crystals known as piezoelectric crystals, housed in the transducer, also known as a probe (Fig. 2.2). The electric current causes heating and polarizing of the lead atoms that are loosely bound within a crystal matrix. The crystal will then expand and contract, converting electrical energy into an acoustic wave. This phenomenon of converting electric energy into a pressure/sound wave energy and vice versa is known as the piezoelectric effect. Today these elements are commonly made from ceramic materials [3, 4].

The basic components of an ultrasound probe (From Whittingham [2]. Reprinted with permission from Elsevier Limited)
The frequency of the wave produced is dependent on the pulses of electrical current and the plate thickness of the piezoelectric material. Typical frequencies of ultrasound waves, i.e., transducers used in urological exams, are between 2.0 and 15 MHz, which are above the limits of human hearing. These acoustic waves are transmitted into the patient by the transducer, with the aid of a coupling gel, when the transducer is placed on the body. The efficiency of this process is improved by the presence of an impedance barrier, the rubber surface present on the transducer. These sound waves can then be reflected, refracted, scattered, or absorbed by the body.
The ultrasound wave is affected by the physical characteristics of the tissue through which it is propagated and then reflected. As the wave travels through the body, ultrasound echoes are received by the transducer. These echoes are then converted back into electric energy, which are then processed and translated into an image on the screen.
The Principles and Physics of Ultrasound in the Body
The ultrasound wave is a mechanical wave. Its movement through tissue causes oscillation of the tissue in a longitudinal direction, propagating the mechanical wave. As the ultrasound wave moves through different types of tissues, i.e., density, the elements of the tissue will oscillate higher or lower in relation to its ambient state, without net motion.
Frequency
The number of waves or pulses occurring in time, i.e., seconds, and is expressed in Hertz (Hz). Wavelength (λ) describes the physical space that one pulse length occupies. Frequency and wavelength are inversely related because of their relationship to velocity (velocity = frequency × wavelength). A higher frequency will result in a shorter wavelength and vice versa. For ultrasound imaging, the general ultrasound tissue velocity or speed is given as a constant (c) at 1,540 m/s [5, 6].
Assuming constant velocity (c), the depth (D) at which the interface occurred can be calculated as D = c/2 x (time from pulse generated to echodetection). The number 2 reflects that the wave traveled from the transducer to a point and the sound wave traveled back from that point, prior to being received by the transducer [4].
Amplitude
The maximum height or size that the wave travels in the positive or negative direction. The clinical significance of the wave amplitude is that it corresponds to the energy contained in the mechanical wave. Energy is equal to the amplitude squared. In clinical terms of the grayscale image, the amplitude affects the pixel brightness so that a greater amplitude wave produces pixels that are brighter [4].
Reflection
There are two types of wave reflections that occur and are received by the transducer that demonstrate clinical significance, specular echo and scatter echo.
When the transducer sends and receives a wave that is reflected off a smooth/flat surface, perpendicular to the angle of the moving sound wave, the echo is considered a specular or mirrorlike echo. The angle of reflection will be equal to the angle of incidence keeping with Snell’s Law. This type of echo, the specular echo, is characteristically reflected with the highest intensity strength and directionality. Specular echoes are seen from the linings of hollow viscera, blood vessels, fascial planes, organ capsules, skin, and gas or bone surfaces. To help correct for the speckling characteristic seen in some tissues, a technique called compounding can be used. Compounding sends sound waves into the tissue from multiples angles. Sending compound waves enables better image contrast by combining specular echoes, so they are more likely to be detected which results in minimizing speckling.
When sound waves are reflected off surfaces with irregularities, and the irregularities are similar in size to the wavelength of the sound wave, the energy of the wave is dispersed in all directions. This is known as scatter. The scatter echo returning to the transducer is therefore weaker and typically only detectible if several of the scattered wavelets are superimposed to produce an additive effect. Scattering accounts for the textured appearance of a tissue type, which is a result of an interference pattern, and is referred to as speckling. This property gives parenchyma such as the liver or testicles their characteristic appearance and makes them distinguishable from other structures. However, it should be noted that there is a spectrum between specular echoes and scattering with most tissues demonstrating properties that fall between the two extremes.
Rarefaction
It should also be stated that when a sound wave pulse is sent from the transducer, the wave does not necessarily propagate in a uniform and linear manner. Rather, the wave pulse becomes distorted as it travels through the tissue medium with some areas of the pulse having higher frequency components or harmonics corresponding to areas with increasing density of the medium. A portion of the wave would then travel faster than the rarefaction component of the wave which travels slightly slower. Rarefaction artifacts can occur therefore at the interface of two types of tissue as the angle of the sound wave is no longer linear. This can be seen at tissue interfaces such as fat and soft tissue or at soft tissue fluid interfaces. In the latter, the part of the beam that does not pass through the fluid is less intense that those traveling through the fluid structure. The difference in distortion is dependent on the initial sound wave intensity. The higher the acoustic power, the stronger the harmonics, and therefore a greater difference between the weaker sections of the wave frequency can occur. Stronger areas of the beam are typically located in the central section of the wave beam. Additionally, since it takes a few cycles to ramp up the intensities, frequencies are also weaker within the first few millimeters of tissue penetrated. Machines that filter out and select for a particular frequency produce a better image with improved contrast and counteract this distortion.
Absorption
The energy from the sound wave stimulates the tissue particles to move, enabling the sound wave to be transmitted as an acoustic vibration. If the tissue particles move in a cohesive and organized manner, then the vibration is transmitted efficiently. However, if the particle movement becomes chaotic and disjointed, then the sound wave will become chaotic, and the energy from the sound wave will be lost and converted into heat. When sound wave energy is lost by this method, it is referred to as absorption. Absorption is greater when the percentage of large particles in the tissue is increased; thus, the tissue has a greater viscosity. Similarly, absorption is dependent on the frequency of the sound wave with greater absorption occurring with higher frequencies. Per 1 cm depth of sound wave penetration, 1 dB is lost per 1 MHz transmitted. Thus, the higher the frequency, the more decibels are lost per centimeter of tissue causing the potential depth of penetration to be decreased. Since the speed of the sound wave traveling through soft tissues is constant, the time delay of the reflected sound wave can be used to calculate the depth of reflected image.
Attenuation
Anytime energy is lost and not returned to the transducer it is referred to as attenuation. Absorption is only one type of attenuation and was explained in the previous paragraph. Another type of attenuation occurs when the sound wave is reflected or refracted in such a way that the wave is unable to be returned in the same plane as to be detected by the receiving transducer. When a sound wave crosses an interface between two different tissues, some of the wave’s energy is reflected. The degree or proportion of the energy in the wave that is reflected is dependent on the change in the tissue density across that interface, also known as the impedance mismatch.
Typically, only a small percentage of reflection occurs with interfaces of similar tissues (<10 %). However, a tissue-gas interface leads to almost complete reflection of the wave and with tissue-bone or tissue-calculus interfaces resulting in almost 60–75 % of the wave being reflected. When this degree of reflection occurs, an acoustic shadow is then created. The acoustic shadow prevents visualization of structures deep to this interface as there had been almost complete reflection of the sound wave. The dark band is caused as the tissue absorbs the sound wave faster than the background, and the area deep to the highly attenuating region appears dark. Fat, gas, and calcifications are especially associated with shadowing (Fig. 2.3). Calcifications that are smaller than 5 mm will demonstrate shadowing when higher-resolution transducers are used. Similarly, aggregates of fine calcifications can shadow if their size and density is sufficiently high. Another type of shadowing is known as edge shadows or edge artifact that appears as fine, dark lines extending deep to curved surfaces. These are commonly seen in isolated cysts or at the edge of a testis (Fig. 2.4).

Arrow pointing to a calculus (white arrow) in the distal right ureter demonstrating the phenomenon known as shadowing (green arrow)

Edge artifact is demonstrated on both the superior and inferior edges of this testis (red arrows)
In contrast, there can be increased transmission when waves are less attenuated, such as transmission of sound waves through a simple cyst. The posterior wall of the cyst can artificially appear hyperechoic. This is known as through transmission (Fig. 2.5).

Cyst in left kidney mid pole demonstrates the phenomenon of through transmission (arrow)
Acoustic Impedance
This occurs at the interface of two tissue types, i.e., tissues with different densities. Part of the wave will be reflected and part will continue longitudinally through the tissues. The more different the tissues at the interface, the greater the contrast of the image obtained versus those of similar tissue density.
Acoustic Intensity
This is defined as the power per unit area of the ultrasound pulse. The more ultrasound waves concentrated in a smaller area, the more the intensity of the sound waves and the more detailed the image. The larger the cross-sectional energy, the less intensity per unit area, the lower the amplitude.
Resolution
This is defined as the ability to distinguish two objects that are in close proximity to one another. There are two types of resolution, axial resolution and lateral resolution, which are important in generating the image.
Axial resolution is the ability to differentiate between objects that are in the direction of the traveling wave or in front of one another. This property is dependent on the frequency of the sound wave. A higher frequency results in better image resolution due to the shorter sound wavelength, allowing for differentiation of objects that are close to each other. However, higher frequencies have more rapid attenuation as it passes through tissues, and resolution therefore is limited by depth.
Lateral resolution is the ability to identify two separate objects that are next to each other. This characteristic is dependent on both the focus width of the ultrasound wave beam and the transducer. The narrower beam of focus for a particular depth enables better lateral resolution. For a larger beam of focus, i.e., scanned field of view, the acoustic intensity is less resulting in less amplitude and less resolution. Remember also the average velocity of a wave in human tissues is given as constant at 1,540 m/s, and a change in frequency equals a change in wavelength [5, 6]. This ultimately affects the depth of resolution. At higher frequencies, shorter wavelengths are produced allowing better resolution of more superficial structures. For deeper structures, longer wavelengths are required with lower frequencies resulting in poor resolution. Typically for imaging structures such as the testicles or pediatric kidney, a higher frequency such as >7.5 MHz is used. But, for deeper structures such as the adolescent or adult kidney, 3.5–5 MHz is preferred.
The Transducers
There are many types of transducers available, each with its own advantages and disadvantages that make it uniquely suitable for various clinical applications of tissue imaging (Fig. 2.6). There are two general types of transducer classifications: mechanical and electronic steering. The mechanical types, of which there are two, rotating and oscillating, require the beam to be swept to image. The electronic steering transducers generate the beam sweep electronically by activating the crystal elements sequentially. The transducers used for conventional day-to-day imaging in the medical field are of the electronically steered category. The electronically steered transducers typically have a bandwidth of frequencies, such as 3–5 MHz or 6–15 MHz.

Three of the more commonly used transducers
Electronically arrayed probes are the most common type of probe and are beneficial due to their compact size without moving parts. They contain an array of transducer elements but currently are limited to using frequencies below 15 MHz. Most linear and curvilinear probes can consist of 128–256 narrow transducer elements; however, only approximately 30 adjacent elements will be used to send a pulse at one time [2]. After the pulse is transmitted and received, the beam steps the array by dropping an element from the end and adding an element to the opposite end. Focusing at the depth of the scanning plane is achieved by firing of the outer elements in the group earlier than the central elements. The receiving of the focused beam is automatically controlled to match the depth of the echo. For initial reception, only 2–4 elements are used for closer targets, but as the target is deeper, the number of elements used to receive the returning echoes is increased.
Phased array probes scan in a sector field of view. Typically, phased arrays contain an average of 128 narrow transducer elements, which are all used at one time for scanning the plane. After the initial transmission and reception, the beam is steered at a new angle, and the elements are fired at varying times to enable all elements to arrive at the same time at the targeted focus [2, 3]. A new focus automatically advanced along the scan line after each transmission.
Modern array probes typically combine both techniques of steeping and steering the firing elements. Trapezoidal or virtual curvilinear scans are examples of such probes. They have a field of view similar to that of the curvilinear probed but without the disadvantage of the convex face.
Linear array transducers produce sound waves parallel to each other and produce a rectangular image. The width of the image and number of scan lines are the same at all tissue levels. This has the advantage of good near-field resolution. These typically have higher frequency bandwidths such as 9 or 6–15 MHz [3].
Sector transducers also known as vector array transducers have a small footprint and create a fanlike image that is narrow near the transducer and increase in width with deeper penetration. It is widely used in echocardiography but has been proven to be very useful scanning abdominal organs in small infants, such as the kidneys.
Curvilinear array transducers can be thought of as a combination of the linear and sector transducers. The probe emits sound waves as a diverging field of view, as wide as the linear array at the surface but fanning out with increasing depth. These often have frequencies of 2–5 MHz, as the advantage of a larger field of view is at a greater depth from the probe. The density of the scan lines decreases with increasing distance from the transducer.
There are also multiple tools at the disposal of the sonographer on the machine—slider posts to control gain, the ability to add focal zones, control the frequency within the dynamic range of the transducer, zoom in on an image, and change the depth to mention a few.
Despite significant advances in ultrasound technology, there are limitations to achieving optimal resolutions at greater depths. These limitations prompted the development of intracavitary probes such as transrectal probes for imaging the prostate and endovaginal probes for gynecological examinations. As these probes are now in much closer proximity to what were traditionally deep structures from an anterior abdominal wall approach, they are typically able to operate at frequencies between 7 and 15 MHz and provide high-resolution images as the depth of penetration has been decreased [1, 3].
Overview of Common Ultrasound Real-Time B-Mode Imaging
Grayscale Ultrasound
Grayscale real-time B-mode is the most commonly used mode of ultrasonography. A two-dimensional image consisting of variations of gray coloration (brightness) is dependent on the amplitude of the reflected sound wave. Strong echoes or large amplitude waves will be represented by shades near the white end of the spectrum, and weak echoes or waves having small amplitudes will correspond to shades in the black part of the spectrum. The position of the pixel is determined by the time it takes for the sound wave to be reflected back to the transducer. With experience, practitioners are able to decipher normal and abnormal patterns of echogenicity for the specific structures and tissues.
Doppler Ultrasonography
Continuous wave Doppler enables motion to be captured such as blood cells traveling in vessels or particles of urine flowing into the bladder seen as ureteral jets. The principle of capturing motion is derived from the knowledge that sound wave frequency will be changed based on the direction and velocity of moving objects relative to the observer, a phenomenon known as the Doppler shift. The frequency of the reflected wave will be greater than the original frequency when contacting an object moving towards the transducer. Similarly, the reflected wave frequency will be smaller when contacting an objection moving away from the transducer. In continuous wave Doppler, therefore, the moving structure will reflect the beam at different frequencies, which are received by a parallel array of crystals. This then can be processed into an audible sound, with those of lower frequency registering a lower pitch/sound and higher frequencies a higher pitch/sound. Motion moving both towards and away from the transducer can be differentiated with color Doppler by assigning colors (conventionally blue and red) to objects moving towards and away from the transducer that is then superimposed on the grayscale image.
Duplex Ultrasound
Pulsed color wave Doppler occurs when pulses of sound are transmitted and received by the same transducer. This allows for the ability to assess depth of where the signal originated [7]. This limits the ability to assess very fast moving objects accurately. When employing pulse wave color Doppler, a small sample is interrogated, i.e., a “gated” sample. The B-mode scan image may have to be periodically updated when in pulse wave mode to verify gate placement. The sample window or gate can be wider or more focused as needed. The wider the gate, however, the less chance to detect small amounts of flow (Fig. 2.7).

Pulsed wave Doppler with color image aiding the placement of the sampling window to obtain an arterial tracing in a testicle. The flow is towards the transducer with the spectral waveform displayed above the baseline
Spectral Doppler refers to the graphic display of the changing velocities by a spectrum analyzer to aid in ease of interpretation. The spectral graph represents velocity on the vertical axis and time on the horizontal axis. Furthermore, the direction of flow towards the transducer is displayed above the baseline, and flow away from the transducer is depicted below. This can be done both for pulse wave and continuous color Doppler. The auditory signal again is processed so that one would hear a lower pitch hum sound for a slower moving vascular structure such as a vein as compared to the higher pitch variability sound of an artery (Fig. 2.8).

(a) Color Doppler image of the testes. Blue represents flow away from the transducer; red represents flow to the transducer in a different patient (b) power Doppler image which does not reflect direction but only the presence of Doppler flow
Power Doppler is another type of Doppler mode. Rather than assessing direction of flow or velocity, this mode assesses only intensity of signal. This is to aid for detection of blood flow in very small vessels and can be helpful also when optimal angles of insonation cannot be performed [7].
Attention to technique in the performance of Doppler imaging is paramount. The accuracy of the measured flow velocity is very dependent on the angle of the transmitted sound wave beam. The beam angle must measure the flow velocity at less than 90°, as the accuracy of the velocity is inversely proportional to the beam angle [7]. The reported error of a beam measured without an angle (0°) to the flow is minimal; however, angles measured at 60° and greater from the flow have large amounts of error and should not be used [5]. Additionally, the technologist/physician must ensure that the appropriate scale, wall filter, and PRF (pulse repetition frequency) are utilized, dictated by the type of exam and indication to optimally obtain Doppler signal.
Methods to Improve Image Quality
There have been many advances in the mechanics of ultrasound, to enhance image quality. To discuss all of the various technologies is beyond the scope of this chapter, but the more common advances to improve image quality in use and being evaluated are as follows:
Time Gain Compensation: TGC refers to the process where the received signals are all uniformly preamplified by application of depth-dependent echo gain factors so that the end result is that essentially the same type of reflective structures, regardless of depth, will have the same level of brightness. This process compensates for the attenuation of sound waves of deeper structures, allowing for visualization of both near-field and far-field structures at the same time. This is known also as swept gain and depth gain compensation [4].
Tissue Harmonics: This process takes advantage of the natural creation of harmonic waveforms within the soft tissues of the body. It was discovered by accident from experiments with microbubble contrast agents in ultrasound. During those experiments, it was noted that the tissue would generate a multiple of the fundamental wave and these harmonic waveforms could be received by the transducer. Stronger harmonic signals were generated at greater tissue depths, i.e., farther from the skin surface. Therefore, there is less artifact present from near-field acoustic reflective surfaces. As these received signals are generated by the body, there is less tissue to travel through resulting in a better signal-to-noise ratio. The beam itself is also narrower than the fundamental beam resulting in superior lateral resolution in the far field as compared to the fundamental beam. These factors result in sharper imaging at greater depths. Due to limitations of most commercially available transducers, it is the second harmonic wavelength which is twice the wavelength of the fundamental, i.e., transmitted, wavelength that is utilized [4].
Spatial Compounding: This process obtains information from several different angles of insonation and combines them to produce a single image. For a linear transducer, the multiple parallel lines would be obtained in several orientations. The echoes of the multiple acquired signals in the different orientations are then averaged, and a compound image is generated. This leads to less artifact including speckle and noise, thereby improving resolution [4].
Chip Encoding: One way to overcome the limitation inherent to higher frequencies and maintain resolution for greater depths is to use a method to transmit coded pulses. Such pulses are produced for a longer duration, and the frequency of each pulse is increased to a peak during the generation of the pulse. A scanner is used to condense these long pulses down into shorter pulses by utilizing a matched decoding filter. The result of the conversion is improved spatial resolution at greater depths by reducing the signal-to-noise ratio [4].
Ultrasound Contrast Agents: These agents have been in use for some time in Europe and Japan and are gaining popularity in the United States, with several investigations under way [8]. These contrast agents consist of microbubbles of air or perfluorocarbon gas stabilized by a protein, lipid, or polymer shell. The half-life of the bubble is a few minutes, enough to assess blood flow in the lesions in the liver or kidney, for example. As the gas diffuse out of the bubble, the bubble itself dissolves. It has also been used to detect vesicoureteral reflux [9]. Although US contrast material has been approved for clinical use for cardiac diagnosis in the United States for a number of years, its use for other radiologic indications, including uroradiologic, is currently under investigation [8, 9].
Performing GU-Indicated Ultrasounds in Children
Ultrasound imaging is performed in children for the purposes of investigation, screening, or surveillance (Table 2.1). It is important for the ultrasound to be performed in a systematic and standard fashion in order to yield a reproducible and clinically relevant study. While this principle is true for all imaging studies, it is particularly important in ultrasound as each study may vary with the skill and technique of the person performing the study.
Renal Ultrasound: The kidney is one component of a complete retroperitoneal ultrasound study. The other components include the abdominal aorta, origins of the common iliac arteries, the inferior vena cava, and any abnormalities encountered. The kidneys are imaged in both the longitudinal and transverse planes starting with the child in the supine position (Fig. 2.9). Asking the child to take a deep inspiration may improve visualization of the kidney, by causing it to move caudally below the ribs. In the young child or one who cannot follow such commands, a bolster placed under the flank or positioning the child on the side with the ipsilateral arm raised above the head may help open up the space between the ribs and the iliac crest which may allow for a better imaging window to access the kidney. If necessary, one can also try to image the child in the prone position to access the kidney between the ribs (Fig. 2.10). The right kidney is commonly imaged along the anterior axillary line, using the liver as an acoustic window. The left kidney is imaged along the mid- and posterior axillary lines, using the spleen as an acoustic window. Imaging is generally performed with a curved linear array probe using frequencies of 4–8 MHz for children under 18 months and 3.5–5 MHz probes for older children. The kidney’s location, orientation, axis, size, echogenicity of parenchyma compared to the liver, and corticomedullary differentiation are documented (Fig. 2.11). Any abnormalities of contour, duplication of the collecting system, visualization of proximal ureter, and the presence of stones, hydronephrosis, cysts, or masses should be evaluated and described. The physician and technologist must be aware of the unique features of a neonatal kidney as compared to older children and adults. There are standard charts that can be referred to regarding mean renal length by age [3].

Curvilinear ultrasound probe used during performance of a renal ultrasound. The probe is placed in the transverse (left) as well as sagittal (right) planes

Images (a) and (c) are obtained with pt in standard supine position with bowel gas obscuring portions of the kidneys. Same patient images (b) and (d) were obtained in the prone position with a bolster with improved visualization of the kidneys and more accurate measurements

Image of the right kidney in a child. There is corticomedullary differentiation with the medullary pyramids appearing as slightly darker triangular regions in the cortex. The renal sinus is more echogenic due to the presence of renal sinus fat
Bladder: The bladder is the major but not the only component of the pelvic ultrasound, which also includes the surrounding organs such as rectum, ovaries and uterus in girls, and prostate and seminal vesicles in boys. The bladder is imaged with the child in the supine position, commonly using a sector array probe using 4–8 MHz for children less than 18 months and curved array 3.5–5 MHz for older children. The bladder should be imaged in two orthogonal planes, traditionally transverse and longitudinal/coronal, with the bladder adequately distended. The bladder wall thickness is evaluated, as well as the intraluminal and extraluminal structures, noting if abnormalities such as dilated distal ureters, ureteroceles, abnormal echoes within the bladder, or a dilated proximal urethra known as the keyhole sign are present. Normal structures are documented as well such, as the uterus and ovaries, stool in rectum, and the prostate and seminal vesicles, and note is made if and how much free fluid is present posterior to the bladder. The transverse images are captured moving the probe caudally from the pubis to the umbilicus in 1–2 cm intervals. The longitudinal images are obtained moving from the midline in either direction at 1–2 cm intervals. Measurements recorded are the maximum height and width of the urine-distended bladder in the transverse plane and the length in the sagittal plane. Bladder volume can be determined by multiplying height, width, and length obtained by 0.65 – the standard formula of volume of an ellipsoid. Similarly, it is important to perform the study after voiding to assess the post-void residual or the presence of abnormalities suppressed by a distended bladder (Fig. 2.12). The color Doppler mode can be employed in the general region of the ureteral orifices along bladder floor to detect ureteral jets, i.e., efflux of urine into the bladder [1, 3] (Fig. 2.13).

Transverse images of the bladder. The top image, taken prior to voiding, demonstrates calculation of the ladder volume using three dimensions that can be related to expected bladder volumes for age. The bottom image demonstrates adequate emptying of the bladder of the same child

Images of the bladder. Color Doppler can be employed to help identify ureteral jets
Scrotum: The scrotal examine includes imaging of the testis, epididymis, and the spermatic cord and the scrotal wall. This evaluation is performed with the child in the supine position and the scrotum supported by a folded towel placed between the thighs. In older children and adolescents, the penis is positioned suprapubically and held in place with a second towel or by the patient. Scanning is performed using a high-frequency linear transducer such as 6–15 MHz. Both testes and epididymis should be compared together for size, echogenicity, and vascularity in the transverse and longitudinal axis (Figs. 2.14 and 2.15). Note should be made of any abnormal echotexture, mass, and presence or absence of hydrocele or varicocele. Spectral Doppler analysis of the bilateral intratesticular vasculature should be performed when indicated. In patients presenting with acute scrotum, the asymptomatic side should be scanned first so that grayscale and color Doppler gain settings are set as the baseline for comparison to the affected side. It is important that the parameters for both color Doppler and spectral Doppler imaging are set appropriately in order to optimally evaluate the intratesticular vessels, which can be very challenging in the prepubertal patient. These parameters may need to be set at low PRFs and low wall filters in order to document blood flow [3]. If a varicocele is suspected, the exam should be performed during a Valsalva maneuver and/or by placing the child in the upright position to optimize the chance of detecting the venous distention.

Normal scrotal ultrasound. The left image demonstrates a sagittal view of the testis and the head and tail of the epididymis. The right image demonstrates a transverse view documenting the presence of two homogeneous testes

Single longitudinal image through a testis with demonstration of the echogenic mediastinum and homogenous appearance to the testicular parenchyma
References
Sanders RC. Clinical sonography: a practical guide. 2nd ed. Boston: Little Brown and Company; 1991.
Whittingham TA. Medical diagnostic applications and sources. Prog Biophys Mol Biol. 2007;93:84–110.
Siegel M. Pediatric sonography. 3rd ed. Philadelphia: Lippincott, Williams &Wilkins; 2002.
Hangiandreou N. B mode US: basic concepts and new technology. Radiographics. 2003;23:1019–33.
Gilbert BR. Office scrotal ultrasound. Part I: ultrasound anatomy, physical principles and ultrasound safety. AUA Update Ser. 2008;27(1):1–7.
Levitov A, Levitov A. Chapter 2. Physics of sound, ultrasound and Doppler effect and its diagnostic utility. In: Levitov A, Mayo P, Slonim AD, editors. Critical care ultrasonography. New York: McGraw Hill; 2009.
Boote E. Doppler US techniques: concepts of blood flow detection and flow dynamics. Radiographics. 2003;23:1315–27.
Brannigan M, Burns P, Wilson S. Blood flow patterns in focal liver lesions at microbubble-enhanced US. Radiographics. 2004;24:921–35.
Darge K. Voiding urosonography with ultrasound contrast agents for the diagnosis of vesicoureteric reflux in children. Pediatr Radiol. 2008;38(1):40–53.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Rosen, J.C., Nicolay, L., Palmer, J.S. (2014). Principles of Ultrasound. In: Palmer, L., Palmer, J. (eds) Pediatric and Adolescent Urologic Imaging. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8654-1_2
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8654-1_2
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8653-4
Online ISBN: 978-1-4614-8654-1
eBook Packages: MedicineMedicine (R0)