
Abstract
The presacral or retrorectal space is the site of a group of heterogeneous and rare tumors that display indolent growth and produce ill-defined symptoms. As detection is often difficult and delayed, patients frequently present with tumors that have reached considerable size and involve multiple organ systems, complicating their treatment. The diagnosis and management of these tumors have evolved in recent years due to improved imaging modalities, a better understanding of tumor biology, adjuvant chemoradiation therapy, and a more aggressive surgical approach. Few surgeons have the opportunity to treat these complex lesions, and the care of these patients can be greatly optimized by an experienced, multidisciplinary team.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Malignant Peripheral Nerve Sheath Tumor
- Dermoid Cyst
- Preoperative Biopsy
- Aggressive Surgical Approach
- Presacral Space
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
-
The presacral or retrorectal space is the site of a group of heterogeneous and rare tumors that display indolent growth and produce ill-defined symptoms. As detection is often difficult and delayed, patients frequently present with tumors that have reached considerable size and involve multiple organ systems, complicating their treatment. The diagnosis and management of these tumors have evolved in recent years due to improved imaging modalities, a better understanding of tumor biology, adjuvant chemoradiation therapy, and a more aggressive surgical approach. Few surgeons have the opportunity to treat these complex lesions, and the care of these patients can be greatly optimized by an experienced, multidisciplinary team.
Anatomy and Neurophysiology
-
The boundaries of the retrorectal region include the posterior wall of the rectum anteriorly and the sacrum posteriorly (Fig. 21.1).
Fig. 21.1 
Relationship of pelvic structures to presacral space
-
This space extends superiorly to the peritoneal reflection and inferiorly to the rectosacral fascia and the supralevator space.
-
Laterally, the area is bordered by the ureters, the iliac vessels, and the sacral nerve roots (Fig. 21.2a).
Fig. 21.2 
(a) Anterior view of pelvic anatomy. (b) Posterior view or pelvic anatomy with sacral elements removed
-
-
Several important vascular and neural structures are located in this area and injury to them may have important physiologic rectoanal sequelae as well as neurologic and musculoskeletal consequences.
-
If all sacral roots on one side of the sacrum are sacrificed, the patient will continue to have normal anorectal function.
-
Likewise, if the upper three sacral nerve roots are left intact on either side of the sacrum, the patient’s ability to spontaneously defecate and to control anorectal contents will remain essentially intact.
-
If, however, both S-3 nerve roots are sacrificed, the external anal sphincter will no longer contract in response to gradual balloon dilation of the rectum, and this will translate clinically into variable degrees of anorectal incontinence and difficult defecation.
-
-
If sacrectomy is to be performed, the surgeon must be familiar with the relationship among the thecal sac, sacral nerve roots, sciatic nerve, piriformis muscle thecal sac, and sacrotuberous and sacrospinous ligaments (Fig. 21.2b).
-
Structurally, the majority of the sacrum can be resected; if more than half of the S-1 vertebral body remains intact, pelvic stability will be maintained.
-
However, preoperative radiation to the sacrum may ultimately lead to stress fractures if only S-1 remains. As such, spinopelvic stability may be augmented with fusion in select patients.
-
-
Knowledge of anatomy of the thigh and lower extremity is also required in complex cases requiring muscle or other soft tissue flaps. It is important to discuss with patients preoperatively the potential neuromuscular and visceral losses that may occur during the operation and how this will influence their function and quality of life.


Classification
General Considerations
-
Presacral lesions are rare. Reports from various large referral centers have indicated that their incidence may be as low as 1 in 40,000 hospital admissions (0.014 %).
-
Lesions found in the presacral space can be broadly classified as congenital or acquired and benign or malignant. Two-thirds of lesions are congenital, two-thirds of which are benign and one-third neoplastic.
-
As this area contains totipotential cells that differentiate into three germ cell layers, a multitude of tumor types may be encountered.
-
The classification first described by Uhlig and Johnson has been used for many years and divides tumors into broad categories; congenital, neurogenic, osseous, and miscellaneous. We have modified and updated this system to subcategorize tumors into malignant and benign entities, as this greatly impacts therapeutic approaches (Table 21.1 ).
Table 21.1 Classification of presacral tumors
Gross and Histologic Appearance
-
Epidermoid cysts result from defects during the closure of the ectodermal tube. They are histologically composed of stratified squamous cells, do not contain skin appendages, and are typically benign.
-
Dermoid cysts also arise from the ectoderm, but histologically they contain stratified squamous cells and skin appendages. These are also generally benign.
-
Epidermoid and dermoid cysts tend to be well circumscribed and round and have a thin outer layer. Occasionally, they communicate with the skin surface producing a characteristic postanal dimple. They are most common in females and the infection rate may be high as they are often misdiagnosed as a perirectal abscess and operatively manipulated.
-
Enterogenous cysts are lesions thought to originate from sequestration of the developing hindgut; if related with the rectum, they are called rectal duplication cysts. Because they originate from endodermal tissue, they can be lined with squamous, cuboidal, or columnar epithelium. Transitional epithelium may also be found. These lesions tend to be multilobular with one dominant lesion and smaller satellite cysts. Like dermoid and epidermoid cysts, they can become infected and are more common in women. These are generally benign, but case reports have described malignant transformation within rectal duplications.
-
Tailgut cysts, which are sometimes referred to as cystic hamartomas, are congenital lesions arising from remnants of normally regressing postanal primitive gut. They are more common in females and can be seen as multiloculated or biloculated cysts on magnetic resonance imaging (MRI) (Fig. 21.3). These cysts are composed of squamous, columnar, or transitional epithelium that may have a morphologic appearance similar to that of the adult or fetal intestinal tract. The presence of glandular or transitional epithelium differentiates this lesion from an epidermoid or dermoid cyst. Malignant transformation has been reported in up to 13 % in some series.
Fig. 21.3 
Tailgut cyst
-
Teratomas are true neoplasms derived from totipotential cells and include all three germ cell layers. They may undergo malignant transformation to squamous cell carcinoma arising from the ectodermal tissue or rhabdomyosarcoma arising from the mesenchymal cells. Anaplastic tumors are also seen in which the tissue of origin may not be distinguishable. Histologically, these tumors are referred to as either “mature” or “immature” reflecting the degree of cellular differentiation. Teratomas are more common in females and in the pediatric age group and are often associated with other anomalies of the vertebra, urinary tract, or anorectum. In adults, malignant degeneration can occur in 40–50 %. Incomplete or intralesional resection increases the likelihood of malignant degeneration. These lesions can also become infected and be misdiagnosed as a perirectal abscess or fistula. Diagnosis is often delayed and these tumors may reach considerable size.
-
Sacrococcygeal chordoma is the most common malignancy in the presacral space. These tumors are believed to originate from the primitive notochord which embryologically extends from the base of the occiput to the caudal limit in the embryo. They have a predilection for the pheno-occipital region at the base of the skull and for the sacrococcygeal region in the pelvis (Fig. 21.4). They predominate in men and are rarely encountered in patients younger than 30 years of age. These tumors may be soft, gelatinous, or firm and may invade, distend, or destroy bone and soft tissue. Hemorrhage and necrosis within tumors may lead to secondary calcification and pseudocapsule formation. Common symptoms include pelvic, buttock, and lower back pain aggravated by sitting and alleviated by standing or walking. Diagnosis is often delayed and these tumors may reach a considerable size. Although chordomas are low- to intermediate-grade malignant lesions, a radical surgical approach that achieves negative margins greatly improves survival.
Fig. 21.4 
Distribution of chordomas (Mayo Clinic orthopedic database)
-
Anterior sacral meningoceles are a result of a defect in the thecal sac and may be seen in combination with presacral cysts or lipomas. Typical symptoms include constipation, low back pain, and headache exacerbated by straining or coughing. Anterior sacral meningocele may be associated with other congenital anomalies, such as spina bifida, tethered spinal cord, uterine and vaginal duplication, or urinary tract or anal malformations. Surgical management consists of ligation of the dural defect.
-
Neurogenic tumors include neurilemmomas, ganglioneuromas, ganglioneuroblastomas, neurofibromas, neuroblastomas, ependymomas, and malignant peripheral nerve sheath tumors (neurofibrosarcoma, malignant schwannomas, and neurogenic sarcomas). In a Mayo Clinic series, schwannomas were the most common benign tumor and malignant peripheral nerve sheath tumors the most common malignant lesions. Although neurogenic tumors tend to slowly grow, they may eventually reach considerable size. Preoperative differentiation between benign and malignant pathology can be difficult without a tissue biopsy but is of paramount importance to guide the operative approach.
-
Osseous tumors include chondrosarcoma, osteosarcoma, myeloma, and Ewing’s sarcoma. These tumors arise from the bone, cartilage, fibrous tissue, and marrow. Due to relatively rapid growth, these lesions often reach considerable size, and pulmonary metastases are common. All osseous tumors of the presacral space are associated with sacral destruction. Although benign, giant-cell tumors are locally destructive and can metastasize to the lungs (“benign metastasizing giant-cell tumor”).
-
Miscellaneous lesions in this region include metastatic deposits, inflammatory lesions related to Crohn’s disease or diverticulitis, hematomas, and anomalous pelvic ectopic kidneys. Carcinoid tumors of the presacral space are unusual but have been reported.
-
Overall, most presacral tumors occur in females and are cystic.
-
Most solid tumors are chordomas and more commonly seen in males.
-
Benign lesions are frequently asymptomatic and are incidentally discovered during routine gynecologic examination which may explain the greater incidence in females.
-
By contrast, malignant tumors are more often symptomatic but still commonly found late due to their vague symptomatology.
-
Some presacral tumors present as part of a congenital syndrome, such as Currarino syndrome, which is a combination of presacral mass, anorectal malformations, and sacral anomalies. Diagnosis and Management
-


History and Physical Examination
-
Due to their indolent course, presacral tumors are commonly found incidentally at the time of periodic pelvic or rectal examination.
-
Symptomatic patients typically complain of vague, long-standing pain in the perineum or low back.
-
Pain may be aggravated by sitting and improved by standing or walking.
-
Several clues may alert the clinician to the presence of a retrorectal cystic lesion, including repeated operations for anal fistula, the inability of the examiner to uncover the primary source of infection at the level of the dentate line, a postanal dimple, or fullness and fixation of the precoccygeal area.
-
Some patients may give a history of referral to a psychiatrist because of clinicians’ inability to ascertain the origin of their chronic, ill-defined pain. Patients with larger tumors may complain of constipation and/or rectal and urinary incontinence and sexual dysfunction due to the sacral nerve root involvement.
-
Patients should be carefully examined, focusing on the perineum and rectal examination and assessing for a postanal dimple.
-
In a series from our institution, 97 % of presacral tumors could be palpated on rectal exam. Digital rectal exam (DRE) typically reveals the presence of an extrarectal mass displacing the rectum anteriorly with a smooth and intact overlying mucosa. Rectal examination is also critical in assessing the level of the uppermost portion of the lesion, degree and extent of fixation, and relationship to other pelvic organs, such as the prostate.
-
Rigid or flexible sigmoidoscopy can be used to assess the overlying mucosa and rule out transmural penetration of the tumor.
-
A careful neurologic exam focusing on the sacral nerves and musculoskeletal reflexes is mandatory and may also aid in the diagnosis of extensive local tumor invasion.
Diagnostic Tests
-
The presence of a presacral tumor can be confirmed with imaging modalities such as computerized tomography (CT), MRI, and endorectal ultrasound (ERUS). Simple anterior-posterior and lateral radiographs (AP/LAT) of the sacrum can identify osseous expansion, destruction, and/or calcification of soft tissue masses, but are typically not helpful in rendering a specific diagnosis.
-
A chordoma is the most common tumor causing these findings, but sarcomas or benign, locally aggressive tumors, such as giant-cell tumor, neurilemmoma (schwannoma), and aneurysmal bone cysts, may also cause extensive bony destruction.
-
The characteristic “scimitar sign” on plain radiographs denotes the presence of an anterior sacral meningocele, a diagnosis that can be confirmed with conventional myelography or MRI with gadolinium.
-
CT, MRI, and positron emission tomography (PET) scan have dramatically changed the way in which these tumors are evaluated. Computerized tomography and MRI complement each other and are the most important radiographic studies in evaluating a patient with a presacral lesion. Computerized tomography can determine whether a lesion is solid or cystic and whether adjacent structures, such as the bladder, ureters, and rectum, are involved (Fig. 21.5a–c). CT is also the best study to evaluate cortical bone destruction. MRI is highly recommended because of its multiplanar capacity and improved soft tissue resolution that is essential for planning specific lines of resection (Fig. 21.6a, b). Sagittal views assist in decision making in regard to need for and level of sacrectomy (Fig. 21.6c). MRI is also more sensitive than is CT in spinal imaging, showing associated cord anomalies, such as a meningocele, nerve root, and foraminal encroachment by tumor or thecal sac compression.
Fig. 21.5 
Massive cystic teratoma with sacral appendage. (a) CT image of teratoma, intrapelvic portion and (b) extrapelvic portion, (c) including fully developed phalanx
Fig. 21.6 
MRI of pelvic neurofibroma displacing the rectum anteriorly and laterally. (a) T1-weighted coronal image. (b) T2-weighted coronal image. (c) Sagittal view with tumor exiting the third sacral foramen
-
In patients with presacral cystic lesions thought to be the source of a chronically draining sinus, fistulogram may occasionally help clarify the diagnosis. ERUS has been used by some to characterize retrorectal tumors and its relationship to the muscularis propria of the rectum.


Preoperative Biopsy
-
Historically, the role of preoperative biopsy of presacral tumors has been a controversial topic.
-
In the past, some authors have considered any presacral tumor deemed resectable as a contraindication to preoperative biopsy, with only a minority of authors stating that all solid tumors should be preoperatively sampled by biopsy. This recommendation in part may have to do with the fact that the literature on this topic is sparse and outdated, especially when one considers the availability of modern imaging, better knowledge of tumor biology, and new opportunities for neoadjuvant therapy. Indeed, some patients substantially benefit from preoperative chemotherapy and radiation, especially in osseous tumors, such as Ewing’s sarcoma, osteogenic sarcoma, and neurofibrosarcoma. Preoperative tissue diagnosis is essential to the management of solid and heterogeneously cystic presacral tumors. For example, the surgical approach and necessary margins is dramatically different when faced with a neurofibroma as compared to a neurofibrosarcoma.
-
When performed correctly, preoperative biopsy can only improve the overall management, rather than harm it.
-
What is clear about preoperative biopsies of presacral tumors is that they should never be transrectally or transvaginally performed. In the presence of a cystic lesion, such an approach is likely to result in infection rendering its future complete excision more difficult and increasing the likelihood of postoperative complications and recurrence. More importantly, inadvertent transrectal needling of a meningocele may lead to disastrous sequelae, such as meningitis and even subsequent death. Moreover, as the biopsy tract needs to be removed en bloc with the specimen, transrectal biopsy would mandate proctectomy in a patient whose rectum may otherwise have been spared.
-
There is rarely an indication to biopsy a purely cystic presacral lesion. From a technical standpoint, a presacral tumor biopsy should be done by a radiologist with experience in the evaluation and management of pelvic tumors. In planning the approach for a biopsy, the surgeon should always consider the resection margins so that the needle tract can be removed en bloc with the specimen. The transperineal or parasacral approach is usually ideal and falls within the field of the pending surgical resection (Fig. 21.7a, b). Transperitoneal, transretroperitoneal, transvaginal, and transrectal biopsy should be avoided. Biopsy tracts should never traverse neurovascular planes. Normal coagulation studies are required prior to biopsy, as hematoma formation and/or bleeding potentially contaminate(s) involved areas. PET-CT scan can be useful to guide biopsy needles into small focal areas of high tumor density.
Fig. 21.7 
(a) Preoperative biopsy technique using CT guidance. (b) Parasacral approach to presacral neurogenic tumor

Role of Preoperative Neoadjuvant Therapy
-
Modern protocols and the wide availability of neoadjuvant tumor irradiation and systemic chemotherapy have revolutionized the management of patients with complex malignancies. It is in large part due to these new treatment modalities prior to surgery that a preoperative diagnosis is of paramount importance.
-
One of the significant advantages of preoperative irradiation is that it allows treatment to a smaller radiation field. Postoperative irradiation for a pelvic tumor would require irradiation of the entire surgical bed, previous tumor site, all contaminated surgical planes, and the sites of all skin incisions. This increased radiation exposure is associated with increased morbidity. Furthermore, should “spillage” occur during resection of a radiosensitive tumor, this contamination may be with previously irradiated necrotic, nonviable cells. A third, and perhaps most important, advantage of preoperative irradiation in sensitive tumors is the fact that decreased tumor size is often observed. A decrease in tumor size in a pelvic tumor may allow the surgeon to spare vital structures, which would have had to be sacrificed in order for wide margins to be achieved without prior radiation. Additionally, a smaller tumor often means a surgery of a lesser magnitude and therefore less risk for intraoperative complications.
-
Large tumors in the presacral space, especially sarcomas, are notorious for systemic metastasis. Neoadjuvant chemotherapy is the cornerstone of treatment for diagnoses such as Ewing’s sarcoma and osteogenic sarcoma.
-
Most non-chordoma malignant presacral tumors are sarcomas. The use of adjuvant therapy for presacral sarcomas in our recent review followed protocols typically for other types of soft tissue sarcomas.
-
Regarding malignant neurogenic tumors, the use of adjuvant therapy has been recently reported by our institution.
Surgical Treatment
Rationale for Aggressive Approach
-
The rationale for an aggressive surgical approach for presacral tumors is based on several arguments. The lesion may already be malignant or transform into a malignant state if left in place. In patients with teratomas, especially those patients in the pediatric age group, the risk of malignant transformation is considerable and continues to dramatically increase if removal is delayed or incomplete. Untreated anterior sacral meningoceles may become infected and lead to meningitis, which is associated with high mortality. Cystic lesions may become infected making their excision difficult and increasing the possibility of postoperative infection and future recurrence. A presacral mass in a young woman may cause dystocia at the time of delivery. Lastly, benign and malignant tumors left untreated may grow to considerable size making surgical resection much more complicated.
-
In the past, many surgeons have adopted a rather defeatist attitude toward sacrococcygeal chordomas and other tumors in this area based on a number of erroneous misconceptions. Presacral tumors may produce vague symptoms, which leads to a delay in diagnosis for months or even years. Thus, patients may seek medical treatment late in the course of their disease, and the presence of a large mass in this often unfamiliar and complex anatomic area makes some surgeons reluctant to consider aggressive surgical approach for fear of serious operative and postoperative complications.
-
Finally, and most importantly, tumors in this area have been inadequately treated in the past because of tumor violation, their large size and location, and fear of neurologic complication and/or musculoskeletal instability. Preoperative tumor violation can take place when such tumors are biopsied or intraoperatively when margins of resection are inadequate or tumor cells are spilled in an effort to be too conservative. When a surgeon is attempting to avoid injury to the rectal wall or important neurologic structures, they may inappropriately restrict excision and compromise oncologic outcome. For malignant lesions wide, en bloc removal of adjacent organs, soft tissue, and bone (if locally adherent) is the goal of resection.
Role of Multidisciplinary Team
-
It is of great importance that an experienced team consisting of a colorectal surgeon, orthopedic oncologic surgeon, spine surgeon, urologist, plastic surgeon, vascular surgeon, musculoskeletal radiologist, medical oncologist, radiation oncologist, and specialized anesthesiologist evaluate and surgically treat tumors that are large and extend to or destroy the hemipelvis or the upper half of the sacrum.
Surgical Approach
-
Careful surgical planning is important in deciding how to approach these tumors whether it be an anterior approach (abdominal), posterior approach (perineal), or a combined abdominoperineal approach. Computerized tomography and MRI help define the margins of resection and the relationship of the tumor to the sacral level (Fig. 21.8). Small and low-lying lesions can be removed transperineally through a parasacral incision, whereas tumors extending above the S-3 level, especially if large, often require a combined anterior and posterior approach.
Fig. 21.8 
Relationship of tumor to sacral level and proposed approach
-
For large malignant lesions requiring extended resection, a plastic surgeon plays a significant role, as adequate soft tissue coverage can often be difficult. Most often, the authors use the transabdominal rectus abdominis myocutaneous (TRAM) flap, which fills dead space and can cover large cutaneous defects left by the resection.

Preoperative Considerations
-
Optimizing patients for surgery is of extreme importance in a majority of these cases.
-
Adequate nutritional repletion with total parenteral nutrition or with a feeding tube may be necessary in patients who present severely debilitated.
-
In technically complex cases, when we expect a long operative time and significant debilitation postoperatively, we consider placement of a temporary intravena caval filter, since the risk of deep venous thrombosis and pulmonary embolus is high and postoperative anticoagulation may be contraindicated.
-
Preoperative selective coil embolization done by an interventional radiologist may be useful in patients with large, vascular tumors to decrease intraoperative bleeding.
-
A multidisciplinary team should preoperatively review films and plan surgical strategy to avoid confusion during the day of surgery.
-
An operating theater capable of managing massive transfusion requirements is mandatory, as is an anesthesiologist comfortable with the physiologic management needed during the procedure.
-
Posterior Approach
-
For low-lying tumors, the patient is placed in the prone jackknife position with the buttocks spread with tape (Fig. 21.9a).
Fig. 21.9 
(a) Positioning for posterior approach. (b) Coccygectomy. (c) Index finger in the anal canal to “push” tumor outward facilitating dissection
-
An incision is made over the lower portion of the sacrum and coccyx down to the anus taking care to avoid damage to the external sphincter. Resection of the tumor may be facilitated by transection of the anococcygeal ligament and coccyx (Fig. 21.9b).
-
The lesion can then be dissected from the surrounding tissues, including the rectal wall, in a plane between the retrorectal fat and the tumor mass itself. In the case of very small lesions, the surgeon may double-glove the left hand and, with the index finger in the anal canal and lower rectum, push the lesion outward, away from the depths of the wound (Fig. 21.9c) facilitating dissection of the lesion off the wall of the rectum without injury. If necessary, the lower sacrum or coccyx or both can be excised en bloc with the lesion to facilitate excision.
-
An intersphincteric approach has been described for very low-lying tumors. It is performed in a lithotomy position. Through a V-shaped or radial incision posterior to the anus, the intersphincteric plane is opened and bluntly dissected. The anal canal and internal sphincter are separated from the external sphincter up to the level of the puborectalis sling. The dissection is continued upward in the retrorectal fatty space. The division of Waldeyer’s fascia may be necessary to expose the upper surface of the levator ani muscles.
-

Combined Abdominal and Sacral-Perineal Approach
-
If the upper pole of the tumor extends clearly above the S-3 level, an anterior and posterior approach is usually indicated.
-
Patients may be placed in the supine or lateral position, depending on the surgeon’s preference and previous experience. A variety of techniques and positioning to the abdominal-perineal approach have been described. If an anterior-posterior approach is necessary, the patient can be placed in a “sloppy-lateral” position to facilitate a simultaneous two-team approach (Fig. 21.10a–c).
Fig. 21.10 
(a) Modified lateral position for anterior exposure via a midline (solid line) or ilioinguinal (dashed line) incision. (b) Anterior exposure of the vessels and tumor. (c) Posterior approach to the sacrum (dashed line)
-
We always recommend cystoscopy and bilateral ureteral stent placement before laparotomy.
-
Through a midline incision, the abdomen should be carefully examined to rule out metastasis or other important pathology.
-
After the lateral attachments to the sigmoid have been mobilized and the presacral space is entered just below the promontory, the posterior rectum can be dissected from the upper sacrum down to the upper extension of the tumor. The ureters and hypogastric nerves are identified and protected. The rectum can then be mobilized laterally and, if necessary, anteriorly.
-
If a malignant tumor can be safely separated from the posterior wall of the rectum without compromising a wide margin, the lesion can be dissected in a plane between its capsule and the mesorectal fat to preserve the rectum. If the tumor is extremely large, markedly compressing and displacing the rectum, making dissection between the rectal vault and the tumor hazardous, one should remove the rectum en bloc with the tumor and the involved segments of the sacrum. It is mandatory in malignant cases that no structures attached to the specimen should be separated with dissection and that they are removed en bloc with the primary tumor mass.
-
In the presence of very large tumors, blood loss during the procedure can be substantial. These potentially adverse sequelae may be minimized by ligating the middle and lateral sacral vessels and both the internal iliac arteries and veins (Fig. 21.11). When ligating the internal iliac artery, in order to reduce the risk of perineal necrosis, it is best to preserve the anterior division from which the inferior gluteal artery arises. This maneuver is often performed in conjunction with permissive hypotension. A vascular surgeon can be helpful during this portion of the procedure especially in patients that have had prior irradiation or have distorted vascular anatomy.
Fig. 21.11 
Ligation of the middle sacral and internal iliac vessel
-
There have been reports using minimally invasive laparoscopic techniques as an approach for presacral tumor resection, both for anterior-only and for anterior-posterior approaches. If the anterior portion of a combined anterior-posterior approach can be done laparoscopically (rectum divided, colostomy made, tumor partially mobilized, vasculature ligated), it should decrease the morbidity of the overall operation significantly.


Follow-Up Considerations
-
The authors recommend an annual visit, including a digital rectal examination, to assess for recurrence of a benign lesion. If digital rectal examination reveals a mass, a CT scan is done. We recommend a baseline CT at 1 year following surgery and then repeated at every 5 years, even if examination is normal.
-
In the case of malignant tumors, the patients are closely followed with particular attention to local recurrence and pulmonary metastasis. An annual pelvic MRI and chest CT scan are performed for the first 5 years. If the patient rectum was left in place, annual DRE with possible anoscopy is performed by the colorectal surgeon. Patients are offered repeat resection for locally advanced tumors and for pulmonary metastasis if all disease can be removed operatively.
Results of Treatment
Malignant Lesions
-
Results of surgical treatment of presacral lesions depend on both the natural behavior of the tumor and the adequacy of resection. If wide margins were not achieved during resection of a malignant lesion or if the tumor is violated, one can expect a high local recurrence rate and a poor overall outcome. In general, most malignant tumors reported in the literature have had a rather poor prognosis, but many such tumors had been incompletely resected or excised piecemeal, breaking oncologic principles.
Congenital Cystic Lesions
-
In general, cystic lesions can be treated adequately by complete excision via a posterior approach. Large cystic lesions such as teratomas extending high into the pelvis can be excised via a combined abdominal-perineal approach. There continues to be some debate as to whether or not a coccygectomy needs to be done for all resections of congenital cystic lesions.
Algorithm
-
Based on the experience at our institution, we have established a decision-making algorithm to guide the management of presacral tumors (Fig. 21.12).
Fig. 21.12 
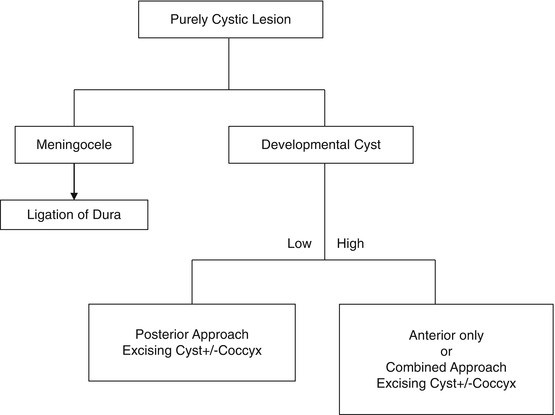
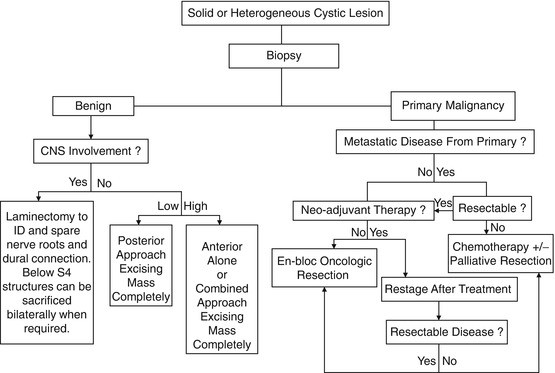
Proposed treatment algorithm



Conclusions
-
Presacral tumors are rare, the differential diagnosis is extensive, and their discovery is notoriously difficult and late. A high index of suspicion is needed to identify these patients.
-
Once a benign or malignant presacral lesion is discovered and histologically diagnosed, it should be treated, even if the patient is asymptomatic. CT and MRI imaging can help differentiate between benign and malignant and cystic and solid and accurately define the extent of adjacent organ and bony involvement to guide operative planning.
-
Completely cystic lesions, in general, do not require preoperative biopsy unless malignancy is suspected. All solid tumors and heterogeneous cysts should be considered for biopsy to rule out malignancy, guide neoadjuvant therapy, and plan the extent of resection.
-
An aggressive approach, by an experienced, multidisciplinary team, that can achieve a tumor-free, en bloc resection, avoid tumor violation, restore spinopelvic stability, and minimize intraoperative and postoperative complications should decrease the risk of local recurrence and improve survival. Minimally invasive approaches may improve overall recovery and the quality of life in selected patients.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Dozois, E.J., Marcos, M.D.H. (2014). Presacral Tumors. In: Beck, D., et al. The ASCRS Manual of Colon and Rectal Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8450-9_21
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8450-9_21
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8449-3
Online ISBN: 978-1-4614-8450-9
eBook Packages: MedicineMedicine (R0)