
Abstract
-
With any significant degree of adhesiolysis, there is an increased risk of enterotomies. Therefore, the entire bowel should be carefully inspected at the end of the procedure.
-
All serosal tears should be repaired with imbricating seromuscular sutures in either a single- or two-layer closure.
-
A bowel resection with anastomosis may be needed if there are multiple full-thickness enterotomies in a short segment of bowel. The viability of the ends should be confirmed if there was any mesenteric injury.
-
Long longitudinal seromyotomies may be treated by conversion to a full-thickness laceration and closure in a strictureplasty fashion.
-
Failure to recognize and repair an enterotomy may lead to peritonitis which may be difficult to detect in the first 24–48 h after surgery.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Unrecognized Enterotomies and Enterocutaneous Fistulae
-
With any significant degree of adhesiolysis, there is an increased risk of enterotomies. Therefore, the entire bowel should be carefully inspected at the end of the procedure.
-
All serosal tears should be repaired with imbricating seromuscular sutures in either a single- or two-layer closure.
-
A bowel resection with anastomosis may be needed if there are multiple full-thickness enterotomies in a short segment of bowel. The viability of the ends should be confirmed if there was any mesenteric injury.
-
Long longitudinal seromyotomies may be treated by conversion to a full-thickness laceration and closure in a strictureplasty fashion.
-
Failure to recognize and repair an enterotomy may lead to peritonitis which may be difficult to detect in the first 24–48 h after surgery. A high index of suspicion with a low threshold for re-exploration is required as the usual markers of bowel perforation (leukocytosis, fever, and pneumoperitoneum) may not be reliable.
-
At reoperation for a missed enterotomy in the early postoperative period, if the edges are viable, a primary repair can be done. If conditions are not favorable, a diverting stoma should be considered proximal to the repair.
-
At relaparotomy, if bilious fluid is encountered and no enterotomy is found, a duodenal, gastric, or gallbladder injury must be excluded. Insufflation of the small bowel with gas via an NG tube and filling the abdomen with saline may help localize the enterotomy. If still no enterotomy is found, drains can be placed in each paracolic gutter and the pelvis in hopes of allowing a controlled enterocutaneous fistula to develop.
-
An unrecognized enterotomy, presenting with enteric drainage from the incision, may be nonoperatively managed if there are no signs of sepsis.
-
Any reoperation after the first postoperative week is often extremely difficult as dense vascular adhesions may be encountered and the risk of making further enterotomies or a mesenteric vascular injury is high. Therefore, complete bowel rest, a nasogastric tube, nutritional support, and broad-spectrum antibiotics are initiated.
-
A computed tomography scan is obtained to look for an abscess or undrained fluid. A collection >4 cm may be percutaneously drained.
-
Assistance by an enterostomal therapist (WOCN) regarding skin care and pouching the fistula may be helpful.
-
Total parenteral nutrition may be required if the fistula output is high. H2 antagonists may be added to the TPN.
-
Somatostatin analogs may be useful to decrease the volume of the fistula output but do not improve the rate of fistula closure.
-
Spontaneous fistula closure is typically less than 50 %. Factors attributed to reduced fistula closure rates are high output (because of proximal location), distal obstruction, local sepsis, radiation exposure, short or epithelialized tract, malignancy, foreign body in the tract (such as mesh or sutures), Crohn’s disease, and malnutrition.
-
Enterocutaneous fistulas that close typically do so within the first month.
-
Fibrin glue has been described. The success rate is low, but nothing is lost in trying this technique.
-
Surgical intervention should be delayed until all sepsis is resolved, adequate nutrition is restored, and intra-abdominal adhesions have softened to allow for a safe reoperation. Surgery should be delayed at least 6 weeks from the time of the last laparotomy, but 3–6 months may be more appropriate. The longer one waits until reoperation the better. Delay must be balanced against the patient’s medical and social condition.
Anastomotic Complications
-
Anastomotic complications are usually related to technical factors such as ischemia, tension, poor technique, stapler malfunction, or preexisting conditions such as local sepsis, poor nutrition, immunosuppression, morbid obesity, and radiation exposure.
-
Division of the lateral attachments of the descending colon, complete mobilization of the splenic flexure, high ligation of the inferior mesenteric artery, separation of the omentum from the distal transverse colon and mesocolon, and division of the inferior mesenteric vein at the lower edge of the pancreas are techniques to aid in the creation of a tension-free colorectal anastomosis.
-
To reduce the risk of anastomotic ischemia, adequate bleeding should be noted at the cut edge of the bowel along with pulsatile bleeding from the divided marginal artery.
-
When the distal transverse colon is the proximal end of a colorectal anastomosis, additional length to obtain a tension-free anastomosis may be obtained by passing the colon through the ileal mesentery (behind the terminal ileum) before being brought into the pelvis.
-
If severe malnutrition (albumin <2.0 or weight loss >15 %) or significant immunosuppression (chemotherapy, high-dose steroids, antitumor necrosis factor drugs) is present, an end colostomy and Hartmann stump or proximal ileostomy should be considered to minimize the risk of anastomotic complications.
-
An ileostomy can be closed at 1.5–3 months. A laparotomy for a Hartmann reversal is generally deferred for 6 months.
-
Before a Hartmann reversal, obese patients are encouraged to lose weight which allows for easier construction of a deep pelvic anastomosis.
-
When operating on irradiated bowel, one end of an anastomosis should be from nonirradiated bowel. Intersecting staple lines (such as double-stapled technique) may have a higher predisposition to leak and a single-stapled or handsewn anastomosis may be considered.
-
Table 10.1 lists the steps to minimize a leak from an anastomosis.
Table 10.1 Steps to minimize risk of leak from colorectal or coloanal anastomosis
Bleeding
-
Most anastomotic bleeding is minor and manifested by dark blood mixed in the first bowel movement after surgery.
-
Bleeding can occur after a stapled or handsewn anastomosis but is probably more common after one is stapled. Careful inspection can allow intraoperative control of the bleeding and reduce the postoperative risk. Also stapling a side-to-side anastomosis using the antimesenteric border (avoiding inclusion of the mesentery) reduces the risk of bleeding.
-
Bleeding points on a stapled anastomosis should be controlled with a suture rather than the Bovie as a deep burn injury may lead to a delayed leak. Full-thickness staple line reinforcement with interrupted sutures can help ensure optimal hemostasis.
-
Delayed detection of bleeding from a circular stapler or staple line of a J pouch (ileal or colonic) may need to be addressed on the ward. Steps to control bleeding include:
-
1.
Proctoscopy is done to evacuate all clots.
-
2.
A rectal tube (or Foley) is inserted and 1:100,000 epinephrine solution is instilled. The tube is clamped and the solution remains in the rectum/neorectum for 15 min.
-
3.
If the bleeding persists, the procedure is repeated. Endoscopic cautery or epinephrine injection is another option.
-
4.
If the bleeding continues to persist or the patient has hypotension, a transanal examination in the operating room is carried out.
-
1.
-
Treatment for delayed bleeding from an inaccessible anastomosis (such as an ileocolic) usually begins with supportive care including correction of any coagulopathy.
-
Angiography may be required to localize the site and allow selective vasopressin infusion.
-
Alternately using a colonoscope, if the bleeding site can be visualized, it can be treated with cautery, epinephrine injection, or endoscopic clips.
-
Rarely reoperation with oversewing is required.
-
Leaks
-
The lowest leak rate is found after a small bowel or ileocolic anastomosis (1–3 %).
-
The highest leak rate is after a coloanal anastomosis (10–20 %). The incidence of leak is strongly associated with the distance of the anastomosis from the anal verge.
-
The ileal pouch-anal anastomosis has a leak rate of 5–10 %.
-
Immunosuppressive drug therapy (prednisone >40 mg/day and antitumor necrosis factor alpha agents) is a significant risk factor associated with an ileal pouch-anal anastomotic leak.
Role of Fecal Diversion
-
A proximal stoma minimizes the consequences of an anastomotic leak but does not reduce the actual incidence of a leak.
-
A proximal stoma may reduce the need for surgical intervention should a leak occur.
-
Table 10.2 lists indications when a diverting ileostomy should be considered.
Table 10.2 Indications for a diverting loop ileostomy -
Patients with comorbidities who lack the “physiologic reserve” to tolerate an anastomotic leak should strongly be considered for proximal diversion even if other risk factors are not present.
-
Neoadjuvant radiation therapy in patients undergoing a low pelvic anastomosis for rectal cancer does not appear to increase the incidence of an anastomotic leak. However, surgeons tend to cover this anastomosis with a proximal stoma which may reduce the clinical manifestations of a leak.
Role of Pelvic Drains
-
The use of a drain to minimize the risk of an anastomotic leak is controversial, and the use of a drain has been shown to neither harm nor benefit an anastomosis.
-
One study did show the use of a drain reduced the incidence of clinical anastomotic leak after short-course neoadjuvant radiation therapy.
Diagnosis and Management of Anastomotic Leak
-
Free anastomotic leaks are leaks with fecal contents spread throughout the abdominal cavity.
-
Patients present with fever, tachycardia, hypotension, leukocytosis, and peritonitis.
-
Feculent fluid may egress via the surgical incision (or pelvic drain if present).
-
Radiological studies may localize the leak but should not delay reoperation.
-
Patients with a free leak should be taken to the operating room after fluid resuscitation and intravenous antibiotics are administered.
-
After a thorough washout, the treatment is dictated by the findings.
-
Most colorectal anastomosis will require anastomotic takedown and an end colostomy.
-
To minimize the effects of a friable rectal stump (that cannot be closed with staples or sutures nor brought to the skin surface as a mucous fistula), placement of transabdominal and transanal drains is indicated.
-
Selective small bowel or ileocolic anastomotic defects can be repaired. However, resection of the anastomosis with creation of a new anastomosis or stoma is the most conservative option.
-
Placement of the repaired anastomosis under the surgical incision will result in an enterocutaneous fistula instead of a second bout of peritonitis should a second leak occur.
-
Any concern regarding viability of the bowel ends necessitates takedown of the anastomosis and creation of a stoma.
-
Small defects in a colorectal anastomosis, in select circumstances, may be repaired and a proximal ileostomy created. This should be avoided when there is a large fecal load between the ileostomy and the repaired anastomosis.
-
Creation of a stoma in the setting of peritonitis can be challenging due to a thickened rigid mesentery. If difficulty exists in creating the conventional stoma, two options exist:
-
1.
A loop end stoma provides extra mesenteric length and better blood supply than a traditional end stoma.
-
2.
Bringing the stoma up to the skin through the upper aspect of the midline incision can sometimes be the only alternative. In some severe cases, the bowel can only be wrapped in gauze and matured 5–7 days later to ensure viability and avoid complete mucocutaneous separation and retraction.
-
1.
-
A contained anastomotic leak is walled off and typically located in the pelvis presenting as an abscess.
-
If the abscess is small and contrast flows freely into the bowel, the patient can be treated with intravenous antibiotics, bowel rest, and observation.
-
Larger abscesses or those removed from the site of the anastomosis may require radiologically guided drainage.
-
A contained leak rarely requires immediate operative intervention, but surgery may eventually be required if the patient develops a cutaneous fistula, anastomotic stricture, or chronic presacral cavity.
Fistulae
-
Colocutaneous fistulas frequently close with conservative management (total parenteral nutrition or low residue diet and fistula pouching to protect the skin).
-
Many patients do not require IV nutrition and can eat a solid diet while being monitored for fistula closure.
-
After 3–6 months if the fistula persists, reoperation with reconstruction of the anastomosis can be performed.
-
Successful injection of fibrin glue has been reported as an alternative to reoperation.
-
Colovaginal fistula typically results from either an anastomotic leak that necessitates through the vaginal cuff (in a woman who has had a hysterectomy) or the inadvertent inclusion of the vaginal wall in the staple line. Spontaneous closure is rare in either of these circumstances.
-
Intolerable or copious vaginal drainage may require proximal diversion. Alternatively a daily large-volume enema to evacuate colonic contents may defer a stoma until repair is undertaken.
-
At 3–6 months reoperation can be performed. Options for repair include an advancement flap (colonic or vaginal), a rectal sleeve advancement flap, tissue interposition (labus majorum or gracilis), or laparotomy with a redo coloanal anastomosis.
-
Chronic presacral abscess or sinus may be seen after a leak from a coloanal/rectal or ileal pouch-anal anastomotic leak.
-
The presentation may be subtle with vague pelvic pain, fevers, increased stool frequency, urgency, or bleeding.
-
A pelvic CT usually shows presacral inflammation. A contrast enema demonstrates the posterior midline sinus extending from the anastomosis into the presacral space.
-
During an exam under anesthesia, a probe is placed in the posterior anastomotic defect, and the chronic cavity is laid open with cautery or the laparoscopic linear cutting stapler. Either process divides the luminal-cavity septum and allows free drainage and healing of the cavity by secondary intention.
-
An endoscopically placed vacuum-sponge device has been described as a method to close early and late presacral sinuses.
-
A redo coloanal anastomosis is considered for persistent sinuses after failure of other treatments.
-
For redo coloanal anastomosis, the two-stage Turnbull-Cutait is a useful operation. During the first stage, the failed anastomosis is resected and the sepsis in the presacral space debrided. The descending colon is mobilized and brought out through the anal canal (Fig. 10.1a) and the exteriorized segment wrapped with gauze (Fig. 10.1b). After 5–10 days the patient returns to the operating room and the exteriorized segment is excised (Fig. 10.1c) and a delayed coloanal anastomosis is performed (Fig. 10.1d).
Fig. 10.1 
(a–d) Turnbull-Cutait abdominoperineal pull-through procedure

Stricture
-
Anastomotic strictures can present 2–12 months after surgery with increasing constipation and difficulty evacuating.
-
Causes of anastomotic stricture include leak, ischemia, or, if initially done for malignancy—recurrent cancer.
-
For strictures after a cancer operation, recurrence must be excluded with a CT scan and positron emission tomography (PET) scan. For any mass or abnormality, biopsy is mandatory.
-
Low colorectal, coloanal, or ileal pouch-anal anastomosis may be successfully dilated with a finger or rubber dilators. Dilatation is more successful if initiated within the first few weeks after surgery.
-
Most coloanal and ileoanal anastomosis has some degree of stricture in the early postoperative period (particularly if a diverting stoma is present). Since most are soft, they can easily be dilated with an index finger. All these anastomosis should undergo digital examination 4–6 weeks after surgery or just before stoma closure (which occurs usually around 2–3 months after initial surgery).
-
Narrowed colorectal, colocolic, or ileocolic strictures may be treated with endoscopic balloon dilatation.
-
If these measure fail, or if the stricture is extremely tight or long, revisionary surgery may be required. These operations are difficult and in some cases permanent fecal diversion is the only option.
Genitourinary Complications
Ureteral Injuries
-
A ureter injury usually occurs at one of four specific points during pelvic dissection:
-
The first is high ligation of the inferior mesenteric artery between the upper and middle third of the left ureter. This is usually a transection injury and can be repaired primarily using an end-to-end repair over a stent.
-
The second is at the level of the sacral promontory; when mobilizing the upper mesorectum, the left ureter may be closely associated with the sigmoid colon or adherent to it. The injury may be tangential and not easily recognized, especially in the setting of a phlegmon or abscess. Ureteric stents help recognize an injury at this level but not prevent it. Injury at this level is managed by primary repair or ligation of the distal stump with creation of a ureteroneocystostomy with Boari flap or psoas hitch repair.
-
Mobilization in the deep pelvis may injure the ureter at the ureterovesical junction during the anterior-lateral dissection in the plane between the lower rectum, pelvic sidewall, and bladder base. The ureter may also be injured during lateral stalk division.
-
The final area of injury occurs during the most cephalad portion of the perineal phase of the operation. The ureter may be (unknowingly) divided near the ureterovesical junction. Limited exposure (obese patient, android pelvis) increases the chance of injury.
-
-
Repair of the last two areas of injury requires reimplantation creating a ureteroneocystostomy. The ureter is tunneled through the bladder wall creating a mucosa-to-mucosa anastomosis.
-
Figure 10.2 outlines the anatomic relations of the pelvic nerves.
Fig. 10.2 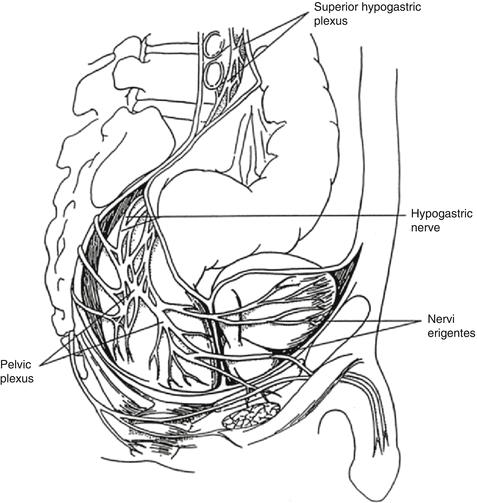
Anatomic relations of the pelvic nerves. Damage to the superior hypogastric plexus during high ligation of the inferior mesenteric artery (IMA) or to the hypogastric nerves at the sacral promontory during mobilization of the upper mesorectum results in retrograde ejaculation. Damage to the pelvic plexus during the lateral dissection or to the nervi erigentes or cavernous nerves while dissecting the anterior plane may result in erectile dysfunction
-
Immediate intraoperative recognition of a ureteral injury and repair is the key to minimizing the consequences. Less than 50 % of ureteral injuries are identified intraoperatively usually because an injury is not suspected.
-
If a difficult pelvic dissection is anticipated such as in patients with prior pelvic surgery, inflammation, locally advanced tumor, recurrent Crohn’s disease, chronic diverticulitis, leaked pelvic anastomosis, and pelvic irradiation, preoperative placement of ureteric stents should be considered. These may aid in localization of the ureters and facilitate identification and repair should an injury occur.
-
If an intraoperative ureteric injury is suspected, indigo carmine can be administered intravenously. After several minutes the urine turns blue-green and the operative field can be inspected for staining.
-
Ureteral stents should be used selectively due to potential complications (obstruction secondary to hematoma, perforation, or acute renal failure).

Urethral Injuries
-
Iatrogenic urethral injuries occur during abdominoperineal resection or total proctocolectomy. A large diameter Foley may be useful to avoid injury in patients deemed at high risk for a urethral injury.
-
The injury usually involves the membranous or prostatic portion of the urethra, and the bladder catheter may be visualized through the defect.
-
An anterior rectal tumor with penetration close or into the prostate may obscure anatomic planes making this injury difficult to avoid. Also edema after neoadjuvant radiation therapy can also increase the risk of injury.
-
Small injuries can be repaired with 5-0 chromic sutures while leaving the Foley in place to stent the repair for 2–4 weeks.
-
Larger injuries or those discovered in the postoperative period require proximal urinary diversion with a suprapubic catheter and a delayed repair. Repair of this type of injury requires a urologist experienced in urethral reconstruction and typically utilizes a gracilis muscle flap.
Bladder Injury
-
Bladder injuries are frequent and can occur during resection of an adherent rectosigmoid cancer or diverticular phlegmon.
-
Injuries to the dome of the bladder:
-
When recognized immediately, a two-layer repair while leaving the Foley in place for 7–10 days is sufficient to address the bladder injury.
-
A cystogram prior to Foley removal to confirm healing may be considered.
-
-
Injuries to the base of the bladder:
-
Repair of injuries located at the base of the bladder carries a risk of occlusion of the ureteral orifice at the area of the trigone.
-
Opening the dome of the bladder to directly visualize the interior while performing the repair helps prevent occlusion.
-
Ureteral patency at the conclusion of the repair should be confirmed.
-
-
Unrecognized bladder injuries:
-
Unrecognized bladder injuries will present in the postoperative period with urine in the abdominal cavity, pneumaturia, or fecaluria.
-
Urinary and fecal diversion may be needed to temporize the situation until repair can safely be done.
-
During takedown of the colovesical fistula with primary bladder repair, if possible, interposition of omentum between the bowel and bladder repair is performed.
-
Foley catheter drainage is continued for 1–2 weeks after surgery with confirmation of healing by a cystogram prior to Foley removal.
-
Urinary Dysfunction
-
Temporary bladder dysfunction with some degree of voiding difficulty is nearly universal after an APR. This can persist 5–7 days and requires continuation of bladder catheterization.
-
The inferior hypogastric nerves which control bladder contractility (via parasympathetic input) may be injured if the endopelvic fascia is breached.
-
A small number of patients have permanent dysfunction and may need a urological consultation. Prostatectomy or intermittent self-catheterization may be required.
Sexual Dysfunction (Male)
-
Fifteen to fifty percent of male patients have some degree of sexual dysfunction after an APR for rectal cancer. Factors attributable to this wide range include age, preoperative libido, adjuvant radiation therapy, definition of dysfunction, time of follow-up, and social barriers preventing a frank discussion of the topic.
-
Ejaculatory problems such as retrograde ejaculation are the most common type of sexual dysfunction and the most likely to resolve within 6–12 months.
-
Dysfunction results from damage to the superior hypogastric (sympathetic plexus) during high ligation of the IMA or to the hypogastric nerves at the sacral promontory during upper rectal mobilization.
-
Erectile dysfunction results from injury to the nervi erigentes or cavernous nerves (branches of the pelvic plexus that course anterior to Denonvillier’s fascia at the lateral border of the seminal vesicles). Parasympathetic innervation controls inflow and retention of blood within the corpora cavernosa.
-
Injury occurs during lateral dissection or while dissecting in the anterior plane by Denonvillier’s fascia.
-
Tailoring the anterior dissection may decrease the risk of injury. For posterior tumors rectal mobilization on the rectal side of Denonvillier’s fascia may protect the small cavernous nerves.
-
Factors that also increase the risk of nerve injury are older age, poor preoperative libido, and a low rectal tumor requiring APR (this has a two to three times increased risk versus a low anterior resection).
-
Sildenafil is an effective treatment for male patients with erectile dysfunction after proctectomy.
Sexual Dysfunction (Female)
-
The incidence of sexual dysfunction after proctectomy in women is hard to quantify and reported to be 10–20 %.
-
Symptoms include dyspareunia and inability to produce vaginal lubricant and achieve organism.
Female Infertility
-
After restorative proctectomy, the postoperative infertility rate can exceed 50 % in women.
-
This rate has implications regarding preoperative counseling and possible modification of surgical technique to minimize the effect of pelvic adhesions.
-
The infertility is felt to be secondary to pelvic adhesions that interfere with transit of the egg from the ovary to the fallopian tubes.
-
Measures to minimize pelvic adhesions such as tacking the ovaries to the anterior abdominal wall and wrapping the adnexa in anti-adhesion barrier are frequently used but not scientifically tested.
Trapped Ovary Syndrome
-
After restorative proctocolectomy, the ovary and tube may become “trapped” in pelvic adhesions. With each menstrual cycle, fluid accumulates in the cavity and expands.
-
Symptoms include pelvic or lower abdominal pain particularly on the side of the trapped ovary.
-
CT scan or ultrasound reveals a cystic lesion with no air and no surrounding inflammation.
-
Operative treatment consists of unroofing the cyst and fluid evacuation, pelvic adhesiolysis, and suspension of the ovary to the pelvic brim or iliac fossa with sutures. This condition may be prevented by ovary suspension at the time of initial surgery.
-
Figure 10.3 shows a CT that demonstrates a “trapped” ovary in the right pelvis
Fig. 10.3 
CT scan demonstrating “trapped” ovary in the right pelvis

Small Bowel Obstruction
-
In managing patients with a small bowel obstruction, the critical component is operative intervention before bowel ischemia and necrosis develops.
-
Finding nonviable bowel at laparotomy increases the risk of death fourfold.
-
It is very important to distinguish between early (<30 days) and late postoperative small bowel obstruction.
Presentation and Diagnosis
-
The most common signs of a small bowel obstruction are nausea, vomiting, colicky pain, abdominal bloating, and obstipation.
-
The hallmarks of strangulated bowel are fever, tachycardia, leukocytosis, sepsis, peritoneal signs, and continuous (versus intermittent) pain. If any of these signs are detected, there should be a high suspicion for ischemia.
-
Nearly one-third of patients with strangulated bowel are not diagnosed until laparotomy; therefore the traditional parameters are neither sensitive nor specific.
Radiographic Studies
Plain Radiographs
-
Have 60 % sensitivity in detecting a small bowel obstruction.
-
On supine and upright plain abdominal x-rays, dilated, air-filled loops of small bowel, air-fluid levels, and an absence or paucity of colonic air are typical findings of a small bowel obstruction.
-
These findings may be absent in a proximal obstruction or if the dilated bowel is mostly fluid filled.
-
Pneumatosis intestinalis or portal vein gas is worrisome for advanced bowel ischemia.
CT Scans
-
Have 90–100 % sensitivity in diagnosing small bowel obstruction.
-
Abdominopelvic CT is becoming the primary imaging modality for patients suspected of having a small bowel obstruction.
-
This study can establish the diagnosis, precisely define a transition point, show a closed loop obstruction, and reveal secondary causes of obstruction (tumor, hernia, intussusception, volvulus, or inflammatory conditions such as Crohn’s disease or radiation enteritis).
-
This study can also show signs of progressing ischemia such as bowel wall thickening, pneumatosis, or portal vein gas.
Contrast Studies
-
This study should be done with water-soluble agents.
-
With a distal obstruction, a contrast enema can evaluate the colon.
-
An antegrade study can differentiate a partial versus complete bowel obstruction. Failure of contrast material to reach the colon within 24 h is used by some surgeons as an indication for surgical exploration.
-
An antegrade study may speed resolution of a partial small bowel obstruction presumably via an osmotic effect (but no definitive studies fully prove this).
Initial Therapy and Nonoperative Management
-
For patients with signs of perforation or ischemia, rapid correction of fluid and electrolyte deficits is done prior to laparotomy. This also includes insertion of a urinary catheter, broad-spectrum antibiotics, and a nasogastric tube. It is important to decompress the stomach prior to general anesthesia to reduce the risk of aspiration.
-
Expectant management in patients without signs of perforation or ischemia results in resolution of an adhesive small bowel obstruction in 80 %. The success rate is significantly lower in patients with a complete obstruction.
-
Expectant management includes IV fluids and electrolyte replacement, bowel rest, and NG tube decompression.
-
Nasoenteric (long) tubes have a balloon at the end (Gowen tube) and require endoscopic placement. Due to the special expertise needed to place these tubes, they are not typically used today.
-
A nonoperative course includes serial exams for the first 24–48 h. Detection of increasing pain, peritoneal signs, or changes that suggest bowel ischemia mandate exploratory laparotomy. Obstructions that do not resolve beyond 48 h are unlikely to do so.
-
Narcotic analgesia to comfort the patient without altering mental status is acceptable.
Decision to Operate
-
Any patient with concern for bowel ischemia or strangulation should be operated upon.
-
The distinction between partial and complete obstruction can be difficult. Patients with a complete obstruction have a low incidence of resolution with conservative management. There is a lower threshold to operate on patients with a complete bowel obstruction to avoid progression to strangulated bowel.
-
Passage of flatus is not an accurate predictor of a partial bowel obstruction because a patient with a complete obstruction may continue to pass gas that is distal to the obstructed point.
-
Bowel function beyond 12 h after the onset of obstructive symptoms decreases the likelihood of a complete obstruction.
-
The onset of flatus after the initial period of obstructive symptoms usually signals resolution of the obstruction.
Surgical Technique for Small Bowel Obstruction
-
Broad-spectrum antibiotics active against enteric pathogens are administered before the peritoneal cavity is entered via a midline incision.
-
Bowel loops will be distended and often adherent to the undersurface of the abdominal wall, so great care is taken to avoid an inadvertent enterotomy entering the peritoneal cavity.
-
When the fascia is encountered, gentle pressure with the bevel of the scalpel versus a cutting stroke may assist in identifying a bowel loop before an enterotomy occurs.
-
Optimally, a single constricting band will be encountered that can be sharply divided and relieve the obstruction.
-
If the peritoneal cavity is totally obliterated, the undersurface of the incisional scar is first cleared to allow opening of the entire incision.
-
Next dissection is carried laterally to the paracolic gutters to allow placement of a self-retaining retractor.
-
Needle decompression of dilated bowel loops may produce additional working space.
-
With severe adhesions (“frozen abdomen”), injection of saline between bowel loops may facilitate adhesiolysis.
-
Mobilization of the entire mass of small bowel loops which are stuck in the pelvis (versus individual loops) is helpful. Freeing the mass and then rolling it up and out of the pelvis is the optimal technique.
-
Lysing adhesions from the small bowel mesentery to the retroperitoneum until the duodenum is encountered can be performed next.
-
Lastly, individual loops are separated and all bowel is examined carefully for coexisting pathology, enterotomies, or serosal tears.
-
Assessment of bowel viability involves examining the color, peristalsis, and mesenteric pulsations. If in doubt, the bowel should be wrapped in warm packs and reexamined after 15 min.
-
If bowel viability is still in question, systemic injection of fluorescein dye followed by inspection of the bowel under a Wood’s lamp or use of a Doppler probe may aid in decision making.
-
If there is still a question of viability and the involved area is a short segment, resection may be the best option. If there is an extensive length of questionable bowel, before committing to a massive small bowel resection, a second-look operation in 24 h should be planned.
-
Once the point of obstruction is addressed, it is debatable whether complete adhesiolysis is required. If the majority of adhesions can safely be divided, this can aid in inspection of the entire length of small bowel in order to look for serosal tears or an enterotomy. If an anti-adhesion barrier is to be used, complete adhesiolysis also may facilitate placement.
Special Situations
Early Postoperative Bowel Obstruction
-
Bowel obstruction less than 30 days after a pelvic or abdominal procedure should generally not be managed with an operation unless there is concern for ischemic or necrotic bowel. The development of strangulation during this time frame is extremely rare.
-
An intense inflammatory response begins 7–10 days postoperatively and leads to hypervascular adhesions that may obliterate the abdominal cavity.
-
If patients undergo early reoperation between day 10 and 6–12 weeks postoperatively, the hypervascular adhesions may lead to extensive enterotomies with the risk of subsequent fistulization being extremely high. Additionally, a higher risk of vascular injuries or serosal tears may lead to massive bowel resections.
-
Initial management of an early bowel obstruction is NG decompression and IV fluids for the first 5–7 days.
-
If a bowel obstruction persists at postoperative day 10, a percutaneous gastrostomy tube may be placed for long-term decompression and the patient started on hyperalimentation.
-
The patient is discharged on this conservative regimen. If the obstruction does not resolve, laparotomy is planned at least 6–12 weeks later (if not longer).
-
During this period before relaparotomy, if signs of sepsis develop, a CT scan should be performed immediately. Any abscess or fluid collection caused by an enteric leak can be percutaneously drained and a controlled enterocutaneous fistula established.
-
Exploration before postoperative day 10 can usually be done safely if a true obstruction is promptly recognized.
-
There is a role for laparoscopic enterolysis in selected settings by appropriately trained skilled surgeons.
Anastomotic “Overhealing”
-
Rarely, “overhealing” of an early adhesion between the linear cut staple lines for a side-to-side anastomosis can lead to obstruction.
-
This can be prevented when placing the final stapler (that closes the anastomosis) by maximally distracting the two completed staple lines.
-
This problem is diagnosed by a water contrast study and conservatively treated.
-
Decompression with a long tube may be ideal as the balloon-tipped catheter may break the healing web.
-
For an ileocolic anastomosis, colonoscopic balloon dilatation may be used.
-
Operative intervention is the last resort and requires resection and reanastomosis.
Prevention of Adhesions
-
Ninety percent of patients develop adhesions when the visceral or parietal peritoneum has been disturbed.
-
There is a progression from early to mature adhesions that takes approximately 6 weeks.
-
Strategies to minimize or prevent adhesions include gentle handling of tissues, use of powder-free gloves, and copious lavage of the peritoneal cavity at the conclusion of the operative procedure.
-
If severe adhesion formation is expected, placement of a long intestinal tube (usually a Baker tube via a jejunostomy) to “splint” the bowel open during adhesion formation had been advocated.
-
The use of a bioresorbable membrane (modified sodium hyaluronate and carboxymethylcellulose) has been reported to reduce extent, incidence, and severity of adhesions. Whether this leads to a clinically significant reduction in reoperation for bowel obstruction is unclear.
-
The use of anti-adhesion material may be justified for patients who are anticipated to be at high risk for future reoperation. The drawback of using this barrier material is that it only prevents adhesions between surfaces where it is applied.
Pelvic Bleeding
-
Serious bleeding during pelvic surgery usually results from injury to the presacral venous plexus or the internal iliac vessels (or their branches). This can be a devastating event and could lead to death of the patient.
-
If the bleeding is moderate, completion of the proctectomy may allow the bleeding to stop or slow. After the rectum has been removed, the area usually is better visualized and a bleeding point can be addressed.
-
The fragility of the presacral venous plexus makes control of bleeding from this area difficult. Attempts at suture ligation or electrocoagulation usually result in increased bleeding.
-
The first measure should be direct finger pressure or pressure with a cotton pledget to allow anesthesia to “catch up” with resuscitation.
-
One method of permanent hemostasis is to use sterile thumbtacks or specially designed “occluder pins.” These are driven into the sacrum at right angles to occlude the site of bleeding.
-
Another method is to suture a rotated flap of rectus abdominis muscle (based on the inferior epigastric pedicle) on either side of the bleeding site to tamponade the opening.
-
Alternatively a 2 × 2 cm2 of rectus muscle can be sutured over the bleeding site and electrocoagulated to form a secure coagulum on the surface of the bleeding plexus.
-
If all these measures fail or the patient is unstable, the pelvis can be tightly packed with several laparotomy sponges. The ends of the sponges are brought out through the lower portion of the abdominal incision. The remaining incision is closed and the patient resuscitated in the intensive care. After 24–48 h the patient is returned to the operating room for pelvic pack removal.
-
Wound Infection and Intra-abdominal Abscess
Wound Infection
-
Currently, the wound infection rate is 5–10 %.
-
Risk factors for wound infection include malnutrition, diabetes mellitus, immunosuppression, age >60 years, American Society of Anesthesiologists score >2, fecal contamination, length of hospitalization before surgery, and extent of surgery.
-
Mechanical bowel preparation does not decrease the incidence of wound infection.
-
Wound infections usually present around the fifth postoperative day.
-
Wound infections are characterized by erythema, warmth, tenderness, fever, and purulent drainage.
-
Initial treatment is opening the wound and debridement if necrotic tissue is present. A packing regimen is started after adequate drainage and the wound allowed to heal by secondary intention.
-
Antibiotics are not typically needed unless there is cellulitis.
-
For larger wounds, after several days of wet to dry dressings, a vacuum-assisted wound closure device may be applied. This device will only need to be changed every 3–5 days and wounds typically close within several weeks.
-
Deep infections of the rectus muscle and fascia may result in dehiscence that requires operative debridement and repair.
-
Infections from Clostridium perfringens or beta-hemolytic Streptococcus can lead to invasive wound infections.
-
A high level of suspicion is important for a timely diagnosis. These infections occur within 1–2 days of surgery and may be associated with minimal skin changes.
-
Fever and unusually severe wound pain in the early postoperative period should prompt opening the wound. The drainage is typically thin gray fluid.
-
Thorough wound exploration in the operating room along with debridement of all devitalized tissue back to healthy bleeding edges is required.
-
Broad-spectrum antibiotics which include high-dose penicillin are also needed.
-
Intra-abdominal Abscess
-
Intra-abdominal abscesses can result from anastomotic leaks, enterotomies, or spillage of bowel contents at the time of surgery.
-
Patients present with fever, leukocytosis, and abdominal or pelvic pain 5–7 days after surgery.
-
The diagnostic modality of choice is CT scan of the abdomen and pelvis with IV and oral contrast. Rectal contrast is included in patients with a colorectal anastomosis.
-
The characteristic findings on CT scan are a fluid collection with a thickened, enhancing rim, surrounding inflammatory stranding, and possible air bubbles.
-
A collection proximal to a staple line and the presence of contrast material in the abscess are both suggestive of an anastomotic leak.
-
Radiological percutaneous drainage can be accomplished to adequately drain the abscess 65–90 % of the time. Success depends on size, complexity, etiology, and microbial flora.
-
IV antibiotics are usually administered.
-
Once the cavity has collapsed and no fistula to the bowel is identified, the catheter can be removed.
-
Some abscesses cannot be drained percutaneously due to the lack of a safe “radiographic window” for drainage.
Perineal Wound Infection
-
Eleven to fifty percent of perineal wounds can have delayed healing due to a perineal wound infection.
-
The rigidity of the boney pelvis combined with a wide resection of perineal soft tissue and levator muscles will result in dead space cephalad to the skin closure that can easily become infected.
-
Technical factors to reduce perineal wound infections include reapproximation of subcutaneous tissues, suction drainage of the pelvis (to prevent hematoma and resultant fibrosis), and filling the dead space with an omental pedicle graft.
-
For benign disease, a cuff of levator muscle can be left just outside the external sphincter muscle. This will allow closure of the levators and reduction in dead space.
-
Neoadjuvant radiation therapy increases the incidence of perineal wound infections that can lead to a nonhealed perineal wound at 30 days.
-
Intraoperative radiation further increases the rate of perineal wound complications.
-
Factors associated with perineal wound problems include long operative time (>300 min), intraoperative hypothermia, and fecal contamination during perineal dissection.
-
In patients with inflammatory bowel disease, an intersphincteric dissection may lead to improved perineal wound healing due to preservation of the external anal sphincter. Figure 10.4a–c illustrates the technique of an intersphincteric dissection.
Fig. 10.4 
(a) Technique of intersphincteric proctectomy. (b) The mucosa overlying the intersphincteric groove is incised near the dentate line, and the dissection is carried cephalad between the internal and external sphincters. (c) This results in retention of the external sphincters and levators, which are then closed in the midline
-
For a perineal wound infection, the skin is opened and wet to dry packing begun. When the wound is clean, a vacuum-assisted closure device can be applied.
-
For a chronic perineal sinus, closure may require wound debridement and myocutaneous flap reconstruction with the gracilis, inferior gluteus, or rectus abdominis muscle.
-
After proctectomy, the small bowel may adhere to the raw surfaces in the pelvis which could lead to a small bowel obstruction.
-
Methods to exclude small bowel from the pelvis include closure of the pelvic peritoneum, posteriorly retroverting the uterus, rotating the cecum into the pelvis, or the excluding the pelvis using absorbable mesh. Absorbable mesh has been associated with obstruction and fistulization.
-

Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Dietz, D.W. (2014). Postoperative Complications. In: Beck, D., et al. The ASCRS Manual of Colon and Rectal Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8450-9_10
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8450-9_10
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8449-3
Online ISBN: 978-1-4614-8450-9
eBook Packages: MedicineMedicine (R0)