
Abstract
Executive function (EF) is a complex construct that encompasses a variety of cognitive abilities that allow for impulse control, strategic planning, cognitive flexibility, and goal-directed behavior. Executive functions have been studied in nearly every major childhood disorder including externalizing and internalizing disorders. A universally accepted definition of EF does not exist, and many have criticized the broad definitions of the construct. For example, Pennington and Ozonoff (1996) noted, “in both neuropsychology and cognitive psychology, the definition of EFs is provisional and under-specified” (p. 55). Fletcher (1996) also acknowledged that EFs are difficult to define and described EFs as “factorially complex.” More recently, Jurado and Rosselli (2007) acknowledged that the fundamental question of “whether there is one single underlying ability that can explain all the components of executive functioning or whether these components constitute related but distinct processes” remains unanswered. To complicate matters, a large variety of tasks that purportedly measure executive functions have been used in the literature. What remains unclear is specifically which executive function tasks are used most often in the literature and on which executive tasks are groups most likely to differ? Hence, the purpose of this review is to conduct a systematic search of the childhood internalizing and externalizing literature to determine (a) executive function tasks that are used in the literature, (b) executive function tasks that are most commonly used, (c) executive function tasks on which clinical and control groups differ most frequently, and (d) executive function tasks on which clinical groups differ most frequently. To begin, a review will be provided regarding executive function performance of children with commonly diagnosed externalizing and internalizing disorders. Next, specific findings regarding the type, usage, and discriminant ability of executive function tasks will be presented followed by implications and suggestions for future research.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Bipolar Disorder
- Executive Function
- Conduct Disorder
- Oppositional Defiant Disorder
- Executive Functioning
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Executive function (EF) is a complex construct that encompasses a variety of cognitive abilities that allow for impulse control, strategic planning, cognitive flexibility, and goal-directed behavior. Executive functions have been studied in nearly every major childhood disorder including externalizing and internalizing disorders. A universally accepted definition of EF does not exist, and many have criticized the broad definitions of the construct. For example, Pennington and Ozonoff (1996) noted, “in both neuropsychology and cognitive psychology, the definition of EFs is provisional and under-specified” (p. 55). Fletcher (1996) also acknowledged that EFs are difficult to define and described EFs as “factorially complex.” More recently, Jurado and Rosselli (2007) acknowledged that the fundamental question of “whether there is one single underlying ability that can explain all the components of executive functioning or whether these components constitute related but distinct processes” remains unanswered. To complicate matters, a large variety of tasks that purportedly measure executive functions have been used in the literature. What remains unclear is specifically which executive function tasks are used most often in the literature and on which executive tasks are groups most likely to differ? Hence, the purpose of this review is to conduct a systematic search of the childhood internalizing and externalizing literature to determine (a) executive function tasks that are used in the literature, (b) executive function tasks that are most commonly used, (c) executive function tasks on which clinical and control groups differ most frequently, and (d) executive function tasks on which clinical groups differ most frequently. To begin, a review will be provided regarding executive function performance of children with commonly diagnosed externalizing and internalizing disorders. Next, specific findings regarding the type, usage, and discriminant ability of executive function tasks will be presented followed by implications and suggestions for future research.
Attention-Deficit/Hyperactivity Disorder
Attention-deficit/hyperactivity disorder (ADHD) is characterized by developmentally inappropriate levels of impulsivity and hyperactivity, and attention deficits, and affects 3–7 % of the school-age population (American Psychiatric Association, 2013). Executive functions have been studied extensively in children, and in general, studies have found that children with ADHD tend to perform poorly on EF tasks relative to nondisabled peers and these deficits may begin early in life (e.g., Barkley, Edwards, Laneri, Fletcher, & Metevia, 2001; Barkley, Murphy, & Bush, 2001; Fuggetta, 2006; Klimkeit, Mattingley, Sheppard, Lee, & Bradshaw, 2005; Nigg, Blaskey, Huang-Pollock, & Rappley, 2002; Seidman, Biederman, Faraone, Weber, & Ouellete, 1997; Weyandt, Rice, Linterman, Mitzlaff, & Emert, 1998; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005). For example, preliminary studies have found that preschoolers with ADHD demonstrated EF impairments relative to their peers (Byrne, DeWolfe, & Bawden, 1998; DuPaul, McGoey, Eckert, & VanBrakle, 2001; Mahone, Pillion, & Heimenz, 2001) and inhibition problems in preschool may be predictive of EF deficits and ADHD in later childhood (Berlin, Bohlin, & Rydell, 2003; Friedman et al., 2007). With regard to long-term outcome, Biederman et al. (2007) completed a 7-year follow-up study of 85 males with ADHD and reported that the majority (69 %) maintained EF deficits into adulthood. Others (e.g., Fischer, Barkley, Smallish, & Fletcher, 2005; Hinshaw, Carte, Fan, Jassy, & Owens, 2007; Rinsky & Hinshaw, 2011) have conducted similar longitudinal studies of children with ADHD into adolescence and adulthood, and collectively, these findings suggest that EF deficits may emerge early in life in children with ADHD and the impairments are likely to persist into adolescence and possibly adulthood.
Not all studies have found EF deficits in children with ADHD, however, and impairments are commonly found on some but not all EF measures (Barkley, Grodzindky, & DuPaul, 1992; Berlin, Bohlin, Nyberg, & Janols, 2004; Geurts, Verte, Oosterlaan, Roeyers, & Sergeant, 2005; Lawrence et al., 2002; Rhodes, Coghill, & Matthews, 2005; Seidman, Biederman, Weber, Hatch, & Faraone, 1998; Tsal, Shalev, & Mevorach, 2005; Weyandt, 2004; Weyandt & Willis, 1994). These findings raise questions about the specificity and sensitivity of EF tasks and collectively suggest that ADHD is not associated with global deficits in EF as has been frequently reported in the literature, but may, however, be characterized by specific EF deficits (Barkley, 2010; Pennington & Ozonoff, 1996; Sergeant, Geurts, & Oosterlaan, 2002; Weyandt, 2005; Wu, Anderson, & Castiello, 2002). The specific EF components that might be compromised in ADHD are equivocal, although response inhibition has been implicated in multiple studies (Barkley, 1997, 2010; Denckla, 1996; Mahone & Hoffman, 2007; Wu et al., 2002). As noted by Weyandt (2009), the inconsistencies across studies may be due in part to methodological factors including sample size, statistical power, inclusion and diagnostic criteria used for ADHD, subtypes of ADHD, EF tasks employed, psychometric properties of the EF tasks, age, sex, ethnicity, comorbidity, intelligence, and statistical methods used to analyze data.
In summary, the literature suggests that EF deficits are not necessarily unique to ADHD and they are not necessary or sufficient for a diagnosis of ADHD. In addition, when EF impairments are present in children with ADHD, they tend to be specific rather than global impairments.
Conduct Disorder and Oppositional Defiant Disorder
Conduct disorder (CD) is characterized by a “persistent pattern of behavior in which the basic rights of others or major age-appropriate societal norms or rules are violated” (DSM-IV-TR, APA, 2000). CD is diagnosed more frequently in males than females and is estimated to affect 1–10 % of the child population (DSM-IV-TR, APA, 2000). Oppositional defiant disorder (ODD) is defined as a “recurrent pattern of negativistic, defiant, disobedient, and hostile behavior toward authority figures.” Like CD, ODD occurs more frequently in males than females and affects 2–16 % of the child population (DSM-IV-TR, APA, 2000).
Compared to the ADHD literature, fewer studies have explored EFs in children with CD or ODD. Earlier studies by Moffitt and Henry (1989) and McBurnett et al. (1993) found that children with ADHD and comorbid CD displayed EF deficits but not children with CD only. Speltz, DeKlyen, Calderon, Greenberg, and Fisher (1999) examined EF performance in preschoolers with ADHD and ODD or ODD alone and found that those with ADHD and ODD performed more poorly on two EF measures (Motor Planning Task and the Verbal Fluency subtest of the McCarthy Scales of Children’s Abilities) compared to preschoolers with ODD only. Clark, Prior, and Kinsella (2000) found similar results with adolescents with ADHD relative to adolescents with CD or ODD. Giancola, Mezzich, and Tarter (1998), however, found that females with CD displayed EF deficits relative to a control group as measured by overall performance on seven neuropsychological tasks. Unfortunately, given the analyses used in the study (i.e., Principal Components Analysis), group performance on specific EF tasks was not reported.
More recently, Herba, Tranah, Rubia, and Yule (2006) found that adolescents with conduct problems demonstrated EF impairments on a motor response inhibition task (i.e., Stop Task) but not on other EF measures. It is important to note that these children were identified in schools based on rating scales and did not necessarily have diagnosed CD. In addition, similar to the ADHD literature, many of the children had comorbid attention problems, and therefore it is difficult to determine the degree to which attention and impulsivity contributed to the findings rather than conduct related issues. Kim, Kim, and Kwon (2001) also reported that adolescents with CD displayed EF deficits on an inhibition task (i.e., Wisconsin Card Sorting Test, WCST) relative to a control group, but differences were not found on additional EF measures (Visual Performance Test, Contingent Continuous Performance Test, Stroop Test, Spatial Memory Test, and Recognition Test). Toupin, Dery, Pauze, Mercier, and Fortin (2000), however, found that children with CD displayed significant impairments on four of five EF tasks (WCST number of preservative errors, WCST number of preservative responses, Rey-Osterrieth Complex Figure (ROCF) copy accuracy, and Stroop number of word colors) even after ADHD and socioeconomic status were statistically controlled. Morgan and Lilienfeld (2000) conducted a meta-analysis that included 39 studies (4,589 participants) that examined EF and CDs. Studies that included one or more of six commonly used EF tasks were included in the meta-analyses (Porteus Mazes, Category Test, Stroop Test, WCST, Verbal Fluency tests, and Trail Making Test). Overall, Morgan and Lilienfeld found those with conduct problems performed worse than control participants on EF measures. The effect sizes ranged substantially, however, depending on the specific task. Lastly, Sergeant et al. (2002) conducted a selective review of CD, ODD, and ADHD studies and concluded that deficits in EF are not unique to ADHD and that children with CD and ODD often display inhibition deficits on EF measures.
In conclusion, earlier reviews reported that EF deficits were not characteristic of children and adolescents with CD after comorbid ADHD was factored out (e.g., Pennington & Ozonoff, 1996). More recent studies, however, suggest that inhibition deficits may be characteristic of both ADHD and CD but whether children with CD display impairments on additional EF measures is equivocal. Similar to the ADHD literature, methodological problems characterize many of the CD/ODD studies including differences in inclusionary criteria, diagnostic criteria, age, gender, and measurement variables.
Tourette’s Disorder
Tourette’s disorder (TD) is characterized by multiple motor tics and one or more vocal tics and is estimated to affect 5–30 children per 10,000 (American Psychiatric Association, 2000). The onset of TD is before age 18 and the disorder occurs more often in males than females. Compared to ADHD and CD/ODD, very few studies are available concerning EFs in children with TD. Of the studies that have been conducted, no consistent EF finding has emerged. A few studies have found that children with TD display a slower and/or more variable reaction time on continuous performance tests compared to children without TD, but some have questioned the role attention problems may have played in these findings (e.g., Harris et al., 1995; Schuerholz, Singer, & Denckla, 1998; Shucard, Benedict, Tekok-Kilic, & Lichter, 1997). In an effort to address the comorbidity issue, Harris et al. (1995) compared the performance of children with TD only, children with ADHD only, and children with both ADHD and TD on ten EF tasks (including Test of Variables of Attention (TOVA), WCST, ROCF, Multilingual Aphasia Examination-Controlled Word Fluency subtest). Results revealed that children with ADHD and children with ADHD plus TD performed more poorly on EF tasks compared to children with TD only (although children with TD also displayed EF impairments). After controlling for IQ, scores on the ROCF were significantly worse in TD plus ADHD than TD only. A control group was not included in this study, however, precluding comparison with nondisabled children.
Channon, Pratt, and Robertson (2003) also compared EF performance in three groups—those with TD only, TD and ADHD, and TD and obsessive-compulsive disorder (OCD). Results revealed that those with TD and ADHD performed poorly on several EF measures (e.g., Six Elements Test, Hayling category A and B), whereas those with TD performed poorly on only one EF measure (e.g., Hayling Test category A) as compared to the control group. Similar results were reported by Schuerholz et al. (1998) who compared the performance of children with TD only, ADHD only, and TD and ADHD and a comparison group and found girls with TD performed lower on Letter Word Fluency than children in the other groups. Furthermore, girls with TD and ADHD had the greatest variability of reaction time on the TOVA and were slowest on the Letter Word Fluency. Mahone et al. (2002) also reported that children with TD plus ADHD and children with ADHD only demonstrated poorer performance on the five measures of the Behavior Rating Inventory of Executive Function (BRIEF). The TD only group did not differ from comparison children (or children with ADHD). Similarly, Chang, McCracken, and Piacentini (2007) administered EF tasks to children who had TD alone, OCD alone, and control participants and did not find significant differences in performance across the three groups. The authors noted that those with TD showed “trends toward impairments” in EF but the findings were not robust. Ozonoff and Strayer (2001) compared the performance of children with TD, children with autism, and comparison children on working memory tasks and also did not find group differences. Other studies have also reported no differences between adolescents with TD and control participants on working memory tasks (e.g., Crawford, Channon, & Robertson, 2005).
In an earlier study, Ozonoff and Jensen (1999) compared EF performance using the WCST, Tower of Hanoi (TOH), and the Stroop Color-Word Test in three groups of children, those with TD only, ADHD only, and autism only, and nondisabled comparison children. Results revealed that children with TD did not show impairments on any of the EF tasks, children with ADHD showed impairment on only one task (Stroop), and children with autism showed deficits on two of the EF tasks (WCST and TOH). Cirino, Chapieski, and Massman (2000) compared the WCST performance of children and adolescents with TD only to children with ADHD and comorbid TD and did not find differences between the two groups.
In summary, no clear pattern of EF deficits emerges in the literature concerning children with TD. A few studies, but not all, have reported greater response-time variability on continuous performance tasks. Preliminary studies suggest that working memory is not characteristically impaired with children with TD. Some studies suggest that children with TD may have EF deficits particularly with response time and memory search (e.g., poor performance on Hayling Test, timed continuous performance task on TOVA, and Letter Word Fluency), but they may not be as severe as EF deficits in other disorders such as ADHD. Results are equivocal with respect to the performance of children with TD on planning tasks and measures of cognitive flexibility. What is clear is that distinct and robust impairments in EF do not appear to be characteristic of children with TD. Additional, methodologically sound studies are needed to address whether subtle differences in EF may exist between children with TD and other types of childhood psychopathology.
Anxiety Disorders
Taxometric approaches in the field of developmental psychopathology typically identify a general anxious-depressed syndrome within a broader grouping of internalizing disorders (Achenbach & Edelbrock, 1983). As such, unlike the DSM-IV-TR (American Psychiatric Association, 2000), anxiety usually is not differentiated from depression as a separate diagnostic category, and distinctions usually are not made among various types of anxiety disorders. In contrast, the DSM-IV-TR specifically identifies one kind of anxiety disorder (i.e., separation anxiety disorder) as one of the “Disorders Usually First Diagnosed in Infancy, Childhood, or Adolescence” (p. 39) and provides child and adolescent diagnostic criteria for several other anxiety disorders including panic disorder, specific phobia, social phobia, OCD, posttraumatic stress disorder (PTSD), acute stress disorder, and generalized anxiety disorder.
Toren et al. (2000) compared a group of children (n = 19; M age = 11.5 years) who had been diagnosed with separation anxiety disorder and overanxious disorder (based on DSM-III criteria) (American Psychiatric Association, 1987) to a group of children who were comparable in terms of age and gender (n = 14; M age = 11.5 years) with no history of psychopathology. Despite the common comorbidity of anxiety and depression among children, a strength of this study was that not one of the children in the clinical group met criteria for major depression. Neuropsychological and EF measures included the California Verbal Learning Test (Delis, Cullum, Butters, Cairns, & Prifitera, 1988), the ROCF Test (Osterrieth, 1944), and the WCST (Heaton, 1981; Spreen & Strauss, 1991). Thus, neurocognitive functions assessed included verbal processing, visuospatial processing, and EF.
When the ten measures on the California Verbal Learning Test were analyzed as a single composite (using multivariate analysis of variance techniques), children with anxiety disorders showed verbal-processing deficits relative to children with no history of psychopathology (Toren et al., 2000). Follow-up univariate analyses, however, failed to identify any one of those ten measures as a reliable discriminator when considered separately. The three measures on the ROCF Test failed to discriminate between children with anxiety disorders and those with no history of psychopathology, either as a composite or when considered as separate dependent variables. Similarly, no group differences were found on a composite of the five measures on the WCST. Univariate results, however, showed differences on two WCST measures: total errors and perseverative responses (see Table 5.1). Overall, then, these findings suggest possible generalized deficits in verbal or linguistic abilities and in a set-shifting or cognitive-flexibility component of EF, with sparing of visuospatial organization skills among children with anxiety disorders.
Emerson, Mollet, and Harrison (2005) also found that boys who were anxious and depressed showed EF deficits relative to boys with no psychiatric history on two tests designed to measure set shifting and concept formation. These investigators argued that although anxiety and depression each may contribute separately to neurocognitive processing, the fact that these two categories commonly co-occur highlights the importance of examining the comorbid condition. Expressed here, of course, is the traditional trade-off between internal and external validity issues: on the one hand, a concern for the clinical integrity of nosological categories vs., on the other hand, the value of representativeness and generalizability to existing populations.
A sample of boys (n = 19; age = 9–11 years) who scored high (albeit not necessarily at clinical levels) on measures of both depression (i.e., Child Depression Inventory; Kovacs & Beck, 1977) and anxiety (the Trait subscale of the State-Trait Anxiety Inventory for Children; Spielberger, Edwards, Lushene, Montuori, & Platzek, 1973) was compared to a similar group of boys who scored low on both of these measures on Parts A and B of the Trail Making Test and on the Concept Formation subtest of the Woodcock Johnson Test of Cognitive Abilities (Woodcock & Johnson, 1989). Both groups showed similar completion times on Part A and Part B of the Trail Making Test. In contrast, however, they differed in terms of the number of perseverative errors that they made (on both Part A and Part B). Participants in the anxious-depressed group showed lower levels of accuracy, implicating possible impairments in the ability to shift mental set. The two groups also differed in terms of accuracy on the Concept Formation subtest, with those in the anxious-depressed group showing greater degrees of difficulty on a task that requires one to solve problems based on abstract rules of categorization. Although acknowledging the lack of any data at a physiological or anatomical level of analysis, Emerson et al. (2005) speculated that these findings were consistent with evidence implicating frontal lobe EF deficits in children with symptoms of both anxiety and depression.
In a well-designed study of children with PTSD, Beers and De Bellis (2002) also found evidence of EF deficits among children with this anxiety-based disorder. Children (n = 14, M age = 11.4 years) who had been identified as maltreated (e.g., sexual abuse, physical abuse, witnessing domestic abuse) by a child-protective-service agency and who subsequently had been diagnosed with PTSD were compared to a similar group of children who were healthy and who had not been maltreated. An extensive battery of neuropsychological tests (described by Spreen & Strauss, 1998) was administered that included two measures of language, six measures of attention, six measures of abstract reasoning/EF, six measures of learning and memory, five measures of visuospatial functioning, and four measures of psychomotor speed. After corrections for multiple significance tests, children with PTSD showed deficits relative to children without PTSD on two of the six measures of attention (i.e., Stroop Color-Word Test: Color/Word, which is a measure of interference control; cf. Doyle et al., 2005; Digit Vigilance Tests: omission errors, which is a measure of sustained attention) and on two of the six measures of abstract reasoning/EF (i.e., WCST, categories completed, which is an EF measure of problem solving and set shifting; cf. Doyle et al., 2005; Controlled Oral Word Association Test, animal naming, which is an EF measure of verbal fluency). There were no differences found on any of the language, learning and memory, visuospatial functioning, or psychomotor-speed tests, suggesting some degree of specificity in terms of the neurocognitive domains that were assessed.
In concluding that these results supported EF differences between children with and without maltreatment-related PTSD, Beers and De Bellis (2002) acknowledged that the sample size studied was relatively small and that these children also experienced comorbid conditions such as major depressive disorder, dysthymic disorder, separation anxiety disorder, and ADHD (inattentive subtype). Moreover, the extent to which results were related to maltreatment or to the presence of psychopathology could not be assessed.
Using neuroimaging technology, Carrion, Garrett, Menon, Weems, and Reiss (2008) found differences between youth with and without posttraumatic stress symptoms when they performed a Go/No-Go task during a functional magnetic resonance imaging (fMRI) scan. The accuracy and response times for the Go/No-Go task were similar between the two groups; however, the control group displayed greater middle frontal cortex activation, whereas the group with posttraumatic stress symptoms demonstrated greater medial frontal activation.
Finally, an anxiety disorder that has received a great deal of research attention, particularly in terms of its neurological basis, is OCD. This disorder is characterized by recurring obsessions or compulsions that are time-consuming or cause significant distress or impairment (American Psychiatric Association, 2000). The perseverative and ego-dystonic nature of cognitive impulses (i.e., obsessions) and the repetitive behaviors that accompany them as an attempt to reduce anxiety (compulsions) have led many to consider the disorder from an executive-dysfunction perspective (see Friedlander & Desrocher, 2006). Once believed to be rare among children, OCD now has been shown to present lifetime prevalence rates that range from about.5 to 2.1 %, with comparable estimates for both children and adults (Evans & Leckman, 2006). The age of onset for childhood OCD ranges from about 6 to 11 years (M age = 10.3 years); Shin et al. (2008) studied children from Korea diagnosed with OCD, ADHD, tic disorder, and depressive disorder, and controls were compared using the Wechsler Intelligence Scale-Revised (WISC-R) and the WCST. The children with OCD performed the worst on the perceptual organization tasks and had significantly more errors and used fewer strategies on the WCST compared to the control group. This study also demonstrated that deficits in EF that are apparent in adults with OCD are similar in children with OCD. Both children and adults with OCD have demonstrated EF deficits in mental set shifting, which provides further evidence for the hypothesis of frontal-striatal dysfunction in individuals with OCD.
Unfortunately, little research has addressed the neuropsychological characteristics of children with OCD. For example, it would be interesting to compare the EF abilities of children with early-onset OCD to children without OCD as well as to adults with early-onset OCD, adults with late-onset OCD, and adults without OCD. Indeed, these kinds of studies could help to clarify if differences between earlier- and later-onset OCD are associated with neurodevelopmental issues, qualitative differences between potential subtypes of the disorder, or perhaps an interaction between these factors.
In summary, the neurophysiological basis of anxiety disorders has been widely studied (e.g., Gray, 1987; Zahn-Waxler, Klimes-Dougan, & Slattery, 2000), and the neuropsychological construct of EF among youth with separation anxiety disorder, overanxious disorder, PTSD, and OCD has received recent attention. Specifically, EF deficits in set shifting, cognitive flexibility, concept formation, interference control, and verbal fluency have been documented among children with separation anxiety disorder, overanxious disorder, and PTSD (Beers & De Bellis, 2002; Emerson et al., 2005; Toren et al., 2000). Little research has addressed the EFs of children with OCD, but studies of adults with early- vs. late-onset OCD subtypes implicate EF deficits associated with working memory and the ability to shift mental set for those with later-onset OCD but not for those with earlier-onset OCD. Additional research is needed to help clarify the relationship between the development of EF in childhood and adolescence and OCD subtypes.
Depression
Although several investigators convincingly have argued that depression is probably better conceptualized as a taxometric continuum vs. a discrete category of psychopathology (Hankin, Fraley, Lahey, & Waldman, 2005; Prisciandaro & Roberts, 2005), the three depressive, unipolar disorders described in the currently used DSM-IV-TR (APA, 2000) nosology are (a) major depressive disorder, (b) dysthymia, and (c) adjustment disorder with depressed mood. The overall 30-day prevalence rate of a major depressive episode is about 5 %, with the highest prevalence rates among female teens and young-adult males (Kessler et al., 2008). The prevalence of unipolar depression among children younger than 15 years is relatively rare and ranges from.4 to 2 % (Costello et al., 2002; Hankin et al., 1998).
Channon (1996), using nonclinical samples, found that older adolescents (i.e., first- and second-year university undergraduate students) who scored relatively higher (suggesting a naturally occurring dysphoric mood) on the Beck Depression Inventory (BDI; Beck, 1978) required more trials to attain criterion-level performances and made more perseverative as well as non-perseverative errors on the standard version of the WCST than a similar group of individuals who scored relatively lower on the BDI. Thus, in this study, older adolescents in the dysphoric group showed more difficulty than those in the control group in EF shifting set correctly and in altering their behavior in response to feedback.
In summary, little research has been conducted on the EF abilities among youth who are depressed. Studies that have included late adolescents (e.g., Channon, 1996) have suggested some degree of sensitivity of EF tasks in identifying unipolar depression, but less specificity. Given the neuropsychological discontinuities that are characteristic of human development and the heterotypic nature of child, adolescent, and adult depression, however, generalizing EF findings to younger individuals with depression requires great caution.
Bipolar Disorder
There has been a history of controversy about the identification of mania, a major criterion for bipolar disorder (BD), among children and adolescents, but recent evidence suggests that much of this debate may be associated with diagnostic challenges rather than to extremely low incidence rates as once was thought (Biederman, 2003). For example, Costello et al. (2002) reported no epidemiological evidence of BD among children younger than 13 years old and only about a 1 % lifetime prevalence rate among adolescents aged 14–18 years. The reliability of these estimates, however, has been questioned because of (a) inadequate sample sizes, (b) different definitions and criteria applied to the diagnosis of BD, and (c) the putative heterotypic continuity of symptoms of this disorder across the lifespan (Costello et al., 2002). BD among children may present as irritability and aggression rather than as euphoric mood and is likely to present as continuous, chronic, and rapidly cycling (Geller & Luby, 1997).
Biederman (2003) has documented a growing consensus on the significance of serious consequences of affective dysregulation among children and adolescents and the increased scientific and clinical attention that they have received in recent years. Much of this attention has focused on the neurocognitive concomitants of BD among children, especially those involving EF. When BD has been studied among child and adolescent populations, however, results often have been complicated by its comorbidity with ADHD and other disruptive as well as internalized disorders. When reviewing the epidemiology of BD within this population, Costello et al. (2002) found that the majority of children and adolescents classified with BD (i.e., 60–90 %) showed comorbid ADHD, leading to significant diagnostic confusion.
Doyle et al. (2005) studied the EF (e.g., working memory, interference control) and other (e.g., processing speed, sustained attention, visuospatial organization) EF characteristics of a sample (n = 57) of youth with BD between 10 and 18 years old, comparing them to same-aged youth with no history of bipolar or other mood disorders on a variety of tasks. Not surprisingly, comorbidity rates between the two samples differed markedly for several externalizing disorders (ADHD, CD, and ODD) as well as anxiety disorders. In fact, 74 % of those in the bipolar group met criteria for ADHD, whereas only 17 % in the control group met those criteria. An even larger discrepancy occurred for comorbid ODD between those with and without BD (i.e., 93 % and 20 %, respectively). Results demonstrated that youth with BD showed impairments relative to those without any history of mood disorders on selected measures within several of the EF and non-EF neurocognitive areas that were assessed. Children with BD demonstrated significantly poorer performance on Digit Span, Digit Symbol/Coding, Stroop Color, Stroop Color-Word, and the Auditory Continuous Performance Test (Doyle et al., 2005). Among other EF tasks, no differences were found on any of the three measures of abstract problem solving and set shifting; among the non-EF tasks, no differences were found on any of the two measures of visuospatial organization or one measure of verbal learning. Thus, although measures of planning (e.g., Tower of London, TOL) and verbal fluency were not administered, traditional EF measures, such as those assessed on the WCST for shifting of set, failed to discriminate between the groups. One strength of this study was the fact that the effects of ADHD were statistically controlled; therefore, results cannot be attributed to this comorbidity. On the other hand, one might question the representativeness and generalizability of the findings, given the natural coincidence of ADHD with BD among youth. That is, perhaps these are not really dissociable clusters of symptoms. It also is unclear why ADHD was controlled, whereas other forms of psychopathology (e.g., ODD) were not. This study, therefore, provided limited evidence that particular aspects of EF may be affected in youth with BD, which included one measure of interference control and two measures of working memory.
Dickstein et al. (2004), however, did include some of these more traditional EF constructs, such as an intradimensional/extradimensional set-shifting task (described as a task that “mirrors the WCST”; p. 34) and the Stockings of Cambridge (described as a “modified version of the TOL task,” which is essentially a spatial planning task; p. 34). In this study, a group of children with pediatric BD (M age = 13 years) was compared with a similar group of normal controls on a variety of neurocognitive tasks including a simple pointing task, pattern recognition, and several tasks of spatial memory, in addition to the set-shifting task and the Stockings of Cambridge.
Over 20 t-tests were conducted on measures derived from these tasks in analyzing potential differences between children with and without BD. Given the preliminary nature of this study, no corrections for multiple significance tests were conducted, but only two of these tests were significant at p <.01: (a) the number of errors made prior to an extradimensional shift on the set-shifting task and (b) the mean correct latency of a pattern-recognition memory task. Here, children with BD made more errors and took longer to respond than those without BD. Interestingly, there were no differences between the groups on any of five measures for the Stockings of Cambridge task. Moreover, other than the number of errors made prior to an extradimensional shift, only one other of seven measures on the intradimensional/extradimensional set-shifting task discriminated between the two groups at p <.05. Results suggested that deficits in attentional set shifting and visuospatial memory potentially may be implicated in pediatric BD. Unfortunately, the sample sizes for each group were small (n = 21 in each group), and at the time of testing, all children in the bipolar group were taking at least one psychotropic medication (over half were taking four or more medications) and over half of these children were diagnosed with comorbid ADHD (over 70 % met ADHD criteria during their lifetimes). Thus, Dickstein et al. (2004) cautioned that these findings are best considered as preliminary.
Meyer et al. (2004) found that 6 of 32 offspring of mothers with BD and 3 of 42 offspring of mothers with unipolar depression were diagnosed with BD as young adults (Radke-Yarrow, 1998). Records of the EF measures administered (WCST, Trail Making Test Part B [TMT-B]) to these nine individuals when they were adolescents were compared with similar measures for offspring who were later diagnosed with unipolar depression (n = 22) and those who showed no evidence of a mood disorder as young adults (n = 64). On WCST measures of EF obtained during adolescence, those who were diagnosed with BD during young adulthood (n = 9) showed more preservative errors, fewer categories completed, and fewer conceptual-level responses than those who showed no evidence of mood disorders as adults (Meyers et al., 2004; Radke-Yarrow, 1998). No differences were found among the young-adult groups on their adolescent performances on the Trail Making Test. Results showed that, among those participating in this study, 67 % of the high-risk offspring who were diagnosed with BD as young adults previously had shown EF deficits as adolescents. In contrast, only 19 % of the high-risk offspring who were diagnosed with unipolar depression as young adults previously had shown EF deficits as adolescents, and only 17 % of the high-risk offspring who showed no mood-disorder symptoms as young adults previously had shown EF deficits as adolescents. Thus, this study suggests that there may be a specific profile of neurocognitive deficits that include EF (as well as visuospatial memory and sustained attention) that precede the adult onset of bipolar disorder but are unrelated to unipolar depression (Klimes-Dougan, Ronsaville, Wiggs, & Martinez, 2006; cf. Dickstein et al., 2004).
In summary, there is a growing consensus about the significance of BD among children, and several studies have targeted its EF concomitants. Although results often have been confounded with significant comorbidity issues, children and adolescents with BD reliably have demonstrated impairments relative to those without any history of mood disorders on several EF and non-EF neurocognitive measures: EF tasks that have been implicated include working memory, interference control, and set shifting and non-EF tasks that have been implicated include processing speed, sustained attention, and visuospatial memory (Dickstein et al., 2004; Doyle et al., 2005; Klimes-Dougan et al., 2006). Moreover, in addition to evidence of the sensitivity of these EF and non-EF neurocognitive constructs as potential risk factors for BD, there also is some evidence of their specificity. In other words, there is accumulating evidence for a specific profile of EF and non-EF neurocognitive deficits that precede the adult onset of BD but are unrelated to unipolar depression. For example, data from Meyer et al. (2004) show that individuals identified as having EF impairments during adolescence are much more likely to develop BD, but no more likely to develop unipolar depression, during young adulthood than adolescents without these deficits. Although these findings require replication with other samples, they present significant implications for prevention and early intervention.
Collectively, these studies indicate that EF deficits often accompany a variety of childhood psychopathologies; however, the nature of these deficits remains equivocal. Findings also suggest that EF tasks may be sensitive to the identification of deficits in childhood populations; however, they often lack specificity. Methodological differences across studies are problematic and may obfuscate subtle differences in EFs among children with different types of disorders. Future research is needed to elucidate further the specific types of EF deficits that co-occur with childhood externalizing and internalizing disorders and to determine whether these deficits are global or unique to each disorder.
It is the purpose of this review to examine the executive tests most commonly used within the research literature. This review will also examine the percentage of times that different executive function tests have shown significant between-group differences. In addition, this review will examine the percentage of comparisons between individual internalizing disorders and externalizing disorders, and control groups have shown significant differences.
Method
Search and Retrieval
We attempted to identify and retrieve all empirical studies and meta-analyses published after 1999 that examined executive functioning abilities in children and adolescents with specific internalizing and externalizing disorders. The search and retrieval process was conducted using the keywords: Executive Function + ADHD, Executive Function + Attention Deficit/Hyperactivity Disorder, Executive Function + Conduct Disorder, Executive Function + Oppositional Defiant Disorder, Executive Function + Tourette’s Disorder, Executive Function + Major Depressive Disorder, Executive Function + Dysthymia, Executive Function + Bipolar Disorder, Executive Function + Cyclothymia, Executive Function + Generalized Anxiety Disorder, Executive Function + Social Phobia, Executive Function + Obsessive Compulsive Disorder, Executive Function + OCD, Executive Function + Posttraumatic Stress Disorder, Executive Function + PTSD, Executive Function + Specific Phobia, Executive Function + Panic Disorder, Executive Functioning Deficits. The search and retrieval process included a comprehensive search of the following bibliographic databases: PsycINFO, PsycARTICLES, and MEDLINE. All studies were retrieved from the University of Rhode Island’s electronic library between June and August of 2010 and then again in January of 2012.
Eligibility Criteria
Studies were selected for review based on the following criteria:
-
1.
The study was published in English.
-
2.
The study was published no earlier than 2000.
-
3.
The study only included children and adolescent ages 18 and younger.
-
4.
The study involved the comparison of executive functioning performance between individuals with at least one of the specified internalizing or externalizing psychological disorders and a control group or a comparison group characterized by the presence of a psychological or psychiatric disorder. The specified internalizing and externalizing disorders included ADHD, conduct disorder, ODD, Tourette’s disorder, major depressive disorder, dysthymia, bipolar disorder, cyclothymia, generalized anxiety disorder, OCD, social phobia, PTSD, specific phobia, and panic disorder.
Results
A total of 141 studies were identified that met eligibility criteria and were included in the study. The studies are summarized in Table 5.1. Note that the “Number of Times Used” column represents the number of published articles that have used each of these tests to examine between-group comparisons. The “Sensitivity to Group Differences” column represents the total number of times each of these tests was used to examine between-group comparisons.
Across all studies that were examined, there were a total of 164 different tests used to measure executive function. As seen in Table 5.1, there were eight tests that were used to assess executive functioning in more than ten studies. The other 156 tests were used to assess executive function in less than ten studies. As expected, the percentage of times tests showed significant between-group differences varied across executive function tests. The BRIEF was associated with significant differences between clinical groups (% of comparisons), or between clinical and control groups (% of comparisons), 67 % of the times it was used. The Go/No-Go Test was associated with significant differences between clinical groups (% of comparisons), or between clinical and control groups (% of comparisons), 46 % of the times it was used.
The Continuous Performance Test and test variants were associated with significant differences between clinical groups (33 % of comparisons), or between clinical and control groups (50 % of comparisons), 43 % of the times it was used. Significant between-group differences on the Stroop Color and Word Test and test variants occurred 38 % of the total times it was used, with significant differences occurring during 17 % of comparisons between clinical groups and 59 % of comparisons between clinical and control groups. Significant between-group differences on the Trail Making Test occurred 36 % of the total times it was used, with significant between-group differences occurring during 19 % of comparisons between clinical groups and 44 % of comparisons between clinical and control groups. The WCST was associated with significant between-group differences 33 % of the total times it was used, with significant differences occurring during 16 % of comparisons between clinical groups and 43 % of comparisons between clinical and control groups. The ROCF Test and Rey Complex Figure Test were associated with significant differences between groups 33 % of the total times it was used, with significant differences occurring during 19 % of comparisons between clinical groups and 43 % comparisons between clinical and control groups. Finally, the TOL test and variants of the TOL were associated with significant differences between clinical groups or between clinical groups and controls only 4 % of the total times it was used, with significant differences occurring during 5 % of comparisons between clinical groups and 3 % of comparisons between clinical and control groups.
The percentage studies showing significant between-group differences across all executive function tests varied across clinical groups. The results are summarized in Table 5.2. Note that subtypes of clinical disorders were not differentiated. Also, comparisons that included subtypes of the same disorder (e.g., ADHD-HI and ADHD-C) and comparisons between groups of individuals with the same diagnosis (e.g., ADHD and ADHD comorbid with Specific Learning Disability) were excluded. In addition, comparisons using comorbid conditions for the diagnosis of interest were also excluded.
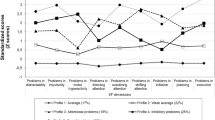
Studies comparing individuals with conduct disorder to other clinical or control groups found significant between-group differences 42 % of the time. Studies comparing individuals with ADHD to other clinical or controls groups found significant between-group differences on executive function test performance 40 % of the time. PTSD and a comparison group found significant between-group differences 31 % of the time. Studies comparing executive function test performance in individuals with major depressive disorder and a comparison group found significant between-group differences 28 % of the time, while studies comparing executive function test performance in individuals with OCD and a comparison group found significant between-group differences 21 % of the time. Studies comparing individuals with bipolar disorder to other clinical or control groups found significant between-group differences 20 % of the time, while studies examining executive function test performance in individuals with ODD found significant between-group differences 19 % of the time. Finally, studies examining Tourette’s disorder and a comparison group found significant between-group differences 15 % of the time.
Discussion
Currently there are a vast number of neuropsychological measures purported to measure executive functioning or individual isolated components of executive functioning. While some studies use standardized neuropsychological assessments such as the Development Neuropsychological Assessment (NEPSY) (Spruyt, Capdevila, Kheirandish-Gozal, & Gozal, 2009) to assess executive functioning, many others have primarily relied on tests created within research labs and that have been used exclusively for research purposes (Gohier et al., 2009). Due to the enormous variability in the type of assessments used for executive functioning assessment, the purpose of this study was to conduct a comprehensive review of the literature to determine which executive functioning tests are used most often among researchers when assessing executive functioning in samples of individuals with internalizing and externalizing forms of psychopathology. Similarly, this review also examined the frequency with which the most commonly used tests of executive function reveal significant differences in performance between clinical and control participant groups as well as between multiple clinical participant groups. In addition, as executive functioning impairments are reported to be characteristic of a number of different internalizing and externalizing forms of psychopathology (Willcutt, Pennington, Olson, Chhabildas, & Hulslander, 2005), the proportion of research studies in which individuals with specific forms of internalizing and externalizing forms of psychopathology demonstrate impairments on executive functioning test performance remains unexplored. Therefore, this review also provided a comparison of the total proportion of studies that have found significant differences between clinical and control participant groups and multiple clinical participant groups across different forms of psychopathology.
In order to identify the executive functioning tests and assessments most commonly used within the internalizing and externalizing psychopathology research literature, we conducted an extensive literature search and review of all related articles published between 2000 and 2011. We compiled a database that included all relevant studies that met our inclusion/exclusion criteria and were then able to identify the wide range of different executive functioning tests that have been used and identify the frequency of their usage. Although there were a total of 164 identified measures of executive functioning, we only provided further analyses for the executive tests that were used with a relatively higher frequency. Based on our findings, authors tend to use The Stroop Color-Word Test and variants, WCST and variants, and Trail Making Test and variants more often than other measures of executive function. This finding suggests that much of what is currently known about childhood/adolescent executive functioning abilities in internalizing and externalizing forms of psychopathology is dependent on the quality of these three assessments.
Despite their widespread usage, these tests are not necessarily the most effective at discriminating between different clinical and control groups. Indeed, results have revealed that the BRIEF, the Continuous Performance Test and variants, and the Go/No-Go Test are sensitive to between-group differences more often than each of the three more commonly used tests. These results indicate that perhaps different executive functioning assessments may be more appropriate for addressing different types of research questions. Furthermore, these results may help shed light on the inconsistent results between studies examining executive functioning impairments in individuals with psychopathology. Given that there were a total of 164 executive tests used, it is undeniable that these tests ultimately measure the executive function construct or components of the executive function construct with more or less accuracy. Similarly, since some measures are more sensitive to group differences than others, the reported findings from individual studies may be a function of the test used rather than the executive function purported to be assessed.
Findings also revealed considerable variability in the proportion of times that participant groups with specific forms of internalizing and externalizing forms of psychopathology demonstrated impaired performance on executive function tests. Based on the present findings, when compared to clinical or control groups, individuals with conduct disorder and ADHD tend to more often show performance differences on executive function measures compared to individuals with disorders such as Tourette’s disorder and ODD. In addition, there was also noticeable variability in the degree to which the specified clinical groups demonstrated significant differences in executive function test performance when their performance was compared to other clinical groups or control groups. These findings suggest that when compared to other clinical and/or control groups, individuals with some forms of psychopathology, such as major depressive disorder, demonstrate executive functioning performance differences more often than individuals with other forms of psychopathology.
Limitations
The present study identified specific inclusion criteria and 141 studies were included. Clearly a comprehensive review of the frequencies and proportions of executive tests used across the entire body of executive functioning literature was beyond the scope of this paper. It is quite possible, however, that the inclusion of all disorders within the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR; American Psychiatric Association, 2000) would lead to different results. Similarly, although not a focus of the present review, these results did not disaggregate by age, which prohibits an examination of the degree to which different tests are used across different developmental levels.
For several of the clinical groups examined, there were only a very limited number of studies that have examined executive function performance. For instance, there were no between-group comparisons that included individuals with panic disorder, social phobia, generalized anxiety, specific phobia, cyclothymia, and dysthymia. This finding considerably limits the degree to which we can compare the results for these disorders to the disorders more commonly examined (e.g., ADHD, bipolar disorder).
Although we examined the proportion of studies that found significant between-group differences across different executive functioning measures, we did not use meta-analytic procedures that take into account effect sizes and the magnitude of between-group differences. However, the purpose of this review was to examine the current body of existing literature and identify the most commonly used executive functioning assessments, as well as determine the proportion of studies related to internalizing and externalizing forms of psychopathology that report significant between-group differences in executive functioning performance. Although the application of meta-analytic procedures would be quite informative, examining the magnitude of between-group differences on executive functioning tests was not the aim of this review.
Suggestions for Future Research
This selective review of literature concerning EFs in externalizing and internalizing childhood disorders has revealed a number of interesting findings. Regarding ADHD, studies collectively suggest that EF deficits are neither unique to the disorder nor are they necessary or sufficient for a diagnosis of ADHD. When EF impairments are present with ADHD, they tend to be specific rather than global impairments. Findings are inconsistent as to whether comorbid disorders are related to EFs in children with ADHD. With regard to CD, earlier studies suggested that EF deficits were not characteristic of children with CD after comorbid ADHD was statistically controlled for; however, recent findings suggest that EF deficits may indeed be characteristic of both children with CD and children with ADHD. No clear pattern of EF deficits emerges in the literature concerning children with TD. A few studies, but not all, have reported greater response-time variability on continuous performance tasks with this population. Preliminary studies suggest that working memory is not characteristically impaired with children with TD. Results are equivocal with respect to the performance of these children on planning tasks and measures of cognitive flexibility. Overall, distinct and robust impairments in EF do not appear to be characteristic of children with TD. Additional, methodologically sound studies are needed to address whether subtle differences in EF may exist between children with TD and other types of childhood psychopathology.
With regard to internalizing disorders of childhood, the current research literature on the relationship between EF deficits and internalized forms of developmental psychopathology is unequally distributed. Specifically, in contrast to research conducted with adult populations, very little research has been conducted linking EF to child and adolescent depression. This dearth of evidence seems curious, given the popularity of cognitive-behavioral interventions and the use of psychotropic medications to treat depression among youth. On the other hand, it is perhaps understandable, given the taxometric identification of a broadband, internalizing, or anxious-depressed syndrome that has been identified in empirical investigations of child and adolescent populations (Achenbach & Edelbrock, 1983), contrasted with less support for the kinds of narrowband classification distinctions made among DSM-IV-TR diagnoses (American Psychiatric Association, 2000).
In addition, several studies have been conducted in the area of childhood BD and EF (Dickstein et al., 2004; Doyle et al., 2005), and the longitudinal work that has been conducted in this area (Klimes-Dougan et al., 2006; Meyers et al., 2004) provides important implications for prevention and early intervention. Similarly, with the exception of OCD, research also has begun to accumulate that assesses potential EF deficits among children with a variety of kinds of anxiety disorders (Beers & De Bellis, 2002; Emerson et al., 2005; Toren et al., 2000). Finally, there seems to be an emerging consensus about the importance of differentiating early- vs. late-onset of OCD (e.g., Geller et al., 2001), and research has documented EF differences among adults with these two subtypes (Roth, Milovan, Baribeau, & O’Connor, 2005). Developmental studies, however, have yet to be conducted in this area. Also, future studies examining a wider range of psychological and psychiatric disorders may better reflect the true frequency with which different executive function tests are used.
Given the findings of the current review, authors of future studies examining between-group performances in executive functioning should choose their executive function measures carefully. It must be recognized that some executive function measures (e.g., the BRIEF) are more likely to reveal between-group differences than other measures (e.g., TOL and variants) despite the fact that both measures are purported to measure executive functioning. These findings are pertinent to clinicians as it appears that some neuropsychological tests of executive functioning are better than others at discriminating between clinical groups or clinical groups and controls groups.
References
Achenbach, T. M., & Edelbrock, C. (1983). Child behavior checklist. Burlington, VT: University Associates in Psychiatry.
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (rev.). Washington, DC: Author.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington: Author.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121, 65–94.
Barkley, R. A. (2010). Differential diagnosis of adults with ADHD: The role of EF and self regulation. The Journal of Clinical Psychiatry, 71(7), e17. doi:10.4088/JCP.9066tx1c.
Barkley, R. A., Edwards, G., Laneri, M., Fletcher, K., & Metevia, L. (2001). Executive functioning, temporal discounting, and sense of time in adolescents with attention deficit hyperactivity disorder (ADHD) and oppositional defiant disorder (ODD). Journal of Abnormal Child Psychology, 29, 541–556.
Barkley, R. A., Grodzindky, G., & DuPaul, G. J. (1992). Frontal lobe functions in attention deficit disorder with and without hyperactivity: A review and research report. Journal of Abnormal Child Psychology, 20, 163–188.
Barkley, R. A., Murphy, K. R., & Bush, T. (2001). Time perception and reproduction in young adults with attention deficit hyperactivity disorder. Neuropsychology, 15, 351–360.
Beck, A. T. (1978). Depression inventory (BDI). Philadelphia: Center for Cognitive Therapy.
Beers, S. R., & De Bellis, M. D. (2002). Neuropsychological function in children with maltreatment-related posttraumatic stress disorder. American Journal of Psychiatry, 159(3), 483–486.
Berlin, L., Bohlin, G., Nyberg, L., & Janols, L. O. (2004). How well do measures of inhibition and other executive functions discriminate between children with ADHD and controls? Child Neuropsychology, 10, 1–13.
Berlin, L., Bohlin, G., & Rydell, A. M. (2003). Relations between inhibition, executive functioning, and ADHD symptoms: A longitudinal study from age 5 to 8 ½ years. Child Neuropsychology, 9, 255–266.
Biederman, J. (2003). Pharmacotherapy for attention-deficit/hyperactivity disorder (ADHD) decreases the risk for substance abuse: Findings from a longitudinal follow-up of youths with and without ADHD. Journal of Clinical Psychiatry, 64, 3–8.
Biederman, J., Petty, C. R., Fried, R., Doyle, A. E., Spencer, T., Seidman, L. J., et al. (2007). Stability of executive function deficits into young adult years: A prospective longitudinal follow-up study of grown up males with ADHD. Acta Psychiatrica Scandinavica, 116, 129–136.
Byrne, J. M., DeWolfe, N. A., & Bawden, H. N. (1998). Assessment of attention-deficit hyperactivity disorder in preschoolers. Child Neuropsychology, 4, 49–66.
Carrion, V. G., Garrett, A., Menon, V., Weems, C. F., & Reiss, A. L. (2008). Posttraumatic stress symptoms and brain function during a response inhibition task: An fMRI study in youth. Depression and Anxiety, 25(6), 514–526.
Chang, S. W., McCracken, J. T., & Piacentini, J. C. (2007). Neurocognitive correlates of child obsessive compulsive disorder and Tourette’s syndrome. Journal of Clinical and Experimental Neuropsychology, 29, 724–733.
Channon, S. (1996). Executive dysfunction in depression: The Wisconsin card sorting test. Journal of Affective Disorders, 39(2), 107–114.
Channon, S., Pratt, P., & Robertson, M. M. (2003). Executive function, memory, and learning in Tourette’s syndrome. Neuropsychology, 17, 247–254.
Cirino, P. T., Chapieski, M. L., & Massman, P. J. (2000). Card sorting performance and ADHD symptomatology in children and adolescents with Tourette syndrome. Journal of Clinical and Experimental Neuropsychology, 22, 245–256.
Clark, C., Prior, M., & Kinsella, G. J. (2000). Do executive function deficits differentiate between adolescents with ADHD and oppositional defiant/conduct disorder? A neuropsychological study using the Six Elements Test and Hayling Sentence Completion Test. Journal of Abnormal Child Psychology, 28, 403–414.
Costello, E. J., Pine, D. S., Hammen, C., March, J. S., Plotsky, P. M., Weissman, M. M., et al. (2002). Development and natural history of mood disorders. Biological Psychiatry, 52(6), 529–542.
Crawford, S., Channon, S., & Robertson, M. M. (2005). Tourette’s syndrome: Performance on tests of behavioural inhibition, working memory and gambling. Journal of Child Psychology and Psychiatry, 46, 1327–1336.
Delis, D. C., Cullum, C. M., Butters, N., Cairns, P., & Prifitera, A. (1988). Wechsler memory scale-revised and california verbal learning test: Convergence and divergence. The Clinical Neuropsychologist, 2(2), 188–196.
Denckla, M. B. (1996). A theory and model of executive function: A neuropsychological perspective. In G. R. Lyon & N. A. Krasnegor (Eds.), Attention, memory, and executive function (pp. 263–277). Baltimore: Paul H. Brookes.
Dickstein, D. P., Treland, J. E., Snow, J., McClure, E. B., Mehta, M. S., Towbin, K. E., et al. (2004). Neuropsychological performance in pediatric bipolar disorder. Biological Psychiatry, 55(1), 32–39.
Doyle, A. E., Wilens, T. E., Kwon, A., Seidman, L. J., Faraone, S. V., Fried, R., et al. (2005). Neuropsychological functioning in youth with bipolar disorder. Biological Psychiatry, 58(7), 540–548.
DuPaul, G. J., McGoey, K. E., Eckert, T. L., & VanBrakle, J. (2001). Preschool children with attention-deficit/hyperactivity disorder: Impairments in behavioral, social, and school functioning. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 508–515.
Emerson, C. S., Mollet, G. A., & Harrison, D. W. (2005). Anxious-depression in boys: An evaluation of executive functioning. Archives of Clinical Neuropsychology, 20(4), 539–546.
Evans, D. W., & Leckman, J. F. (2006). Definitions and clinical descriptions 405. Developmental Psychopathology: Risk, Disorder, and Adaptation, 3, 404.
Fischer, M., Barkley, R. A., Smallish, L., & Fletcher, K. (2005). Executive functioning in hyperactive children as young adults: Attention, inhibition, response perseveration, and the impact of comorbidity. Developmental Neuropsychology, 27, 107–133.
Fletcher, J. M. (1996). Executive functions in children: Introduction to the special series. Developmental Neuropsychology, 12, 1–3.
Friedlander, L., & Desrocher, M. (2006). Neuroimaging studies of obsessive–compulsive disorder in adults and children. Clinical Psychology Review, 26(1), 32–49.
Friedman, N. P., Haberstick, B. C., Willcutt, E. G., Miyake, A., Young, S. E., Corley, R. P., et al. (2007). Greater attention problems during childhood predict poorer executive functioning in late adolescence. Psychological Science, 18, 898–900.
Fuggetta, G. P. (2006). Impairment of executive functions in boys with attention deficit/hyperactivity disorder. Child Neuropsychology, 12, 1–21.
Geller, D. A., Biederman, J., Faraone, S. V., Bellordre, C. A., Kim, G. S., Hagermoser, L., et al. (2001). Disentangling chronological age from age of onset in children and adolescents with obsessive-compulsive disorder. The International Journal of Neuropsychopharmacology, 4(2), 169–178.
Geller, B., & Luby, J. (1997). Child and adolescent bipolar disorder: A review of the past 10 years. Journal of the American Academy of Child and Adolescent Psychiatry, 36(9), 1168–1176.
Geurts, H. M., Verte, S., Oosterlaan, J., Roeyers, H., & Sergeant, J. A. (2005). ADHD subtypes: Do they differ in their executive functioning profile? Archives of Clinical Neuropsychology, 20, 457–477.
Giancola, P. R., Mezzich, A. C., & Tarter, R. E. (1998). Executive cognitive functioning, temperament, and antisocial behavior in conduct-disordered adolescent females. Journal of Abnormal Psychology, 107, 629–641.
Gohier, B., Ferracci, L., Surguladze, S. A., Lawrence, E., El Hage, W., Kefi, M. Z., et al. (2009). Cognitive inhibition and working memory in unipolar depression. Journal of Affective Disorders, 116(1), 100–105.
Gray, J. A. (1987). Perspectives on anxiety and impulsivity: A commentary. Journal of Research in Personality, 21(4), 493–509.
Hankin, B. L., Abramson, L. Y., Moffitt, T. E., Silva, P. A., McGee, R., & Angell, K. E. (1998). Development of depression from preadolescence to young adulthood: Emerging gender differences in a 10-year longitudinal study. Journal of Abnormal Psychology, 107(1), 128–140.
Hankin, B. L., Fraley, R. C., Lahey, B. B., & Waldman, I. D. (2005). Is depression best viewed as a continuum or discrete category? A taxometric analysis of childhood and adolescent depression in a population-based sample. Journal of Abnormal Psychology, 114(1), 96–110.
Harris, E. L., Schuerholz, L. J., Singer, H. S., Reader, M. J., Brown, J. E., Cox, C., et al. (1995). Executive function in children with Tourette syndrome and/or attention deficit hyperactivity disorder. Journal of the International Neuropsychological Society, 1, 511–516.
Heaton, R. K. (1981). A manual for the Wisconsin card sorting test. Los Angeles: Western Psychological Services.
Herba, C. M., Tranah, T., Rubia, K., & Yule, W. (2006). Conduct problems in adolescence: Three domains of inhibition and effect of gender. Developmental Neuropsychology, 30, 659–695.
Hinshaw, S. P., Carte, E. T., Fan, C., Jassy, J. S., & Owens, E. B. (2007). Neuropsychological functioning of girls with attention-deficit/hyperactivity disorder followed prospectively into adolescence: Evidence for continuing deficits? Neuropsychology, 21, 263–273.
Jurado, M. B., & Rosselli, M. (2007). The elusive nature of executive functions: A review of our current understanding. Neuropsychology Review, 17, 213–233.
Kessler, R. C., Gruber, M., Hettema, J. M., Hwang, I., Sampson, N., & Yonkers, K. A. (2008). Co-morbid major depression and generalized anxiety disorders in the National Comorbidity Survey follow-up. Psychological Medicine, 38(3), 365–374.
Kim, M. S., Kim, J. J., & Kwon, J. S. (2001). Frontal P300 decrement and executive dysfunction in adolescents with conduct problems. Child Psychiatry and Human Development, 32, 93–106.
Klimes-Dougan, B., Ronsaville, D., Wiggs, E. A., & Martinez, P. E. (2006). Neuropsychological functioning in adolescent children of mothers with a history of bipolar or major depressive disorders. Biological Psychiatry, 60(9), 957–965.
Klimkeit, E. I., Mattingley, J. B., Sheppard, D. M., Lee, P., & Bradshaw, J. L. (2005). Motor preparation, motor execution, attention, and executive functions in attention deficit/hyperactivity disorder (ADHD). Child Neuropsychology, 11, 153–173.
Kovacs, M., & Beck, A. T. (1977). An empirical-clinical approach toward a definition of childhood depression. In J. G. Schulterbrandt & A. Raskin (Eds.), Depression in childhood: Diagnosis, treatment, and conceptual models (pp. 1–25). New York: Raven Press.
Lawrence, V., Houghton, S., Tannock, R., Douglas, G., Durkin, K., & Whiting, K. (2002). ADHD outside the laboratory: Boys’ executive function performance on tasks in videogame play and on a visit to the zoo. Journal of Abnormal Child Psychology, 30, 447–462.
Mahone, E. M., Cirino, P. T., Cutting, L. E., Cerrone, P. M., Hagelthorn, K. M., Hiemenz, J. R., et al. (2002). Validity of the Behavior Rating Inventory of Executive Function in children with ADHD and/or Tourette syndrome. Archives of Clinical Neuropsychology, 17, 643–662.
Mahone, E. M., & Hoffman, J. (2007). Behavior ratings of executive function among preschoolers with ADHD. Clinical Neuropsychology, 21, 569–586.
Mahone, E. M., Pillion, J. P., & Heimenz, J. R. (2001). Initial development of an auditory continuous performance test for preschoolers. Journal of Attention Disorders, 5, 93–106.
McBurnett, K., Harris, S. M., Swanson, J. M., Pfiffner, L. J., Tamm, L., & Freeland, D. (1993). Neuropsychological and psychophysiological differentiation of inattention/overactivity and aggression/defiance symptom groups. Journal of Clinical Child Psychology, 22, 165–171.
Meyers, C. A., Smith, J. A., Bezjak, A., Mehta, M. P., Liebmann, J., Illidge, T., et al. (2004). Neurocognitive function and progression in patients with brain metastases treated with whole-brain radiation and motexafin gadolinium: Results of a randomized phase III trial. Journal of Clinical Oncology, 22(1), 157–165.
Moffitt, T. E., & Henry, B. (1989). Neuropsychological assessment of executive functions in self-reported delinquents. Development and Psychopathology, 1, 105–118.
Morgan, A. B., & Lilienfeld, S. O. (2000). A meta-analytic review of the relation between antisocial behavior and neuropsychological measures of executive function. Clinical Psychology Review, 20, 113–136.
Nigg, J. T., Blaskey, L. G., Huang-Pollock, C., & Rappley, M. D. (2002). Neuropsychological executive functions and DSM-IV ADHD subtypes. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 59–66.
Osterrieth, P. (1944). The test of copying a complex figure: A contribution to the study of perception and memory. Archive de Psychologie, 30, 206–356.
Ozonoff, S., & Jensen, J. (1999). Brief report: Specific executive function profiles in three neurodevelopmental disorders. Journal of Autism and Developmental Disorders, 29, 171–177.
Ozonoff, S., & Strayer, D. L. (2001). Further evidence of intact working memory in autism. Journal of Autism and Developmental Disorders, 31, 257–263.
Pennington, B. F., & Ozonoff, S. (1996). Executive functions and developmental psychopathology. Journal of Child Psychology and Psychiatry, 37, 51–87.
Prisciandaro, J. J., & Roberts, J. E. (2005). A taxometric investigation of unipolar depression in the National Comorbidity Survey. Journal of Abnormal Psychology, 114(4), 718–728.
Radke-Yarrow, M. (1998). Children of depressed mothers: From early childhood to maturity. Cambridge, England: University Press.
Rhodes, S. M., Coghill, D. R., & Matthews, K. (2005). Neuropsychological functioning in stimulant-naïve boys with hyperkinetic disorder. Psychological Medicine, 35, 1109–1120.
Rinsky, J. R., & Hinshaw, S. P. (2011). Linkages between childhood executive functioning and adolescent social functioning and psychopathology in girls with ADHD. Child Neuropsychology, 17, 368–390.
Roth, R. M., Milovan, D., Baribeau, J., & O’Connor, K. (2005). Neuropsychological functioning in early-and late-onset obsessive-compulsive disorder. The Journal of Neuropsychiatry and Clinical Neurosciences, 17(2), 208–213.
Schuerholz, L. J., Singer, H. S., & Denckla, M. B. (1998). Gender study of neuropsychological and neuromotor function in children with Tourette syndrome with and without attention-deficit hyperactivity disorder. Journal of Child Neurology, 13, 277–282.
Seidman, L. J., Biederman, J., Faraone, S. V., Weber, W., & Ouellete, C. (1997). Toward defining a neuropsychology of attention deficit-hyperactivity disorder: Performance of children and adolescents from a large clinically referred sample. Journal of Consulting and Clinical Psychology, 65, 150–160.
Seidman, L. J., Biederman, J., Weber, W., Hatch, M., & Faraone, S. V. (1998). Neuropsychological functioning in adults with attention-deficit hyperactivity disorder. Biological Psychiatry, 44, 260–268.
Sergeant, J. A., Geurts, H., & Oosterlaan, J. (2002). How specific is a deficit of executive functioning for attention-deficit/hyperactivity disorder? Behavioural Brain Research, 130, 3–28.
Shin, M. S., Choi, H., Kim, H., Hwang, J. W., Kim, B. N., & Cho, S. C. (2008). A study of neuropsychological deficit in children with obsessive-compulsive disorder. European Psychiatry, 23(7), 512–520.
Shucard, D. W., Benedict, R. H., Tekok-Kilic, A., & Lichter, D. G. (1997). Slowed reaction time during a continuous performance test in children with Tourette’s syndrome. Neuropsychology, 11, 147–155.
Speltz, M. L., DeKlyen, M., Calderon, R., Greenberg, M. T., & Fisher, P. A. (1999). Neuropsychological characteristics and test behaviors of boys with early onset conduct problems. Journal of Abnormal Psychology, 108, 315–325.
Spielberger, C. D., Edwards, C. D., Lushene, R. E., Montuori, J., & Platzek, D. (1973). STAIC, state-trait anxiety inventory for children. Redwood City, CA: Mind Garden.
Spreen, O., & Strauss, E. (1991). A compendium of neuropsychological tests: Administration, norms and commentary. New York: Oxford University Press.
Spreen, O., & Strauss, E. (1998). A compendium of neuropsychological tests: Administration, norms, and commentary (2nd ed.). New York: Oxford University Press.
Spruyt, K., Capdevila, O. S., Kheirandish-Gozal, L., & Gozal, D. (2009). Inefficient or insufficient encoding as potential primary deficit in neurodevelopmental performance among children with OSA. Developmental Neuropsychology, 34(5), 601–614.
Toren, P., Wolmer, L., Rosental, B., Eldar, S., Koren, S., Lask, M., et al. (2000). Case series: Brief parent–child group therapy for childhood anxiety disorders using a manual-based cognitive-behavioral technique. Journal of the American Academy of Child and Adolescent Psychiatry, 39(10), 1309–1312.
Toupin, J., Dery, M., Pauze, R., Mercier, H., & Fortin, L. (2000). Cognitive and familial contributions to conduct disorder in children. Journal of Child Psychology and Psychiatry, 41, 333–344.
Tsal, Y., Shalev, L., & Mevorach, C. (2005). The diversity of attention deficits in ADHD: The prevalence of four cognitive factors in ADHD versus controls. Journal of Learning Disabilities, 38, 142–157.
Weyandt, L. L. (2004). Neuropsychological performance of adults with ADHD. In D. Gozal & D. Molfese (Eds.), Attention deficit hyperactivity disorder: From genes to animal models to patients. Totowa, NJ: Humana Press.
Weyandt, L. L. (2005). Executive function in children, adolescents, and adults with attention deficit hyperactivity disorder: Introduction to the special issue. Developmental Neuropsychology, 27, 1–10.
Weyandt, L. L. (2009). Executive functions and attention deficit hyperactivity disorder. The ADHD Report, 17(6), 1–7.
Weyandt, L. L., Rice, J. A., Linterman, I., Mitzlaff, L., & Emert, E. (1998). Neuropsychological performance of a sample of adults with ADHD, developmental reading disorder, and controls. Developmental Neuropsychology, 14, 643–656.
Weyandt, L. L., & Willis, W. G. (1994). Executive functions in school-aged children: Potential efficacy of tasks in discriminating clinical groups. Developmental Neuropsychology, 10, 27–38.
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biological Psychiatry, 57, 1336–1346.
Willcutt, E. G., Pennington, B. F., Olson, R. K., Chhabildas, N., & Hulslander, J. (2005). Neuropsychological analyses of comorbidity between reading disability and attention deficit hyperactivity disorder: In search of the common deficit. Developmental Neuropsychology, 21, 35–78.
Woodcock, R. W., & Johnson, M. B. (1989). WJ-R tests of cognitive ability. Itasca, IL: Riverside.
Wu, K. K., Anderson, V., & Castiello, U. (2002). Neuropsychological evaluation of deficits in executive functioning for ADHD children with or without learning disabilities. Developmental Neuropsychology, 22, 501–531.
Zahn-Waxler, C., Klimes-Dougan, B., & Slattery, M. (2000). Internalizing disorders of childhood and adolescence: Progress and prospects for advances in understanding anxiety and depression. Development and Psychopathology, 12, 443–466.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Weyandt, L.L. et al. (2014). A Review of the Use of Executive Function Tasks in Externalizing and Internalizing Disorders. In: Goldstein, S., Naglieri, J. (eds) Handbook of Executive Functioning. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-8106-5_5
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8106-5_5
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-8105-8
Online ISBN: 978-1-4614-8106-5
eBook Packages: Behavioral ScienceBehavioral Science and Psychology (R0)