
Abstract
Tobacco use is the only shared risk factor for the world’s four leading noncommunicable diseases: cardiovascular disease, diabetes, cancer, and chronic respiratory illnesses. Tobacco use accounts for six million deaths annually, including an estimated 600,000 deaths from nonsmokers involuntarily exposed to secondhand smoke (World Health Organization. Fact Sheet Number 339—tobacco. Retrieved July 28, 2011, from http://www.who.int/mediacentre/factsheets/fs339/en/index.html, 2011d). In addition to cigarette smoking, which is the most common form of tobacco use, the evolution of patterns of tobacco use, or more precisely, the pursuit of nicotine, has resulted in the development of novel products from pharmaceutical companies (nicotine replacement therapy), entrepreneurs (nicotine water and electronic cigarettes), and tobacco companies (snus and dissolvables). These products are changing the face of nicotine addiction, and their influence on dual use patterns, cessation, and nicotine uptake are largely unclear. This chapter discusses the harm caused by tobacco and secondhand smoke, as well as smoking prevalence rates worldwide. The tobacco industry is discussed in terms of its economic value, its marketing techniques, the industry’s undue influence, and the basics of growing tobacco. Global tobacco control initiatives, such as the World Health Organization’s Framework Convention on Tobacco Control, and global methods for curbing tobacco use are discussed and presented as a means for controlling tobacco globally, as well as the possible relevance of tobacco control strategies for the reduction of other chronic disease risk factors
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
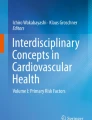
Noncommunicable diseases (NCDs), including heart attacks and strokes, cancers, diabetes, and chronic respiratory disease kill more than 36 million people annually and account for over 63 % of worldwide deaths (WHO 2011f, g). Tobacco use is the only shared risk factor for the four leading NCDs (see Fig. 8.1), and globally tobacco use kills nearly as many people annually as the other three risk factors combined (WHO 2008, 2011f). Cigarettes, the primary cause of the world’s most damaging NCDs, are the most deadly artifact in human history (Proctor 2012a). Tobacco use was responsible for 100 million deaths in the twentieth century, and if current trends continue, approximately one billion people will die from tobacco use during the twenty-first century (Peto and Lopez 2000).

Noncommunicable diseases and risk factors. Reproduced with permission by WHO. Credit: WHO
Harm from Tobacco and Secondhand Smoke Exposure
When individuals inhale cigarette smoke, either directly or secondhand, they are inhaling more than 7,000 chemicals: hundreds of these are hazardous, and at least 69 are known to cause cancer. (U.S. Department of Health and Human Services 2010)
Active Smoking
At the beginning of the twentieth century, lung cancer, nearly always caused by cigarette smoking, was considered rare, and Dr. Isaac Adler, a pioneer in lung cancer research, noted its rarity in 1912, saying:
On one point, however, there is nearly complete consensus of opinion, and that is that primary malignant neoplasms of the lungs are among the rarest forms of the disease. This latter opinion that the extreme rarity of primary tumors has persisted for centuries (Adler 1912).
During the twentieth century, the evidence establishing the causal link between smoking and cancer continued to develop. Through experimental research, in the early 1930s Angel Roffo demonstrated that cancers developed along the “smoking highway” (lips, tongue, throat, cheek, bronchial passages, etc.) wherever the tissue was exposed to tars during the act of smoking (Proctor 2006). Today, clinical observation, experimental research, and epidemiological research have overwhelmingly established the causal relationship between smoking and cancer.
The fact that smoking causes so much cancer, and so little is done to prevent it, is a worldwide tragedy and embarrassment. Tobacco use results in almost six million deaths globally each year, and smoking causes cancers of the lung, larynx, oral cavity, pharynx, esophagus, pancreas, bladder, kidney, cervix, stomach, and can cause acute leukemia (US DHHS 2004; WHO 2012a). Each year, approximately one and a half million people die from lung cancer throughout the world, and nearly 80 % of male and almost 50 % of female lung cancer deaths are the result of smoking (Ezzati and Lopez 2003). The smoking and cancer link is so severe that since 1980, middle-aged men in Poland were more likely to die from smoking-related cancers than from all other causes of cancer combined (see Fig. 8.2) (IARC 2007a). In 2012 in the USA, estimates indicate that more Americans will die from lung and bronchus cancer (160,340) than from the next four leading causes of cancer combined (colon: 51,690, breast: 39,510, pancreas: 37,390, and prostate: 28,170) (ACS 2012). Due to the delayed disease burden of smoking, global lung cancer rates and deaths are expected to continue to rise and an estimated two million people will die annually from lung cancer during the next few decades (Proctor 2012b).

Smoking-attributed cancers in males in Poland result in more deaths than all other cancers combined. Reproduced with permission by Tobacco Control. Credit: Tobacco Control
In addition to causing lung and other cancers, tobacco use is a cause of death for the other leading NCDs, and the number of individuals impacted is expected to increase globally in the coming decades. Cardiovascular disease is the leading global cause of death, and smoking is a risk factor for cardiovascular diseases, such as coronary heart disease and stroke (US DHHS 2004; WHO 2011a). Smoking increases illness and death among diabetics by exacerbating common diabetes-related complications among the 346 million individuals who have diabetes worldwide (Haire-Joshu et al. 1999; WHO 2011c). Smoking is the primary cause of chronic respiratory illnesses, such as chronic obstructive pulmonary disease, which inflicts over 64 million people globally and is not curable (US DHHS 2004; WHO 2011b).
The harm associated with tobacco use is a function of nicotine addiction and the desire to obtain nicotine as quickly and efficiently as possible. Combustion, or burning tobacco leaves, is the traditional way of absorbing nicotine. In addition to delivering nicotine efficiently to the bloodstream, combustion creates carbon monoxide, nitrosamines, other tobacco-specific carcinogens, and a variety of other toxic substances resulting in a myriad of health effects and problems to the cardio-respiratory system, such as lung cancer, emphysema, and heart disease. When tobacco is used orally, it causes mouth cancer and other harm to the oral mucosa. When human tissue is exposed to the carcinogens in tobacco smoke or products, major harm results to all areas exposed, hence Roffo’s “smoking highway” of the 1930s (Proctor 2006).
Globally, tobacco use is responsible for approximately 16 % of deaths among men and 7 % of deaths among women age 30 and older, with the highest mortality rates occurring in high- and middle-income countries (see Table 8.1) (WHO 2012c). Tobacco-related deaths are concentrated in these populations because sufficient time has passed since the significant uptake of cigarette smoking within the population, and the countries are now experiencing the delayed illness and mortality caused by smoking (Thun et al. 2012). For example, in the USA approximately 400,000 smokers die each year as a result of smoking, and an additional eight million current and former smokers are living with a chronic condition caused by smoking (Hyland et al. 2003).
The harm from tobacco use varies as a function of how the nicotine is delivered. For example, if nicotine is absorbed as part of nicotine replacement therapy (NRT) provided by pharmaceutical companies to assist with smoking cessation, the harm is minimal. These NRT products undergo rigorous premarket testing to assure their safety and efficacy. If nicotine is absorbed through some of the many novel nicotine delivery systems that are currently being introduced, such as snus, electronic cigarettes (e-cigarettes), dissolvables, and orbs, the risk is unknown due to the lack of research and regulation of these new products (see Global Types of Tobacco: Novel Nicotine Products). If nicotine is absorbed orally through smokeless tobacco, the damage tends to be located in the oral cavity. If nicotine is absorbed through combusted tobacco products, the harm is inflicted throughout the body, but particularly in the cardio-pulmonary areas. The use of tobacco to obtain nicotine is harmful whether the products are smoked, chewed or inhaled, and subsequently there is no safe way of using tobacco. Additional research is needed to determine if there are safer ways to obtain nicotine, such as NRT, and novel products need to be evaluated for safety and efficacy before being allowed on the commercial market.
Secondhand Smoke
Secondhand smoke, also known as passive smoking, involuntary smoking, or “forced smoking,” harms individuals who have made the conscious decision not to smoke or who are unable to remove themselves from exposure to someone else’s smoke. Nonsmokers exposed to secondhand smoke inhale the same carcinogens inhaled by smokers (mainstream smoke), as well as the unfiltered smoke that comes from the burning end of the cigarette (sidestream smoke), and the associated health effects of chronic exposure have been a public health concern for decades. Documentation of the increased lung cancer risk from secondhand smoke began to emerge in the early 1980s based on epidemiological analyses in Greece, Japan, and the USA (Trichopoulos et al. 1981; Hirayama 1981; Garfinkel 1981). The level of public health concern rose substantially in 1986 when three organizations issued studies linking the risk of lung cancer and exposure to secondhand smoke. The International Agency for Research on Cancer (IARC), the U.S. National Research Council, and the U.S. Surgeon General all concluded that involuntary exposure to secondhand smoke causes increased cancer risk (IARC 1986; National Research Council 1986; U.S. Department of Health and Human Services 2006). In 1992, the U.S. Environmental Protection Agency concluded that secondhand smoke was a human lung carcinogen and responsible for 3,000 lung cancer deaths annually in U.S. nonsmokers (EPA 1992). The 2006 Surgeon General’s Report on Involuntary Smoking confirmed the causal relationship between secondhand smoke and lung cancer, estimating a 20–30 % increased risk of lung cancer for a nonsmoker living with a smoker (US DHHS 2006).
There is no safe level of exposure to secondhand smoke, and the act of breathing secondhand smoke immediately harms the respiratory and cardiovascular systems (US DHHS 2006). The 2006 U.S. Surgeon General’s report on involuntary smoking documented the dangers of secondhand smoke exposure and found sufficientFootnote 1 and suggestiveFootnote 2 evidence of many diseases and illnesses among adults and children exposed to secondhand smoke. Exposure to secondhand smoke over the long term can result in lung cancer and coronary artery disease in adults. Expectant mothers, fetuses, and infants are at particular risk of negative health consequences when exposed to secondhand smoke. Infants and children who are exposed to secondhand smoke can experience low birth weight, respiratory problems, and behavioral and learning issues, and exposure contributes to Sudden Infant Death Syndrome (SIDS) (US DHHS 2006).
Nearly 40 % of children and a third of nonsmoking adults worldwide were exposed to secondhand smoke in 2004 (Öberg et al. 2011). Each year, 600,000 individuals die from secondhand smoke, and 75 % of these deaths occur among women and children (Öberg et al. 2011). In China, approximately 95 % of women do not smoke and are more likely to die from chronic exposure to secondhand smoke from their spouses or workplaces than they are to die from active smoking themselves (Gan et al. 2007). Deaths caused by exposure to secondhand smoke are involuntary and entirely preventable, and tobacco control measures should be taken to protect nonsmokers from “forced smoking” and prevent these needless deaths
Global Types of Tobacco
Snus is less dangerous than cigarettes, for sure, but it is very hard to find anything more dangerous than cigarettes … [T]here is no natural law that says 30 percent of the population should be nicotine addicts. Goran Pershagen, professor at Stockholm’s Karolinska Institute, 2007 (Hundley 2007)
Tobacco products and their use vary greatly around the world, with combusted cigarettes as the primary means for consuming nicotine. Smokeless tobacco, also commonly referred to as oral tobacco, is widely popular, especially in certain regions of the world.
Relatively new to the tobacco market are novel nicotine products. New products are emerging regularly, particularly from the tobacco industry under the guise of reducing health risks, and this will only increase the variation in the number and type of nicotine products available to consumers. The result of novel nicotine products might mean that individuals use new products, such as snus, nicotine lozenges, dissolvables, and e-cigarettes, instead of traditional means of consuming tobacco, or they may use these novel products in addition to their traditional means of using tobacco, resulting in the dual use of tobacco products, and even higher levels of exposure to nicotine and other potentially harmful compounds.
Smoking Tobacco
Tobacco is most commonly consumed through the combustion of manufactured cigarettes, although cigars, pipes, waterpipes, kreteks, and bidis are other common forms of smoking tobacco. Through combustion, tobacco leaves are burned at high temperatures and the smoke is then inhaled. This method is the most efficient way for the brain to receive nicotine, and nearly six trillion cigarettes are manufactured and consumed annually, with the highest consumption occurring in high- and middle-income countries (ERC 2010). Manufactured cigarettes contain more than 7,000 ingredients and additives, approximately 69 of which are proven to cause cancer (USDHS 2012). While manufactured cigarettes are the most popular tobacco product worldwide, other smoking tobacco products dominate in various regions. For example, bidis, which are created by hand rolling tobacco in a temburni leaf, are the most heavily consumed smoked tobacco product in India, accounting for more than 80 % of the country’s tobacco market (Gilmore 2012). Kreteks, or clove cigarettes with exotic flavorings, dominate the tobacco market in Indonesia. Hookah, or water pipes through which tobacco is smoked, is most common in North Africa, the Mediterranean, and parts of Asia, but its popularity is spreading worldwide.
Smokeless Tobacco
Smokeless tobacco is a nonhomogenous group of tobacco-containing products that are primarily used orally, but sometimes used nasally. Globally, smokeless tobacco products/preparations range from those containing only cured tobacco to complex products including a range of chemical ingredients (sweetener, flavorings, moisteners, alkaline agents, etc.) and, in some cases, nontobacco plant material (betel leaf, areca nut, tonka bean, etc.) (IARC 2004, 2007b; Stanfill and Stepanov in press; Stanfill et al. 2011). In terms of form and consistency, smokeless tobacco are available in a variety of forms, including, but not limited to, ground tobacco, dry tobacco, twisted tobacco leaves, loose tobacco, tars, pastes, tobacco-containing chewing gum, dissolvable tablets, pressed cakes, pellets, powders, and mixtures of tobacco with other materials (IARC 2004, 2007b; SCENIHR 2008). Some products are manufactured, but many are hand-prepared for sale or personal use. In all there are approximately 35 distinct product/preparation types documented to date and the number continues to grow as new ones, many from remote areas, are characterized (Stanfill et al. 2011; IARC 2004, 2007b; SCENIHR 2008). Key ingredients, which impact addictiveness and toxicity among various smokeless tobacco products, include tobacco (can vary in type and species), alkaline agents (that boost free nicotine levels), areca nut (a known carcinogen) and other plant materials that can add additional toxicants.
The prevalence of smokeless tobacco varies by region. Approximately 8.1 million individuals in the USA and 258 million individuals in Southeast Asia use oral tobacco (Stanfill et al. 2011). In a recent global study of 53 products from nine countries, it was found that total nicotine concentrations in smokeless tobacco products varied from 0.16 to 34.1 mg/g (Stanfill et al. 2011). Even higher total nicotine concentrations (up to 95 mg/g) have been reported in nass from Uzbekistan (Brunnemann et al. 1985). By comparison, cigarettes contain approximately13.9 mg per cigarette and smokers ultimately absorb 1–2 mg per cigarette (Connolly et al. 2007; ACS 2011). Over 30 carcinogens, including the potent tobacco-specific N-nitrosamines, are found in various oral tobacco products, and the carcinogenic content varies by product and region (IARC 2004, 2007b; SCENIHR 2008; Stanfill et al. 2011).
Novel Nicotine Products
Novel nicotine products are being created by tobacco companies and entrepreneurs in an effort to keep individuals addicted to nicotine, and to possibly reduce the toxic exposure and disease that occurs from traditional cigarette and oral tobacco use. New products that have been created by the tobacco industry include noncombustible cigarettes (e.g., Eclipse, Accord, Premier) and oral tobacco or dissolvables (e.g., lozenges, strips, snus, sticks, orbs). In 2012, Altria Group, the parent company of Philip Morris USA, decided to test market a new disc-like product that does not contain tobacco. The product, Verve, is made from a polymer, nontobacco cellulose fibers with mint flavoring and nicotine (Blackwell 2012). In 2010, 10 % of British American Tobacco’s sales came from new products, and almost half of those products were not available the year before (Gilmore 2012). Tobacco companies are expanding product lines and interests in order to maintain their status as the primary means for people to receive nicotine.
Entrepreneurs have entered the nicotine and tobacco market with products such as nicotine water, gels, wafers, candy, inhalers, and electronic nicotine delivery systems (ENDS), such as e-cigarettes. ENDS first appeared in 2004 and have grown significantly in popularity since that time. Creators of e-cigarettes believe they are effective at delivering nicotine and are more acceptable than regular cigarettes, and thus should be used as a replacement product for cigarettes (Henningield and Zaatari 2010). Tobacco companies are becoming more involved in new tobacco products and technology, causing the tobacco markets to converge. In 2011 Philip Morris International bought patent rights to a technology that delivers nicotine-infused aerosol (Kesmodel and Korn 2011). In 2012 Lorillard acquired Blu Cigs, an electronic cigarette company, allowing Lorillard to enter the e-cigarette market previously held by entrepreneurs (Lorillard 2012).
Novel nicotine products, sold by both tobacco companies and entrepreneurs, are largely unregulated and the risks associated with their use are mostly unknown. While some products are defined as “potential reduced-exposure products” (PREPS), there is little research about these products and a 2001 U.S. Institute of Medicine report noted that the public health impact of PREPS is unknown, acknowledging that these products could potentially have an overall negative effect on population health (Stratton et al. 2001). The use of novel nicotine products is concerning as it might result in dual use (usage of cigarettes and other nicotine products) and could ultimately mean individuals are exposed to higher levels of nicotine than when smoking cigarettes alone. Additionally, the use of novel nicotine products could mean individuals use alternate products rather than quitting nicotine altogether. The 2012 U.S. Surgeon General Report on tobacco and youth notes that one-third of female high school students and one-half of male high school students used more than one tobacco product, making this age group a target for the dual use of tobacco products (US DHHS 2012). While tobacco products vary worldwide, the emerging novel nicotine delivery systems will increase this variation while potentially leading to new addiction and health issues.
As outlined, there is a proliferation of novel nicotine delivery products on the market. The gradual movement away from combusted products, particularly in developed countries, has major implications for global tobacco use and the fundamental issue of nicotine addiction. When and if nicotine can be delivered safely, we must ask ourselves if it is sound public policy to allow for widespread nicotine addiction from the many products now available. There are many health, social, and economic implications of nicotine addiction, and due to the novelty of these products, the full impact of novel nicotine use and addiction is not yet known.
Prevalence of Cigarette Use
Nobody should cry because of lower consumption of a product that kills half the people who use it. Danny McGoldrick, Vice President of research at the Campaign for Tobacco-Free Kids, 2007 (Cauchon 2007)
In most high-income countries, men and women smoke at roughly the same rates, although men smoke slightly more than women. However, in many parts of the world, particularly in emerging markets, it is not uncommon for men to smoke ten times more than women (Eriksen et al. 2012). Worldwide, there are one billion adult smokers, equaling nearly 20 % of the world’s adult population (Eriksen et al. 2012). Several high-income countries and regions have documented declining daily smoking rates for males and females combined (see Table 8.2) (Australian Institute of Health and Welfare 2011; Centers for Disease Control and Prevention 2011a; Health Canada 2011; Mercado 2011; Ministry of Health, Singapore 2010; Organization for Economic Co-Operation and Development 2011a, b). These declining rates show that tobacco control measures are effective and that it is feasible to expect and work towards daily smoking rates in the single digits.
Tobacco Epidemic
Over the course of a century, smoking patterns and the resultant disease, reflects an epidemic curve, with a rapid onset, plateau, and a more gradual decline. While smoking is often referred to in “epidemic” terms when considering the long view (over the course of a century), in the short term, smoking can be viewed as being “endemic” in that it is a risk factor that is present in every country of the world and that changes in smoking rates occur rather slowly. The global tobacco problem, as documented in high-income populations, plays out over the course of a century and can be segmented into four stages: the beginning of the epidemic, the significant increase in smoking prevalence, a decline in smoking prevalence, and then several decades later a spike in smoking-related illnesses and diseases (Lopez et al. 1994; Thun et al. 2012). In general, countries in stage one have smokers who are wealthy, educated, and referred to as “innovators.” While these individuals tend to quit sooner, their behavior is imitated by individuals in lower education and income groups. These individuals are more likely to continue the habit, have a harder time quitting, and have fewer resources available for dealing with the harm caused by smoking. Although countries may have similar smoking prevalence rates, each country’s stage in the tobacco epidemic is important. For example, two countries may have the same smoking prevalence rate, but the two countries may be in different stages of the epidemic. One country may be in the early stages of the epidemic and experience different challenges, with increased smoking rates and the morbidity and mortality that results from tobacco use still yet to come. Another country in the latter stages, may have already experienced the peaking of smoking rates and is still confronted with the morbidity and mortality resulting from tobacco use.
Adult Male Prevalence
Almost 800 million men throughout the world smoke cigarettes, and over 80 % of these smokers live in low- and middle-income countries (Eriksen et al. 2012; WHO 2011h). The 2010 weighted average of smoking prevalence among males in high-income countries is 30 %, 34 % in middle-income countries, and 21 % in low-income countries (Eriksen et al. 2012).Footnote 3 The smoking prevalence rate for men in most high-income countries has leveled out and in some cases is decreasing (Thun et al. 2012). Smoking prevalence rates for men in middle- and low-income countries vary, but these rates are typically increasing and have not yet reached a plateau. Among adults, men generally smoke more than women, and there are nearly 50 countries where men’s smoking rates are at least ten times as high as women’s smoking rates (Eriksen et al. 2012).
Adult Female Prevalence
Nearly 200 million adult women throughout the world smoke cigarettes (Eriksen et al. 2012). Over the past few decades, the highest female smoking rates have been concentrated in high-income countries, and half of the world’s female smokers live in these countries (Eriksen et al. 2012; WHO 2011h). The 2010 weighted average of smoking prevalence among women in high-income countries is 19 %, 5 % in middle-income countries and 3 % in low-income countries (Eriksen et al. 2012).Footnote 4 The female smoking rates in many high-income countries are nearly equal with male smoking rates, and there are two countries (Nauru and Sweden) where women smoke more than men (Thun et al. 2012; Swedish National Institute of Public Health 2009; WHO 2011h). The lower prevalence rates among females in middle- and low-income countries demonstrate the potential for female smoking rates to skyrocket in these areas. Changes in women’s rights, economics, cultural norms, and political influence may result in increased smoking rates among women in middle- and low-income countries (Thun et al. 2012). If these rates increase to meet the rates of male smokers, a public health catastrophe would occur that will lead to decades of future illness, an increase in noncommunicable diseases, and ultimately an increase in tobacco-related mortality.
Youth Prevalence
While smoking rates among adult males and females vary greatly, there is less variance in rates among boys and girls between the ages of 13–15. The smoking rates among boys and girls differ by less than 5 percentage points in almost half of the world’s countries, and there are at least 25 countries where girls smoke more than boys (see Table 8.3) (CDC 2011b, c). It is unclear if current youth smoking patterns among girls will lead to more adult female smokers. But it is clear that if this pattern continues, there will be an increase in female tobacco-related illness and disease. The vast majority of smokers begin the habit during their youth, and tobacco companies have long viewed youth as a target market for their products. A 1984 document from R.J. Reynolds noted that “younger adults are the only source of replacement smokers” (Reynolds 1984). Tobacco control measures need to be implemented that curb youth smoking rates and prevent youth uptake of tobacco while regulating the tobacco industry from marketing to youth. Only these actions can save future generations from tobacco-related illness and death.
Smoking and Social Factors
While tobacco use is a behavioral risk factor for illness and disease, many social factors influence tobacco use. There is a direct correlation between income level and education (Riordan 2012). In the USA in 2010, 28.9 % of adult smokers were living below the poverty level compared to 18.3 % of adult smokers who were living at or above the poverty level (CDC 2011d). In terms of the correlation between education and smoking, 25.1 % of adults who did not graduate from high school smoked, 9.9 % of adults who had a college degree smoked and 6.3 % of adults with a graduate degree smoked (CDC 2011d). These statistics support the idea that increased education and income levels are associated with lower smoking rates. The tie between smoking and social factors, such as education and income, is true in high-income countries, demonstrated by the above examples from the USA, but these patterns also prove true in some middle- and low-income countries as well. A cross-national sample of 50 low-, middle-, and high-income countries found that increased education was linked to lower smoking rates in males and that males working in nonmanual positions were less likely to smoke than those in agricultural or manual work positions (Pampel and Denney 2011). The results of the study indicate that social and economic patterns of cigarette use among individuals in low- and middle-income countries seems to follow the same patterns previously seen in high-income countries and that increased smoking prevalence in low- and middle-income countries will widen the disparities in smoking-related mortality in these countries (Pampel and Denney 2011). Due to tobacco’s tie with social factors, certain subpopulations are disproportionately impacted by tobacco. In the USA, minority populations are more at-risk for lower educational attainment and income, and these populations often smoke at higher rates and maintain the habit over time, exacerbating existing health disparities. In addition to racial and ethnic groups, other U.S. populations that experience higher smoking rates are the mentally ill, single-mothers, the homeless, and the long-term unemployed (David et al. 2010).
Global Tobacco Industry
Tobacco use is unlike other threats to global health. Infectious diseases do not employ multinational public relations firms. There are no front groups to promote the spread of cholera. Mosquitoes have no lobbyists. Report on the Committee of Experts on Tobacco Industry Documents (Zeltner Report), 2000
Economics
Smoking has strong business and economic dimensions, and in general, the tobacco industry acts in a collusive manner with the ultimate goal to benefit the companies, irrespective of the harm caused to its customers. The tobacco industry is dominated by six main tobacco manufacturers who market, manufacture, and politic in a similar manner. In 2010, the value of the global tobacco market was around half a trillion dollars,Footnote 5 similar to the gross domestic product of Poland and Sweden (ERC 2010; Euromonitor 2011; The World Bank 2011). The top six cigarette companies include China National Tobacco Corporation, Philip Morris International, Japan Tobacco Company, British American Tobacco, Imperial Tobacco and Altria/Philip Morris USA. In 2010, the combined revenue of these six companies was $346.2 billion and their combined profit totaled $35.1 billion, which was equal to the combined profits of Coca-Cola, Microsoft, and McDonald’s in the same year (see Table 8.4) (Altria 2010; British American Tobacco 2010; Businessweek 2010a, b, c; Imperial Tobacco 2010; Japan Tobacco 2010; Philip Morris International 2010; Wang 2011).
China National Tobacco Corporation (CNTC), the largest tobacco company in the world, is a state-owned monopoly. Therefore, tobacco control in China is balanced between the economic benefits from government production and sale of tobacco, the collection of taxes from tobacco sales on one hand, and the health of the public on the other. China leads the world in tobacco production, farming, and consumption. In 2008, China manufactured more than two trillion of the world’s six trillion cigarettes (ERC 2010). The country grew 43 % of the world’s tobacco in 2009, more than the other top nine tobacco-consuming countries combined (FAO 2009b). China also leads the world in cigarette consumption, with more than a third of the world’s cigarettes being smoked by Chinese men (ERC 2010). In 2011 the tobacco industry in China contributed approximately 8 % of the central government’s revenue (Netscribes 2012). China’s statistics related to population size, smoking prevalence, and the industry’s size and influence makes this country central to the topic of global tobacco.
Tobacco Marketing
Tobacco companies have long used marketing techniques to advance their products, and the first U.S. tobacco advertisement, which promoted snuff, ran in 1789 by the company now known as Lorillard Tobacco (James 2009). The tobacco industry claims that the goal of its tobacco advertising is to encourage adult smokers to switch brands or maintain their current brand status. In fact, tobacco advertising is often aimed at securing new consumers, especially youth. The 2012 U.S. Surgeon General’s report on youth smoking found that the “evidence is sufficient to conclude that there is a causal relationship between advertising and promotional efforts of the tobacco companies and the initiation and progression of tobacco use among young people” (US DHHS 2012, p. 6). In 2010, tobacco companies in the USA spent $8.05 billion marketing cigarettes and an additional $444 million marketing smokeless tobacco (FTC 2012a, b). Over $23 million is spent each day in the U.S. by tobacco companies on cigarette and smokeless tobacco advertising and promotions (FTC 2012a, b). Cigarette marketing is 48 % higher and smokeless tobacco marketing is 277 % higher than it was in 1998, the year of the U.S. Master Settlement Agreement (US DHHS 2012). Tobacco companies focus their advertising spending on price discounts, coupons, and retail-value added promotions (such as buy-one get-one free offers), effectively lowering the cost of smoking to the consumer. These cost-reduction promotions account for 81 % of cigarette marketing expenditures in the U.S. (FTC 2012a).
Despite increasing marketing restrictions, tobacco companies promote their products in any manner possible, and this practice occurs globally. In advance of a proposed Health Ministry ban on marketing cigarettes in Russia, cigarette company Donskoy Tabak introduced an advertisement of a female teen licking an ice cream cone. The caption read “If you’re not allowed it, but you really want it, then you can have it” (see Fig. 8.3) (Okorokova 2011). When Cambodia banned tobacco advertising and sponsorship in 2011, tobacco company Korean Tobacco & Ginseng (KT&G) changed its name to Korean Tomorrow & Global, likely in an effort to allow the company to keep its recognized initials and tobacco association without violating advertising regulations (Kong and Assunta 2012). Shanghai Tobacco Company created a specialty brand of cigarettes called “Love China” and displayed the text on generic billboards supposedly to promote patriotism and love of country, but that in effect, were bypassing marketing restrictions and advertising a specific cigarette brand (see Fig. 8.4) (Live China 2011). As technology and social media progress, tobacco companies are utilizing new media options for brand placement and promotion (James 2009). It is essential that tobacco control advocates understand the changing influence and role of new media technology, use it to their advantage and learn how tobacco companies are and could use new media to circumvent marketing restrictions.

Russian example of current tobacco advertising. Reproduced with permission. Credit: Katarina Radovic

“Love China” picture. Reproduced with permission. Credit: Michael Eriksen
Undue Influence
Tobacco companies spend millions of dollars annually to influence politics, legislation and business, and this practice is common worldwide. The undue influence of these companies occurs through direct political influence, legislative action, indirect influence, and corporate social responsibility (e.g., charitable giving among other activities). In 2010 in the USA, 168 lobbyists were employed by companies with tobacco interests, and a total of $16.6 million was spent directly on influencing U.S. political decisions (Opensecrets.org 2011). Tobacco companies commonly use legislation as a tool to protect their products. A recent and monumental example is the court action British American Tobacco, Philip Morris, Imperial, and Japan Tobacco brought against the Australian government when it passed plain packaging laws in 2011. Indirect influence occurs through partnerships the tobacco industry has made with organizations such as convenience store owners, advertising associations, and farmers’ associations. Additionally, tobacco companies commonly fund front groups who in turn promote the agendas of the tobacco companies. Corporate social responsibility includes charitable donations that conveniently promote the image of tobacco companies. For example, China National Tobacco Corporation has sponsored more than 60 elementary schools, and pro-tobacco messages, such as “Genius comes from hard work/ Tobacco helps you to be successful” are posted on the school grounds (NTD Television 2010). Tobacco companies work to maintain their image and client base, and this is done through both obvious and more covert measures.
Growing Tobacco
Tobacco is grown in at least 124 of the world’s countries on 4.2 million hectares of agricultural land (FAO 2013a; Australian Institute of Health and Welfare 2011). In 2009, 7.5 million tonnes of tobacco were produced globally (FAO 2013a, b). Most tobacco is grown in low- and middle-income countries, and growing tobacco contributes to a cycle of poverty for farmers and laborers. Farmers are required to purchase infrastructure and equipment from tobacco companies, often going into debt, with little or no profit remaining. Tobacco workers are exposed to pesticides and nicotine which result in neurological damage and green tobacco sickness (WHO 2004). Additionally, land used to grow tobacco cannot be used for growing other food, which can contribute to undernourishment in countries already experiencing food and hunger problems. For example, Malawi is a top tobacco producing country with an undernourishment rate of 27 %. In 2008, Malawi grew 1 tonne of tobacco per hectare, but could have grown 14.6 tonnes of potatoes on the same hectare of land (FAO 2008a, b, c; FAO 2011a, b).
Global Tobacco Control
Defendants have marketed and sold their lethal products with zeal, with deception, with a single-minded focus on their financial success, and without regard for the human tragedy or social costs that success exacted. U.S. District Judge Gladys Kessler’s Final Opinion: Summary of Findings Against the Tobacco Industry, August 2006
WHO Framework Convention on Tobacco Control and Global Resources
While a thorough discussion of global tobacco control is beyond the scope of this chapter, there are several resources and interventions aimed at global tobacco control. The World Health Organization’s Framework Convention on Tobacco Control (WHO FCTC) provides an evidence-based treaty that addresses the global tobacco epidemic (WHO 2011e). The treaty is one of the most rapidly embraced treaties with 176 parties as of 2013 (WHO 2012b). Additionally, mounting global resources and dedication to the topic of tobacco control is of paramount importance. Since 2006, Michael Bloomberg, philanthropist and Mayor of New York City, has pledged a total of $600 million for global tobacco projects, primarily focused on low- and middle-income countries. This former smoker turned tobacco control advocate, made his most recent pledge of an additional $220 million at the 15th World Conference on Tobacco OR Health in March 2012 in Singapore (Lopatto 2012). Bloomberg’s contributions, combined with the efforts of the Bill & Melinda Gates Foundation, lend a combined $725 million in global tobacco control. This monumental support leads the way for further attention and resources for global tobacco control efforts.
Legal Challenges and Litigation
Under the U.S. Master Settlement Agreement of 1998, seven major tobacco companies agreed to pay 46 States approximately $206 billion in revenue over a 25-year period. The tobacco companies also agreed to change their marketing strategies, open previously closed documents, and finance a multi-billion anti-smoking campaign (National Association of Attorneys General 1998). While the lawsuit was intended to prevent youth smoking and reimburse states for healthcare costs of smokers, the agreement did not mandate that revenues be dedicated to tobacco prevention or cessation initiatives (National Association of Attorneys General 1998). The CDC Best Practices for Comprehensive Tobacco Control recommended in 2007 that the States spend a combined total of $3.7 billion annually on evidence-based state tobacco control programs (CDC 2007). In 2010, the total state and federal expenditures for tobacco control totaled $641.1 million (CDC 2012). In addition to the payments from the Master Settlement Agreement, states also collect excise taxes on cigarette sales, totaling almost $24 billion combined for all states in 2010 (CDC 2012). In contrast, in 2010 the states spent only 2.4 % of total state tobacco revenues on tobacco control programs (CDC 2012).
Other countries have launched law suits against tobacco companies in an effort to recover healthcare costs for smokers. In mid-2012, Quebec launched a $60 billion lawsuit against tobacco companies, joining the ranks of four other Canadian Provinces (Ontario, British Columbia, New Brunswick, and Newfoundland). Quebec’s lawsuit is significant in that it means half of the country’s provinces have now sued the tobacco industry, and Quebec’s $60 billion in reparations is the highest amount being sought in damages by any of the provinces that have sued thus far (The Canadian Press 2012).
Industry Accountability
In furthering global tobacco control, the tobacco industry must be held accountable for the damage and harm their products cause worldwide. This requires increased discovery into the industry and their inner workings. This can occur, in part, through further mandates for the release and disclosure of industry documents and methodology. Individuals must learn firsthand how the tobacco industry employs manipulation to further their own gain. With this knowledge, it will hopefully no longer be socially acceptable to support tobacco companies, their products, or initiatives.
Cessation Interventions
Tobacco control initiatives vary globally, and interventions such as those outlined in the WHO FCTC may need to be implemented differently depending on each country’s prevalence of tobacco use, types of tobacco used, and social norms. Despite the variability in countries, some tobacco control methods are universal, such as the use of tobacco taxes and quitlines. Economics have shown that as price increases, consumption decreases. While this varies slightly depending on the elasticity of products, it has been shown globally that increased tobacco taxes result in decreased consumption (Chaloupka et al. 2012). Easily accessible and free quitlines are an effective tobacco cessation method, yet slightly more than a quarter of the world’s countries have quitlines available (WHO 2011h). Other aspects of tobacco-control, such as cessation interventions, vary globally. For example, pharmacologic products have been successful in assisting in cessation among smokers in the U.S., and approximately half of all smokers attempt quitting each year (Zhu et al. 2012). Other countries, such as China, will benefit more from population-based interventions that build self-efficacy and demonstrate the feasibility of quitting.
Graphic Warning Labels and Plain Packaging
Graphic health warnings were first introduced on cigarette packages by Canada in 2000. As of early 2012, at least 49 countries have graphic warning labels and approximately 30 countries and jurisdictions met the WHO FCTC criteria of graphic warning labels covering at least 30 % of the package (Campaign for Tobacco-Free Kids 2011; Physicians for a Smoke-Free Canada 2012). The effectiveness of warning labels must be apparent to tobacco companies as they have sued countries implementing these policies, and in the case of New Zealand, have found ways to counter the warning labels, such as including adhesive seals or stickers in their Dunhill cigarettes. The stickers, which read “exclusively Dunhill,” conveniently can be placed to cover the majority of the pack’s warning labels (Simpson 2012).
Australia led the world in 2011 by passing the first plain packaging legislation and requiring that all cigarettes be sold in plain, brown packages starting in December 2012 (Parliament of Australia 2011). The goal of plain packaging is to decrease the appeal of tobacco products to consumers, primarily to youth, to increase the effectiveness and noticeability of the health warnings, to decrease the ability of packaging to mislead consumers, and to ultimately help curb smoking rates (Australian Government Department of Health and Ageing 2011). Despite Big Tobacco’s claims that plain packaging will not work, four major tobacco companies have mounted law suits against the Australian government, thus indicating their concern over the possible impacts of plain packaging. Additionally, Honduras and Ukraine have filed complaints with the World Trade Organization (WTO) citing that plain packaging violates trade agreements, and it is likely that the plain packaging debate will be decided by the WTO (Miles 2012). The world is anxiously watching and anticipating the results of this strong tobacco control law and its potential impact on cigarette users and tobacco companies.
Changing Social Norms
In order to further tobacco control, global advocates must continue to change social norms in a manner similar to what has occurred with secondhand smoke in developed countries (see Fig. 8.5). At its most basic level, smoking creates secondhand smoke, which harms those forced to breathe it. This involuntary exposure on those who have chosen not to smoke is a “negative externality” and has resulted in unprecedented citizen mobilization and action in many high-income countries. The harm and annoyance caused by involuntary exposure and the resultant mobilization for action was confirmed and validated through research and reports, such as the Surgeon General Reports in the U.S. Once sufficient evidence was gathered and accepted, individuals demanded social action and protection from secondhand smoke. As social norms changed, public smoking became unacceptable and ultimately smoking was seen as a “deviant” behavior. Once the social norm changed, the government and institutions began to change their rules and policies to comply with the social norm and to protect nonsmokers from negative externalities. A 2006 study found that increased social unacceptability of smoking is nearly as effective at reducing cigarette consumption as increasing tobacco taxes. The study found that if the social unacceptability of smoking in the USA increased by 40 %, there would be a 15 % decrease in consumption. This decrease in consumption could also be achieved by a tax increase of $1.17 per pack, indicating the effectiveness of changing social norms in order to decrease tobacco consumption (Alamar and Glantz 2006). This process of changing social norms that has occurred first in developed countries must be replicated throughout the world so that changes in the social unacceptability of smoking is accelerated and that citizens demand policies and regulations that protect them from the harm caused by involuntary exposure to secondhand smoke.

Process of social change. Permission not needed
Tobacco Control as a Lesson for Other Risk Factors
Tobacco control has been one of the central focuses of public health for the past few decades, resulting in evidence-based guidelines, interventions, and frameworks. Many of the tobacco control measures, such as price increases, marketing restrictions, changes in labeling and product information have implications for the other risk factors of unhealthy diets, physical inactivity, and alcohol use. The topic of how tobacco control lessons relate to unhealthy diets, and particularly preventing childhood obesity are outlined as an example of this relationship between tobacco control and other NCDs. Some of these lessons may also be relevant to the risk factors of physical inactivity and alcohol use, but are not explored in detail in this chapter.
Comparison of Risk Factors: Tobacco and Unhealthy Diets
There are many similarities, but also differences, in reducing tobacco use and improving dietary behavior. The most important difference is that food is necessary for survival and tobacco is completely unnecessary. Another difference lies in the fact that the tobacco industry, with their subversive advertising, manipulation, deception, and secrets, is a significant part of the tobacco control problem. On the other hand, the food industry has the potential to be a part of the obesity solution, although whether they will be so or not has yet to be determined.
The lessons learned through tobacco control about product and ingredient labeling can be successfully applied to preventing unhealthy diets. In terms of product and ingredient labeling, the tobacco industry attempted to mislead consumers by marketing products as “light” or “low tar.” These terms led consumers to mistakenly believe that using these products was a “healthier” choice than smoking regular cigarettes, but this is not the case and consumers of these products experience the same negative health effects as those who smoke regular cigarettes. Similarly, product labeling on food and drinks can be confusing and misleading, as it is relatively unregulated and the industry and companies can choose how to label products and what information to include on front-of-label packaging (Brownell and Koplan 2011). An example of a confusing aspect of the U.S. nutrition labeling system is the fact that information is presented on one serving, yet often a bag of chips or soft drink contain multiple servings and consumers may not notice the serving information and recognize the full amount of calories and fat that are being consumed (Lyn et al. 2012). Food products can benefit from more intuitive and consistent labeling that will help consumers make informed choices. The U.S. Food and Drug Administration announced in 2009 that it will make recommendations that manufacturers must meet for front-of-package labeling and shelf labels, and since this announcement two major food-industry trade associations have formed an industry-created front-of-package labeling system called “Nutrition Keys.” (US DHHS 2009; Brownell and Koplan 2011). Some grocery store chains have implemented their own point-of-purchase labels, such as the Guiding Stars program found in a grocery store chain in the northeastern part of the U.S. This three-tiered star icon is placed on shelves and rates food and beverage products. The clear and simple message of the stars appears to be effective in changing food purchases among consumers (Sutherland et al. 2010). The United Kingdom and Australia have considered traffic-light labeling that uses the colors red, yellow, and green to show which nutrients in the food should be consumed in low, medium, or high levels (Australian Medical Association 2011). In general, front-of-label packaging and nutrition labels should be based on research and science and should be presented in a clear, easy to understand, and consistent method.
Both food consumption and tobacco consumption are influenced by marketing, and the lessons learned from tobacco control can be applied to help prevent obesity. The goal of marketing is to promote, sell, or distribute a particular service or product, and thus tobacco and food marketing aims at getting consumers to purchase particular tobacco or food products, and hopefully become returning customers. The tobacco industry has taken marketing to an extreme and has successfully managed to sell a product that kills half of all long-term users (WHO 2011d). Tobacco marketing is aimed at getting new smokers, maintaining brand loyalty, and convincing other smokers to switch. Tobacco marketing takes place through advertisements, social media, sponsorships, promotions, give-aways, and discounts. Youth are particularly influenced by tobacco marketing and therefore the WHO FCTC has proposed global tobacco marketing bans and restrictions. Food marketing occurs through similar channels as tobacco and business marketing. Consumers are inundated with brand names and messages through traditional media (e.g., mail, commercials, point-of-sale advertisements, billboards), social media, as well as promotions (e.g., coupons, sales, and giveaways). Youth are exposed to additional marketing at school through product placement in vending machines and specific brand foods in cafeterias (Lyn et al. 2012). Tobacco companies also utilize Corporate Social Responsibility (CSR) programs to further their image. For example, in 2010 Philip Morris International contributed $25 million in donations to global nonprofits and initiatives. In reality, this was less than 1 % of the company’s net profits of $7.5 billion, but it helped further their image and name recognition (Philip Morris International 2011). A comparison has been drawn between the use of CSR by big tobacco and the soda industry. Since sugary beverages are often implicated in the global tobacco crisis, beverage companies have launched extensive CSR campaigns (Dorman et al. 2012). Like the CSR campaigns of big tobacco, the soda industry focuses their campaigns on individual responsibility and choice, increasing product popularity, and preventing regulation (Dorman et al. 2012). A unique difference between the CSR campaigns of big tobacco and the soda industry is that the soda industry can openly focus on young audiences and they initiated their campaigns quickly following the backlash about soda’s contribution to the obesity epidemic (Dorman et al. 2012).
While the tobacco control movement can provide a helpful model for obesity prevention, there are several important differences between the prevention models for these two risk factors. For example, the global tobacco control model focuses on population-based initiatives to curb smoking and deter new smokers. Alternatively, obesity programs often focus on individual-level interventions and programs. Tobacco has proven to be a price-sensitive commodity and price increases result in decreased consumption. It is unclear how taxation of certain food products will impact consumers, and there is some concern that low-income groups could be disproportionately affected (Lyn et al. 2012). While taxing food products is a somewhat new concept, several countries are taking the first steps to see if this is an effective method to prevent obesity. Some countries, such as Hungary, Denmark, and France have implemented “fat taxes” on unhealthy foods or sweetened drinks (Mytton et al. 2012). A 2012 study found that these types of taxes must be at 20 % or more of the food value to have an impact on consumption (Mytton et al. 2012). New York has proposed a ban on soft drinks that are 16 ounces or larger (CBS News 2012). While the New York ban is highly controversial and debated, a 2012 study found that a penny-per-ounce tax on sugar-sweetened beverages would be effective in reducing consumption of sugary beverages by 15 % among adults ages 25–64. If this tax were implemented during the study period (between 2010 and 2020), it would result in a savings of $17 billion in medical costs and would generate approximately $13 billion in annual tax revenue, indicating that taxing unhealthy products might be an effective method in curbing the obesity epidemic (Wang et al. 2012).
The above examples compare the tobacco control lessons to obesity prevention. Many of the lessons learned from tobacco control can also be applied to physical inactivity and alcohol consumption, although the research is less established in these areas. For example, a 2012 study found that a 25-cent per drink increase on alcohol would be effective at reducing excessive drinking (Stuckler et al. 2012; Daley et al. 2012). There is emerging research on the impact that global producers have on increasing the consumption of unhealthy foods, alcohol, and tobacco (Stuckler et al. 2012). Unhealthy diets, physical inactivity, and alcohol consumption, along with tobacco use, are risk factors for the world’s most damaging NCDs. The risk factor of tobacco use has been and continues to be addressed globally, and the other risk factors can be addressed using some aspects of the tobacco control model. All three risk factors can benefit from the global recognition and recommendations provided by overarching organizations. For example, the World Health Organization’s Framework Convention on Tobacco Control (WHO FCTC) is the world’s most rapidly embraced treaty that provides guidelines and recommendations for addressing tobacco-related issues. WHO offers guidelines and recommendations about diets, physical inactivity, and alcohol consumption through the WHO Global Strategy on Diet, Physical Activity and Health and through the WHO Global Strategy for Reducing the Harmful Use of Alcohol. A global health treaty, currently referred to as the Framework Convention on Global Health has been proposed by the Joint Action and Learning Initiative on National and Global Responsibilities for Health (JALI). The Framework Convention on Global Health has been endorsed by the UN Secretary-General, and this type of global framework would help improve global health and reduce inequalities (Gostin 2012). While these global strategies are not binding like the WHO FCTC is for those countries that have ratified it, they represent a global recognition of the importance of these risk factors, their influence on global health, and the need for unified and proven methods to address these risk factors.
Conclusion
We’ve come a long way, bullies. We will not be fazed by your harassment. Your products kill nearly 6 million people each year. You run a killing and intimidating industry, but not in a crush-proof box. Tobacco industry: the number and fortitude of your public health enemies will damage your health. Margaret Chan, Director-General of the World Health Organization at the World Conference on Tobacco OR Health, 2012
Tobacco and its use have evolved considerably over the past decades. Society has moved from a complete absence of understanding about the dangers of tobacco to a full awareness of the extent of harm it causes. Despite this knowledge, more than a billion adults still currently smoke cigarettes. It is now known that tobacco use results in morbidity and mortality, but that individuals can successfully quit this damaging addiction. The tobacco industry, which remains highly secretive, has finally been held partially accountable for their fraudulent and damaging ways. Smoking rates in many high-income countries have hit a plateau and some have even declined, but these countries have paid high direct and indirect costs for the tobacco-related illness and death they have and continue to experience. Unfortunately, the harm caused by today’s tobacco use will extend decades into the future as today’s smokers, especially young smokers, will undoubtedly develop tobacco-related illness and diseases (Thun et al. 2012). The world is at a unique juncture as high-income smoking rates have started to level out and global tobacco control is now in a position to prevent smoking rates (and thus illness and disease rates) in middle- and low-income countries, especially among women, from ever reaching the levels seen in high-income countries. Country leaders and tobacco control advocates must take seriously the possibility that female and youth smoking rates have the potential to increase, and all must do everything in their power to prevent further death from tobacco use. Tobacco needs to be treated commensurate with the harm it causes, and we must take drastic measures to stop tobacco use from killing one person every 6 seconds (WHO 2011d).
Notes
- 1.
Sufficient evidence indicates a strong suggestion of a causal relationship.
- 2.
Suggestive evidence suggests an indicative but not causal relationship.
- 3.
Data derived from the following sources: WHO Report on the Global Tobacco Control 2011, UN Population Estimates, World Bank Income Categorizations.
- 4.
Data derived from the following sources: WHO Report on the Global Tobacco Control 2011, UN Population Estimates, World Bank Income Categorizations.
- 5.
The value of the global tobacco market varies between $375 and $650 billion USD depending on where in the distribution channel (retail vs. manufacturing) the value is measured.
References
Adler, I. (1912). Primary malignant growths of the lungs and bronchi: A pathological and clinical study. London: Longmans, Green and Co.
Alamar, B., & Glantz, S. A. (2006). Effect of increased social unacceptability of cigarette smoking on reduction in cigarette consumption. American Journal of Public Health, 96(8), 1359–1363.
Altria Group Inc. (2010). 2010 annual report. Retrieved August 9, 2011, from http://investor.altria.com/phoenix.zhtml?c=808.
American Cancer Society. (2011). Learn about cancer: Cigarette smoking. Retrieved July 3, 2012, from http://www.cancer.org/Cancer/CancerCauses/TobaccoCancer/CigaretteSmoking/cigarette-smoking-tobacco.
American Cancer Society. (2012). Cancer facts & figures 2012. Atlanta, GA: American Cancer Society. Retrieved March 27, 2012, from http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-031941.pdf.
Australian Government Department of Health and Ageing. (2011). Public consultation on plain packaging of cigarettes. Retrieved 29 March, 2012, from http://www.yourhealth.gov.au/internet/yourhealth/publishing.nsf/Content/plainpack-tobacco#.T3RxzXnYEUg.
Australian Institute of Health and Welfare. (2011). 2010 National Drug Strategy Household Survey Report. Retrieved October 5, 2011, from http://www.aihw.gov.au/publication-detail/?id=32212254712.
Australian Medical Association. (2011, November 30). Traffic light food labelling. Retrieved July 3, 2012, from http://ama.com.au/traffic-light-labelling.
Blackwell, J. R. (2012, May 23). Altria to test market new nicotine product in Virginia. Richmond Times-Disptach. Retrieved July 3, 2012, from http://www2.timesdispatch.com/business/virginia-news/2012/may/23/tdbiz01-altria-to-test-market-new-nicotine-product-ar-1935376/.
British American Tobacco. (2010). Annual report 2010. Retrieved August 9, 2011, from http://www.bat.com/servlet/SPMerge?mainurl=%2Fgroup%2Fsites%2Fuk__3mnfen.nsf%2FvwPagesWebLive%2FDO52AK34%3Fopendocument%26amp%3BSKN%3D1.
Brownell, K. D., & Koplan, J. P. (2011). Front-of-package nutrition labeling—an abuse of trust by the food industry. The New England Journal of Medicine, 346(25), 2373–2375. Retrieved July 3, 2012, from http://www.nejm.org/doi/full/10.1056/NEJMp1101033.
Brunnemann, K. D., Genoble, L., & Hoffmann, D. (1985). N-Nitrosamines in chewing tobacco: An international comparison. Journal of Agricultural and Food History, 33, 1178–1181.
Businessweek. (2010a). McDonalds Corporation: 2010 financials. Retrieved August 9, 2011, from http://investing.businessweek.com/research/stocks/financials/financials.asp?ticker=MCD:US.
Businessweek. (2010b). Microsoft Corporation: 2010 financials. Retrieved August 9, 2011, from http://investing.businessweek.com/research/stocks/financials/financials.asp?ticker=MSFT:US.
Businessweek. (2010c). The Coca-Cola Company: 2010 financials. Retrieved August 9, 2011, from http://investing.businessweek.com/research/stocks/financials/financials.asp?ticker=KO:US.
Campaign for Tobacco-Free Kids. (2011). Pictoral warning labels by country and jurisdiction. Retrieved April 10, 2012, from http://global.tobaccofreekids.org/files/pdfs/en/WL_examples_en.pdf.
Cauchon, D. (2007). Smoking declines as taxes increase. USA Today. Retrieved April 12, 2012, from http://www.usatoday.com/news/health/2007-08-09-1Alede_N.htm.
CBS News. (2012, June 12). Mayor Bloomberg’s soda ban proposal to be submitted to NYC health board today. Retrieved June 30, 2012, from http://www.cbsnews.com/8301-504763_162-57451372-10391704/mayor-bloombergs-soda-ban-proposal-to-be-submitted-to-nyc-health-board-today/.
Centers for Disease Control and Prevention. (2007, October). Best Practices for Comprehensive Tobacco Control Programs—2007. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; Reprinted with corrections.
Centers for Disease Control and Prevention. (2011a). Current smoking, adults, early release. Retrieved November 2, 2011, from http://www.cdc.gov/nchs/data/nhis/earlyrelease/201106_08.pdf.
Centers for Disease Control and Prevention. (2011b). Global tobacco surveillance system: Global School-Based Health Survey. Retrieved October 15, 2011, from http://www.cdc.gov/gshs/andviapersonalcommunication.
Centers for Disease Control and Prevention. (2011c). Global tobacco surveillance system: Global Youth Tobacco Survey. Retrieved October 15, 2011, from http://nccd.cdc.gov/gtssdata/Ancillary/Documentation.aspx?SUID=1&DOCT=1 and via personal communication.
Centers for Disease Control and Prevention. (2011d). Vital signs: Current cigarette smoking among adults aged ≥ 18 years—United States, 2005–2010. Retrieved June 21, 2012, from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6035a5.htm?s_cid = mm6035a5_w.
Centers for Disease Control and Prevention. (2012). State tobacco revenues compared with tobacco control appropriations—United States, 1998–2010. Retrieved July 3, 2012, from http://www.cdc.gov/mmwr/pdf/wk/mm6120.pdf.
Chaloupka, F. J., Yurekli, A., & Fong, G. T. (2012). Tobacco taxes as a tobacco control strategy. Tobacco Control, 21(2), 172–180.
Chan, M. (2012). The changed face of the tobacco industry—Keynote address at the 15th World Conference on Tobacco OR Health. Retrieved April 12, 2012, from http://www.who.int/dg/speeches/2012/tobacco_20120320/en/.
Connolly, G. N., Alpert, H. R., Wayne, G. F., & Koh, H. (2007). Trends in smoke nicotine yield and relationship to design characteristics among popular U.S. cigarette brands 1975–2005. A report of the Tobacco Research Program, Division of Public Health Practice, Harvard School of Public Health. Retrieved July 3, 2012, from http://www.hsph.harvard.edu/nicotine/trends.pdf.
Daley, J. I., Stahre, M. A., Chaloupka, F. J., & Naimi, T. S. (2012). The impact of a 25-cent-per-drink alcohol tax increase. American Journal of Preventive Medicine, 42(4), 382–389.
David, A., Esson, K., Perucic, A., & Fitzpatrick, C. (2010). Tobacco use: Equity and social determinants. In E. Blas & A. S. Kurup (Eds.), Equity, social determinants and public health programmes (pp. 199–207). Geneva: World Health Organization.
Dorman, L., Cheyne, A., Friedman, L. C., Wadud, A., & Gottlieb, M. (2012). Soda and tobacco industry corporate social responsibility campaigns: How do they compare? PLoS Medicine, 9(6), e1001241. doi:10.1371/journal.pmed.1001241.
ERC. (2010). World cigarette reports 2010. Suffolk: ERC Group Ltd.
Eriksen, M., Mackay, J., & Ross, H. (2012). The tobacco atlas (4th ed.). Atlanta, GA: American Cancer Society.
Euromonitor International. (2011). Passport database. Retrieved October 1, 2011.
Ezzati, M., & Lopez, A. (2003). Estimates of global mortality attributable to smoking in 2000. The Lancet, 362, 847–852.
Federal Trade Commission. (2012a). Cigarette report for 2009 and 2010. Retrieved May 21, 2013, from http://www.ftc.gov/os/2012/09/120921cigarettereport.pdf.
Federal Trade Commission. (2012b). Smokeless tobacco report for 2009 and 2010. Retrieved May 21, 2013, from http://www.ftc.gov/os/2012/09/120921tobaccoreport.pdf.
Food and Agricultural Organization. (2008a). FAOSTAT data, tobacco unmanufactured: Area harvested, 2008. Retrieved April 1, 2011, from http://faostat.fao.org/site/567/DesktopDefault.aspx?PageID=567.
Food and Agricultural Organization. (2008b). FAOSTAT data, tobacco unmanufactured: Production quantity, 2008. Retrieved April 1, 2011, from http://faostat.fao.org/site/567/DesktopDefault.aspx?PageID = 567#ancor.
Food and Agricultural Organization. (2008c). FAOSTAT data, potatoes: Production quantity, 2008. Retrieved April 1, 2011, http://faostat.fao.org/site/567/DesktopDefault.aspx?PageID = 567#ancor.
Food and Agricultural Organization. (2011a). Hunger statistics: 2005–2007. Retrieved April 1, 2011, from http://www.fao.org/hunger/en/.
Food and Agricultural Organization. (2011b). Hunger map 2010: Prevalence of undernourishment in developing countries (2005–2007). Retrieved April 1, 2011, from http://faostat.fao.org/site/563/default.aspx.
Food and Agricultural Organization. (2013a). FAOSTAT data, tobacco unmanufactured: Area harvested, 2011. Retrieved May 21, 2013, from http://faostat.fao.org/site/567/DesktopDefault.aspx?PageID=567.
Food and Agricultural Organization. (2013b). FAOSTAT data, tobacco unmanufactured: Production quantity, 2011. Retrieved May 21, 2013, from http://faostat.fao.org/site/567/DesktopDefault.aspx?PageID=567.
Gan, Q., Smith, K., Hammond, K., & Hu, T. (2007). Disease burden of adult lung cancer and ischaemic heart disease from passive tobacco smoking in China. Tobacco Control, 16(6), 417–422.
Garfinkel, L. (1981). Time trends in lung cancer mortality among nonsmokers and a note on passive smoking. Journal of the National Cancer Institute, 66(6), 1061–1066.
Gilmore, A. B. (2012). Understanding the vector in order to plan effective tobacco control policies: An analysis of contemporary tobacco industry materials. Tobacco Control, 21(2), 119–126.
Gostin, L. O. (2012). A framework convention on global health: Health for All, Justice for All. Journal of the American Medical Association, 307(19), 2087–2092. doi:10.1001/jama.2012.4395.
Haire-Joshu, D., Glasgow, R. E., & Tibbs, T. L. (1999). Smoking and diabetes. Diabetes Care, 22(11), 887–1898.
Health Canada. (2011). Canadian Tobacco Use Monitoring Survey: Summary of annual results for 2010. Retrieved October 5, 2011, from http://www.hc-sc.gc.ca/hc-ps/tobac-tabac/research-recherche/stat/_ctums-esutc_2010/ann_summarysommaire-eng.php.
Henningield, J. E., & Zaatari, G. S. (2010). Electronic nicotine delivery systems: Emerging science foundation for policy. Tobacco Control, 19(2), 89–90.
Hirayama, T. (1981). Non-smoking wives of heavy smokers have a higher risk of lung cancer: A study from Japan. British Medical Journal (Clinical Research Ed.), 282(6259), 183–185.
Hundley, T. (2007, September 16). Snuffing out smokes. Chicago Tribune. Retrieved August 2, 2011, from http://articles.chicagotribune.com/2007-09-16/business/0709150068_1_snus-smokeless-tobacco-tobacco-product/2.
Hyland, A., Vena, C., Bauer, J., Li, Q., Giovino, G.A., Yang, J., et al. (2003). Cigarette smoking-attributable morbidity—United States, 2000. Morbidity and Mortality Weekly Review. Atlanta, GA: Centers for Disease Control and Prevention.
Imperial Tobacco. (2010). Annual report and accounts 2010. Retrieved August 9, 2011, from http://www.imperial-tobacco.com/files/financial/reports/ar2010/index.asp?pageid=64.
International Agency for Research on Cancer (IARC). (1986). IARC monographs on the evaluation of the carcinogenic risk of chemicals to humans: Tobacco smoking. IARC 38. Lyon, France: IARC press
International Agency for Research on Cancer (IARC). (2004). Monograph 85: Betel-quid and areca-nut chewing and some tobacco specific N-nitrosamines. Retrieved June 5, 2012, from http://monographs.iarc.fr/ENG/Monographs/vol85/index.php.
International Agency for Research on Cancer (IARC). (2007a). The hazards of smoking and the benefits of stopping: Cancer Mortality and overall mortality. IARC handbooks of cancer prevention (Vol. 11, pp. 15–27). Lyon: IARC press.
International Agency for Research on Cancer (IARC). (2007b). Smokeless tobacco and some tobacco-specific N-nitrosamines. In: IARC monographs on the evaluation of carcinogenic risks to humans (Vol. 890. Lyon, France. Retrieved June 5, 2012, from http://monographs.iarc.fr/ENG/Monographs/vol89/index.php.
James, R. (2009, June 15). Cigarette advertising. Time Magazine. Retrieved April 1, 2012, from http://www.time.com/time/magazine/article/0,9171,1905530,00.html.
Japan Tobacco Inc. (2010). Annual report 2010. Retrieved August 9, 2011, from http://www.jti.com/documents/annualreports/Annualreport2010.pdf.
Kesmodel, D., & Korn, M. (2011, May 27). Philip Morris Looks to Nicotine Aerosol. The Wall Street Journal. Retrieved June 21, 2011, http://online.wsj.com/article/SB10001424052702304066504576347513991162274.html.
Kessler, G. (2006). Final Opinion Civil Action No. 99-2496 (GK). United States District Court for the District of Columbia. Retrieved April 12, 2012, from http://www.tobaccofreekids.org/content/what_we_do/industry_watch/doj/FinalOpinion.pdf.
Kong, M., & Assunta, M. (2012). Worldwide news and comment—Cambodia: KT&G? ‘Korean Tomorrow & Global’, Of Course. Tobacco Control, 21(2), 82–86.
Live China. (2011, May 8). Chinese Love “China Love” Cigarettes. Retrieved July 3, 2012, from http://golivechina.com/newsitem/chinese-love-china-love-cigarettes/.
Lopatto, E. (2012, March 22). Mayor Bloomberg donates $220 million to fight smoking abroad. Bloomberg. Retrieved April 1, 2012, http://www.bloomberg.com/news/2012-03-22/mayor-bloomberg-donates-220-million-to-fight-smoking-overseas.html.
Lopez, A., Collishaw, N., & Piha, T. (1994). A descriptive model of the cigarette epidemic in developed countries. Tobacco Control, 3, 242–247.
Lorillard. (2012). Lorillard, Inc. Reports First Quarter 2012 Results and Acquisition of blu ecigs. Retrieved July 3, 2012, from http://investors.lorillard.com/phoenix.zhtml?c=134955%26p=irol-newsArticle%26ID=1687024%26highlight.
Lyn, R., Moore, B. J., & Eriksen, M. (2012). The application of public health lessons to stemming the obesity epidemic. In S. R. Akabas, S. A. Lederman, & B. J. Moore (Eds.), Textbook of obesity: Biological, psychological, and cultural influences (pp. 58–83). Chichester: John Wiley & Sons.
Mercado, S. (2011). World Health Organization: Western Pacific Region Office, Personal communication.
Miles, T. (2012). Honduras joins WTO complaint on Australia tobacco packaging. Retrieved April 11, 2012, from http://www.reuters.com/article/2012/04/04/wto-australia-tobacco-idUSL6E8F4BQC20120404.
Ministry of Health, Singapore. (2010). National Health Survey 2010, Singapore. Epidemiology and Disease Control Division, Ministry of Health, Singapore. Retrieved April 9, 2012, from http://www.moh.gov.sg/content/dam/moh_web/Publications/Reports/2011/NHS2010%20-%20low%20res.pdf.
Mytton, O. T., Clarke, D., & Rayner, M. (2012). Taxing unhealthy food and drinks to improve health. British Medical Journal, 344, e2931. Retrieved July 5, 2012, from http://www.bmj.com/content/344/bmj.e2931.
National Association of Attorneys General. (1998). Master settlement agreement. Retrieved July 10, 2012, from http://www.naag.org/backpages/naag/tobacco/msa/msa-pdf/MSA%20with%20Sig%20Pages%20and%20Exhibits.pdf.
National Research Council, Committee on Passive Smoking. (1986). Environmental tobacco smoke: Measuring exposures and assessing health effects. Washington, DC: The National Academies Press.
Netscribes. (2012, February). Tobacco market – China. Netscribes Food & Beverage Industry Series.
NTD Television. (January 26, 2010). Tobacco companies sponsor 69 elementary schools in China. Retrieved July 3, 2011, from. http://english.ntdtv.com/ntdtv_en/ns_china/2010-01-26/907134456872.html.
Öberg, M., Jaakkola, M., Woodward, A., Peruga, A., & Prüss-Ustün, A. (2011). Worldwide burden of disease from exposure to secondhand smoke: A retrospective analysis of data from 192 countries. The Lancet, 377, 139–146.
Okorokova, L. (2011, August 25). Teenage cigarette scandal. The Moscow News. Retrieved August 28, 2011, from http://themoscownews.com/society/20110825/188961025.html.
OpenSecrets.org. (2011). Tobacco. Retrieved July 28, 2011, from http://www.opensecrets.org/industries/lobbying.php?cycle = 2010%26ind = A02.
Organization for Economic Co-Operation and Development (OECD). (2011a). OECD health data 2011: Frequently requested data. Retrieved November 29, 2011, from http://www.oecd.org/document/16/0,3746,en_2649_37407_2085200_1_1_1_37407,00.html.
Organization for Economic Co-Operation and Development (OECD). (2011b). Stat extracts: Health status. Retrieved October 5, 2011, from http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT.
Pampel, F. C., & Denney, J. T. (2011). Cross-national sources of health inequality: Education and Tobacco Use in the World Health Survey. Demography, 48, 653–674.
Parliament of Australia. (2011). Tobacco Plain Packaging Bill. Retrieved March 29, 2012, from http://www.yourhealth.gov.au/internet/yourhealth/publishing.nsf/Content/6B16D93A9E2CF9CECA2579540005F62D/$File/Tobacco%20Plain%20Packaging%20Bill%202011%20-%20Exposure%20Draft%20-%2031%20March%202011.pdf.
Peto, R., & Lopez, A. (2000). The future worldwide health effects of current smoking patterns. Clinical Trial Service Unit & Epidemiological Studies Unit—University of Oxford. Updated via personal communication, June 2011. Retrieved December 3, 2011, from http://www.ctsu.ox.ac.uk/pressreleases/2000-08-02/the-future-worldwide-health-effects-of-current-smoking-patterns.
Philip Morris International. (2010). Annual report 2010. Retrieved August 9, 2011, from http://investors.pmi.com/phoenix.zhtml?c=146476&p=irolreportsannual.
Philip Morris International. (2011). Charitable contributions 2010. Retrieved July 3, 2011, from http://www.pmi.com/eng/about_us/corporate_contributions/documents/2010_charitable_contributions_total.pdf.
Physicians for a Smoke-Free Canada. (2012). Picture based cigarette warnings. Retrieved April 12, 2012, from http://www.smoke-free.ca/warnings/default.htm.
Proctor, R. (2006, June). Angel H Roffo: the forgotten father of experimental tobacco carcinogenesis. Bulletin of the World Health Organization, 84(6), 494–496.
Proctor, R. (2012a). Golden holocaust: Origins of the cigarette catastrophe and the case for abolition. Berkeley, CA: University of California Press.
Proctor, R. N. (2012b). The history of the discovery of the cigarette–lung cancer link: Evidentiary traditions, corporate denial, global toll. Tobacco Control, 21(2), 87–91.
Report on the Committee of Experts on Tobacco Industry Documents. (2000). Tobacco company strategies to undermine tobacco control activities at the World Health Organization. Retrieved August 12, 2011, from http://www.who.int/tobacco/en/who_inquiry.pdf.
Reynolds, R. J. (1984). RJR report—young adult smokers: Strategies and opportunities. Retrieved October 6, 2011, from http://legacy.library.ucsf.edu/tid/fet29d00/pdf.
Riordan, M. (2012). Tobacco and socioeconomic status. Campaign for tobacco-free kids. Retrieved June 21, 2012, from http://www.tobaccofreekids.org/research/factsheets/pdf/0260.pdf.
Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR). (2008, February 6). Opinion On Health Effects Of Smokeless Tobacco Products . Taken from 22nd Plenary Meeting. Retrieved June 5, 2012, from http://ec.europa.eu/health/ph_risk/committees/09_scenihr/scenihr_opinions_en.htm#5.
Simpson, D. (2012). Worldwide news and comment—New Zealand: Pack seal can cover warnings. Tobacco Control, 21(2), 82–86.
Stanfill, S. B., & Stepanov, I. (in press). Chapter 3. Global View of smokeless tobacco products: constituents and toxicity. Smokeless tobacco and public health: A global perspective.
Stanfill, S. B., Connolly, G. N., Zhang, L., Jia, T. L., Henningfield, J., Richter, P., et al. (2011). Surveillance of international oral tobacco products: Total nicotine, un-ionized nicotine and tobacco-specific nitrosamines. Tobacco Control, 20, e2. doi:10.1136/tc.2010.037465.
Stratton, K., Shetty, P., Wallace, R., & Bondurant, S. (Eds.). (2001). Clearing the smoke: Assessing the science base for tobacco harm reduction. Washington, DC: Institute of Medicine, National Academy Press.
Stuckler, D., McKee, M., Ebrahim, S., & Basu, S. (2012). Manufacturing epidemics. The role of global producers in increased consumption of unhealthy commodities including processed foods, alcohol, and tobacco. PLoS Medicine, 9(6), e1001235.
Sutherland, L. A., Kaley, L. A., & Fischer, L. (2010). Guiding stars: The effect of a nutrition navigation program on consumer purchases at the supermarket. The American Journal of Clinical Nutrition, 91(suppl), 1090S–1094S.
Swedish National Institute of Public Health. (2009). Public health 2009: Open comparisons. Retrieved August 25, 2011, from http://www.fhi.se/PageFiles/9183/open-comparisons-2009.pdf.
The Canadian Press. (2012, June 8). Quebec sues big tobacco companies for $60-billion, joining four other provinces in lawsuits. Retrieved July 3, 2012, from http://news.nationalpost.com/2012/06/08/quebec-sues-big-tobacco-companies-for-60-billion-joining-four-other-provinces-in-lawsuits/.
The World Bank. (2011). Gross domestic product, 2010. Retrieved June 21, 2011, http://siteresources.worldbank.org/DATASTATISTICS/Resources/GDP.pdf.
Thun, M., Peto, R., Boreham, J., & Lopez, A. D. (2012). Stages of the cigarette epidemic on entering its second century. Tobacco Control, 21(2), 96–101.
Trichopoulos, D., Kalandidi, A., Sparros, L., & MacMahon, B. (1981). Lung cancer and passive smoking. International Journal of Cancer, 27(1), 1–4.
U.S. Department of Health and Human Services. (2004). The health consequences of smoking: A report of the Surgeon General. Atlanta, GA: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
U.S. Department of Health and Human Services. (2006). The health consequences of involuntary exposure to tobacco smoke: A report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
U.S. Department of Health and Human Services. (2009). Guidance for industry—letter regarding point of purchase food labeling. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Food Safety and Applied Nutrition. Retrieved July 3, 2012, from http://www.fda.gov/Food/GuidanceComplianceRegulatoryInformation/GuidanceDocuments/FoodLabelingNutrition/ucm187208.htm.
U.S. Department of Health and Human Services. (2010). How tobacco smoke causes disease: The biology and behavioral basis for smoking-attributable disease: A report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
U.S. Department of Health and Human Services. (2012). Preventing tobacco use among youth and young adults: A report of the Surgeon General—executive summary. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
U.S. Environmental Protection Agency. (1992). Respiratory health effects of passive smoking: Lung cancer and other disorders. Washington, DC: U.S. Environmental Protection Agency, Office of Research and Development, Office of Air and Radiation.
Wang, Y. C., Coxson, P., Shen, Y. M., Goldman, L., & Bibbins-Domingo, K. (2012). A penny-per-ounce tax on sugar-sweetened beverages would cut health and cost burdens of diabetes. Health Affairs, 31(1), 199–207. doi:10.1377/hlthaff.2011.0410.
Wang, Ke-an. (2011). Think tank Beijing. Personal communication.
World Health Organization. (2004). Tobacco and poverty: A vicious circle. Retrieved April 25, 2011, from http://www.who.int/tobacco/communications/events/wntd/2004/en/wntd2004_brochure_en.pdf.
World Health Organization. (2008). 2008–2013 action plan for the global strategy for the prevention and control of noncommunicable diseases. Retrieved August 16, 2011, from http://whqlibdoc.who.int/publications/2009/9789241597418_eng.pdf.
World Health Organization (2011a). Cardiovascular diseases (CVDs). Retrieved March 30, 2012, from http://www.who.int/mediacentre/factsheets/fs317/en/index.html.
World Health Organization. (2011b). Chronic obstructive pulmonary disease (COPD). Retrieved March 30, 2012, from http://www.who.int/mediacentre/factsheets/fs315/en/index.html.
World Health Organization. (2011c). Diabetes. Retrieved March 30, 2012, from http://www.who.int/mediacentre/factsheets/fs312/en/index.html.
World Health Organization. (2011d). Fact Sheet Number 339—tobacco. Retrieved July 28, 2011, from http://www.who.int/mediacentre/factsheets/fs339/en/index.html.
World Health Organization. (2011e). Framework Convention on Tobacco Control. Retrieved May 22, 2013, from http://www.who.int/fctc/en/.
World Health Organization. (2011f). Noncommunicable diseases. Retrieved March 30, 2012, from http://www.who.int/mediacentre/factsheets/fs355/en/index.html#.
World Health Organization. (2011g). United Nations high-level meeting on Noncommunicable Disease Prevention and Control. Retrieved March 30, 2012, from http://www.who.int/nmh/events/un_ncd_summit2011/en/.
World Health Organization. (2011h). WHO report on the Global Tobacco Epidemic, 2011: warning about the dangers of tobacco. Geneva: World Health Organization
World Health Organization. (2012a). Cancer. Retrieved March 30, 2012, from http://www.who.int/mediacentre/factsheets/fs297/en/.
World Health Organization. (2012b). Parties to the WHO framework convention on tobacco control. Retrieved May 22, 2013, from http://www.who.int/fctc/signatories_parties/en/index.html.
World Health Organization. (2012c). WHO global report: Mortality attributable to tobacco. Geneva: World Health Organization. Retrieved March 26, 2012, from http://whqlibdoc.who.int/publications/2012/9789241564434_eng.pdf.
Zhu, S. H., Lee, M., Zhuang, Y. L., Gamst, A., & Wolfson, T. (2012). Interventions to increase smoking cessation at the population level: How much progress has been made in the last two decades? Tobacco Control, 21(2), 110–118.
Acknowledgments
Special acknowledgments to Stephen B. Stanfill, Research Chemist, Centers for Disease Control and Prevention, National Center for Environmental Health for his assistance with the smokeless tobacco section.
For more information on tobacco visit the comprehensive Web site www.tobaccoportal.org.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Eriksen, M., Whitney, C. (2013). Risk Factors: Tobacco. In: McQueen, D. (eds) Global Handbook on Noncommunicable Diseases and Health Promotion. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-7594-1_8
Download citation
DOI: https://doi.org/10.1007/978-1-4614-7594-1_8
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-7593-4
Online ISBN: 978-1-4614-7594-1
eBook Packages: MedicineMedicine (R0)