
Abstract
Epilepsy is a serious neurological disorder and in up to one-third of individuals with epilepsy, medication does not adequately control their seizures. Surgery is currently the most effective treatment in patients with pharmacoresistant epilepsy and postsurgical seizure freedom depends on accurately identifying the epileptogenic region. Broad bandwidth direct brain recordings in presurgical patients and chronic models of epilepsy reveal brief spontaneous bursts of electrical activity in the interictal EEG termed high-frequency oscillations (HFOs; 80–600 Hz) that are believed to reflect fundamental neuronal disturbances responsible for epilepsy. In the epileptic brain, pathological HFOs (pHFOs) are strongly linked to brain areas capable of generating spontaneous seizures, and in some cases the occurrence of pHFOs can predict the transition to ictus. Experimental evidence indicates a correlation between postsurgical seizure freedom and removal of tissue generating interictal and ictal pHFOs, thus supporting the view that pathological HFOs could be a biomarker to epileptogenicity.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
3.1 Introduction
3.1.1 Brief History of Electroencephalography
There were many pioneering achievements in the discovery of brain electrical activity and electroencephalography (EEG) that are reviewed in greater detail elsewhere (Brazier 1961; Niedermeyer 1993), but some are highlighted here to place the relatively new domain of high frequency (>80 Hz) activity in the context of EEG. In 1875, Richard Caton first reported spontaneous electrical activity from the brains of rabbits and monkeys (Caton 1875). During this early period of electrophysiological investigation of the brain, there were a number of studies describing spontaneous activity (Beck 1890; Pravdich-Neminsky 1913), evoked brain activity using electrical stimulation (Danilevsky 1891) and studies on abnormal electrical discharges in experimentally induced epilepsy (Kaufman 1912; Cybulski and Jelenska-Maciezyna 1914). Extending the EEG work in animals, groundbreaking studies were carried out by Hans Berger who recorded the first EEG in humans (Berger 1929). Berger’s initial study published in 1929 described large amplitude electrical activity occurring at ten waves (cycles) per second (hertz, Hz) in awake subjects with eyes closed that was termed “alpha” rhythm and another faster, smaller amplitude activity (average period of 35 ms) that appeared when subjects opened their eyes that was labeled “beta” waves (Berger 1929). In addition, Berger also observed a 3 Hz rhythm during seizures in patients with epilepsy that was clearly illustrated and thoroughly described by Frederic Gibbs and colleagues as the now typical 3 Hz spike-and-wave ictal rhythm associated with absence epilepsy (Berger 1933; Gibbs et al. 1935, 1936). The number of neurophysiological studies of epilepsy grew rapidly with improvements in EEG instruments and techniques [review by (Collura 1993)], and a clinical role of scalp and intracerebral EEG was established for localizing epileptogenic brain areas in the surgical treatment of epilepsy (Penfield 1939; Bailey and Gibbs 1951; Jasper 1941; Jasper et al. 1951; Talairach et al. 1958; Crandall et al. 1963). Importantly, the increasing practice of intracerebral EEG and the development of wide bandwidth digital recording systems with fast sampling rates revealed ictal and interictal high-frequency oscillations (HFOs) 80 Hz and higher in presurgical patients (Fisher et al. 1992; Allen et al. 1992; Bragin et al. 1999a, b). These more recent developments in the field of EEG have propelled a new line of basic and clinical studies of HFOs associated with normal and abnormal function in the mammalian brain.
3.1.2 EEG Rhythms
In the context of EEG and magnetoencephalography (MEG), the term rhythm or oscillation generally refers to a pattern consisting of a regular variation in the signal around a baseline value repeated over time. Based on a convention of describing electromagnetic oscillations with respect to a dominant period or frequency, the traditional EEG labels and frequency bands consist of delta (1–4 Hz), theta (>4–8), alpha/mu (>8–13 Hz), beta (>13–30 Hz), and gamma (>30–80 Hz). Slow oscillations (<1 Hz) are a relatively new category (Steriade et al. 1993), as is a broad category labeled HFOs that include “ripples” (>80–200 Hz) (O’Keefe and Nadel 1978; Buzsaki et al. 1992), “fast ripples” (>200–600 Hz) (Bragin et al. 1999a, b), and “sigma bursts” (600 Hz and above) (Curio et al. 1994). Gamma could also be considered within the category of HFOs based on similarities in frequency and possibly mechanisms of neuronal synchronization as well as functions (Engel and da Silva 2012). The current discussion, however, concentrates on HFOs defined as oscillations with a central spectral frequency between 80 and 600 Hz that occur in hippocampal formation and neocortex.
In spite of the seemingly distinct EEG frequency bands, oscillation frequency spectra do not always fall within band limits. For example, in the normal mammalian brain, HFOs above 80 Hz and extending up to 200 Hz have been labeled “high” or “fast” gamma (Crone et al. 2006; Sullivan et al. 2011; Belluscio et al. 2012), which overlaps with frequencies associated with ripples generated hippocampus CA1 (Csicsvari et al. 1999a). Evidence suggests gamma proper (i.e., 30–80 Hz) and fast gamma could arise via different mechanisms (Belluscio et al. 2012), while fast gamma in CA3 and ripples in CA1, although spatially distinct patterns, appear to share common mechanistic properties (Sullivan et al. 2011). In addition, fast ripples and fast ripple-frequency HFOs are not always clearly distinguished (e.g., spontaneous vs. sensory evoked, hippocampus or neocortex or both). Furthermore, in the normal dentate gyrus, there is little evidence for ripples, yet the epileptic dentate gyrus can generate ripple-frequency HFOs and fast ripples and both are considered to be pathological (Bragin et al. 2004). These examples illustrate the confusion in the terminology and how labeling oscillations based on frequency alone provides little information on the mechanisms of generation or distinguishing normal from abnormal oscillations (Engel et al. 2009). Recommendations have been made to standardize the description of HFOs not only in terms of (1) frequency range but also indicate (2) whether HFOs arise spontaneously or are evoked, (3) occur during behavior or specific brain state, e.g., non-rapid eye movement (non-REM) or REM sleep, (4) occur transiently (burst) or as a steady state event, and (5) the brain area in which they occur (Jefferys et al. 2012). While additional information will help establish common terminology, identifying different types of HFO in the normal and epileptic brain depends on a better understanding of the mechanism underling their generation.
3.2 High-Frequency Oscillations in Normal Mammalian Brain
3.2.1 Hippocampal Sharp Wave–Ripple Complexes
In order to understand the potential mechanisms and role(s) of abnormal HFOs in the epileptic brain, it would be helpful to first describe the mechanisms generating HFOs in the normal brain. The most well-studied HFO in the normal intact brain are spontaneous ripples (80–200 Hz) in the non-primate hippocampal CA1 and CA3 subfields, subicular and entorhinal cortices (Chrobak and Buzsaki 1996). Ripples are also found in hippocampus and adjacent structures of non-primate human and humans (Skaggs et al. 2007; Bragin et al. 1999a; Le Van Quyen et al. 2008; Staba et al. 2002a). Ripples occur during episodes of waking immobility, feeding and grooming behavior, and non-REM sleep and commonly coincide with large amplitude sharp waves (Fig. 3.1a) (Buzsaki et al. 1992; Buzsaki 1986). The latter EEG events reflect irregular population bursts of CA3 neurons that likely arise when extra-hippocampal inputs (e.g., cholinergic input from septum) that normally suppress burst firing are reduced (Buzsaki et al. 1983). During sharp waves, the CA3 excitatory impulses are projected forward via the Schaffer collateral system onto dendrites of CA1 pyramidal cells and various types of interneurons that increases spike firing (Buzsaki et al. 1992; Csicsvari et al. 1999b; Ylinen et al. 1995; Klausberger et al. 2003). Through local chemical synaptic interactions, and likely gap junction and ephaptic interactions (Draguhn et al. 1998; Schmitz et al. 2001; Traub et al. 1999; Anastassiou et al. 2010; Bikson et al. 2004; Jefferys and Haas 1982), synchronous firing among CA1 pyramidal and some interneurons (e.g., basket cells) triggers a brief (~30–100 ms) ripple oscillation. The extracellular-recorded ripple reflects active inward currents of synchronously discharging neurons, largely pyramidal cells and possibly interneurons, and synchronous fast inhibitory postsynaptic potentials (IPSPs) from basket cells (Ylinen et al. 1995).

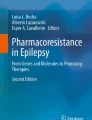
Normal and pathological HFOs. (a) Spontaneous ripple recorded in CA1 of normal rat during non-REM sleep using tungsten microwires (diameter 40 μm). Ripple appears in broad bandwidth (0.1 Hz–1 kHz; top) and bandpass filter (80–200 Hz; middle) traces recorded above the pyramidal cell layer (str. pyr.). Sharp wave (spw) is shown in broad bandwidth trace recorded below pyramidal cell layer within stratum radiatum (str. rad.; bottom). (b) Averaged somatosensory evoked potential (sep; 1 Hz–2 kHz; top trace) recorded in rat barrel cortex during contralateral whisker stimulation. Bandpass filter trace (200–600 Hz; bottom) illustrates fast ripple-frequency HFO superimposed the initial component of the biphasic positive–negative (P1–N1) slow wave. Signal recorded on one electrode (diameter 100 μm) of a 64-contact epipial grid electrode array (bottom). (c) Broad bandwidth (1 Hz–3 kHz; top trace) interictal EEG spike associated with pHFO recorded in entorhinal cortex ipsilateral to seizure onset of patient with MTLE. pHFO occurs on descending limb of depth-negative component of interictal spike. Bottom trace illustrates pHFO on shorter time scale. Signal recorded on a microelectrode like the one shown at the bottom of panel (d). (d) Spontaneous pHFO in the absence of EEG spike. Interictal pHFO recorded in subiculum ipsilateral to seizure onset of patient with bilateral MTLE on a microelectrode (each 40 μm in diameter) extending beyond the distal tip of a clinical depth electrode (bottom). (e) Broad bandwidth (1 Hz–3 kHz; top trace) EEG illustrating pHFO recording a clinical depth electrode (“macroelectrode” like in panel (d)) positioned in anterior hippocampus. Bandpass filtered (200–600 Hz) trace illustrating fast ripple-frequency HFO. Note the small amplitude HFO (denoted by black triangles) and difference in amplitude between HFO recorded on clinical depth electrode (~25 μV peak-to-peak) and HFOs captured on microelectrodes in panels (c) and (d) (>1 mV)
3.2.2 Neocortical HFOs
There are several conditions when HFOs occur in normal neocortex, but studies are needed to clarify the mechanisms associated with the different types of HFOs. In cats, neocortical HFOs (80–200 Hz) occur spontaneously during non-REM sleep and ketamine anesthesia (Grenier et al. 2001). In rats, HFOs (400–600 Hz) are associated with high-voltage spindles and can be evoked with electrical stimulation of the thalamus (Kandel and Buzsaki 1997), and mechanical stimulation of the rat’s whisker evokes HFOs (200–600 Hz) in somatosensory cortex (Fig. 3.1b) (Jones and Barth 1999). In general, neocortical neuronal firing increases during HFOs and in particular fast-spiking cells (presumably GABAergic interneurons) discharge bursts of spikes time-locked to the negative wave of extracellular spontaneous or sensory-evoked HFO (Grenier et al. 2001; Jones et al. 2000). Some pyramidal cells such as rhythmic bursting cells fire spikes coincident with troughs of the spontaneous HFO (Grenier et al. 2001), while regular-spiking cell responses included a combination of subthreshold potentials, single or less frequently multiple spikes (Jones et al. 2000). Evidence thus far suggests that neocortical HFOs reflect firing of pyramidal cells synchronized through excitatory synaptic transmission (Ikeda et al. 2002) and possibly gap junctions or ephaptic field effects. Interestingly, antagonism of GABA-A receptor-mediated transmission does not suppress sensory-evoked HFOs, but rather significantly increases their duration in rats (Jones and Barth 2002). In this latter study, further antagonism of fast inhibition generated abnormal spontaneous slow waves associated with HFOs similar to the paroxysmal activity observed in cats under ketamine that showed a disruption in time-locked discharges of fast-spiking cells with HFO (Grenier et al. 2003). These data suggest that fast IPSPs do not contribute significantly to extracellular HFO in normal neocortex, but similar to hippocampal ripples, inhibitory processes likely play an important role in regulating principal cell spike firing during spontaneous as well as sensory-evoked neocortical HFOs.
3.2.3 Physiological Significance of HFOs
The synchrony of neuronal activity associated with HFOs has been implicated with physiological processes such as encoding information (Singer 1993), sensorimotor integration (Murthy and Fetz 1992), and memory consolidation (Buzsaki 1996). The former are presumed to be mediated primarily by gamma oscillations, while the latter involve hippocampal ripples. There exists ample neurophysiologic data from non-primate and human studies that supports a role of sharp wave-ripples in memory consolidation during sleep (Kudrimoti et al. 1999; Nadasdy et al. 1999; Clemens et al. 2007; Wierzynski et al. 2009; Siapas and Wilson 1998; Axmacher et al. 2008; Le Van Quyen et al. 2010). Most of the evidence is indirect, however, two studies showed that electrical stimulation timed to disrupt neuronal discharges associated with sharp wave–ripple complexes during slow wave sleep was associated with significant learning and performance impairments during subsequent waking episodes (Girardeau et al. 2009; Ego-Stengel and Wilson 2010). If ripples do play a role in memory consolidation, then hippocampal damage associated with epilepsy such as hippocampal sclerosis in mesial temporal lobe epilepsy (MTLE) might impede ripple generation and produce hippocampal-dependent memory impairments. Indeed, one study found reduced performance on spatial memory tasks in patients with temporal lobe epilepsy (Abrahams et al. 1999). In addition, the generation of spontaneous pathological HFOs could disrupt the normal spatiotemporal sequence of spike firing during endogenous ripples and produce learning or memory deficits (Buzsaki and Silva 2012).
3.3 HFOs in the Epileptic Brain
3.3.1 Pathological HFOs in Epileptic Animals
Spontaneous HFOs termed “fast ripples” (200–600 Hz) were first described in the unilateral intrahippocampal kainic acid (KA) rat model of temporal lobe epilepsy (TLE) (Bragin et al. 1999b, 2000). In these initial studies, fast ripples appeared as brief bursts primarily during interictal episodes while rats were asleep and were considered abnormal because they localized to injected dentate gyrus and hippocampus where seizures began and they could also occur during the onset of some hippocampal seizures. Subsequent studies found fast ripples and ripple-frequency HFOs in the dentate gyrus of epileptic rats and both were considered “pathological HFOs” (pHFOs) because previous studies did not find ripples in the normal dentate gyrus (Bragin et al. 1999b), both were only found in KA-treated rats that subsequently developed spontaneous seizures, and the sooner pHFOs appeared after KA-induced status epilepticus, the sooner spontaneous seizures appeared (Bragin et al. 2004, 2005). Evidence from other chemically induced status epilepticus models (e.g., pilocarpine) supports the strong association between pHFOs and epileptogenicity as well as severity of neuron loss (Foffani et al. 2007; Levesque et al. 2011). However, recent evidence from the intrahippocampal tetanus toxin model of TLE indicates that status epilepticus or extensive neuron loss are not required for the generation of pHFOs (Jiruska et al. 2010b), suggesting there could be different types and mechanisms generating pHFOs.
3.3.2 Mechanisms Generating pHFOs
Currently there are no reliable means for separating pHFOs from normal HFOs in the epileptic brain, but understanding the mechanisms generating pathological and normal HFOs could reveal properties unique to each group that could provide the basis for such strategies. Microelectrode recordings in the intact dentate gyrus and hippocampus of post-status epilepticus epileptic rats suggest interictal pHFOs reflect a brief burst of population spikes that arise from clusters of pathologically interconnected neurons (or PIN clusters) that generate abnormally synchronous discharges (Bragin et al. 1999b, 2000, 2007b). It appears principal cells are the primary contributors to pHFOs because in vivo juxta-cellular studies carried out in the dentate gyrus of pilocarpine-treated epileptic rats found an increase in granule cell discharges aligned with the negative waves of the extracellular pHFO (in some cases a single population spike) and reduction in presumed basket cell firing (Bragin et al. 2011) (contrast with normal CA1 ripples described in Sect. 3.2.1). Furthermore, in hippocampal tissue with high concentrations of extracellular K+, it seems recurrent excitatory connections among CA3 pyramidal cells generate synchronous firing and bursts of population spikes (Dzhala and Staley 2004). These data argue for a limited role of inhibitory processes in the generation of dentate gyrus and hippocampal pHFOs and little contribution of IPSPs to extracellular current sources, which is consistent with persistence of in vitro pHFOs after suppressing GABA-A receptor-mediated transmission (D’Antuono et al. 2005; Foffani et al. 2007).
In spite of results in the preceding paragraph and principal cell’s elongated dendritic architecture that can give rise to open fields with strong extracellular current flow, it is possible that some types of interneurons are active during pHFOs and could contribute current flow in the local extracellular environment. While basket cells fire during normal CA1 ripples, other types of interneurons stop firing (Ylinen et al. 1995; Klausberger et al. 2003). It appears Bragin and colleagues were recording from single basket cells during pHFOs in epileptic dentate gyrus (Bragin et al. 2011), but this pattern of activity might not reflect all types of interneurons. Symmetrical depolarization of an interneuron’s spherically projecting dendrites would likely generate a close field with current dipoles canceling one another. However, if interneuron dendrites were depolarized in a spatially asymmetrical or temporally asynchronous pattern, then a detectable dipole might be produced (Buzsaki et al. 2012). Morphological alterations in some epileptogenic lesions (e.g., hippocampal sclerosis) might contain axonal sprouting and synaptic reorganization that activate interneurons and produce current sources in a manner not found in normal tissue (Menendez de la Prida and Trevelyan 2011). Studies are needed to determine if this is correct and whether in the epileptic brain there exists unique HFOs that reflect interneuron discharges that might play a role in maintaining the interictal state.
Recordings in the intact rodent epileptic brain explain some but not all of the features associated with pHFOs. For example, the mechanisms that underlie synchronous neuronal spike firing are not known. It is reasonable that gap junctions could play a role and there is evidence from in vitro and network modeling studies for pHFOs in the absence of chemical synaptic transmission (Draguhn et al. 1998; Jiruska et al. 2010a; Roopun et al. 2010). In addition, synchrony of neuronal discharges might be achieved more easily under conditions that promote excitability, e.g., cell type-specific neuron loss, alterations in inhibition, gliosis, axon spouting, synaptic reorganization (Esclapez et al. 1999; Esclapez and Houser 1999; Shao and Dudek 2005; Huberfeld et al. 2007). Indeed, single neuron studies in patients with epilepsy found increased interictal excitability and synchrony of neuronal discharges in the seizure onset zone (SOZ), and more recently evidence for neuronal hyperexcitability associated with gray matter loss in the mesial temporal lobe SOZ (Staba et al. 2002b, 2011).
Evidence for synchronous principal cell bursting appears to explain pHFOs that occur at frequencies up to 300 Hz (Dzhala and Staley 2004; Foffani et al. 2007; Ibarz et al. 2010), but since single neurons rarely fire at frequencies greater than 300 Hz (Colder et al. 1996; Staba et al. 2002b, c), this neuronal mechanism does not adequately explain how pHFOs up to 600 Hz occur. It has been recently proposed that pHFOs such as fast ripples emerge from the out-of-phase firing between small groups of neurons with individual neurons discharging at low frequencies and few neurons firing during consecutive waves of the extracellular pHFO (Foffani et al. 2007; Ibarz et al. 2010; Jiruska et al. 2010a). This hypothesis better explains the precision of spike firing and frequency spectra of individual pHFO, as well as the spectral variability from one pHFO to the next (Dzhala and Staley 2004; Foffani et al. 2007; Ibarz et al. 2010; Menendez de la Prida and Trevelyan 2011). It is less clear how phase differences could arise between groups of neurons, although several possibilities might promote out-of-phase firing, such as weak ephaptic field effects, neuron loss, circuit reorganization, or irregular spread of activity throughout neuronal networks (Menendez de la Prida and Trevelyan 2011; Kohling and Staley 2011).
3.3.3 HFOs in Clinical Epilepsy
3.3.3.1 Recording and Detection of HFOs
The optimal size and configuration of electrodes to capture HFOs is not known. Studies in epileptic rats and presurgical patients using small diameter microelectrodes (40–60 μm) estimate the volume of tissue generating pHFOs could be as small as 1 mm3 (Bragin et al. 2002a, b). Since a large electrode compared to microelectrode might be positioned at a greater distance from a pHFO-generating site and electrical potential attenuates in direct proportion to the square of distance from the current source(s), a large electrode might record pHFOs less reliably. In addition, the effective surface area of a large electrode would average extracellular current sources within a larger volume of tissue than a microelectrode that might also reduce pHFO signal (e.g., ~6 mm2 for clinical depth electrode contact versus 0.0013 mm2 for a microelectrode). A number of studies using electrodes with different diameters and configurations have captured pHFOs with remarkably similar results that suggests the volume of tissue generating pHFOs could be much larger (Bragin et al. 1999a; Staba et al. 2002a; Urrestarazu et al. 2007; Khosravani et al. 2008; Crepon et al. 2010; Schevon et al. 2009). Furthermore, one study compared hippocampal ripples and fast ripples recorded with electrodes of different sizes and found no difference in duration or spectral frequency with respect to electrode diameter (Chatillon et al. 2011). However, in this same study the mean amplitude of ripples and fast ripples was significantly lower and rates of each higher compared to the respective amplitudes and rates of these HFOs reported in a previous microelectrode study (compare Fig. 3.1c–e) (Bragin et al. 1999b). By contrast, another study found a significant reduction in the number of fast ripples recorded with standard clinical electrodes compared to microelectrodes (Worrell et al. 2008). Based on current evidence, it is clear that identifying the optimal electrode(s) to reliably capture all types of HFOs and developing uniform HFO criteria and detection strategies will be important for the use of HFOs in clinical studies.
There are no formal criteria for HFOs, but the features typically reported in studies using different types of electrodes include amplitude (10–1,000 μV), frequency (80–600 Hz), and duration (10–100 ms) (Worrell et al. 2012). Detection methods generally fall into categories of manual review, supervised and unsupervised computer-automated detection with strengths and weaknesses associated with all methods (Staba et al. 2002a; Gardner et al. 2007; Crepon et al. 2010; Zelmann et al. 2012). Most strategies include a comparison between the continuous bandpass filtered signal and an energy threshold computed from a baseline period to detect episodes that exceed threshold and selected as putative HFOs. The baseline can be the entire continuous signal that could result in high threshold values for electrodes containing significant HFO activity or computed from epochs that do not contain HFOs, but this requires careful review and no guarantee the chosen epochs is representative of the continuous signal. Scalp and intracranial EEG recordings contain physiological and epileptiform sharp transients (interictal EEG spikes) and artifacts (electrode noise, eye- and muscle-related activity) that contain high frequency power and digital filtering of these events could be incorrectly interpreted as HFOs (Benar et al. 2010; Worrell 2012). Manual post hoc review of putative events in the unfiltered signal can confirm the authenticity of HFOs, although this can be time consuming and subjective. Automated review using other aspects of the signal can also be used (e.g., duration, number of waves, inter-event interval), which imposes restrictions on HFOs features. Based on the potential use of HFOs in the localization of the epileptogenic zone (i.e., brain area(s) necessary and sufficient for generating spontaneous seizures) and surgical planning, it seems prudent that the detection of HFOs should not be based solely on results of signal processing, but include a step of expert review.
3.3.3.2 Interictal HFOs
Initial studies describing spontaneous interictal HFOs (80–600 Hz) were carried out in presurgical patients with MTLE using microelectrodes and found a strong association between fast ripples, but not ripple-frequency HFOs, and the SOZ (Fig. 3.1c–d) (Bragin et al. 1999a, b). Subsequent quantitative studies confirmed the association of fast ripples with SOZ (Staba et al. 2002a), and fast ripples and ripple-frequency HFOs with states of vigilance, finding that the rates of both types of HFOs were highest during episodes of non-REM sleep (Staba et al. 2004). Voltage depth analysis in entorhinal cortex indicated fast ripples and ripple-frequency HFOs were generated within cell lamina of entorhinal cortex, but the fast ripples could arise from smaller cellular areas compared to ripple-frequency HFOs (Bragin et al. 2002b). Moreover, higher rates of fast ripples and lower rates of ripple-frequency HFOs correlated with hippocampal atrophy and reduced neuron densities (Staba et al. 2007; Ogren et al. 2009). These data suggest that morphological alterations associated with hippocampal sclerosis in MTLE could be an anatomical substrate for hippocampal fast ripples and some ripple-frequency HFOs that could also be pathological.
Studies using larger diameter electrodes and commercial clinical electrodes verified and extended microelectrode studies of HFOs. The link between fast ripples, as well as ripple-frequency HFOs, and SOZ was confirmed in MTLE and neocortical epilepsy, although fast ripples appear more specific to the SOZ particularly in MTLE (Jacobs et al. 2008; Crepon et al. 2010). In addition, one study found pHFOs in epileptogenic tissue extending beyond areas pathology in other lesional epilepsies (Jacobs et al. 2009a), and another study found pHFOs in the SOZ of patients with normal MRI (Andrade-Valenca et al. 2012), although histological analysis of resected tissue indicated gliosis and neuron loss in many of these patients. The explanation for association between ripple-frequency HFOs and SOZ is not clear, but these HFOs appear similar to pHFOs described in microelectrode studies and some have suggested a bias of larger diameter electrodes to capture pHFOs versus normal HFO including ripples (Crepon et al. 2010; Engel and da Silva 2012). In contrast to the studies cited above that have focused on pHFOs that occur as brief bursts in the EEG, recent work has identified continuous interictal HFO (>80 Hz, >500 ms in duration) activity in hippocampus of presurgical patients (Mari et al. 2012), although this study did not find evidence for continuous HFO that was unique to epileptogenic tissue.
Several studies have emphasized the spatial and temporal association between pHFOs and interictal EEG spikes. Interictal EEG spikes can be useful for identifying epileptogenic tissue (Lieb et al. 1978), but EEG spikes can also occur outside of the epileptogenic region and their accuracy can dependent on state of vigilance, i.e., wakefulness vs. sleep (Wieser et al. 1979; Lieb et al. 1980; Sammaritano et al. 1991). A large percentage of EEG spikes occur independently of pHFOs and vice versa, although some EEG spikes do contain pHFOs yet the pHFO might not be visible in broad bandwidth recordings unless the signal is filtered or detected using statistical time–frequency analysis (Urrestarazu et al. 2007; Kobayashi et al. 2009). Importantly, studies suggest that EEG spikes with pHFOs as well as pHFOs alone more accurately localize epileptogenic regions than EEG spikes alone (Jacobs et al. 2008, 2010). The mechanisms that give rise to EEG spike–pHFO complexes are not known, but studies have found a dissociation between EEG spikes and pHFOs during medication withdrawal and with respect to seizures (Zijlmans et al. 2009, 2011). In addition, others have proposed that tissue with EEG spikes containing pHFOs reflect hypersynchronous discharges of neurons that actively participate in the generation and propagation of epileptiform activity. By contrast, sites with EEG spikes that do not contain pHFOs receive abnormal input that is not sufficient to generate hypersynchronous neuron activity (Bragin et al. 2010).
As discussed in Sects. 3.3.1 and 3.3.2 ripple-frequency HFOs in dentate gyrus are considered abnormal, but it is not known if ripple-frequency HFOs outside the dentate gyrus are abnormal and, if so, how to distinguish them from normal ripples. In presurgical patients, ripple-frequency HFOs can occur in hippocampus, subicular and entorhinal cortices and share several important features with ripples in the normal rodent hippocampus. Human ripples occur most frequently during the ON-periods (likely the UP-phase) of non-REM sleep and least often during REM sleep (Bragin et al. 1999a; Staba et al. 2002a, 2004; Nir et al. 2011). Single neuron analysis found a significant increase in both putative interneurons and pyramidal cells during spontaneous ripples in entorhinal cortex (Le Van Quyen et al. 2008). In this same study, spike firing was aligned with the negative wave of the extracellular ripple in a cell type-specific, time-dependent manner similar to the firing pattern of pyramidal cells and some interneurons during normal rodent hippocampal ripples (Klausberger et al. 2003). With respect to the hypothesized role of hippocampal ripples in cognitive performance (Sect. 3.2.3), one patient study found that the rate of ripples in rhinal cortex correlated with the number of successfully recalled items learned during a prior waking period (Axmacher et al. 2008). Developing strategies to reliably identify normal HFOs like hippocampal ripples in the epileptic brain will greatly benefit patient studies investigating the functional roles of HFOs in learning, memory, and sleep.
3.3.3.3 Ictal HFOs
Hypotheses for the role of pHFOs in the transition to ictus in clinical epilepsy derive largely from animal studies. In vitro evidence indicates pHFO-generating sites are surrounded by tissue containing strong inhibition and a reduction in inhibition expands the area generating pHFOs (Bragin et al. 2002a). Moreover, in the intact dentate gyrus of epileptic rats showed a progressive increase in pHFO amplitude, power, and duration preceding seizure onset that could reflect the growth and coalescence of PIN clusters (Bragin et al. 2005). Data such as these form the basis of one hypothesis of seizure genesis that proposes pre-ictal pHFOs arising from PIN clusters trigger wide spread feedback inhibition that subsequently evolves into hypersynchronous discharges as a result of rebound from global inhibition (Bragin et al. 2007a). This hypothesis with respect to clinical EEG might appear as a sequence of single or multiple pre-ictal large amplitude spikes associated with slow wave and low voltage fast activity that evolves to slow rhythmic EEG discharges (Spencer et al. 1992a, b; Bragin et al. 2007a). If correct, then analysis of wide bandwidth EEG should detect an increase in spectral power corresponding with pHFO frequencies before or during the onset of seizures. Several patients studies have indeed detected an increase in pHFO power in the SOZ during or preceding ictal onset by several minutes to seconds (Fisher et al. 1992; Allen et al. 1992; Traub et al. 2001; Jirsch et al. 2006; Khosravani et al. 2008; Worrell et al. 2004). In these same studies, changes in pHFO power were chiefly detected in the primary SOZ and rarely in sites of secondarily generalization of patients with focal epilepsy (Jirsch et al. 2006). Similar changes in pHFOs occurred during epileptic spasms and in some cases before the clinical onset (Ochi et al. 2007; Akiyama et al. 2005, 2006; Ramachandran Nair et al. 2008; Nariai et al. 2011a, b). In one of these latter studies (Akiyama et al. 2006), pHFO power could be observed spreading across cortex and increasing in size during the seizure.
Results from the studies cited above contrast with data from other patient studies that found less predictable changes in pHFO during transition ictus (Zijlmans et al. 2011; Jacobs et al. 2009b), suggesting pHFOs could be one of many possible mechanisms involved with seizure genesis. However, in the epileptic brain, if ripple-like HFOs exist that reflect inhibitory processes and regulate neuronal excitability, then the irregular occurrence or progressive reduction of these HFOs might facilitate the transition to ictus (Bragin et al. 2010). An in vitro study found beta-frequency oscillatory activity largely driven by interneuron firing during seizure onset, but IPSPs progressively declined and principal cell firing increased along with the evolution of the seizure (Gnatkovsky et al. 2008). One interpretation of these data is that some HFOs in the intact epileptic brain are associated with inhibitory processes that could prevent the transition to ictus.
3.3.3.4 Role of pHFOs in Epilepsy
Since pHFOs appear to reflect unique epileptic neuronal disturbances, pHFOs provide a novel approach to investigate basic neuronal mechanisms of epileptogenicity, seizure generation and epileptogenesis, the development and progression of tissue capable of generating spontaneous seizures (Bragin et al. 2004; Engel and da Silva 2012). Experimental studies in animals and presurgical patients with epilepsy described in the preceding sections indicate pHFOs could be used to identify epileptogenic tissue and thus serve as a biomarker of epileptogenicity (Bragin et al. 2008). Additional evidence in support of this role derive from retrospective studies that show a strong correlation between postsurgical seizure freedom and removal of tissue generating interictal or ictal pHFOs (Jacobs et al. 2010; Wu et al. 2010; Akiyama et al. 2011; Ochi et al. 2007; Nariai et al. 2011b; Fujiwara et al. 2012). As a biomarker of epileptogenicity pHFOs could also identify the presence and severity of the epileptic condition (Ogren et al. 2009; Staba 2012). Scalp EEG or other noninvasive modalities such as MEG or EEG with functional MRI that might detect pHFOs could be used in differential diagnosis of epilepsy versus acute symptomatic seizures and administer appropriate treatment immediately (Engel and da Silva 2012). Towards these goals a recent study recording EEG from scalp electrodes found gamma (40–80 Hz) and HFOs (>80 Hz) that were associated with the SOZ in patients with focal seizures (Andrade-Valenca et al. 2011). Pathological HFOs might be used as a biomarker to evaluate the efficacy of therapy more quickly without having to wait for the occurrence of seizures. Finally, pHFOs could be used to identify individuals at risk for epilepsy after potential epileptogenic insults and evaluating antiepileptogenic therapy or possibly provide an indication for surgical referral in cases of pharmacoresistant epilepsy (Engel and da Silva 2012).
3.4 Conclusions
Results from chronic animal models of epilepsy and presurgical patients with focal epilepsy suggest pHFOs can accurately identify the epileptogenic region and possibly the development of epilepsy after an epileptogenic injury. Currently it is not yet possible to unequivocally distinguish pathological from normal HFOs, although in the normal brain HFOs reflect strong inhibitory processes that regulate principal cell firing, whereas in the epileptic brain pHFOs arise from abnormally synchronous principal cell discharges. It appears morphological alterations associated with epileptogenic lesions contribute to the generation of some pHFOs, but not others that primarily arise from functional disturbances in principal and inhibitory circuits. It is anticipated that optimizing electrodes and methods for capturing and analyzing HFOs will provide insight into the mechanisms that synchronize neuronal activity and a basis for separating normal HFOs from pHFOs, and likely identify unique pHFOs in different types of epilepsy. Interictal pHFOs, thus far, are one of few potential biomarkers of epileptogenicity that could be used to localize the epileptogenic zone and assist in the surgical treatment of pharmacoresistant epilepsy, identify the presence and severity of the epileptic condition, and possibly serve as a biomarker to evaluate the efficacy of new antiseizure and anti-epileptogenic therapies.
Abbreviations
- EEG:
-
Electroencephalography
- HFO:
-
High-frequency oscillation
- IPSP:
-
Inhibitory postsynaptic potential
- KA:
-
Kainic acid
- MRI:
-
Magnetic resonance imaging
- MTLE:
-
Mesial temporal lobe epilepsy
- non-REM:
-
Non-rapid eye movement sleep
- pHFO:
-
Pathological high-frequency oscillation
- PIN cluster:
-
Pathologically interconnected neuron cluster
- SOZ:
-
Seizure onset zone
References
Abrahams S, Morris RG, Polkey CE, Jarosz JM, Cox TC, Graves M, et al. Hippocampal involvement in spatial and working memory: a structural MRI analysis of patients with unilateral mesial temporal lobe sclerosis. Brain Cogn. 1999;41(1):39–65. doi:10.1006/brcg.1999.1095.
Akiyama T, Otsubo H, Ochi A, Ishiguro T, Kadokura G, RamachandranNair R, et al. Focal cortical high-frequency oscillations trigger epileptic spasms: confirmation by digital video subdural EEG. Clin Neurophysiol. 2005;116(12):2819–25.
Akiyama T, Otsubo H, Ochi A, Galicia EZ, Weiss SK, Donner EJ, et al. Topographic movie of ictal high-frequency oscillations on the brain surface using subdural EEG in neocortical epilepsy. Epilepsia. 2006;47(11):1953–7.
Akiyama T, McCoy B, Go CY, Ochi A, Elliott IM, Akiyama M, et al. Focal resection of fast ripples on extraoperative intracranial EEG improves seizure outcome in pediatric epilepsy. Epilepsia. 2011;52(10):1802–11. doi:10.1111/j.1528-1167.2011.03199.x.
Allen PJ, Fish DR, Smith SJ. Very high-frequency rhythmic activity during SEEG suppression in frontal lobe epilepsy. Electroencephalogr Clin Neurophysiol. 1992;82(2):155–9.
Anastassiou CA, Montgomery SM, Barahona M, Buzsaki G, Koch C. The effect of spatially inhomogeneous extracellular electric fields on neurons. J Neurosci. 2010;30(5):1925–36. doi:10.1523/JNEUROSCI.3635-09.2010.
Andrade-Valenca LP, Dubeau F, Mari F, Zelmann R, Gotman J. Interictal scalp fast oscillations as a marker of the seizure onset zone. Neurology. 2011;77(6):524–31. doi:10.1212/WNL.0b013e318228bee2.
Andrade-Valenca L, Mari F, Jacobs J, Zijlmans M, Olivier A, Gotman J, et al. Interictal high frequency oscillations (HFOs) in patients with focal epilepsy and normal MRI. Clin Neurophysiol. 2012;123(1):100–5. doi:10.1016/j.clinph.2011.06.004.
Axmacher N, Elger CE, Fell J. Ripples in the medial temporal lobe are relevant for human memory consolidation. Brain. 2008;131(7):1806–17. doi:10.1093/brain/awn103.
Bailey P, Gibbs FA. The surgical treatment of psychomotor epilepsy. J Am Med Assoc. 1951;145(6):365–70.
Beck A. Die Bestimmung der Localisation der Gehirn- und Ruckenmarksfunctionen vermittelst der elektrischen Erscheinungen. Zbl Physiol. 1890;4:473–6.
Belluscio MA, Mizuseki K, Schmidt R, Kempter R, Buzsaki G. Cross-frequency phase-phase coupling between theta and gamma oscillations in the hippocampus. J Neurosci. 2012;32(2):423–35. doi:10.1523/JNEUROSCI.4122-11.2012.
Benar CG, Chauviere L, Bartolomei F, Wendling F. Pitfalls of high-pass filtering for detecting epileptic oscillations: a technical note on “false” ripples. Clin Neurophysiol. 2010;121(3):301–10.
Berger H. Uber das Electrenkephalogram des Menschen. Arch Psychiatr Nervenkr. 1929;87:527.
Berger H. Uber das elektrenkephalogramm des menschen. Arch Psychiatr Nervenkr. 1933;100:301–20.
Bikson M, Inoue M, Akiyama H, Deans JK, Fox JE, Miyakawa H, et al. Effects of uniform extracellular DC electric fields on excitability in rat hippocampal slices in vitro. J Physiol. 2004;557(Pt 1):175–90. doi:10.1113/jphysiol.2003.055772.
Bragin A, Engel Jr J, Wilson CL, Fried I, Buzsaki G. High-frequency oscillations in human brain. Hippocampus. 1999a;9:137–42.
Bragin A, Engel Jr J, Wilson CL, Fried I, Mathern GW. Hippocampal and entorhinal cortex high-frequency oscillations (100–500 Hz) in human epileptic brain and in kainic acid–treated rats with chronic seizures. Epilepsia. 1999b;40(2):127–37.
Bragin A, Wilson CL, Engel Jr J. Chronic epileptogenesis requires development of a network of pathologically interconnected neuron clusters: a hypothesis. Epilepsia. 2000;41 Suppl 6:S144–52.
Bragin A, Mody I, Wilson CL, Engel Jr J. Local generation of fast ripples in epileptic brain. J Neurosci. 2002a;22(5):2012–21.
Bragin A, Wilson CL, Staba RJ, Reddick M, Fried I, Engel Jr J. Interictal high-frequency oscillations (80–500 Hz) in the human epileptic brain: entorhinal cortex. Ann Neurol. 2002b;52(4):407–15. doi:10.1002/ana.10291.
Bragin A, Wilson CL, Almajano J, Mody I, Engel Jr J. High-frequency oscillations after status epilepticus: epileptogenesis and seizure genesis. Epilepsia. 2004;45(9):1017–23.
Bragin A, Azizyan A, Almajano J, Wilson CL, Engel JJ. Analysis of chronic seizure onsets after intrahippocampal kainic acid injection in freely moving rats. Epilepsia. 2005;46(10):1592–8.
Bragin A, Claeys P, Vonck K, Van Roost D, Wilson C, Boon P, et al. Analysis of initial slow waves (ISWs) at the seizure onset in patients with drug resistant temporal lobe epilepsy. Epilepsia. 2007a;48(10):1883–94.
Bragin A, Wilson CL, Engel Jr J. Voltage depth profiles of high-frequency oscillations after kainic acid-induced status epilepticus. Epilepsia. 2007b;48(s5):35–40.
Bragin A, Staba RJ, Engel Jr J. The significance of fast ripples in the evaluation of the epileptogenic zone. In: Luders HO, editor. Textbook of Epilepsy Surgery. Abingdon: Taylor & Francis; 2008. p. 530–6.
Bragin A, Engel Jr J, Staba RJ. High-frequency oscillations in epileptic brain. Curr Opin Neurol. 2010;23(2):151–6.
Bragin A, Benassi SK, Kheiri F, Engel Jr J. Further evidence that pathologic high-frequency oscillations are bursts of population spikes derived from recordings of identified cells in dentate gyrus. Epilepsia. 2011;52(1):45–52. doi:10.1111/j.1528-1167.2010.02896.x.
Brazier MAB. A history of the electrical activity of the brain: the first half-century. London: Pitman; 1961.
Buzsaki G. Hippocampal sharp waves: their origin and significance. Brain Res. 1986;398: 242–52.
Buzsaki G. The hippocampo-neortical dialogue. Cereb Cortex. 1996;6:81–92.
Buzsaki G, Silva FL. High frequency oscillations in the intact brain. Prog Neurobiol. 2012;98(3):241–9. doi:10.1016/j.pneurobio.2012.02.004.
Buzsaki G, Leung LW, Vanderwolf CH. Cellular bases of hippocampal EEG in the behaving rat. Brain Res. 1983;287(2):139–71.
Buzsaki G, Horvath Z, Urioste R, Hetke J, Wise K. High-frequency network oscillation in the hippocampus. Science. 1992;256:1025–7.
Buzsaki G, Anastassiou CA, Koch C. The origin of extracellular fields and currents–EEG, ECoG, LFP and spikes. Nat Rev Neurosci. 2012;13(6):407–20. doi:10.1038/nrn3241.
Caton R. The electrical currents of the brain. Br Med J. 1875;2:278.
Chatillon CE, Zelmann R, Bortel A, Avoli M, Gotman J. Contact size does not affect high frequency oscillation detection in intracerebral EEG recordings in a rat epilepsy model. Clin Neurophysiol. 2011;122(9):1701–5. doi:10.1016/j.clinph.2011.02.022.
Chrobak JJ, Buzsaki G. High-frequency oscillations in the output of the hippocampal-entorhinal axis of the freely behaving rat. J Neurosci. 1996;16(9):3056–66.
Clemens Z, Molle M, Eross L, Barsi P, Halasz P, Born J. Temporal coupling of parahippocampal ripples, sleep spindles and slow oscillations in humans. Brain. 2007;11:2868–78. doi:10.1093/brain/awm146.
Colder BW, Wilson CL, Frysinger RC, Harper RM, Engel Jr J. Interspike intervals during interictal periods in human temporal lobe epilepsy. Brain Res. 1996;719(1–2):96–103.
Collura TF. History and evolution of electroencephalographic instruments and techniques. J Clin Neurophysiol. 1993;10(4):476–504.
Crandall PH, Walter RD, Rand RW. Clinical applications of studies on stereotactically implanted electrodes in temporal lobe epilepsy. J Neurosurg. 1963;20:827–40.
Crepon B, Navarro V, Hasboun D, Clemenceau S, Martinerie J, Baulac M, et al. Mapping interictal oscillations greater than 200 Hz recorded with intracranial macroelectrodes in human epilepsy. Brain. 2010;133:33–45. doi:10.1093/brain/awp277.
Crone NE, Sinai A, Korzeniewska A. High-frequency gamma oscillations and human brain mapping with electrocorticography. Prog Brain Res. 2006;159:275–95. doi:10.1016/S0079-6123(06)59019-3.
Csicsvari J, Hirase H, Czurko A, Mamiya A, Buzsaki G. Fast network oscillations in the hippocampal CA1 region of the behaving rat. J Neurosci. 1999a;19(RC20):1–4.
Csicsvari J, Hirase H, Czurko A, Mamiya A, Buzsaki G. Oscillatory coupling of hippocampal pyramidal cells and interneurons in the behaving rat. J Neurosci. 1999b;19(1):274–87.
Curio G, Mackert BM, Burghoff M, Koetitz R, Abraham-Fuchs K, Harer W. Localization of evoked neuromagnetic 600 Hz activity in the cerebral somatosensory system. Electroencephalogr Clin Neurophysiol. 1994;91(6):483–7.
Cybulski N, Jelenska-Maciezyna X. Action currents of the cerebral cortex (in Polish). Bull Acad Sci Krakow. 1914;Ser B:776–81.
Danilevsky VY. Electrical phenomena of the brain. Fiziol Sbornik. 1891;2:77–88.
D'Antuono M, de Guzman P, Kano T, Avoli M. Ripple activity in the dentate gyrus of disinhibited hippocampus-entorhinal cortex slices. J Neurosci Res. 2005;80:92–103.
Draguhn A, Traub RD, Schmitz D, Jefferys JGR. Electrical coupling underlies high-frequency oscillations in the hippocampus in vitro. Nature. 1998;394:189–92.
Dzhala VI, Staley KJ. Mechanisms of fast ripples in the hippocampus. J Neurosci. 2004;24(40):8896–906.
Ego-Stengel V, Wilson MA. Disruption of ripple-associated hippocampal activity during rest impairs spatial learning in the rat. Hippocampus. 2010;20(1):1–10. doi:10.1002/hipo.20707.
Engel Jr J, da Silva FL. High-frequency oscillations: where we are and where we need to go. Prog Neurobiol. 2012;98(3):316–8. doi:10.1016/j.pneurobio.2012.02.001.
Engel Jr J, Bragin A, Staba RJ, Mody I. High-frequency oscillations: what is normal and what is not? Epilepsia. 2009;50(4):598–604.
Esclapez M, Houser CR. Up-regulation of GAD65 and GAD67 in remaining hippocampal GABA neurons in a model of temporal lobe epilepsy. J Comp Neurol. 1999;412(3):488–505.
Esclapez M, Hirsch JC, Ben-Ari Y, Bernard C. Newly formed excitatory pathways provide a substrate for hyperexcitability in experimental temporal lobe epilepsy. J Comp Neurol. 1999;408:449–60.
Fisher RS, Webber WR, Lesser RP, Arroyo S, Uematsu S. High-frequency EEG activity at the start of seizures. J Clin Neurophysiol. 1992;9(3):441–8.
Foffani G, Uzcategui YG, Gal B, Menendez de la Prida L. Reduced spike-timing reliability correlates with the emergence of fast ripples in the rat epileptic hippocampus. Neuron. 2007;55(6):930–41.
Fujiwara H, Greiner HM, Lee KH, Holland-Bouley KD, Seo JH, Arthur T, et al. Resection of ictal high-frequency oscillations leads to favorable surgical outcome in pediatric epilepsy. Epilepsia. 2012;53(9):1607–17. doi:10.1111/j.1528-1167.2012.03629.x.
Gardner AB, Worrell GA, Marsh E, Dlugos D, Litt B. Human and automated detection of high-frequency oscillations in clinical intracranial EEG recordings. Clin Neurophysiol. 2007;118(5):1134–43.
Gibbs FA, Davis H, Lennox WG. The electroencephalogram in epilepsy and in conditions of impaired conciousness. Arch Neurol Psychiatry. 1935;34:1133–48.
Gibbs FA, Lennox WG, Gibbs EL. The electro-encephalogram in diagnosis and in localization of epileptic seizures. Arch Neurol Psychiatry. 1936;36:1225–35.
Girardeau G, Benchenane K, Wiener SI, Buzsaki G, Zugaro MB. Selective suppression of hippocampal ripples impairs spatial memory. Nat Neurosci. 2009;12(10):1222–3. doi:10.1038/nn.2384.
Gnatkovsky V, Librizzi L, Trombin F, de Curtis M. Fast activity at seizure onset is mediated by inhibitory circuits in the entorhinal cortex in vitro. Ann Neurol. 2008;64(6):674–86. doi:10.1002/ana.21519.
Grenier F, Timofeev I, Steriade M. Focal synchronization of ripples (80–200 Hz) in neocortex and their neuronal correlates. J Neurophysiol. 2001;86(4):1884–98.
Grenier F, Timofeev I, Steriade M. Neocortical very fast oscillations (ripples, 80–200 Hz) during seizures: intracellular correlates. J Neurophysiol. 2003;89(2):841–52.
Huberfeld G, Wittner L, Clemenceau S, Baulac M, Kaila K, Miles R, et al. Perturbed chloride homeostasis and GABAergic signaling in human temporal lobe epilepsy. J Neurosci. 2007;27(37):9866–73. doi:10.1523/JNEUROSCI.2761-07.2007.
Ibarz JM, Foffani G, Cid E, Inostroza M, Menendez de la Prida L. Emergent dynamics of fast ripples in the epileptic hippocampus. J Neurosci. 2010;30(48):16249–61. doi:30/48/16249[pii]10.1523/JNEUROSCI.3357-10.2010.
Ikeda H, Leyba L, Bartolo A, Wang Y, Okada YC. Synchronized spikes of thalamocortical axonal terminals and cortical neurons are detectable outside the pig brain with MEG. J Neurophysiol. 2002;87(1):626–30.
Jacobs J, LeVan P, Chander R, Hall J, Dubeau F, Gotman J. Interictal high-frequency oscillations (80–500 Hz) are an indicator of seizure onset areas independent of spikes in the human epileptic brain. Epilepsia. 2008;49(11):1893–907.
Jacobs J, Levan P, Chatillon CE, Olivier A, Dubeau F, Gotman J. High frequency oscillations in intracranial EEGs mark epileptogenicity rather than lesion type. Brain. 2009a;132(Pt 4):1022–37.
Jacobs J, Zelmann R, Jirsch J, Chander R, Châtillon CE, Dubeau F, et al. High frequency oscillations (80-500Hz) in the preictal period in patients with focal seizures. Epilepsia. 2009b;50(7):1780–92.
Jacobs J, Zijlmans M, Zelmann R, Chatillon CE, Hall J, Olivier A, et al. High-frequency electroencephalographic oscillations correlate with outcome of epilepsy surgery. Ann Neurol. 2010;67(2):209–20.
Jasper HH. Electroencephalography. In: Penfield W, Erickson TC, editors. Epilepsy and cerebral localization. Springfield, IL: Charles C. Thomas; 1941. p. 380–454.
Jasper H, Pertuisset B, Flanigin H. EEG and cortical electrograms in patients with temporal lobe seizures. AMA Arch Neurol Psychiatry. 1951;65(3):272–90.
Jefferys JG, Haas HL. Synchronized bursting of CA1 hippocampal pyramidal cells in the absence of synaptic transmission. Nature. 1982;300(5891):448–50.
Jefferys JG, de la Prida LM, Wendling F, Bragin A, Avoli M, Timofeev I, et al. Mechanisms of physiological and epileptic HFO generation. Prog Neurobiol. 2012;98(3):250–64. doi:10.1016/j.pneurobio.2012.02.005.
Jirsch JD, Urrestarazu E, LeVan P, Olivier A, Dubeau F, Gotman J. High-frequency oscillations during human focal seizures. Brain. 2006;129(6):1593–608.
Jiruska P, Csicsvari J, Powell AD, Fox JE, Chang W-C, Vreugdenhil M, et al. High-frequency network activity, global increase in neuronal activity, and synchrony expansion precede epileptic seizures in vitro. J Neurosci. 2010a;30(16):5690–701. doi:10.1523/jneurosci.0535-10.2010.
Jiruska P, Finnerty GT, Powell AD, Lofti N, Cmejla R, Jefferys JG. Epileptic high-frequency network activity in a model of non-lesional temporal lobe epilepsy. Brain. 2010b;133:1380–90.
Jones MS, Barth DS. Spatiotemporal organization of fast (>200 Hz) electrical oscillations in rat Vibrissa/Barrel cortex. J Neurophysiol. 1999;82(3):1599–609.
Jones MS, Barth DS. Effects of bicuculline methiodide on fast (>200Hz) electrical oscillations in rat somatosensory cortex. J Neurophysiol. 2002;88(2):1016–25.
Jones MS, MacDonald KD, Choi B, Dudek FE, Barth DS. Intracellular correlates of fast (>200 Hz) electrical oscillations in rat somatosensory cortex. J Neurophysiol. 2000;84:1505–18.
Kandel A, Buzsaki G. Cellular-synaptic generation of sleep spindles, spike-and-wave discharges, and evoked thalamocortical responses in the neocortex of the rat. J Neurosci. 1997;17(17): 6783–97.
Kaufman PY. Electrical phenomena in the cerebral cortex (in Russian). Oborz Psikhiat Nevrol eksper Psikol. 1912;7–8(403–424):513–35.
Khosravani H, Mehrotra N, Rigby M, Hader WJ, Pinnegar CR, Pillay N, et al. Spatial localization and time-dependant changes of electrographic high frequency oscillations in human temporal lobe epilepsy. Epilepsia. 2008;50(4):605–16.
Klausberger T, Magill PJ, Marton LF, Roberts JDB, Cobden PM, Buzsaki G, et al. Brain-state and cell-type specific firing of hippocampal interneurons in vivo. Nature. 2003;42:844–8.
Kobayashi K, Jacobs J, Gotman J. Detection of changes of high-frequency activity by statistical time-frequency analysis in epileptic spikes. Clin Neurophysiol. 2009;120(6):1070–7.
Kohling R, Staley K. Network mechanisms for fast ripple activity in epileptic tissue. Epilepsy Res. 2011;97(3):318–23. doi:10.1016/j.eplepsyres.2011.03.006.
Kudrimoti HS, Barnes CA, McNaughton BL. Reactivation of hippocampal cell assemblies: effects of behavioral state, experience, and EEG dynamics. J Neurosci. 1999;19(10):4090–101.
Le Van Quyen M, Bragin A, Staba R, Crepon B, Wilson CL, Engel Jr J. Cell type-specific firing during ripple oscillations in the hippocampal formation of humans. J Neurosci. 2008;28(24): 6104–10.
Le Van Quyen M, Staba R, Bragin A, Dickson C, Valderrama M, Fried I, et al. Large-scale microelectrode recordings of high-frequency gamma oscillations in human cortex during sleep. J Neurosci. 2010;30(23):7770–82. doi:10.1523/JNEUROSCI.5049-09.2010.
Levesque M, Bortel A, Gotman J, Avoli M. High-frequency (80–500 Hz) oscillations and epileptogenesis in temporal lobe epilepsy. Neurobiol Dis. 2011;42(3):231–41. doi:S0969-9961(11)00008-8 [pii] 10.1016/j.nbd.2011.01.007.
Lieb JP, Woods SC, Siccardi A, Crandall PH, Walter DO, Leake B. Quantitative analysis of depth spiking in relation to seizure foci in patients with temporal lobe epilepsy. Electroencephalogr Clin Neurophysiol. 1978;44:641–63.
Lieb JP, Joseph JP, Engel Jr J, Walker J, Crandall PH. Sleep state and seizure foci related to depth spike activity in patients with temporal lobe epilepsy. Electroencephalogr Clin Neurophysiol. 1980;49(5–6):538–57.
Mari F, Zelmann R, Andrade-Valenca L, Dubeau F, Gotman J. Continuous high-frequency activity in mesial temporal lobe structures. Epilepsia. 2012;53(5):797–806. doi:10.1111/j.1528-1167.2012.03428.x.
Menendez de la Prida L, Trevelyan AJ. Cellular mechanisms of high frequency oscillations in epilepsy: on the diverse sources of pathological activities. Epilepsy Res. 2011;97(3):308–17. doi:10.1016/j.eplepsyres.2011.02.009.
Murthy VN, Fetz EE. Coherent 25- to 35-Hz oscillations in the sensorimotor cortex of awake behaving monkeys. Proc Natl Acad Sci U S A. 1992;89(12):5670–4.
Nadasdy Z, Hirase H, Czurko A, Csicsvari J, Buzsaki G. Replay and time compression of recurring spike sequences in the hippocampus. J Neurosci. 1999;19(21):9497–507.
Nariai H, Matsuzaki N, Juhasz C, Nagasawa T, Sood S, Chugani HT, et al. Ictal high-frequency oscillations at 80–200 Hz coupled with delta phase in epileptic spasms. Epilepsia. 2011a;52(10):e130–4. doi:10.1111/j.1528-1167.2011.03263.x.
Nariai H, Nagasawa T, Juhasz C, Sood S, Chugani HT, Asano E. Statistical mapping of ictal high-frequency oscillations in epileptic spasms. Epilepsia. 2011b;52(1):63–74. doi:10.1111/j.1528-1167.2010.02786.x.
Niedermeyer E. Historical aspects. In: Niedermeyer E, Lopes da Silva F, editors. Electroencephalography: basic principles, clinical applications, and related field. Baltimore: Williams & Wilkins; 1993. p. 1–14.
Nir Y, Staba RJ, Andrillon T, Vyazovskiy VV, Cirelli C, Fried I, et al. Regional slow waves and spindles in human sleep. Neuron. 2011;70(1):153–69. doi:10.1016/j.neuron.2011.02.043.
Ochi A, Otsubo H, Donner EJ, Elliott I, Iwata R, Funaki T, et al. Dynamic changes of ictal high-frequency oscillations in neocortical epilepsy: using multiple band frequency analysis. Epilepsia. 2007;48(2):286–96.
Ogren JA, Wilson CL, Bragin A, Lin JJ, Salamon N, Dutton RA, et al. Three dimensional surface maps link local atrophy and fast ripples in human epileptic hippocampus. Ann Neurol. 2009;66(6):783–91.
O'Keefe J, Nadel J. The Hippocampus as a Cognitive Map. Oxford: Clarendon Press; 1978.
Penfield W. The epilepsies: with a note on radical therapy. N Engl J Med. 1939;221(6):209–18.
Pravdich-Neminsky WW. An experiment in the recording of electrical phenomena in the brain of mammals. Zbl Physiol. 1913;27:957–60.
RamachandranNair R, Ochi A, Imai K, Benifla M, Akiyama T, Holowka S, et al. Epileptic spasms in older pediatric patients: MEG and ictal high-frequency oscillations suggest focal-onset seizures in a subset of epileptic spasms. Epilepsy Res. 2008;78(2–3):216–24.
Roopun AK, Simonotto JD, Pierce ML, Jenkins A, Nicholson C, Schofield IS, et al. A nonsynaptic mechanism underlying interictal discharges in human epileptic neocortex. Proc Natl Acad Sci U S A. 2010;107(1):338–43.
Sammaritano M, Gigli GL, Gotman J. Interictal spiking during wakefulness and sleep and the localization of foci in temporal lobe epilepsy. Neurology. 1991;41:290–7.
Schevon CA, Trevelyan AJ, Schroeder CE, Goodman RR, McKhann Jr G, Emerson RG. Spatial characterization of interictal high frequency oscillations in epileptic neocortex. Brain. 2009;132(11):3047–59. doi:10.1093/brain/awp222.
Schmitz D, Schuchmann S, Fisahn A, Draguhn A, Buhl EH, Petrasch-Parwez E, et al. Axo-axonal coupling. a novel mechanism for ultrafast neuronal communication. Neuron. 2001;31(5): 831–40.
Shao LR, Dudek FE. Changes in mIPSCs and sIPSCs after kainate treatment: evidence for loss of inhibitory input to dentate granule cells and possible compensatory responses. J Neurophysiol. 2005;94(2):952–60. doi:10.1152/jn.01342.2004.
Siapas AG, Wilson MA. Coordinated interactions between hippocampal ripples and cortical spindles during slow-wave sleep. Neuron. 1998;21:1123–8.
Singer W. Synchronization of cortical activity and its putative role in information processing and learning. Annu Rev Physiol. 1993;55:349–74.
Skaggs WE, McNaughton BL, Permenter M, Archibeque M, Vogt J, Amaral D, et al. EEG sharp wave and sparse ensemble unit activity in the macaque hippocampus. J Neurophysiol. 2007;98:898–910.
Spencer SS, Guimaraes P, Katz A, Kim J, Spencer DD. Morphological patterns of seizures recorded intracranially. Epilepsia. 1992a;33(3):537–45.
Spencer SS, Kim J, Spencer DD. Ictal spikes: a marker of specific hippocampal cell loss. Electroencephalogr Clin Neurophysiol. 1992b;83(2):104–11.
Staba RJ. Normal and pathologic high-frequency oscillations. In: Noebels JL, Avoli M, Rogawski MA, Olsen RW, Delgado-Escueta AV, editors. Jasper’s basic mechanisms of the epilepsies. 4th ed. Bethesda, MD: National Center for Biotechnology Information (USA); 2012.
Staba RJ, Wilson CL, Bragin A, Fried I, Engel Jr J. Quantitative analysis of high-frequency oscillations (80–500 Hz) recorded in human epileptic hippocampus and entorhinal cortex. J Neurophysiol. 2002a;88(4):1743–52.
Staba RJ, Wilson CL, Bragin A, Fried I, Engel Jr J. Sleep states differentiate single neuron activity recorded from human epileptic hippocampus, entorhinal cortex, and subiculum. J Neurosci. 2002b;22(13):5694–704. doi:20026532.
Staba RJ, Wilson CL, Fried I, Engel Jr J. Single neuron burst firing in the human hippocampus during sleep. Hippocampus. 2002c;12(6):724–34. doi:10.1002/hipo.10026.
Staba RJ, Wilson CL, Bragin A, Jhung D, Fried I, Engel J. High-frequency oscillations recorded in human medial temporal lobe during sleep. Ann Neurol. 2004;56:108–15.
Staba RJ, Frighetto L, Behnke EJ, Mathern GW, Fields TA, Bragin A, et al. Increased fast ripple to ripple ratios correlate with reduced hippocampal volumes and neuron loss in temporal lobe epilepsy patients. Epilepsia. 2007;48(11):2130–8.
Staba RJ, Ekstrom AD, Suthana NA, Burggren A, Fried I, Engel Jr J, et al. Gray matter loss correlates with mesial temporal lobe neuronal hyperexcitability inside the human seizure-onset zone. Epilepsia. 2011;53(1):25–34. doi:10.1111/j.1528-1167.2011.03333.x.
Steriade M, Nunez A, Amzica F. A novel slow (<1 Hz) oscillation of neocortical neurons in vivo: depolarizing and hyperpolarizing components. J Neurosci. 1993;13(8):3252–65.
Sullivan D, Csicsvari J, Mizuseki K, Montgomery S, Diba K, Buzsaki G. Relationships between hippocampal sharp waves, ripples, and fast gamma oscillation: influence of dentate and entorhinal cortical activity. J Neurosci. 2011;31(23):8605–16. doi:10.1523/JNEUROSCI.0294-11.2011
Talairach J, David M, Tournoux P. L'exploration chirurgicale stereotaxique du lobe temporal dans l'epilepsie temporale. Paris: Mason; 1958.
Traub RD, Schmitz D, Jefferys JG, Draguhn A. High-frequency population oscillations are predicted to occur in hippocampal pyramidal neuronal networks interconnected by axoaxonal gap junctions. Neuroscience. 1999;92(2):407–26.
Traub RD, Whittington MA, Buhl EH, LeBeau FE, Bibbig A, Boyd S, et al. A possible role for gap junctions in generation of very fast EEG oscillations preceding the onset of, and perhaps initiating, seizures. Epilepsia. 2001;42(2):153–70.
Urrestarazu E, Chander R, Dubeau F, Gotman J. Interictal high-frequency oscillations (100–500 Hz) in the intracerebral EEG of epileptic patients. Brain. 2007;130(9):2354–66.
Wierzynski CM, Lubenov EV, Gu M, Siapas AG. State-dependent spike-timing relationships between hippocampal and prefrontal circuits during sleep. Neuron. 2009;61(4):587–96.
Wieser HG, Bancaud J, Talairach J, Bonis A, Szikla G. Comparative value of spontaneous and chemically and electrically induced seizures in establishing the lateralization of temporal lobe seizures. Epilepsia. 1979;20(1):47–59.
Worrell G. High-frequency oscillations recorded on scalp EEG. Epilepsy Curr. 2012;12(2):57–8. doi:10.5698/1535-7511-12.2.57.
Worrell GA, Parish L, Cranstoun SD, Jonas R, Baltuch G, Litt B. High-frequency oscillations and seizure generation in neocortical epilepsy. Brain. 2004;127(Pt 7):1496–506.
Worrell GA, Gardner AB, Stead SM, Hu S, Goerss S, Cascino GJ, et al. High-frequency oscillations in human temporal lobe: simultaneous microwire and clinical macroelectrode recordings. Brain. 2008;131(4):928–37.
Worrell GA, Jerbi K, Kobayashi K, Lina JM, Zelmann R, Le Van Quyen M. Recording and analysis techniques for high-frequency oscillations. Prog Neurobiol. 2012;98(3):265–78. doi:10.1016/j.pneurobio.2012.02.006.
Wu JY, Sankar R, Lerner JT, Matsumoto JH, Vinters HV, Mathern GW. Removing interictal fast ripples on electrocorticography linked with seizure freedom in children. Neurology. 2010;75(19):1686–94. doi:10.1212/WNL.0b013e3181fc27d0.
Ylinen A, Bragin A, Nadasdy Z, Jando G, Szabo I, Sik A, et al. Sharp wave-associated high-frequency oscillation (200Hz) in the intact hippocampus: network and intracellular mechanisms. J Neurosci. 1995;15(1):30–46.
Zelmann R, Mari F, Jacobs J, Zijlmans M, Dubeau F, Gotman J. A comparison between detectors of high frequency oscillations. Clin Neurophysiol. 2012;123(1):106–16. doi:10.1016/j.clinph.2011.06.006.
Zijlmans MM, Jacobs JM, Zelmann RM, Dubeau FM, Gotman JP. High-frequency oscillations mirror disease activity in patients with epilepsy. Neurology. 2009;72(11):979–86.
Zijlmans M, Jacobs J, Kahn YU, Zelmann R, Dubeau F, Gotman J. Ictal and interictal high frequency oscillations in patients with focal epilepsy. Clin Neurophysiol. 2011;122(4):664–71. doi:10.1016/j.clinph.2010.09.021.
Acknowledgments
The author would like to thank Dr. Jerome Engel, Jr. for his helpful comments in reviewing this manuscript. The author is supported by NINDS RO1 071048 & 33310.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Staba, R.J. (2013). Pathological Oscillations in the Pharmacoresistant Epileptic Brain. In: Rocha, L., Cavalheiro, E. (eds) Pharmacoresistance in Epilepsy. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-6464-8_3
Download citation
DOI: https://doi.org/10.1007/978-1-4614-6464-8_3
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-6463-1
Online ISBN: 978-1-4614-6464-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)