
Abstract
Primary malignancy of the ovary is fortunately a relatively uncommon condition. In 2011, however, more than 20,000 new cases will likely be diagnosed. Ovarian cancer has a poor reputation for survivorship: nearly three-quarters of all diagnosed patients succumb to the disease, distinguishing it as the most lethal gynecologic malignancy. These statistics largely reflect the clinicopathologic course of the most common type of ovarian cancer, epithelial ovarian cancer, which accounts for more than 80 % of primary cases. However, ovarian cancer may also arise from the germ cells, ovarian stroma, and other supporting tissues; expected survivorship in such cases is generally more favorable as a result of the early stage at diagnosis and the high degree of chemotherapy and radiotherapy sensitivity, when adjuvant therapy is recommended. Generally, younger women with ovarian cancer have a proliferative but noninvasive element designated as “low malignant potential” or “borderline” epithelial ovarian tumor. Clearly distinguishing the individual risk factors and therapeutic options for these subtypes is important, given their occurrence in women of reproductive potential and unique natural history.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Ovarian Cancer
- Epithelial Ovarian Cancer
- Germ Cell Tumor
- Cytoreductive Surgery
- Gynecologic Oncology Group
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Primary malignancy of the ovary is fortunately a relatively uncommon condition. In 2011, however, more than 20,000 new cases will likely be diagnosed. Ovarian cancer has a poor reputation for survivorship: nearly three-quarters of all diagnosed patients succumb to the disease, distinguishing it as the most lethal gynecologic malignancy. These statistics largely reflect the clinicopathologic course of the most common type of ovarian cancer, epithelial ovarian cancer, which accounts for more than 80% of primary cases. However, ovarian cancer may also arise from the germ cells, ovarian stroma, and other supporting tissues; expected survivorship in such cases is generally more favorable as a result of the early stage at diagnosis and the high degree of chemotherapy and radiotherapy sensitivity, when adjuvant therapy is recommended. Generally, younger women with ovarian cancer have a proliferative but noninvasive element designated as “low malignant potential” or “borderline” epithelial ovarian tumor. Clearly distinguishing the individual risk factors and therapeutic options for these subtypes is important, given their occurrence in women of reproductive potential and unique natural history.
Risk factors for epithelial ovarian carcinoma are well established. Age is the strongest patient-related risk factor. Overall, an estimated 1 in 70 women will develop ovarian cancer in their lifetime, with age-specific incidence peaking at 75–80 years of age. This is especially startling considering the aging population in the United States. The second-strongest risk factor is a family history of ovarian and/or breast cancer. Women who are heterozygous for mutations of either BRCA1 or BRCA2 have an estimated lifetime risk of 16–60%. Other risk factors associated with increased risk include nulliparity, involuntary infertility, early menarche, and late menopause. Interestingly, oral contraceptive use, pregnancy, lactation, and tubal ligation are associated with reduced risk. Collectively, on the basis of these observations, the investigation into the etiology of this disease has been focused on factors governing ovulation in the adnexa.
Although the exact process of malignant transformation is not known and is likely not a solitary event, three interrelated theories have been proposed to explain the epidemiological observations. The first posits that incessant ovulation leads to repetitive wounding of the ovarian surface epithelium and generates cellular proliferation in postovulatory repair. Such events could increase the probability of accumulated genomic abnormalities. In addition, this cyclic reparative process is believed to generate ovarian epithelial inclusion cysts, whose epithelia undergo carcinogenic transformation in an environment of aberrant autocrine and paracrine growth factor stimulation. Genomic profiling of these cells has demonstrated that they differ significantly from surface epithelia, and although not overtly phenotypically malignant, they express many factors associated with the cancer genotype.
A second theory postulates that surges of pituitary gonadotropins at ovulation and persistently high concentrations after menopause stimulate surface epithelial cells, which result in accumulation of genetic changes and carcinogenesis.
The third theory, supported by observations of increased risk associated with endometriosis, pelvic inflammatory disease, mumps, and talc or asbestos exposure, is associated with factors governing the inflammatory response. Changes in the redox potential in the setting of ovulation and surface-epithelium repair might account for accumulation of genetic injury promoting cancer transformation. Since the inflammation-like setting in which ovulation occurs is dependent on cyclooxygenase-2 (COX2), this theory lends support to the exploration of the chemopreventive potential of COX2 inhibitors.
Historical Perspective
When MD Anderson opened its doors in 1944, few diagnostic tools or therapeutic modalities were available for the treatment of ovarian cancer. Primary surgery was rather primitive; the aggressive and ultraradical surgical approaches to the treatment of ovarian cancer had not yet evolved. Rather, surgery included possible removal of the ovarian mass(es) without omentectomy or maximum cytoreductive surgery of all gross diseases. The postoperative therapy available from 1944 to approximately 1954 included various radiotherapeutic techniques: intraperitoneal instillation of radioactive gold or chromic phosphate solutions, open-field whole abdominal radiation techniques, or the moving strip technique of delivering whole abdominal radiation. The intraperitoneal techniques were primarily used to control malignant effusions. With these treatments, 5-year survival rates were approximately 65% for stage I, 40% for stage II, 18% for stage III, and 12% for stage IV.
The period between 1955 and 1964 was dominated by alkylating agent chemotherapy, used at MD Anderson for the management of ovarian cancer. The agents used in this treatment included cyclophosphamide, melphalan, chlorambucil, nitrogen mustard, and thio-TEPA. By 1960, early reports indicated objective responses in a high percentage of patients, some of which were dramatic, although drug deaths were also reported. Based on preliminary results, melphalan (l-sarcolysin) was selected as the alkylating agent worthy of further clinical trials.
By 1960, MD Anderson physicians were treating women with ovarian cancer with surgery, irradiation, and chemotherapy in various sequences. Response rates to chemotherapy were generally higher than 50%, and control of malignant effusions was noted. Treatment guidelines that had evolved by this time included the following: (1) Total abdominal hysterectomy and bilateral salpingo-oophorectomy was used if surgically feasible; the omentum was removed only if gross tumor was present. (2) For stage I disease, surgery was used, followed by abdominal strip irradiation. (3) For stages II and III with no tumor implants larger than 2 cm, surgery was used, followed by abdominal strip irradiation with a pelvic boost. (4) For cases with tumor implants larger than 3 cm and/or ascites, chemotherapy with melphalan was administered postoperatively. For patients who had a good response, abdominal strip irradiation was then administered. In addition, during this era, second-look surgery after a designated number of chemotherapy cycles was routinely performed to assess response. For patients who developed progressive disease on melphalan, 5-fluorouracil was occasionally used as second-line chemotherapy. Overall, however, it was difficult to evaluate whether chemotherapy improved survival.
By the mid-1960s, second-look surgery after chemotherapy had become standard. However, only about 12% of patients receiving chemotherapy were candidates for this procedure; the remainder generally developed progressive disease during chemotherapy. Combination chemotherapy was introduced into clinical practice at MD Anderson at this time in the form of the AcFuCy regimen—actinomycin-D, 5-fluorouracil, and cyclophosphamide. This combination regimen was initially used for patients who experienced disease progression while taking melphalan, and response rates in early trials ranged from 35% to 40%. However, compared with melphalan, more serious toxic effects were noted; of the first 47 patients so treated, 6 experienced serious toxic effects, and 3 died of drug complications.
Throughout the mid- to late-1960s, little progress was made. Furthermore, because the options for treatment were extremely limited, all subtypes of ovarian cancer—epithelial tumors, malignant germ cell tumors, and sex cord-stromal tumors—were treated similarly. As the 1970s approached, the only major advance was seen in a number of patients with disseminated ovarian dysgerminoma who had been treated and cured with surgery followed by postoperative irradiation.
By 1970, a number of advances were on the horizon, the most dramatic being the evolution of treatment for girls and young women with malignant ovarian germ cell tumors [1]. About this time, the combination of vincristine, actinomycin-D, and cyclophosphamide (VAC) was first used for nondysgerminomatous germ cell tumors, resulting in significant improvement in survival rates. For patients with stage I disease, the 5-year survival rates ranged from 85% to 90%, and for those with stage III disease, these 5-year rates were approximately 50%. For patients with sex cord-stromal ovarian tumors, surgery remained the cornerstone of therapy throughout the 1970s. No standard postoperative therapy was established, but for patients with newly diagnosed disseminated disease or those with recurrent disease, common treatments during this era included whole abdominal or pelvic irradiation or combination chemotherapy with either AcFuCy or VAC. By the mid-1970s, single-agent doxorubicin was being investigated as well.
For patients with epithelial ovarian cancers, a number of different strategies and treatments were being studied during the 1970s. In 1970, a randomized clinical trial was initiated for women with stage III epithelial ovarian cancer that compared whole abdominal radiation using the moving strip technique with single-agent melphalan. The results of this trial indicated relatively equivalent outcomes but with different toxicities. Melphalan remained the standard postoperative chemotherapy during most of this period.
Beginning in 1973 and ending in 1980, a series of four contract studies sponsored by the National Cancer Institute were conducted. The initial study, conducted between 1973 and 1974, consisted of a three-arm trial of melphalan vs. 5-fluorouracil vs. hexamethylmelamine. The second trial, conducted between 1974 and 1976, randomized patients to melphalan, hexamethylmelamine, doxorubicin, or the combination of hexamethylmelamine and cyclophosphamide. The third trial, conducted between 1976 and 1978, randomized patients to melphalan, the combination of hexamethylmelamine and cyclophosphamide, cisplatin, or the combination of hexamethylmelamine, doxorubicin, and cyclophosphamide. And the final trial, conducted between 1978 and 1980, randomized patients to either the combination of hexamethylmelamine, doxorubicin, and cyclophosphamide or the combination of melphalan and cisplatin.
The major advance during the 1970s was the introduction of cisplatin, which emerged as the most active drug to date for the treatment of ovarian cancer. The other major advance was the standard use of combination chemotherapy by the end of the 1970s. Starting in the early 1980s, the combination of cisplatin and cyclophosphamide became the standard postoperative regimen, and the standard number of cycles was 12, which was simply extrapolated from the melphalan era.
By the end of the 1970s, primary surgery was becoming more aggressive, according to preliminary reports from Boston. Also during this period, neoadjuvant chemotherapy was beginning to be used selectively for women with extensive metastatic disease, massive malignant effusions, or severe comorbidities.
Also of note in the late 1970s, the combination of vinblastine, bleomycin, and cisplatin (Platinol) (VBP) was introduced for patients with malignant ovarian germ cell tumors, leading to further improvement in sustained remissions approaching 100% for stage I disease and 75% for advanced-stage disease. The VBP combination continued to be used during the early part of the 1980s. For patients with ovarian sex cord-stromal tumors, use of VAC gave way to the new combination of cisplatin, doxorubicin (Adriamycin), and cyclophosphamide (PAC) by the early 1980s.
For postoperative treatment of high-risk early-stage epithelial ovarian cancers and advanced-stage cancers during most of the 1980s, the combination of cisplatin and cyclophosphamide continued to be studied in a series of investigator-initiated trials. By the mid-1980s, the number of cycles was abbreviated to 6. Carboplatin was studied in clinical trials during the 1980s, and by the end of the decade, it was being used primarily as a single agent for patients with recurrent disease.
For patients with malignant ovarian germ cell tumors, by the mid-1980s, etoposide (in the combination chemotherapy regimen bleomycin, etoposide, and cisplatin [Platinol] [BEP]) had replaced vinblastine (in the combination regimen vinblastine, bleomycin, and cisplatin [Platinol] [VBP]) [2]. A major advance during this period was the substitution of postoperative BEP chemotherapy for irradiation in patients with ovarian dysgerminoma. This allowed MD Anderson gynecologic oncologists to much better preserve fertility in young patients. In the 1980s, fertility-sparing surgery had become a treatment standard in these patients. For patients with metastatic sex cord-stromal tumors, a clinical trial focused on BEP was initiated in 1988.
In the 1980s, surgical cytoreduction was becoming progressively more aggressive, with the objective of achieving minimal residual disease. However, by the mid-1980s, second-look surgery was becoming obsolete, primarily because of its lack of clinical benefit.
For patients with epithelial ovarian cancers, primary cytoreductive surgery followed by combination cisplatin and cyclophosphamide chemotherapy continued to be the standard until paclitaxel was introduced into clinical trials in the early 1990s. By the mid-1990s, after the publication of the Gynecologic Oncology Group (GOG) 111 protocol, combined paclitaxel and cisplatin became the new standard [3].
For patients with malignant germ cell tumors or sex cord-stromal tumors, treatment advanced little during this period. With the introduction of paclitaxel, some of the latter patients began to be treated with paclitaxel alone or with combined paclitaxel and cisplatin [4].
By the early 2000s, primary cytoreductive surgery was becoming even more aggressive to achieve minimal residual disease, with diaphragmatic stripping or debulking, a greater frequency of splenectomy, and more common bowel surgery or lymph node debulking. Also during this period, findings from the GOG 158 trial were published, which demonstrated that paclitaxel/carboplatin and paclitaxel/cisplatin were equivalent in terms of efficacy, but a better therapeutic index was reported with the former [5]. As a result, carboplatin replaced cisplatin almost completely as the standard regimen for both epithelial tumors and sex cord-stromal tumors. For epithelial ovarian cancer, this combination remains a standard postoperative therapy.
The MD Anderson Cancer Center Experience
The MD Anderson Tumor Registry data set was derived from 12,411 women who were diagnosed as having ovarian cancer between 1950 and 2004. Of this group, 2,536 women had received no previous treatment for ovarian cancer. After excluding patients who had received treatment elsewhere and those who had multiple primary cancers, 1,823 patients received definitive primary treatment at MD Anderson Cancer Center. Thus, based on consistent referral patterns over the years, the majority of women who had been referred with a diagnosis of ovarian cancer had received some types of previous treatment.
Table 9.1 shows the number of patients treated with definitive primary therapy by time period and stage of disease. As expected, almost 80% of women had advanced-stage (stage III or IV) disease. The computed survival curves represent the clinical outcomes for women who received definitive primary treatment at MD Anderson Cancer Center. Figure 9.1 reveals the overall survival rates for all stages of disease. As noted, during this 60-year period, there has been incremental improvement in 5-year survival (from 13.3% to 48%) and in 10-year survival (from 6.7% to 32.6%) (P < 0.0001).

Overall survival rates for patients with ovarian cancer (1944–2004) (P < 0.0001, log-rank test for trend).
In the following sections, the change in overall survival over time by stage of disease is discussed. Although the data are presented with use of the typical Tumor Registry methodology—categorizing disease into local, regional, and distant—this is somewhat problematical for ovarian cancer. The primary method of determining stage for ovarian cancer has historically been based on findings at primary surgery, and this system has been relatively consistent during the period under study. However, the rigor with which surgical staging has been practiced has changed dramatically. In the early decades, surgical staging for apparent early disease was less than optimal in many instances. Thus, the data for both local disease (stage I) and regional disease (stage II) patients may be somewhat suspect during the first half of the study period.
Survival in Women with Localized Disease
As noted in Fig. 9.2, there is no clear trend in improvement over the study period. There are several possible explanations for this finding. First, the number of patients with localized (stage I) disease is relatively small. Furthermore, the inclusion of all histotypes and histologic grades complicates analysis. For instance, we know that women with low-risk disease—stage I low-grade endometrioid carcinomas, low-grade serous carcinomas, mucinous carcinomas, malignant ovarian germ cell tumors, and granulosa cell tumors—have an excellent prognosis, with a 90% or better 5-year survival rate, whereas those with high-risk disease—stage I high-grade endometrioid or serous carcinomas, or clear cell carcinomas—have a 5-year survival of about 50%. Thus, such a heterogeneous group of tumors does not lend itself to a very meaningful analysis.

Survival rates for patients with local (SEER stage) ovarian cancer (1944–2004) (P = 0.39, log-rank test for trend). Because of the very small number of individuals with local ovarian cancer seen from 1944 to 1954, data from this period were excluded. N.A. not applicable.
Survival in Women with Regional Disease
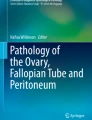
Survival outcome data for women with regional disease—presumably stage II—are presented in Fig. 9.3. It is apparent that overall survival improved markedly during the last two decades of the study period, with 5-year survival rates of 40% or less before the mid-1980s increasing to 77–87% after that. Similarly, 10-year survival rates of 40% or less increased to 68–87%. One possible explanation for this phenomenon is that surgical staging became increasingly accurate during the latter time frame because of better physician education and training. Conversely, in the earlier time frame, patients with apparent regional spread actually had more advanced disease that went undetected because of suboptimal surgical staging.

Survival rates for patients with regional (SEER stage) ovarian cancer (1944–2004) (P < 0.0001, log-rank test for trend). Because of the very small number of individuals with regional ovarian cancer seen from 1944 to 1954, data from this period were excluded. N.A. not applicable.
Survival in Women with Distant Disease
As expected, survival for women with distant or advanced-stage disease was uniformly poor throughout the entire study period (Fig 9.4). However, significant improvement in survival occurred during the last two decades of the study period. Five-year survival rates significantly improved, from less than 14% in the mid-1980s to 21% in the 1985–1994 decade, and then to 35% in the 1995–2004 period. Likewise, 10-year survival rates essentially doubled between the mid-1980s and the last decade of the study period.

Survival rates for patients with distant (SEER stage) ovarian cancer (1944–2004) (P < 0.0001, log-rank test for trend).
Possible explanations for this improvement in outcome for patients with advanced-stage disease include the more widespread practice of aggressive cytoreductive surgery beginning in the 1980s. Additionally, platinum-based combination chemotherapy became the standard postoperative therapy by the mid-1980s, and taxanes were introduced into standard chemotherapy regimens by the mid-1990s.
Current Management Approach
Standard treatment for epithelial ovarian cancer has improved over the past few decades, based on results from randomized trials combined with large-scale descriptive studies. For women with apparent early-stage disease (stages I and II), accurate surgical staging is a major treatment principle. Adjuvant therapy is generally recommended for patients with high-risk disease (stage I high-grade serous and endometrioid tumors, clear cell tumors, and stage II tumors) and consists of taxane/platinum chemotherapy. No postoperative therapy is recommended for those with low-risk disease (stage I low-grade serous and endometrioid tumors and mucinous tumors).
For women with advanced-stage disease, treatment principles consist of maximum primary cytoreductive surgery followed by chemotherapy. For selected patients with serious comorbidities, massive effusions, or extensive disease (e.g., hepatic metastases or extensive upper abdominal disease), neoadjuvant chemotherapy followed by interval cytoreductive surgery is generally recommended. This approach has recently been studied in a European randomized study.
Standard postoperative therapy for advanced-stage patients includes the combination of a taxane (paclitaxel or docetaxel) and carboplatin for six cycles. However, several alternate strategies have been, or are being, studied in randomized clinical trials and are usually considered potential treatment options. Three randomized trials conducted by the GOG have demonstrated enhanced outcome in women with optimal residual disease who received intraperitoneal chemotherapy compared with pure intravenous chemotherapy. Survival improvement was most pronounced in the most recent trial (GOG 172); however, only 42% of women in the intraperitoneal chemotherapy arm were able to complete six cycles, and the toxic effects in terms of neurotoxicity and neutropenia were substantial [6]. Another strategy that has been studied in two randomized trials is the addition of bevacizumab (both concomitantly with chemotherapy and as maintenance therapy); preliminary results appear to be positive, but final reports are not yet available.
For women with advanced-stage disease, maintenance therapy after completion of primary chemotherapy remains an option [7]. One randomized trial demonstrated a progression-free survival advantage for patients who received 12 vs. 3 monthly cycles of paclitaxel, and a follow-up randomized trial is in progress.
For women who develop recurrent disease, the current approach is to categorize them as either platinum-sensitive (treatment-free interval of ≥6 months) or platinum-resistant (treatment-free interval of <6 months). Options for women with platinum-sensitive recurrent disease include combinations of paclitaxel/carboplatin, gemcitabine/platinum, or pegylated liposomal doxorubicin. For those with platinum-resistant disease, treatment options include pegylated liposomal doxorubicin, topotecan, gemcitabine with or without platinum, capecitabine, oral etoposide, hormonal therapy (tamoxifen), docetaxel, or bevacizumab [8]. In addition, for women with platinum-sensitive recurrent disease, secondary cytoreductive surgery has been reported to be potentially beneficial in several retrospective studies and is being studied in multiple randomized clinical trials.
Targeted therapies are a major focus of clinical trials for women with recurrent ovarian cancer. Examples include the use of poly (ADP)-ribose polymerase (PARP) inhibitors in women with BRCA germline mutations, as well as phosphatidylinositol-3 kinase (PI3K)/AKT/mTOR inhibitors and inhibitors of the MAP kinase pathway in women with low-grade serous carcinomas [9, 10]. Concomitantly, separate trials are emerging for women with uncommon subtypes—BRCA germline mutations, low-grade serous carcinomas, clear cell carcinomas, and mucinous carcinomas.
For patients with uncommon histologic types—malignant germ cell tumors and sex cord-stromal tumors—contemporary treatment is quite different. Primary surgery is standard for all patients. For adult patients with all histologic subtypes of malignant germ cell tumors—except stage IA dysgerminoma and stage I, grade 1 immature teratoma—the standard for several years has been postoperative chemotherapy with BEP. However, in the pediatric population, surveillance is being studied as an alternative. Several reports already indicate favorable outcomes with close postoperative surveillance, but further study is warranted, especially for adults.
For patients with sex cord-stromal tumors, primary surgery remains the cornerstone of treatment. For postoperative management, no standard exists. For stage I granulosa cell tumor, no postoperative therapy is recommended. For women with metastatic disease, platinum-based chemotherapy is generally recommended, with BEP or paclitaxel/carboplatin being the two most popular regimens. In addition, patients with stage I poorly differentiated Sertoli–Leydig cell tumors appear to have a poor prognosis, with a relapse rate as high as 60%. Thus, adjuvant chemotherapy may be recommended, although sufficient data indicating a benefit of such are lacking.
Perspective and Future Directions
As the standards for care are methodically assessed, the overarching intent is to extend the lives of our patients. A report from the Surveillance, Epidemiology, and End Results (SEER) program suggests that steady progress is being made in this regard, with years of life gained from treatment nearly doubling between the early 1970s and the 2000s. However, closer examination of these data suggests that the proportion of patients cured of their disease contributes only a small fraction to this statistic, highlighting both the marginal improved efficacy of existing therapy and the urgent need for effective screening and early detection. Nevertheless, the contemporary investigative environment is challenging each of these areas aggressively and with greater statistical rigor.
One particularly promising development is the exponential growth in our understanding of the biological processes of this disease. Concerted efforts to ferret out critically linked processes driving the malignant phenotype have led to the incorporation of novel agents, used both alone and in combination with other agents, such as chemotherapy. The most mature of these currently in use in ovarian cancer is bevacizumab, a chimeric antibody targeting vascular endothelial growth factor A (VEGF-A), which has demonstrated clinical efficacy as a single agent and in combination with chemotherapy in both the recurrent and front-line settings. Several ongoing trials are evaluating its efficacy in combination with various chemotherapy backbones in recurrent disease and in combination with other biological agents. The clinical promise in targeting this pathway for ovarian cancer patients has ushered in a number of new agents that are also in clinical development, including those targeting the recently discovered mechanisms of resistance to VEGF antibody targeting and those focusing on important tumor growth and survivor factors, such as the PI3K family pathway.
Seemingly endless in potential possibilities, this emerging cache of information has enabled the consideration of personalizing treatment to individual tumor characteristics. Numerous challenges abide in this intuitive next step, but at least some inference into the possibility may be realized by reviewing the impact of agents targeting the single-strand DNA repair enzyme, PARP, in patients with germline mutation in BRCA. These patients who develop ovarian cancer generally harbor tumors in which the homologous recombination function from BRCA is impaired, placing greater responsibility on PARP for continued growth. Several PARP inhibitors have entered the clinic, and preliminary evidence supports the hypothesis that these agents are efficacious in this setting; this is because of the inhibitor’s limited toxicity, which is due to the intact function of BRCA in unaffected tissues.
As outlined above, treatment standards for both epithelial and non-epithelial ovarian cancer continue to be refined. MD Anderson continues to play a pivotal role in this progress through its discovery and translation of new therapy options, including the emergence of the therapeutic delivery of non-coding RNA; its expertise in rare tumors of the ovary; its leadership in bringing a global audience to the clinical investigation of these diseases; and its investigative leadership and continued participation in a cooperative group mechanism of investigation.
References
Smith JP, Rutledge JP. Chemotherapy in the treatment of cancer of the ovary. Am J Obstet Gynecol. 1970;107:691–703.
Gershenson DM, Morris M, Cangir A, et al. Treatment of malignant germ cell tumors of the ovary with bleomycin, etoposide, and cisplatin. J Clin Oncol. 1990;8:715–20.
McGuire WP, Hoskins WJ, Brady MF, et al. Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer. N Engl J Med. 1996;334:1–6.
Brown J, Shvartsman HS, Deavers MT, et al. The activity of taxanes in the treatment of sex cord-stromal ovarian tumors. J Clin Oncol. 2004;22:3517–23.
Ozols RF, Bundy BN, Greer BE, et al. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: a Gynecologic Oncology Group study. J Clin Oncol. 2003;21:3194–200.
Armstrong DK, Bundy B, Wenzel L, et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med. 2006;354:34–43.
Herzog TJ, Coleman RL, Markman M, et al. The role of maintenance therapy and novel taxanes in ovarian cancer. Gynecol Oncol. 2006;102:218–25.
Burger RA, Sill MW, Monk BJ, et al. Phase II trial of bevacizumab in persistent or recurrent epithelial ovarian cancer or primary peritoneal cancer: a Gynecologic Oncology Group Study. J Clin Oncol. 2007;25:5165–71.
Fong PC, Boss DS, Yap TA, et al. Inhibition of poly(ADP-ribose) polymerase in tumors from BRCA mutation carriers. N Engl J Med. 2009;361:123–34.
Hennessy BT, Coleman RL, Markman M. Ovarian cancer. Lancet. 2009;374:1371–82.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Coleman, R.L., Gershenson, D.M. (2013). Ovarian Cancer. In: Rodriguez, M., Walters, R., Burke, T. (eds) 60 Years of Survival Outcomes at The University of Texas MD Anderson Cancer Center. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-5197-6_9
Download citation
DOI: https://doi.org/10.1007/978-1-4614-5197-6_9
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-5196-9
Online ISBN: 978-1-4614-5197-6
eBook Packages: MedicineMedicine (R0)