
Abstract
Gonorrhea remains as a significant public health concern with an estimated 88 million new cases per year globally. Gonorrhea is a disease of sexual networks and is most prevalent in youth, men who have sex with men, and the socioeconomically disadvantaged. Highly adaptive through years of co-evolution, gonorrhea has developed multiple ways of evading the human immune system. Although new molecular-based strategies have opened avenues for less invasive testing, education and accessibility issues persist. Novel strategies, including use of the internet and social media, are required to better target high risk groups for education, testing, and treatment. Increasing the availability of youth-friendly health services will also help foster earlier gonorrhea diagnosis and management. The inappropriate and overuse of antibiotics and propensity of gonococcus for mutation has led to growing microbe resistance. Treatment failures now include both oral and intravenous formulations of third generation cephalosporins; key front line recommended gonococcal treatment in many countries. With treatment options dwindling, the need for better preventative strategies has never been more important. This overview highlights some of the major aspects of gonococcal infection, including the epidemiology of the disease with an emphasis on sexual networks, new diagnostic techniques, treatment options in the face of evolving gonococcal resistance, and notes potential new preventative strategies.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Transmitted Infection
- Sexual Network
- Nucleic Acid Amplification Test
- Gonococcal Infection
- Neisseria Species
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
19.1 Introduction
Neisseria gonorrhoeae has been a sexually transmitted scourge of humans for eons. The relationship has been so long and so enduring that a piece of human DNA became entwined with the microbe’s genome many millennia ago [1]. Unfortunately, gonorrhea continues to cause significant morbidity and mortality worldwide. A disease largely of the disadvantaged, gonorrhea disproportionately affects inhabitants of developing countries and those of lower social economic status, globally. Worldwide, the gonorrhea epidemic is primarily focused among young people due to a variety of social and behavioural factors shared by this group.
While little has changed in the clinical presentation of gonorrhea, our understanding of organism pathogenesis and the availability of diagnostic tools has grown. Additionally, multi-drug resistant gonococcal strains have now emerged. Without alternative antibiotics or a candidate vaccine in the pipeline, gonorrhea may soon become untreatable [2, 3]. With dwindling therapeutic options, new prevention strategies based on an understanding of sexual networks and utilizing youth-friendly information modalities, need to be pursued.
Rather than an exhaustive review, the purpose of this article is to supply a snapshot of gonorrhea in the world today with an emphasis on young people living in developed countries. Key topics explored include current epidemiology, risk factors for transmission, benefits and limitations of new diagnostic modalities, treatment options in the context of growing antimicrobial resistance, and novel preventative strategies .
19.2 Gonococcal Pathogenesis
Through the co-evolution of N. gonorrhea and humans, gonococcus has become highly adept at evading host immune defenses. These pathogenic mechanisms have important clinical correlates in terms of infectivity, disease manifestations, development of antibiotic resistance , and the potential for vaccine development.
A number of characteristics are known to contribute to the virulence of N. gonorrhoeae including pili, porin protein, opacity proteins, lipooligosaccharides, reduction modifiable proteins, IgA proteases, and iron- or oxygen-repressible proteins . A detailed discussion of these gene products and molecular systems are available elsewhere [4, 5]. While some gonococcal pathogenic mechanisms are well described, others remain unclear. For example, the recently discovered horizontal gene transfer between humans and N. gonorrhea is currently of unknown significance, beyond its affirmation of the extended length of time the two have co-existed [1].
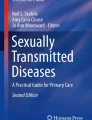
Acquired through sexual contact, N. gonorrhea establishes infection of the urogenital tract by interacting with non-ciliated epithelial cells (Fig. 19.1). The molecular mechanisms responsible for gonococcal infection appear to differ between males and females. For example, invasion of female but not male urogenital cells is facilitated by cervix-specific CR3 complement receptors . Male urethral epithelial cells do not express these receptors. CR3 mediated invasion, in turn, is associated with asymptomatic cervicitis, perhaps explaining the higher incidence of asymptomatic disease in women than men [6]. The formation of biofilms on cervical cells may also play a role in the pathogenesis of N. gonorrhea in women [7].

Pathogenesis of gonococcal infection [5]. (With kind permission from Springer Science+Busness Media B.V. and M Virji)
After adhering to epithelial cell surfaces, gonococcus is engulfed into cells where it replicates intracellularly within phagocytes. The microbe later exits from the basal surface via exocytosis and enters the submucosal space. Mucosal epithelial damage and submucosal invasion lead to the influx of neutrophils with the resultant production of purulent material (e.g., “drip”) into the lumen of infected tissues [4]. Both organism-specific factors, including peptidoglycan and lipopolysaccharide, alongside host-related responses, such as phagocyte production of tumor necrosis factor, contribute to tissue damage [5].
While the majority of invading gonococci are ingested and destroyed by neutrophils, a minority escape innate and early adaptive immune responses, thereby, allowing for persistent infection. Infrequently, disseminated infection occurs [8]. Normally, human serum is capable of killing circulating and mucosal gonococci via the activation of complement. However, some gonococcal strains are serum resistant, inducing defective terminal complement deposition. For example, gonococcus is able to bind C4BP, a key inhibitor of the classical pathway, thereby eluding complement-mediated lysis [9].
Recurrent gonococcal infection is the rule rather than exception. Although natural infection prompts antibody production against gonococcal cell wall components, the impact of the humoral immune response tends to be minimal . Antigenic and phase variation of outer gonococcal components, alongside mimicry of host glycolipids, further limits an effective immune response [4, 5, 10] and is a major reason why vaccines developed using traditional techniques have failed. Additionally, interspecies and as well as interstrain genetic exchange within the Neisseria genus continually introduces novel antigenic components [4] including antibiotic resistance genes.
19.3 Epidemiology
Gonorrhea remains a significant public health concern worldwide. An estimated 88 million people are newly infected on a yearly basis with the majority of cases occurring in the developing world [11]. The reported rate in the developing world is about 20 times the rate in industrialized countries (Table 19.1). Gonorrhea is the second most commonly reported bacterial sexually transmitted infection in many industrialized countries including the United States (US), Canada, and the United Kingdom (UK) [12, 13, 14]. While prevalence and incidence statistics are available for many countries, the current methods of data collection have limitations and likely substantially underestimate infection rates [15, 16, 17].
In general, surveillance data tends to be more robust from countries with national reporting systems such as those found in many industrialized countries including the US, Canada, the UK, Australia, and the Netherlands [18]. For example, the Gonococcal Isolate Surveillance Project (GISP) serves as a sentinel surveillance system in the US, monitoring gonococcal antimicrobial susceptibilities though ongoing testing of a select segment of the US population. Additionally, a number of European countries share a surveillance program called the European Gonococcal Antimicrobial Surveillance Programme (EURO-GASP), part of a broader European STI surveillance network known as the European Surveillance of Sexually Transmitted Infections (ESSTI). A number of these national and multinational systems collect detailed epidemiological and behavioural information in addition to antimicrobial resistance data [19] , aiding in informing preventative as well as treatment strategies [20] . Although an important step in the right direction, surveillance systems remain prone to inaccuracies and the paucity of data from developing countries hinders global evaluation of gonococcal rates and assessment of intervention programs [17, 21, 22]. Strengthening of local country data collecting systems and international collaboration are needed to improve surveillance of gonorrhea on a global scale . Table 19.2 compares rates of gonorrhea in selected countries in Europe with Canada and the United States. The variation in reported rates per 100,000 population is quite wide ranging from a low of 0.25 and 1.7 in Croatia and France, respectively, to much higher rates of 56.38, 56.5 and 111.6 in the Russian Federation, Belarus and the US, respectively.
Comprehensive reviews of the historical epidemiology of gonorrhea are available elsewhere [17, 23] . In brief, gonorrhea rates have fluctuated worldwide over the last hundred years. Peaking around the Second World War in the 1940s and during the “sexual liberation” of the late 1960s and early 1970s, declining gonococcal rates were subsequently observed in the US, Canada and many European countries [12, 24, 25]. Following a transient rise in the 1990s and early 2000s, infection rates have since stabilized or declined in some countries but now show resurgence in others. For example, while gonorrhea rates have fallen in the US, they have risen in Canada [12, 14]. High infection rates also persist in many lower-income countries including Eastern Europe, the Western Pacific, Asia, Africa and Latin America [26, 27, 28].
19.4 Risk Groups: Emphasis on Young People & Sexual Networks
The factors needed to sustain a sexually transmitted infection epidemic are summarized by the case-reproduction ratio (Ro) , an equation used to determine the number of new cases generated by an infected person. This ratio is calculated by the following equation: Ro = b CD, where “ b ” indicates the efficiency of transmission, “C” the number and/or rate of sexual partner change, and “D” the average duration of infectivity [29]. When Ro equals one, the infection is endemic and stable. Ro values greater than or less than one reflect increasing or decreasing infection rates, respectively.
Each component of the case-reproduction ratio reflects a variety of sexually transmitted infection risk factors . For example, the efficacy of transmission (“ b ”) is determined, in part, by gonococcal strain subtype and infectious inoculum [30]. To illustrate the latter, male to female genital-to-genital transmission is more efficient than the reverse (e.g. male to female: 50–70 %; female to male: 20 %), likely due to a higher infectious inoculum in male urethral discharge than vaginal secretions [5, 31, 32]. Host behaviours, such as condom use, also play a role in transmission efficiency (“ b ”) [33, 34, 35].
The variable duration of infectivity (“D”) reflects the time between sexually transmitted infection acquisition and successful treatment or clearance of infection . Gonorrhea is mild or asymptomatic in up to 50 % of infected females and in less than 10 % of infected males [36], delaying or preventing diagnosis, especially in women. Fear of stigmatization, inaccessible diagnostic and treatment services, and therapy noncompliance are other potential reasons for longer periods of infectivity and, hence, increased risk of transmission [17].
The last variable in the case-reproduction ratio, the number and/or rate of sexual partner change (“C”), is self-explanatory. However, this variable is worth exploring further from the standpoint of sexual networks . Long term monogamous sexual relationships are not part of a sexual network. Rather, sexual networks are characterized by core groups of people with frequent partner exchange and high degrees of connectivity [37]. These networks can be remarkably extensive as recently demonstrated by Al-Tayyib & Rietmeijer [38] (Fig. 19.2). Although some sexually transmitted infection cases are detected and treated, infection within the network remains making re-infection probable. Behavioural factors, such as sporadic condom use within the group, promote rapid spread and persistence of sexually transmitted infections [39]. More prevalent in core groups than the general population, gonorrhea is an archetype of sexually transmitted infection transmission and persistence within sexual networks .

Example of an extensive social network among young people in Denver, US [38]. (With permission from A.A. Al-Tayyib)
Teenagers and young adults, due to a combination of social, behavioural and biological factors , are disproportionately affected by sexually transmitted infections [40]. Along with men who have sex with men, street youth, intravenous drug users, and persons in correctional facilities, young people often fit the “core group criteria” of sexual networks [23, 41] . Contributing teen behaviours include multiple concurrent sexual partners [39, 42–47], sequential sexual partnerships of limited duration [40, 48, 49], failure to use barrier protection and the mixing of alcohol, drugs and risky sexual activity [47]. Additionally, the smaller introitus and cervical immaturity of young females confers a biological risk of sexually transmitted infection acquisition [50].
The 2009 National Youth Risk Behavior Survey in the United States reported that 46 % of grade 9 (ages 14–15 years) to grade 12 (ages 17–18 years) students had engaged in sexual intercourse at least once, 34.2 % were currently sexually active (i.e., had sexual intercourse with at least one person during the 3 months prior to the study), and 13.8 % had had sex with ³ 4 people. Of the 34.2 % of currently sexually active teens, 61.1 % reported condom use by themselves or their partner and 21.6 %, alcohol or drugs before the last sexual intercourse. Of the teens surveyed, 7.4 % reported being forced into sex [47].
Early sexual debut further puts teens at risk [51, 52] with 25 % of young people acquiring their first sexually transmitted infection within a year of first sexual intercourse [49, 53]. Although the 2009 US National Youth Risk Behavior Survey showed improvement in some measures as compared to a decade ago (e.g., 2000—49.9 % reported ever having had sexual intercourse; 16.2 %, having ³ 4 lifetime sexual partners) [54], the sexual behaviours of young people continue to put them at increased risk for sexually transmitted infections including gonorrhea .
Gonorrhea rates also vary by racial or ethnic group and by geographic region most likely reflecting background differences in rates within sexual networks . For example, in the US and UK, black ethnic population groups have disproportionately higher gonococcal infection rates [12, 19] than whites. In the US, the gonorrhea rate is 20 times higher in blacks than whites with young black women bearing the heaviest gonorrhea burden [12] . Geographically, gonorrhea rates vary by population density and region. For example, gonorrhea is disproportionately concentrated in London in the UK, and in the South in the US [12, 13].
19.5 Clinical Presentation
The clinical presentation of gonorrhea is well-described elsewhere [55] . Rather than provide a comprehensive overview, only a brief description of infectious manifestations in teenagers and young adults is provided below. A discussion of gonorrhea in neonates and young children is available elsewhere [56].
19.5.1 Genitourinary Infection
As noted above, gonococcal infection in males is asymptomatic in 5–10 % of cases. Symptomatic males most commonly suffer from urethritis , which begins 2–7 days after exposure. Complications are rare in men. Gonorrhea in females, on the other hand, is mild or asymptomatic in up to 50 % of cases. Symptomatic females usually develop cervicitis, typically 3–5 days after exposure. Complications are more common in women than men with the most feared, pelvic inflammatory disease , occurring in 10–20 % of untreated females [57]. Additionally, gonococcal infection during pregnancy poses a risk to both the mother and unborn child [58, 59].
19.5.2 Pharyngeal & Anorectal Gonorrhea
Pharyngeal gonorrhea results from orogenital contact. Although historically considered to only affect men who have sex with men and commercial sex workers, the increasing rates of orogenital sex amongst heterosexual couples has escalated their risk [60]. Pharyngeal gonorrhea is usually clinically silent, tends to resolve spontaneously within 10–12 weeks, and rarely causes complications [59]. However, pharyngeal infection, if not treated, has been linked to disseminated gonorrhea and serves as a potential reservoir for transmission to sexual partners [60]. Additionally, through the genetic exchange between commensal and gonococcal Neisseria species, gonococcal infection of the pharynx facilitates antimicrobial resistance transfer [61].
In males, anorectal gonorrhea occurs almost exclusively from receptive rectal intercourse amongst men who have sex with men. In women, transmural inoculation from vaginal secretions is likely the most common source [62]. Like pharyngeal gonorrhea, anorectal infection is asymptomatic in the majority of cases but serves as an infectious reservoir for transmission to sexual partners [63], a site for microbial genomic exchange and for persistence within sexual networks .
19.5.3 Disseminated Gonococcal Infection (DGI)
Disseminated disease requires bloodstream invasion from local sites of gonococcal infection. However, signs and symptoms of mucous membrane involvement rarely precede disseminated infection. Disseminated gonococcal infection is a rare entity, estimated to occur in only 1–3 % of infected adult patients [59]. Although usually clinically silent, disseminated gonococcal infection can be symptomatic, typically causing mild to moderate illness. Even without treatment, symptoms usually resolve in a matter of days and long-term sequelae are atypical [64]. Infrequently, disseminated gonococcal infection can cause fulminant sepsis and death [65]. Disseminated disease is also associated with infection at other sites, most commonly septic arthritis. Less frequently, disseminated gonococcal infection presents as a triad of tenosynovitis, dermatitis and polyarthralgias without purulent arthritis [64]. Given an association between disseminated gonococcal infection and terminal complement deficiency, patients with recurrent disseminated disease should be tested for immune deficiency [66].
Other forms of disseminated gonococcal disease, including osteomyelitis, meningitis, endocarditis and myocarditis, are infrequently reported [59, 61].
19.6 Diagnosis
19.6.1 Screening
Screening decisions should be based on a solid understanding of epidemiology of gonorrhea . Given that gonorrhea rates vary considerably within and between populations, mass screening for this pathogen has largely been abandoned [23]. While some countries limit testing to symptomatic individuals and their sexual contacts, most recognize the need to extend gonorrhea testing to subpopulations with high prevalence rates and/or risk factors. For example, numerous organizations in the US support routine testing of pregnant women with risk factors, men who have sex with men, and adolescent patients [67]. Less agreement has been reached over screening groups with low prevalence rates but high risk of asymptomatic, complicated infections (e.g., low risk pregnant women). Additionally, optimal screening intervals for at risk populations and the need for post-treatment testing requires further research.
Certainly, both the potential benefits and harms of screening must be considered prior to implementing a testing program. In favor of screening is the identification and subsequent treatment of asymptomatic patients, thereby, preventing disease complications and infectious spread to others (i.e., decreasing the prevalence in a sexual network). However, screening tools must be carefully selected, considering both the sensitivity and specificity of the test, alongside its applicability to the population under investigation [68]. The inverse relationship between disease prevalence and false positivity rate is a well recognized statistical phenomenon. In the context of sexually transmitted infection testing, false positive results are expected to cause needless patient anxiety, potential partner discord, and increase unnecessary antibiotic use. Hence, the limitations of a screening test must always be considered prior to its application.
Given the rise of multi-resistant gonorrhea (see below), the role of screening as a secondary prevention strategy may need to be reevaluated.
19.6.2 Microbiology/Diagnosis
Table 19.3 compares two current microbiological tests, culture and nucleic acid amplification tests (molecular testing), for gonorrhea, noting specimen transport requirements, potential for self collection, rapidity of test, necessary equipment, availability of antibiotic sensitivity testing, relative cost and expertise needed, and ease of coincident chlamydia detection.
19.6.2.1 Diagnosis of Genitourinary Gonorrhea
19.6.2.1.1 Gram Stain
Gram stain is a rapid tool for diagnosis of gonococcal urethritis in symptomatic men . N. gonorrhoeae characteristically appear as Gram-negative intracellular diplococci within polymorphonuclear cells. The coupling of opposing flattened bacterial surfaces produces the organism’s distinctive “kidney bean” shape. In men with symptomatic urethritis , Gram stain has comparable specificity to culture [69]. While a presumptive diagnosis of gonorrhea in this demographic can be made on the basis of Gram stain alone, a negative result does not rule out gonococcal infection [59]. Furthermore, nonurethral specimens from nonsterile sites are not appropriate for Gram stain due to poor specificity.
19.6.2.1.2 Culture
Culture remains an option for gonorrhea testing from genital sites. The appropriate site(s) for specimen collection depend on patient age, gender, and sexual practices as well as clinical manifestations of infection. While the primary site of culture collection from women has been the endocervix, alternative sample sites include the urethra and vagina. Vaginal or urine specimens are recommended for women post-hysterectomy and for prepubertal girls. The primary collection site from men is the urethra. Rectal and pharyngeal swabs should be collected in patients who have engaged in oral and anal intercourse, respectively. Conjunctival cultures should be sent in the cases of suspected gonorrhea ophthalmia . Lastly, blood, synovial, and cerebrospinal fluid specimens should be considered in suspected disseminated disease.
Culture is performed on selective media and incubated in carbon dioxide at 35–37 °C for up to 72 h. Colonies are generally heterogeneous in appearance reflecting variations in piliation and are both catalase and oxidase positive. A variety of options exist for confirmation including carbohydrate utilization, chromogenic enzyme substrate tests, immunologic methods and deoxyribonucleic acid (DNA) probe confirmation tests. Culture has several advantages including acceptable sensitivity, high specificity, relative low cost, and suitability for a variety of clinical specimens. It does not require the costly instrumentation associated with molecular detection and provides a viable organism for antibiotic susceptibility testing and tracking epidemiological trends . There are, however, multiple disadvantages to culture. It requires more invasive sampling techniques; in particular, urethral swabs for men and endocervical swabs for women. Culture also necessitates strict storage and transportation conditions given that N. gonorrhoeae has specialized growth requirements and is highly susceptible to environmental variations. Lastly, culture takes 24–72 h to produce a definite result.
19.6.2.1.3 Nucleic Acid Amplification Diagnostic Techniques (NAATs)
The first non-culture diagnostic tests were based on the detection of specific gonococcal antigens. Suboptimal performance characteristics and high cost favoured the continued use of culture [69]. Antigen-based tests were subsequently supplanted by nucleic acid amplification tests (NAATs) . Although more expensive than culture, nucleic acid detection methods offer a number of advantages over culture including rapid turnaround time and the ability to detect organisms that are nonviable for culture. NAATs are based on detection of species-specific DNA or ribonucleic acid (RNA) sequences. The enhanced sensitivity of NAATs permits testing on a wider variety of specimen types including urethral swabs, endocervical and vaginal swabs as well as urine. A variety of commercial NAATs, involving different amplification techniques and nucleic acid targets, have been approved for the detection of gonorrhea in most developed countries. While NAATs have been approved for endocervical, urethral, vaginal, and urine specimens, culture has been the standard for pharyngeal and anorectal specimens [70] . However, this situation is in transition as increasing data validates the use of NAATs for non-urogenital sites [71, 72].
NAATs sensitivity and specificity depends upon the amplification of organism-specific nucleic acid sequences. The success of a particular NAAT relates to the choice of target gene. Commercial and in-house NAATs have used a variety of genetic targets including the cryptic plasmid (cppB gene), opa genes, cytosine DNA methyltransferase and the 16SrRNA gene. With the potential exception of urine specimens, NAATs generally offer superior sensitivity to culture, attributable to their ability to produce a positive signal from as little as a single copy of target DNA or RNA [69].
NAATs have replaced culture in many countries as the preferred method of diagnosing gonorrhea from genital sites . Many assays offer the advantage of testing for both gonococcal and chlamydia from a single swab or urine speciman—a benefit for both patients and clinicians. The ability to test less invasive specimens such as urine samples and vaginal swabs has a significant advantage over culture as it improves patient acceptance of testing [73] and provides the additional option of self-collected specimens—which many patients find preferable [74, 75] .
Theoretical limitations to NAAT sensitivity are assay-specific. Interstrain genetic differences may result in false negatives due to variable or absent nucleic acid sequences. Given that gonococcal strain distribution varies geographically and temporally, the performance of NAATs may differ both among and within groups over time. However, in general, commercial assays have targeted very stable genes to minimize this issue. Competitive amplification, whereby targets of lesser concentration fail to amplify in multiplex assays, and the presence of inhibitors may also reduce assay sensitivity [70]. Positive internal controls identify some of these technical limitations. Notably, commercial NAATs do not routinely detect antibiotic resistance genes although these may be future targets .
NAATs typically exhibit high specificity. Interspecies homology within the Neisseria genus [76] and frequent horizontal genetic exchange among Neisseria species [70] are theoretical causes of false positive results. Cross-contamination during processing is a risk that must be controlled for with any NAAT to maintain test specificity. Maintaining high specificity is essential in order to maximize the positive predictive value of the test, particularly in low prevalence populations. New multiplex NAATs , which target multiple genes in a single assay, may provide improved target specificity. Additionally, limiting screening programs to high prevalence populations will maximize the positive predictive value of the utilized test.
19.6.2.2 Diagnosis of Pharyngeal and Rectal Gonorrhea
Cultured pharyngeal and rectal swabs generally have poor sensitivity [60]. Several studies have demonstrated the superior sensitivity of NAATs over culture in detecting pharyngeal and rectal gonococcal infection [71, 73, 77, 78]. In addition, although concerns have been raised regarding cross-reactivity with commensal Neisseria species at extragenital sites, many NAATs have been found to have superior specificity to culture. Ongoing validation of assays for the detection of pharyngeal and rectal gonorrhea will help to minimize potential reservoirs of infection and, secondarily, reduce the development of antimicrobial resistance (pharyngeal gonorrhea). .
19.6.2.3 Diagnosis of Disseminated Gonococcal Infection
The yield from cultures is limited in disseminated gonococcal infections. However, it is prudent to culture all potentially infected areas, including genitourinary, rectal, and pharyngeal sites. The presence of a septic joint should prompt arthrocentesis. Mean synovial fluid leukocyte count in disseminated gonococcal infections is typically around 50,000 cells/mm3 although it can be less than 10,000 cells/mm3 [64]. Synovial fluid gram stain and culture are often negative. However, molecular testing of aspirated joint fluid with 16S rDNA PCR can augment diagnostic yield [79, 80] .
Although blood cultures are negative in 50–75 % of cases, at least two blood specimens should be sent for culture in patients presenting with suspected disseminated disease [64]. The positivity rate may be higher in patients with tenosynovitis, dermatitis, and polyarthralgias than those presenting with purulent arthritis. Associated cutaneous lesions can be swabbed for culture but are also of low diagnostic value [81].
19.7 Gonococcal Resistance & Treatment
19.7.1 Resistance History
Since the introduction of antibiotics in 1937 [82], N. gonorrhea has evolved multiple resistance mechanisms, both chromosomal- and plasmid-mediated. The rise in gonococcal resistance can be attributed to both the adaptability of the organism (see pathogenesis above) as well as antibiotic prescribing habits. With regards to the latter, the increased use of over-the-counter and broad spectrum antibiotics combined with inappropriate prescribing policies for many clinical situations have facilitated the emergence of gonococcal resistance.
Introduced in the 1930s, sulfanilamide was the first curative treatment for gonorrhea. However, antibiotic resistance developed rapidly [82] such that penicillins replaced sulfanilamides as first-line gonococcal therapy in the 1940s [83]. Although penicillin remained the mainstay of therapy for several decades, low-level resistance slowly developed with progressive increases in penicillin minimal inhibitory concentrations necessitating higher treatment doses [84]. Tetracycline, used initially to treat penicillin allergic patients with gonorrhea, also became less effective over time [85]. In the late 1970s, the emergence of highly-resistant, penicillinase-producing N. gonorrhoeae marked the end of penicillin as a therapeutic agent for gonorrhea [86] .
Starting in the mid-1980s, quinolones replaced penicillins as the first-line treatment for gonorrhea [87]. Effective single oral dosing, a favorable side effect profile, and excellent efficacy at all anatomical sites made quinolones an attractive therapeutic option. However, isolates resistant to quinolones began to appear by the 1990s, initially in Asia and then quickly spreading—likely initially via travelers and then endemically within high risk groups—to Australia, Hawaii and later to North America and Europe [61, 88]. By the mid- to late-1990s, quinolones were no longer the drug of choice for gonorrhea in most Asia-Pacific countries and by the mid to late 2000s, England, Europe and North America followed suit [73, 89].
Of note, despite a decrease in the use of quinolones for treatment of gonorrhea in the UK, the rate of resistance has continued to climb in England [90] highlighting the resistance problem with gonorrhea. Because gonococcal infection is relatively common and the organism readily shares resistance genes, stopping particular antibiotic treatment of gonorrhea does not result in a diminution of resistance. The gonococcus continues to share resistance genes and still experiences ongoing resistance selection pressure because these antibiotics are widely used to treat other infections.
Extended-spectrum cephalosporins are currently considered first-line therapy for gonorrhea in most countries. Although cephalosporins remain largely effective, growing resistance has been noted throughout the Asia-Pacific, North America and Europe [21, 61, 91, 93–98]. Both the UK and US based surveillance programmes have reported a minimum inhibitory concentration creep to both ceftriaxone and cefixime in recent years [21, 91, 99]. For example, in the US, from 2000 to 2010, the minimum inhibitory concentrations to cephalosporins increased from 0.2 to 1.5 % for cefixime and from 0.1 to 0.4 % for ceftriaxone in 2000 and 2011, respectively [91, 92]. Cases of treatment failure have been reported after oral cephalosporin use in Asia, the UK and Norway [94, 99–101]. Although suspected treatment failure with ceftriaxone is rarely reported [102, 103], a highly multi-resistant N. gonorrhea strain has recently been identified in a sex worker in Japan [104].
Considering the inability to prevent spread of resistant gonococci in the past, the emergence and spread of multi-resistant cephalosporin strains appears probable. Given global travel and sexual tourism this likely will not take long. With no effective single or combined antibiotic treatment to replace cephalosporins, gonorrhea may soon become untreatable. The obvious need for new antibiotic regimens, as the microbe becomes more resistant, is an area that has not received the research attention it deserves. Although the need has clearly been recognized for a number of years [105], novel antibiotic regimens for treating gonococcal infection remain inadequately addressed.
Potential strategies to combat cephalosporin resistance include the promotion of more appropriate antimicrobial use, the development of novel treatment agents and regimens, improved surveillance and reporting networks to facilitate the identification and rapid containment of resistant isolates, as well as more effective sexually transmitted infection control and prevention programs [2, 3, 21, 61, 106] .
19.7.2 Uncomplicated Genitourinary and Anorectal Gonorrhea Treatment Recommendations
Given the differences among national guidelines and the variability of resistance rates between countries, the details on recommended therapeutic regimens have been kept to a minimum. Additionally, the discussion is limited to therapy for adolescent and adult gonorrhea. Unless indicated otherwise, treatment recommendations provided here reflect the recently updated 2010 Centers for Disease Control and Prevention Sexually Transmitted Disease Guidelines (outlined in Table 19.4)
As of 2012, the CDC no longer recommends cefixime as a first-line agent for the treatment of uncomplicated genitourinary and anorectal gonococcal infections. This decision is based on declining cefixime susceptibility among urethral N. gonorrhea isolates from the Gonococcal Isolate Surveillance Program. Dual therapy with intramuscular (IM) ceftriaxone and either a single dose of oral azithromycin or 7 day course of oral doxycycline is now the recommended first-line treatment regimen for genitourinary and anorectal gonorrhea.
In addition to treating coincident Chlamydia trachomatis infection, ceftriaxone combined with azithromycin or doxycycline may serve to improve treatment efficacy and delay the development and spread of cephalosporin-resistant gonococcal isolates. Azithromycin is the preferred agent over doxycycline given the ease and compliance of single-dose treatment regimens and lower prevalence of gonococcal resistance to azithromycin than tetracycline [91].
Patients should avoid sexual activity until their antimicrobial therapy is completed and their symptoms have resolved. In the case of persistent gonococcal infection following first-line therapy, further treatment advice should be sought from an infectious diseases expert.
19.7.3 Treatment of Pharyngeal Gonorrhea
Although usually self-limited, pharyngeal gonorrhea serves as a potential reservoir for infectious transmission and antimicrobial resistance [60, 61] . Hence, pharyngeal gonococcal infection should be treated. More difficult to eradicate than urogenital and anorectal gonococcal infections, current therapy options are limited to a single dose of IM ceftriaxone. Alternative injectable and oral antibiotics, including cefixime, have unreliable efficacy in this treatment context and should be avoided. As with genitourinary and anorectal gonorrhea, co-treatment with azithromycin and/or doxycycline is recommended for pharyngeal gonorrhea.
19.7.4 Treatment of Disseminated Gonococcal Infection
Treatment of DGI requires parenteral therapy with ceftriaxone or an alternative third-generation cephalosporin (e.g., cefotaxime or ceftizoxime). Oral therapy can be considered in patients whose illness is sufficiently mild to permit close outpatient follow-up. However, a patient with uncertain diagnosis, complicated disease, and/or difficulty tolerating oral medications should be hospitalized for the initiation of therapy. Transition to oral cefixime can be considered for susceptible organisms following 24–48 h of clinical improvement on intravenous therapy.
There have been no controlled clinical trials with respect to the duration of treatment for DGI. Antimicrobial therapy should likely be for a minimum of 7 days or continued at least until clinical signs of infection have resolved . Patients with purulent arthritis require joint drainage and 7–14 days of antibiotic therapy [64]. Treatment of meningitis or endocarditis consists of ceftriaxone for 10–14 days or a minimum of 4 weeks, respectively.
19.7.5 Special Treatment Circumstances & Alternative Agents
Ceftriaxone is also first-line treatment for gonococcal infections in pregnant women. Patients with human immunodeficiency virus (HIV) should receive the same treatment for gonorrhea as persons without HIV infection .
A non-beta lactam antibiotic may be needed in the case of severe penicillin or cephalosporin allergy [108]. Potential alternative options to cephalosporins include quinolones, macrolides, and spectinomycin. However, treatment in these cases should be performed in consultation with infectious diseases and, if possible, directed by isolate susceptibility testing.
Alternative safe and effective single-dose injectable cephalosporin regimens are available for urogenital and anorectal gonorrhea and include ceftizoxime, cefoxitin (in combination with probenecid), and cefotaxime. None of these injectable alternatives offers any advantage over ceftriaxone for urogenital infection. Oral substitutes include cefpodoxime and cefuroxime axetil. However, alternative oral and injectable cephalosporins may provide suboptimal efficacy for pharyngeal gonorrhea. Furthermore, caution is necessary when using oral cephalosporins to treat urogenital and anorectal gonorrhea due to increasing rates of gonococcal resistance to cefixime.
Developed and marketed specifically for the treatment of gonorrhea , spectinomycin is an effective alternative for genitourinary but not pharyngeal infection. Resistance tends to be rare and sporadic. However, spectinomycin is an expensive, injectable drug that is not readily available in many countries including the US.
Uncomplicated gonococcal infection can be effectively treated with high-dose azithromycin (2 gm PO once). However, significant gastrointestinal side effects and rapid development of gonococcal resistance necessitate the use of high-dose azithromycin only under special circumstances [79, 91, 109]. As noted above, a single does of azithromycin (1 gm PO) is now recommended in combination with ceftriaxone (250 mg IM) to treat gonorrhea. However, due to growing microbe resistance, treatment failures have been reported even on this combined antibiotic regimen [110].
Quinolones can be considered as second-line treatment agents. However, given high global resistance rates to this antibiotic class, treatment with a quinolone should be delayed until susceptibility results are available. Furthermore, quinolones are contraindicated in pregnant women and persons younger than 18 years of age.
In some parts of the world, aminoglycosides are used to treat gonorrhea . For example, gentamicin is the national first-line treatment for gonococcal infection in Malawi. It has also been used to treat gonorrhea in Mongolia [111–113]. The precise mode of action of aminoglycosides against gonococcus remains unclear. Despite uncertain microbiological resistance breakpoints and limited clinical resistance data, treatment failures with aminoglycosides appear rare [114, 115].
19.7.6 Treatment: Other Recommendations
Reassessment following treatment bestows a number of benefits (e.g., to confirm compliance, ensure resolution of symptoms, enquire about adverse reactions, provide further education and partner notification). However, follow-up visits may not be practical in all settings [36].
As per the 2010 CDC guidelines and 2012 update, repeat testing is not recommended upon completion of gonorrhea treatment with first-line therapy [91, 92]. However, a test of cure should be considered in the following circumstances: if second-line agents are utilized, following treatment of pharyngeal gonorrhea, and/or if symptoms or signs of infection persist. Some countries, such as the UK, recommend a test of cure in all cases, recognizing the emerging problem of resistance to extended-spectrum cephalosporins [36].
Evidence pertaining to the method and timing of test of cure is limited. In cases of persistent symptoms or signs, a repeat culture should be performed at least 72 h after completion of antimicrobial therapy [116] . NAATs are expected to remain positive for weeks following successful treatment and do not allow for the identification of resistant organisms. Thus, a positive NAAT should be followed by a confirmatory culture whenever possible.
Given high rates of recurrence, the identification of N. gonorrhea following treatment is more likely to reflect reinfection rather than treatment failure [117–120]. With this in mind, retesting for re-infection 3 months after treatment is recommended, especially in high risk patients. Additionally, in the case of disease recurrence, further patient education and partner treatment should be pursued.
Chlamydia trachomatis co-infection is common in patients with gonorrhea. With this in mind, patients treated for N. gonorrhea should also be tested and treated for chlamydia. Other sexually transmitted infections should also be considered, including syphilis, HIV, and hepatitis B. The therapy of choice for chlamydia, azithromycin (1 gm PO once) or doxycycline (100 mg BID ´ 7 days), corresponds to the dual therapy now suggested by the CDC for gonorrhea .
Positive gonorrhea cases should be reported to the local public health agency, as per national guidelines, and contact tracing pursued. Contact tracing reduces the risk of re-infection and facilitates the identification and treatment of asymptomatic infections [121]. All sexual partners exposed to an index case within 60 days of symptom onset or diagnosis should be evaluated and treated. If greater than 60 days has passed since the index case has had sexual contact, the most recent sex partner should be contacted. Contact tracing may be performed by patients, physicians or public health departments depending on local and national strategies. To achieve compliance with notification, creative maneuvers have been used. The sexually transmitted infection notification program in British Columbia, Canada (www.gender-focus.com/2011/08/08/std-notification-by-e-card-starts-in) uses humour to garner attention and interest. Patient-delivered therapy to sexual partners has been shown to decrease the rate of gonococcal reinfection [122]. However, this approach may be poorly received by some patients and/or partners. Patient-delivered therapy also leads to missed opportunities to educate sexual partners and to diagnose coexisting sexually transmitted infections. This is particularly problematic for men who have sex with men where the risk of coexisting sexually transmitted infections is high. Given ethical and medicolegal issues around partner delivered therapy, local laws should be reviewed before utilizing partner delivered therapy [123] .
Even with well funded and supported public health and/or patient contact tracing, all infected contacts in a sexual network are unlikely to be tracked down as no one member of the network knows all members. Leaving an infected sexual network member untreated keeps the organism ricocheting around the network.
19.8 Prevention
Most, if not all, countries recognize gonorrhea as a public-health priority. However, the strategies employed to address this sexually transmitted infection vary widely. While early diagnosis and treatment is uniformly pursued, emphasis on prevention has varied among countries [23].
The prevention of sexually transmitted infections in young people has been reviewed elsewhere [124]. To summarize, few trials on the efficacy of sexually transmitted infection prevention programs have been published within the last decade. Amongst published studies, considerable variability in program type and efficacy has been identified. While some prevention strategies have been associated with diminished infection-related risk behaviors, few report corresponding reductions in confirmed sexually transmitted infections . Given that rates of gonorrhea appear to be rising in some industrialized countries as noted earlier, this is especially concerning.
One well-studied preventative measure is condom use . Condoms, as well as other barrier contraceptive methods, provide a high degree of protection against sexually transmitted infections [33–35] . Post-exposure antibiotic prophylaxis also reduces risk of infection but is unlikely to be cost effective [125] . Another strategy, gonococcal mass treatment programs for at risk groups, has been trialed with limited success. Both antibiotic prophylaxis and mass treatment strategies carry the risk of fostering antimicrobial resistance, a serious concern given the emergence of multi-resistant gonococci [126, 127].
New and innovative approaches to prevention are required. In general, recent decades have seen a movement towards multidisciplinary and multileveled approaches with emphasis placed on the integration of gonorrhea prevention programs into already existing community and health-care structures [128] . Additionally, the empowerment of individuals and communities to develop and foster preventative strategies relevant to their particular social contexts is essential . Social networks influence the opinions and decisions of members [129]. Therefore, targeted core group counseling may provide the opportunity for better information dissemination within groups. For example, peer-led rather than outsider-initiated sexual health interventions (i.e., on condom use, contact tracing) are more likely to succeed, as demonstrated in adolescent and other populations [38, 130, 131].
Another important prevention strategy is the use of appropriate communication tools. Young people increasingly rely on the internet and social media as sources of health information [132–134]. With this in mind, sexual health educators need to develop creative ways of getting their message across to teens and young adults. For example, novel Internet-based strategies are being trialed in Alberta, Canada, to tackle the ongoing syphilis epidemic within that province. One approach utilizes a spoof on online dating (http://www.plentyofsyph.com) that has been associated with a significant increase in young people coming forward for testing [2]. Similar strategies could prove useful for other sexually transmitted infections including gonorrhea .
Lastly, more adolescent-friendly health care services are required. Teens tend to live in the “now” and are less likely to seek treatment at appointment-only clinics, especially if wait times are long [135]. Online triage systems and options for testing-only express visits may enhance the efficiency of busy sexually transmitted infection clinics [136, 137]. Drop in clinics, especially if located where young people frequent (e.g., malls and schools) are another option, allowing teens to follow through with “spur of the moment” decisions to get sexually transmitted infection testing .
Learning about sex, sexuality and the prevention of sexually transmitted infections is a basic human right of adolescents [138]. The strategy of “abstinence” or “abstinence until marriage” lacks scientific evidence and is flawed from a medical-ethical standpoint [139]. Given that sexually transmitted infections, including gonorrhea, disproportionately affect young adults, we have a duty to provide adolescents with meaningful knowledge and the skills to protect themselves from acquiring and transmitting sexually transmitted infections. This will require collaboration on many levels, ranging from the family unit and the community to local and national governmental levels.
19.9 Conclusion
Moving into the second decade of the 21st century, N. gonorrhoeae continues to represent a significant public health challenge. Gonococcal rates persist above national and international targets, resulting in needless morbidity and mortality. The emergence of multi-resistant gonorrhea is only going to make this situation worse .
Although the development of NAATs has improved our ability to diagnose gonorrhea, at least in industrialized countries, further refinement of diagnostic techniques is required. In particular, the role of pharyngeal gonorrhea as a significant reservoir of infection and antimicrobial resistance necessitates the development of more effective easy to use diagnostic tools . Furthermore, because resistance is such an important issue, traditional culture and sensitivity testing remains essential for tracking evolving gonococcal resistance both nationally and globally. Sentinel sites where cultures are done routinely will be key.
N. gonorrhea has proved to be a highly adaptable organism. Increasing gonococcal resistance to cephalosporins, with no single dose alternative antibiotics in the pipeline, threatens to make this organism untreatable. Effective and prudent antimicrobial strategies alongside robust national and international gonococcal surveillance programs are very much in need .
Lastly, sexually transmitted infection prevention strategies have never been more important . Public health services should aim to address the behavioral and social factors that put people at risk, including youth-friendly education and health care services. As these move forward, rigorous evaluation and collaboration of prevention strategies will be required at local, national and global levels.
References
Anderson MT, Seifert HS (2011) Opportunity and means: horizontal gene transfer from the human host to a bacterial pathogen. mBio. doi: 10.1128/mBio.00005-11
MacDonald NE, Stanbrook MB, Flegel K, Hebert PC (2011) Gonorrhea: what goes around comes around. CMAJ. doi:10.1503/cmaj.111393. http://www.cmaj.ca/content/early/2011/09/19/cmaj.111393.long
Fisman D, Laupland KB (2011) Sexually transmitted infections in Canada: a sticky situation. Can J Infect Dis Med Microbiol 22(3):80–82
Sparling PF (2008) Biology of Neisseria gonorrhoeae. In: Holmes K, Sparling P, Stamm W, Piot P, Wasserheit J, Corey L, Cohen M (eds) Sexually Transmitted Diseases, 4th edn. McGraw-Hill, China, p 607–626
Virji M (2009) Pathogenic neisseriae: surface modulation, pathogenesis and infection control. Nat Rev Microbiol 7(4):274–286
Edwards JL (2008) The role of complement in gonococcal infection of cervical epithelia. Vaccine 26(Suppl 8):156–161
Steichen CT, Shao JQ, Ketterer MR, Apicella MA (2008) Gonococcal cervicitis: a role for biofilm in pathogenesis. J Infect Dis 198(12):1856–1861
Goldenberg DL, Sexton DJ (2011) Disseminated gonococcal infection (Internet). Waltham, MA: UpToDate; 2011. http://www.uptodate.com/contents/disseminated-gonococcal-infection?source=see_link. Accessed 19 Sept 2011
Blom AM, Ram S (2008) Contribution of interactions between complement inhibitor C4b-binding protein and pathogens to their ability to establish infection with particularly emphasis on Neisseria gonorrhoeae. Vaccine 26(Suppl 8):149–155
Jarvis GA (1995) Recognition and control of neisserial infection by antibody and complement. Trends Microbiol 3(5):198–201
Department of Reproductive Health and Research/World Health Organization (2011) Emergence of multi-drug resistant Neisseria gonorrhoeae—Threat of global rise in untreatable sexually transmitted infections 2011. http://whqlibdoc.who.int/hq/2011/WHO_RHR_11.14_eng_OnlinePDF.pdf
Centers for Disease Control and Prevention (2011) Sexually Transmitted Disease Surveillance 2009. Atlanta: US Department of Health and Human Services; 2010a http://www.cdc.gov/std/stats09/surv2009-Complete_OnlinePDF.pdf. Accessed 19 Sept 2011
Health Protection Agency (2011) Healthy Protection Report weekly report 2011. http://www.hpa.org.uk/hpr/archives/2011/hpr2411_OnlinePDF.pdf. Accessed 19 Sept 2011
Public Health Agency of Canada (2011) Reported cases of notifiable STI from January 1 to June 30, 2009 and January 1 to June 30, 2010 and corresponding annual rates for the years 2009 and 2010, 2010. http://www.phac-aspc.gc.ca/std-mts/stdcases-casmts/index-eng.php Accessed 19 Sept 2011
Catchpole MA (1996) The role of epidemiology and surveillance systems in the control of sexually transmitted diseases. Genitourin Med 72(5):321–329
Kent C (2007) STD Surveillance: Critical and Costly, but Do We Know if It Works? Sex Trans Dis 34(2):81–82
Tapsall J (2011) Antimicrobial resistance in Neisseria gonorrhoeae. WHO; 2001. http://www.who.int/drugresistance/Antimicrobial_resistance_in_Neisseria_gonorrhoeae_OnlinePDF.pdf. Accessed 19 Sept 2011
Paine TC, Fenton KA, Herring A, Turner A, Ison C, Martin A et al (2001) GRASP: a new national sentinel surveillance initiative for monitoring gonococcal antimicrobial resistance in England and Wales. Sex Transm Infect 77(6):398–401
Delpech V, Marin IMC, Hughes G, Nichols T, James L, Ison CA, Gonococcal Resistance to Antibiotics Surveillance Program steering group (2009) Epidemiology and clinical presentation of gonorrhoea in England and Wales: findings from the Gonococcal Resistance to Antimicrobials Surveillance Programme 2001–2006. Sex Transm Infect 85(5):317–321
Dubois-Arber F, Jeannin A, Spencer B, Gervasoni JP, Graz B, Elford J et al (2010) Mapping HIV/STI behavioural surveillance in Europe. BMC Infect Dis 4(10):290–300
Tapsall JW, Ndowa F, Lewis DA, Unemo M (2009) Meeting the public health challenge of multidrug-and extensively drug-resistant Neisseria gonorrhoeae. Expert Rev Anti Infect Ther 7(7):821–834
Unemo M, Fasth O, Fredlung H, Limnios A, Tapsall J (2009) Phenotypic and genetic characterization of the 2008 WHO Neisseria gonorrhoeae reference strain panel intended for global quality assurance and quality control of gonococcal antimicrobial resistance surveillance for public health purposes. J Antimicrob Chemother 63(6):1142–1151
Barnes RC, Holmes KK (1984) Epidemiology of gonorrhea: current perspectives. Epidemiol Rev 6:1–30
Alary M (1997) Gonorrhea: epidemiology and control strategies. Can J Hum Sex 6(2):151–159
Fenton KA, Lowndes CM (2004) Recent Trends in the epidemiology of sexually transmitted infections in the European Union. Sex Transm Infect 80(4):255–263
Uuskula A. Puur A, Toompere K, DeHovitz J (2010) Trends in the epidemiology of bacterial sexually transmitted infections in eastern Europe. Sex Transm Infect 86(1):6–14
World Health Organization (2011) Global prevalence and incidence of selected curable sexually transmitted infections: overview and estimates. World Health Organization; 2001. http://www.who.int/hiv/pub/sti/who_hiv_aids_2001.02_OnlinePDF.pdf. Accessed 19 Sept 2011
Centralized Information System for Infectious Diseases (homepage on the Internet) (2011) Europe: World Health Organization. http://data.euro.who.int/cisid. Accessed 19 Sept 2011
May RM, Anderson RM (1987) Transmission dynamics of HIV infection. Nature 326(6):137–142
Brooks GF (1985) Pathogenesis and immunology of gonococcal infection. In: Brooks GF, Donegan EA (eds) Gonococcal infection. Edward Arnold, London, p 51–82
Holmes KK, Johnson DW, Trostle HJ (1970) An estimate of the risk of men acquiring gonorrhea by sexual contact with infected females. Am J Epidemiol 91(2):170–174
Hooper RR, Reynolds GH, Jones OG, Zaidi A, Wiesner PJ, Latimer KP et al (1978) Cohort study of venereal disease.1: the risk of gonorrhea transmission from infected women to men. Am J Epidemiol 108(2):136–144
Kigbu JH, Nyango DD (2009) A critical look on condoms. Niger J Med 18(4):354–359
Steiner MJ, Cates W Jr (2006) Condoms and sexually-transmiited infections. N Engl J Med 354(25):2642–2643
Warner L, Stone KM, Macaluso M, Buehler JW, Austin HD (2006) Condom use and risk of gonorrhea and Chlamydia: a systemic review of design and measurement factors assessed in epidemiologic studies. Sex Transm Dis 33(1):35–51
Bignell C, FitzGerald M (2011) UK National guideline for the management of gonorrhoea in adults. British Association for Sexual Health and HIV, 2011. http://www.bashh.org/documents/3611 Accessed 19 Sept 2011
Brunham RC (1997) Core group theory: a central concept in STD epidemiology. Venereology 10:34–39
Al-Tayyib AA, Rietmeijer CA (2011) Detecting Chlamydia and gonococcal infections through social and sexual networks. Sex Transm Infect. doi:10.1136/sextrans-2011-050102.59
Ford K, Sohn W, Lepkowski J (2002) American adolescents: sexual mixing patterns, bridge partners, and concurrency. Sex Transm Dis 29(1):13–19
Berlan ED, Holland-Hall C (2010) Sexually transmitted infections in adolescents: advances in epidemiology, screening, and diagnosis. Adolesc Med State Art Rev 21(2):332–346
Stoner BP, Whittington WL, Hughes JP, Aral SO, Homes KK (2000) Comparative epidemiology of heterosexual gonococcal and chlamydial networks: implications for transmission patterns. Sex Transm Dis 27(4):215–223
MacDonald NE, Wells GA, Fisher WA, Warren WK, King MA, Doherty JA et al (1990) High-risk STD/HIV behavior among college students. JAMA 263(23):3155–3159
MacDonald NE, Fisher WA, Wells GA, Doherty JA, Bowie WR (1994) Canadian street youth: correlates of sexually risk-taking activity. Pediatr Infect Dis J 13(8):690–697
Shafti T, Burnstein GR (2004) An overview of sexually transmitted infections in adolescents. Adolesc Med Clin 15(2):201–214
Robertson AA, Thomas CB, St Lawrence JS, Pack R (2005) Predictors of infection with chlamydia or gonorrhea in incarcerated adolescents. Sex Transm Dis 32(2):115–122
Public Health Agency of Canada (2011) Street youth in Canada. Findings from enhanced surveillance of canadian street youth, 1999–2003 (Internet), March 2006. http://www.phac-aspc.gc.ca/std-mts/reports_06/youth-eng.php. Accessed 19 Sept 2011
Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J et al (2010) Youth risk behaviour surveillance-United States, 2009. MMWR Surveill Summ 59(5):1–142
Ford K, Lepkowski JM (2004) Characteristics of sexual partners and STD infection among American adolescents. Int J STD AIDS 15(4):260–265
Forhan SE, Gottlieb SL, Sternberg MR, Xu F, Datta SD, McQuillan GM et al (2009) Prevalence of sexually transmitted infections among female adolescents aged 14 to 19 in the United States. Pediatrics 124(6):1505–1512
Kahn JA, Rosenthal SL, Succop PA, Ho GYF, Burk RD (2002) Mediators of the association between age at first sexual intercourse and subsequent human papillomavirus infection. Pediatrics 109(1):5
Kaestle CE, Halpern CT, Miller WC, Ford CA (2005) Young age at first sexual intercourse and sexually transmitted infections in adolescents and young adults. Am J Epidemiol 161(8):774–780
Jayakody A, Sinha S, Tyler K, Khadr SN, Clark C, Klineberg E et al (2001) Early sexual risk among black and minority ethnicity teenagers: a mixed methods study. J Adolesc Health 48(5):499–506
Tu W, Batteiger BE, Wiche S, Ofner S, Van Der Pol B, Katz BP et al (2009) Time from first intercourse to first sexually transmitted infection diagnosis among adolescent women. Arch Pediatr Adolesc Med 163(12):1106–1111
Kann L, Kichen SA, Williams BI, Ross JG, Lowry R, Grunbaum JA et al (2000) Youth risk behaviour surveillance-United States, 1999. MMWR CDC Surveill Summ 49(5):1–32
Hook EW, Handsfield HH (2008) Gonococcal Infections in the Adult. In: Holmes K, Sparling P, Stamm W, Piot P et al (eds) Sexually transmitted infections, 4th edn. McGraw-Hill, China, p 627–646
Woods WR (2005) Gonococcal infections in neonates and young children. Semin Pediatr Infect Dis 16(4):258–270
Platt R, Rice PA, McCormack WM (1983) Risk of acquiring gonorrhea and prevalence of abnormal adnexal findings among women recently exposed to gonorrhea. JAMA 250(23):3205–3209
Edwards LE, Barrada MT, Hamman AA, Hakanson EY (1978) Gonorrhea in pregnancy. Am J Obstet Gynecol 132(6):637–641
Woods CR, Jr (2009) Gonococcal infections. In: Feigin RD, Cherry JD, Demmler-Harrison GJ, Kaplan SL (eds) Feigin & Cherry’s textbook of pediatric infectious diseases, 6th edn. Elsevier, Philadelphia, p 1366–1393
Kinghorn G (2010) Pharyngeal gonorrhea: a silent cause for concern. Sex transm infect 86(6):413–414
Barry PM, Klausner JD (2009) The use of cephalosporins for gonorrhea: the impending problem of resistance. Expert Opin Pharmacother 10(4):555–577
Kinghorn GR, Rashid S (1979) Prevalence of rectal and pharyngeal infection in women with gonorrhoea in Sheffield. Br J Vener Dis 55(6):408–410
Hunte T, Alcaide M, Castro J (2010) Rectal infections with chlamydia and gonorrhoea in women attending a multiethnic sexually transmitted diseases urban clinic. Int J STD AIDS 21(12):819–822
Goldenberg, DL, Sexton DJ (2011) Disseminated gonococcal infection (Internet). Waltham, MA: UptoDate; 2011 (cited 2011 Sept 11). http://www.uptodate.com/contents/disseminated-gonococcal-infection
Pasquariello CA, Plotkin SA, Rice RJ, Hackney JR (1985) Fatal gonococcal septicemia. Pediatr Infect Dis 4(2):204–206
Rice PA (2005) Gonococcal arthritis (disseminated gonococcal infection). Infect Dis Clin North Am 19(4):853–861
US Preventative Services Task Force (2005) Screening for Gonorrhea: Recommendation Statement. Ann Fam Med 3(3):263–267
Ross JDC (2010) Gonorrhoea: to screen or not screen? Sex Transm Infect 86(6):411–412
Johnson RE, Newhall WJ, Papp JR, Knapp JS, Black CM, Gift TL et al (2002) Screening tests to detect Chlamydia trachomatis and Neisseria gonorrhoeae infections—2002. MMWR Recomm Rep 51(RR-15):1–38
Whiley DM, Tapsall JW, Sloots TP (2006) Nucleic acid amplification testing for Neisseria gonorrhoeae: an ongoing challenge. J Mol Diagn 8(1):3–15
Bachmann LH, Johnson RE, Cheng H, Markowitz L, Papp JR, Palella FJ Jr et al (2010) Nucleic acid amplification tests for diagnosis of Neisseria gonorrhoeae and Chlamydia trachomatis rectal infections. J Clin Microbiol 48(5):1827–1832
Fairley CK, Chen MY, Bradshaw CS, Tabrizi SN (2011) Is it time to move to nucleic acid amplification tests for pharyngeal and rectal gonorrhoea in men who have sex with men to improve gonorrhoea control? Sex Health 8(1):9–11
Centers for Disease Control and Prevention (2007) Update to CDC’s sexually transmitted diseases treatment guidelines, 2006: fluoroquinolones no longer recommended for treatment of gonococcal infections. MMWR Morb Mortal Wkly Rep 56(14):332–336
Graseck AS, Shih SL, Peipert JF (2011) Home versus clinic-based specimen collection for Chlamydia trachomatis and Neisseria gonorrhoeae. Expert Rev Anti Infect Ther 9(2):183–194
Howard EJ, Xu F, Taylor SN, Stoner BP, Mena L, Nsuami MJ et al (2011) Screening methods for Chlamydia trachomatis and Neisseria gonorrhoeae infections in sexually transmitted infection clinics: what do patients prefer? Sex Transm Infect 87(2):149–151
Ison C (2006) GC NAATs: is the time right? Sex Transm Infect 82(6): 515
Bachmann LH, Johnson RE, Cheng H, Markowitz LE, Papp JR, Hook EW 3rd (2009) Nucleic acid amplification tests for diagnosis of Neisseria gonorrhoeae oropharyngeal infections. J Clin Microbiol 47(4):902–907
Razali MF, Fairley CK, Hocking J, Bradshaw CS, Chen MY (2010) Sampling technique and detection rates for pharyngeal gonorrhea using culture. Sex Transm Dis 37(8):522–524
Centers for Disease Control and Prevention (2010) Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep 59(RR-12):1–110
Bonilla H, Kepley R, Pawlak J, Belian B, Raynor A, Saravolatz LD (2011) Rapid diagnosis of septic arthritis using 16S rDNA PCR: a comparison of 3 methods. Diagn Microbiol Infect Dis 69(4):390–395
Burstein GR, Murray PJ (2003) Diagnosis and management of sexually transmitted disease pathogens among adolescents. Pediatr Rev 24(3):75–82
Dees JE, Colston JAC (1937) The Use of Sulfanilamide in Gonococcic Infections. JAMA 108:1855–1858
Herrell WE, Cook EN, Thomspon L (1943) Use of Penicillin in Sulfonamide-resistant Gonorrhea Infections. JAMA 122(5):289–292
Whittington WL, Knapp JS (1988) Trends in resistance of Neisseria gonorrhoeae to antimicrobial agents in the United States. Sex Transm Dis 15(4):202–210
Reyn A, Korner B, Bentzon MW (1958) Effects of penicillin, streptomycin and tetracycline on N. gonorrhoeae isolated in 1944 and in 1957. Br J Vener Dis 34:227–239
Phillips I (1976) Beta lactamase-producing, penicillin-resistant gonococcus. Lancet 2(7987): 656–657
Scott GR, McMillan A, Young H (1987) Ciprofloxacin versus ampicillin and probenecid in the treatment of uncomplicated gonorrhoeae in men. J Antimicrob Chemother 20(1):177–121
Dan M (2004) The use of fluoroquinolones in gonorrhoea: the increasing problem of resistance. Expert Opin Pharmacother 5(4):829–854
Health Protection Agency (2011) Susceptibility testing of N. gonorrhoeae (Internet) 2009a. http://www.hpa.org.uk/web/HPAweb&HPAwebStandard/HPAweb_C/1195733778434. Accessed 19 Sept 2011
Health Protection Agency (2011) STIs Annual Slide Set 2000–2009 (Internet). 2009b. http://www.hpa.org.uk/Topics/InfectiousDiseases/InfectionsAZ/STIs/STIsAnnualDataTables/AnnualSTISlideset/. Accessed 19 Sept 2011
Centers for Disease Control and Prevention (2011) Cephalosporin susceptibility among Neisseria gonorrhoeae Isolates—United States, 2000–2010. MMWR Morb Mortal Wkly Rep 60(26):873–877
Centers for Disease Control and Prevention (2012) Update to CDC’s sexually transmitted diseases treatment guidelines, 2010: oral cephalosporins no longer a recommended treatment for gonococcal infections. MMWR 61(31):590–594
Chisholm SA, Mouton JW, Lewis DA, Nicols T, Ison CA, Livermore DM (2010) Cephalosporin MIC creep among gonococci: time for a pharmacodynamic rethink? J Antimicrob Chemother 65(10):2141–2148
Cole MJ, Chisholm SA, Unemo M, Hoffmann S, van de Laar MJW, Ison CA (2011) European gonococcal antimicrobial surveillance programme (Euro-GASP): towards timelier monitoring. Sex Transm Infect. doi:10.1136/sextrans-2011-050102.63
Kirkcaldy RD, Ballard RC, Dowell D (2011) Gonococcal resistance: are cephalosporins next? Curr Infect Dis Rep 13(2):196–204
Martin IM, Hoffmann S, Ison CA (2006) European surveillance of sexually transmitted infections (ESSTI): the first combined antimicrobial susceptibility data for Neisseria gonorrhoeae in Western Europe. J Antimicrob Chemother 58(3):587–593
WHO Western Pacific Gonococcal Antimicrobial Surveillance Programme (2008) Surveillance of antibiotic resistance in Neisseria gonorrhoeae in the WHO Western Pacific Region. Commun Dis Intell 32(1):48–51
Wang SA, Lee MV, O’Connor N, Iverson CJ, Ohye RG, Whitican RM et al (2003) Multidrug-resistant Neisseria gonorrhoeae with decreased susceptibility to cefixime-Hawaii. Clin Infect Dis 37(6):849–852
Tapsall JW (2009) Neisseria gonorrhoeae and emerging resistant to extended spectrum cephalosporins. Curr Opin Infect Dis 22(1):87–91
Deguchi T, Yasuda M, Yokoi S, Ishida K, Ito M, Ishihara S et al (2003) Treatment of uncomplicated gonococcal urethritis by double-dosing of 200 mg cefixime at a 6 h interval. J Infect Chemother 9(1):35–39
Ito M, Yasuda M, Yokoi S, Ito S, Takahashi Y, Ishihara S et al (2004) Remarkable increase in central Japan in 2001–2002 of Neisseria gonorrhoeae isolates with decreased susceptibility to penicillin, tetracycline, oral cephalosporins, and fluoroquinolones. Antimicrob Agents Chemother 48(8):3185–3187
Tapsall J, Read P, Carmody C, Bourne C, Ray S, Limnios A et al (2009) Two cases of failed ceftriaxone treatment in pharyngeal gonorrhoeae verified by molecular microbiological methods. J Med Microbiol 58(Pt 5):683–687
Unemo M, Golparian D, Hestner A (2011) Ceftriaxone treatment failure of pharyngeal gonorrhea verified by international recommendations, Sweden, July 2010. Euro Surveill 16(6): pii:19792. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19792
Ohnishi M, Saika T, Hoshina S, Iwasaku K, Nakayama S, Watanabe H et al (2011) Ceftriaxone-resistant Neisseria gonorrhoeae, Japan. Emerg Infect Dis 17(1):148–149
Newman LM, Moran JS, Workowski KA (2007) Update on the management of Gonorrhea in adults in the United States. Clin Infect Dis 44(Suppl 3):84–101
Deguchi T, Nakane K, Yasuda M, Maeda S (2010) Emergence and spread of drug resistant Neisseria gonorrhoeae. J Urol 184(3):851–858
Public Health Agency of Canada (2011) Canadian guidelines on sexually transmitted infections, 2008 Edition (Internet). Ottawa, ON: Public Health Agency of Canada; 2008. http://www.phac-aspc.gc.ca/std-mts/sti-its/guide-lignesdir-eng.php. Accessed 19 Sept 2011
Pichichero ME (2005) A review of evidence supporting the American Academy of Pediatrics recommendation for prescribing cephalosporin antibiotics for penicillin-allergic patients. Pediatrics 115(4):1048–1057
Bignell C, Garley J (2010) Azithromycin in the treatment of infection with Neisseria gonorrhoeae. Sex Transm Infect 86(6):422–426
Ison CA, Hussey J, Sankar KN, Evans J, Alexander S (2011) Gonorrhoea treatment failures to cefixime and azithromycin in England. Euro Surveill 16(14):pii: 19833. http://www.eurosurveillance.org/images/dynamic/EE/V16N14/art19833_OnlinePDF.pdf
Daly CC, Hoffman I, Hobbs M, Maida M, Zimba D, Davis R et al (1997) Development of an antimicrobial susceptibility surveillance system for Neisseria gonorrhoeae in Malawi: comparison of methods. J Clin Microbiol 35(11):2985–2989
Ieven M, Van Looveren M, Sudigdoadi S, Rosana Y, Goossens W, Lammens C et al (2003) Antimicrobial susceptibilities of Neisseria gonorrhoeae strains isolated in Java, Indonesia. Sex Trans Dis 30(1):25–29
Lkhamsuren E, Shultz TR, Limnios EA, Tapsall JW (2001) The antibiotic susceptibility of Neisseria gonorrhoeae isolated in Ulaanbaatar, Mongolia. Sex Transm Infect 77(3):218–219
Brown LB, Krysiak R, Kamanga G, Mapanie C, Kanyamula H, Banda B et al (2010) Neisseria gonorrhoeae antimicrobial susceptibility in Lilongwe Malawi, 2007. Sex Transm Dis 37(3):169–172
Vakulenko SB, Mobashery S (2003) Versatility of aminoglycosides and prospects for their future. Clin Microbiol Rev 16(3):430–450
Jephcott AE (1997) Microbiological diagnosis of gonorrhoea. Genitourin Med 73(4):245–252
Fung M, Scott KC, Kent CK, Klausner JD (2007) Chlamydial and gonococcal reinfection among men: a systematic review of data to evaluate the need for retesting. Sex Transm Infect 83(4):304–309
Hosenfeld CB, Workowski KA, Berman S, Zaidi A, Dyson J, Mosure D et al (2009) Repeat infection with chlamydia and gonorrhea among females: a systematic review of the literature. Sex Transm Dis 36(8):478–489
Kissinger PJ, Reilly K, Taylor SN, Leichliter JS, Rosenthal S, Martin DH (2009) Early repeat Chlamydia trachomatis and Neisseria gonorrhoeae infections among heterosexual men. Sex Transm Dis 36(8):498–500
Peterman TA, Tian LH, Metcalf CA, Satterwhite CL, Malotte CK, DeAugustine N et al (2006) High incidence of new sexually transmitted infections in the year following a sexually transmitted infection: a case for rescreening. Ann Intern Med 145(8):564–572
Du P, Coles B, Gerber T, McNutt LA (2007) Effects of partner notification on reducing Gonorrhea incidence rate. Sex Transm Dis 34(4):189–194
Kissinger P, Schmidt N, Mohammed H, Leichliter JS, Gift TL, Meadors B et al (2006) Patient-delivered partner treatment for Trichomonas vaginalis infection: a randomized controlled trial. Sex Transm Dis 33(7):445–450
Saperstein AK, Firnhaber GC (2010) Should you test or treat partners of patients with gonorrhea, chlamydia or trichomoniasis? J Fam Practice 59(1):46–48
DiClemente RJ, Crosby RA (2006) Preventing sexually transmitted infections among adolescents: the glass is half full. Curr Opin Infect Dis 19(1):39–43
Harrison WO, Hooper RR, Weisner PJ, Campbell AF, Karney WW, Reynolds GH et al (1979) A trial of minocycline given after exposure to prevent gonorrhea. NEJM 300(19):1074–1078
Holmes KK, Johnson DW, Kvale PA, Halverson CW, Keys TF, Martin DH (1996) Impact of a Gonorrhea control program, including selective mass treatment in female sex workers. J Infect Dis 174(Suppl 2):230–9
Manhart LE, Holmes KK (2005) Randomized controlled trials of individual-level, population-level, and multileveled interventions for preventing sexually transmitted infections: what has worked? J Infect Dis 191(Suppl 1):7–24
Jourden J, Etkind P (2004) Enhancing HIV/AIDS and STD prevention through program integration. Public Health Rep 119(1):4–11
Yee L, Simon M (2010) The role of the social network in contraception decision-making among young, african american and latina women. J Adolesc Health 47(4):374–380
Kim CR, Free C (2008) Recent evaluations of the peer-led approach in adolescent sexual health education: a systemic review. Int Fam Plann Perspect 34(2):89–90
Berenson AB, Wu ZH, Breitkopf CR, Newman J (2006) The relationship between source of sexual information and sexual behavior among female adolescents. Contraception 73(3):274–278
Borzekowski DLG, Rickert VI (2001) Adolescent cybersurfing for health information: a new resource that crosses barriers. Arch Pediatr Adolesc Med 155(7):813–817
Gray NJ, Klein JD, Noyce PR, Sesselberg TS, Cantrill JA (2005) Health information-seeking behaviour in adolescence: the place of the internet. Soc Sci Med 60(7):1467–1478
Vance K, Howe W, Dellavalle RP (2009) Social internet sites as a source of public health information. Dermatol Clin 27(2):133–136
Ward H, Robinson AJ (2006) Still waiting: poor access to sexual health services in the UK. Sex Transm Infect 82(1):3
Jones R, Menton-Johansson JR, Waters AM, Sullivan AK (2010) eTriage—a novel, web-based triage and booking service: enabling timely access to sexual health clinics. Int J STD AIDS 21(2):30–33
Shamos SJ, Mettenbrink CJ, Subiadur JA, Mitchell BL, Rietmeijer CA (2008) Evaluation of a testing-only “express” visit option to enhance efficiency in a busy STI clinic. Sex Transm Dis 35(4):336–340
Ruiz MS, Gable AR, Kaplan EH, Stoto MA, Fineberg HV, Trussell J (eds) (2001) No time to lose: getting more from HIV prevention. National Academy Press, Washington DC
Santelli J, Ott MA, Lyon M, Rogers J, Summers D (2006) Abstinence-only education policies and program: a position paper of the Society for Adolescent Medicine. J Adolesc Health 38(1):83–87
World Health Organization (2011) Regional Office for Europe. Sexually transmitted infections. http://data.euro.who.int/cisid/Default.aspx?TabID=272714. Accessed 19 Sept 2011
European Centre for Disease Control and Prevention (2011) Annual epidemiological report on communicable diseases in Europe, 2010. http://ecdc.europa.eu/en/publications/Publications/1011_SUR_Annual_Epidemiological_Report_on_Communicable_Diseases_in_Europe_OnlinePDF.pdf. Accessed 19 Sept 2011
Centers for Disease Control and Prevention (2011) Sexually Transmitted Diseases Surveillance, 2008. http://www.cdc.gov/std/stats08/tables/1.htm Accessed 19 Sept 2011
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Smith, J., Mailman, T., MacDonald, N. (2013). How to Get and Get Rid of Gonorrhea. In: Curtis, N., Finn, A., Pollard, A. (eds) Hot Topics in Infection and Immunity in Children IX. Advances in Experimental Medicine and Biology, vol 764. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-4726-9_19
Download citation
DOI: https://doi.org/10.1007/978-1-4614-4726-9_19
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-4725-2
Online ISBN: 978-1-4614-4726-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)