
Abstract
Selenoprotein P (SePP) is a unique selenoprotein in many respects. It carries up to ten selenocysteine moieties, which have been inserted cotranslationally with the help of two separate SECIS elements in its mRNA. The majority of serum SePP is secreted by the liver where hepatocytes convert nutritional selenocompounds into SePP for transport and distribution. Therefore, serum concentration of SePP is a useful biomarker for the selenium status of an individual. Recently, two endocytic receptors, i.e., Lrp2/megalin and Lrp8/ApoE receptor 2, have been identified which participate in target cell-specific SePP uptake and retention. A SePP-cycle has been proposed based on a tissue-specific sequence of reversible biosynthesis, secretion, and reuptake. Brain, testes, and kidney appear to use the SePP-cycle in order to preserve tissue selenium in times of poor nutritional supply. In how far individual genotype differences and common disease signals impair this pathway and disturb normal selenium metabolism and its hierarchical distribution by affecting SePP biosynthesis, secretion of isoforms and reuptake is a central research issue in basic science and biomedicine.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Selenoprotein P (SePP): A Unique Member of the Selenoprotein Family
Among all mammalian selenoproteins, Selenoprotein P (SePP) is unique in several ways; SePP transcripts contain ten selenocysteine (Sec) codons within the open reading frame in both rodents and humans, two separate Sec-insertion sequence (SECIS) elements in the 3′-untranslated region of the transcripts direct cotranslational Sec insertion, and, in addition to extracellular GPx3, SePP is the only selenoprotein secreted into blood accounting for about 50% of selenium in plasma of healthy well-nourished individuals [1–6]. Accordingly, it has been speculated since the first description of SePP that its high selenium content is indicative of a transport function elicited by this unique selenoprotein [7] reaching its cellular targets via specific receptor(s) [8].
This interpretation was corroborated in subsequent studies by a number of complementary findings: e.g., (1) dietary selenium intake controls SePP in parallel to selenium concentrations in plasma [9]; (2) molecular cloning of the rodent cDNA identified a selenium-rich stretch of amino acids comprising an impressive segment of nine selenocysteine (Sec) residues within the C-terminal domain [10] which is well conserved throughout evolution [11]; (3) metabolic labeling studies indicated that dietary selenium is taken up fast by the liver and incorporated into circulating SePP which, slowly declining, gives rise to increasing kidney-derived GPx3 concentrations [12]; (4) SePP constitutes the essential Se-containing component in serum-based cell culture medium supporting growth and survival of primary cells [13, 14]; (5) transgenic mice with genetically disrupted SePP biosynthesis (Sepp-knockout, Sepp −/−) develop a number of Se-dependent phenotypes including growth defect, male infertility, and neuronal abnormalities [15, 16]; and (6) the identification of specific SePP binding and uptake by members of the lipoprotein receptor-related protein (Lrp) family confirms transport by SePP as a regulated and targeted process of selenium supply to specific target tissues [17–19].
Together, these important findings and a number of additional very insightful experiments have contributed to our current understanding of SePP serving as an endogenous selenium transport protein essential for regular selenium distribution, selenium homeostasis, and overall health (Fig. 16.1). In how far SePP fulfills additional important enzymatic, protective, and metabolic functions in vivo is currently subject to intensive research. In the following sections, we review and highlight mainly its selenium transport and supply function.

Structural features of selenoprotein P (SePP). SePP comprises two domains. The N-terminal domain, which is predicted to adopt a thioredoxin-fold, contains a Sec-X-X-Cys motif within the turn between a beta-sheet and alpha-helix, showing weak peroxidase activity. The Sec-rich C-terminal domain is without homology to any known protein and likely serves a transport function. A classical N-terminal signal sequence (SP) directs SePP biosynthesis into the ER lumen. The secreted protein carries three N-glycosylation sites and one O-linked glycosylation site. A heparin-binding domain (HBD) has been identified along with two His-rich domains, which potentially mediate association to the extracellular matrix. SePP isoforms may result from differential glycosylation, proteolytic cleavage, or premature translational termination
2 Lipoprotein Receptor-Related Protein-2 (Lrp2, Megalin) and Lrp8 (ApoER2): Two Multifunctional Endocytic Receptors Involved in SePP Metabolism
Circulating lipoproteins are recognized by glycosylated cell-membrane receptors (lipoprotein receptor-related proteins, Lrp) which serve as recognition, entry, and signaling devices in lipid metabolism [20]. In general, these receptors appear to not only control lipid homeostasis, delivery, and turnover, but are also involved in targeted transport processes and renal reuptake mechanisms of hormone- and vitamin-binding proteins and their ligands [21].
Among these proteins, Lrp2 (also known as megalin or glycoprotein-330) has been shown to be essential for growth, CNS development, and endocrine regulation. It is expressed in epithelial cells of the lung airway, epididymis, mammary gland, inner ear, neural tube, and renal proximal tubules. Importantly, Lrp2 participates in binding and internalization of a whole variety of circulating carrier proteins for specific hydrophobic ligands. Accordingly, Lrp2 knockout mice lacking the receptor in the kidney lose a number of essential hormones and vitamins in their urine by failing to reabsorb, e.g., vitamin D3/vitamin D-binding globulin, progesterone/clara cell secretory protein, vitamin A/retinol-binding protein, androgens and estrogens/sex hormone-binding globulin, thyroid hormones/transthyretin, and vitamin B12/transcobalamin [21, 22]. By now, the importance of Lrp2-mediated (re-)uptake and internalization of hydrophobic ligands along with their high molecular weight carrier proteins from serum or the primary glomerular filtrate has been demonstrated in a number of animal models and in patients with inherited diseases in specific components controlling the uptake or lysosomal dissociation and release process [23, 24].
These findings have challenged the free hormone hypothesis that lipophilic hormones are bound to carrier proteins for reservoir and transport functions only, and that just the free unbound hormones are of endocrine importance. Instead, the respective carrier proteins and bound ligands, in combination with Lrp2, now seem to actively control hormone homeostasis, targeted delivery, and turnover by specific serum protein–endocytic receptor interactions [25]. This mechanism is reminiscent of the active transport principle used by Odysseus et al. in form of the “Trojan Horse” [26]. The additional importance of Lrp2 for selenium homeostasis by specific binding and reuptake of SePP came initially as a surprise to the field of selenium biology [17, 27], but appears highly plausible as a logical addition to the list of functions for this internalizing system controlling the uptake of essential circulating serum factors such as nutrients, vitamins, and hormones.
Lrp8 (Apolipoprotein E receptor 2, ApoER2) contains five functional domains resembling those of the LDL-R (Fig. 16.2). It was originally isolated based on its sequence homology to the LDL-R and very low density lipoprotein receptor (VLDL-R). Lrp8 is one of the cell surface receptors being involved in reelin signaling. Reelin is a large neuronal signaling molecule guiding neuronal cell migration during central nervous system development [28]. Reelin interacts with both Lrp8 and VLDL-R. Genetic inactivation of both receptors leads to neuronal migration deficits, tremor, and ataxia [29]. These findings are in line with the classical reeler phenotype observed in a spontaneously occurring mouse strain characterized by impaired motor coordination, tremor, and ataxia [30].

Schematic structure of endocytic SePP receptors of the lipoprotein receptor-related protein (LRP) family. LRPs, a large number of different serum proteins, in particular Lrp1 and megalin, are multifunctional proteins capable of binding a large number of serum proteins. ApoER2 and megalin have been demonstrated to bind SePP and mediate SePP uptake into target cells in vivo. ApoER2 mediates selenium uptake into Sertoli cells and into neurons. Megalin is highly expressed in the kidney tubule epithelium. Lack of either receptor in mice leads to decreased Se/SePP uptake into respective tissues
Interestingly, a similar neurological phenotype is observed in Sepp −/− mice on diets with low selenium content [31]. This phenotypic resemblance was resolved when Lrp8 was identified as a second receptor capable of SePP recognition, binding, and uptake in testes [18] and brain [19]. Together, a Se-delivery system consisting of SePP as the transport device along with Lrp2 and Lrp8 as tissue-specific endocytic uptake receptors can be envisaged, which appears to constitute the physiological pathway controlling the hierarchical supply of selenium to brain and testes. No evidence has been presented on a potential role of VLDL-R being involved in SePP transport.
3 Mouse Models of Modified SePP, Lrp2, or Lrp8 Expression
3.1 Classical Gene Targeting
Global genetic inactivation of Sepp in mice was simultaneously reported by two independent groups observing a similar phenotype of grossly disturbed selenium metabolism [15, 16]. Interestingly, not only circulating selenium concentrations were decreased in Sepp −/− mice, but also the known preferential targets of selenium supply, i.e., brain and testes, displayed strongly reduced selenium contents. Accordingly, the well-known importance of regular testes selenium for reproduction was corroborated in the male Sepp −/− mice as they were infertile [32, 33].
A neurological phenotype became apparent in Sepp −/− mice which was strictly dependent on nutritional selenium supply [31, 34]. This finding opened a new area of selenium research and is reviewed in Chap. 18 in detail. SePP is now viewed as a local selenium organification, retention, and reversible storage device in brain, safeguarding neuronal selenium content even against an unfavorable gradient of low serum selenium concentrations in times of poor supply [35]. Under regular conditions, the so-called “SePP-cycle” (Fig. 16.3) including local SePP biosynthesis, extracellular deposition, and reuptake appears extremely efficient in order to protect the vulnerable neuronal structures from loss of the essentially needed trace element [4].

Summary of selenium transport processes described in vivo. Dietary selenium is primarily taken up along the absorptive epithelium of the small bowel by transporters specific for inorganic divalent anions (e.g., the sodium-dependent sulfate transporter, NaSi-1) or transporters for amino acids and small peptides. The molecular identity of the different selenocompounds traveling through the portal circulation to the liver has not been fully elucidated. Within the liver, the selenocompounds are converted into Sec-tRNA[Ser]Sec and translationally inserted into selenoproteins. GPx1 has been proposed as a hepatic storage form for excess selenium, which may also be converted into selenosugars or selenonium ions and excreted. Free Sec concentrations in the tissue are very low. The liver is central to Se metabolism as the major source of plasma SePP, which transports selenium to privileged target tissues, e.g., brain, testis, and kidney. Brain selenium supply is complicated, since several cellular membranes must be crossed to finally reach the neurons. Megalin may be involved in SePP uptake along the choroid plexus and ependymal epithelium, while ApoER2 is expressed by neurons. Astrocytes synthesize SePP in vitro and may thus contribute to neuronal Se supply. Neurons express SePP and may store excess selenium extracellularly in the form of SePP. Brain retains its privileged selenium status during dietary restriction via reversible SePP expression, extracellular deposition, and reuptake. We have termed neuronal SePP synthesis and ApoER2-mediated SePP reuptake in brain as “SePP-cycle.” Testis function likewise Fig. 16.3 (continued) depends on ApoER2-mediated SePP uptake. Inactivation of either protein leads to decreased GPx4 expression in maturing spermatozoa and infertility. In contrast to brain, selenite appears not to cross the blood-testis barrier. Megalin expressed along the kidney tubular epithelium is involved in reuptake of SePP from the primary glomerular filtrate. Accordingly, inactivation of megalin leads to urinary loss of SePP. Megalin-positive cells express the highest levels of GPx1, GPx3, and SePP within the kidney, and inactivation of megalin decreases expression of all three proteins. Plasma GPx3 originates from the kidney epithelium, but most GPx3 is deposited locally within the kidney. SePP secretion by the kidney is a novel notion and instructive hypothesis. Another “SePP-cycle” can thus be proposed involving glomerular filtration, reuptake, and renal resynthesis of SePP. Kidney insufficiency in patients is associated with low Se status. Tissues expressing selenoproteins, but not ApoER2 and megalin, likely operate a still elusive Se uptake mechanism which might rely on the poorly characterized selenocompounds from the gastrointestinal tract
Besides providing selenium systemically from liver to the other organs, hepatic SePP biosynthesis plays an important role in preserving whole body selenium status [36]. In comparison to wild-type mice, Sepp −/− mice show a higher selenium loss via the urine. This effect can be ascribed to a better availability of selenium in liver for the production of small selenocompounds which become filtered in the kidneys for secretion, e.g., trimethylselenonium and selenosugars [37]. Hepatic SePP thus fulfills more roles than merely transporting and distributing the trace element by ensuring its efficient biotransformation and organification into a readily usable circulating form. SePP apparently also enables efficient selenium retention in circulation as well as prevention of its renal excretion, a principle well known from homeostatic mechanisms which have evolved for preserving low molecular mass hormones and vitamins.
Lrp2 −/− mice usually die perinatally [38]. A second mutant mouse strain on a different genetic background was independently characterized of which a fraction of mutant mice survive into adulthood [39]. We have used these mice as a model system for the analysis of the physiological functions of Lrp2 in adult mice as discussed later with respect to renal SePP metabolism [27].
In contrast, Lrp8 −/− mice are born at the expected Mendelian ratio and appear grossly normal. Reduced male fertility of these mice was associated with a reduced expression of the selenoenzyme glutathione-peroxidase 4 (GPx4) in the initial segments of the epididymis [40]. The molecular role of GPx4 during spermiogenesis had been elucidated earlier and was shown to depend on a specific “moonlighting” process converting the active selenoenzyme into a component of the intracellular cytoskeleton essential for sperm structure and motility [41]. Therefore, male infertility of Lrp8 −/− mice appears secondary to decreased selenoprotein expression in sperm which in turn depends on SePP-mediated selenium supply [42].
Interestingly, a similar selenium deficiency develops not only in testes but also in brain of Lrp8 −/− mice [19]. Again, the developing phenotype was strictly dependent on the selenium supply leading to severe neurological impairment on experimental diets with reduced selenium content. The phenotypic similarity of the neurological phenotypes of Lrp8 −/− and Sepp −/− mice fed a low selenium diet was again striking and corroborated a function of brain Lrp8 in SePP uptake.
3.2 Isoforms of SePP
The two-domain structure of SePP implies two separate functions for the circulating selenoprotein, i.e., a presumable enzymatic activity linked to the first Sec residue within the N-terminal thioredoxin-like domain and a selenium supply function mainly mediated by the Sec-rich C-terminus [43]. Indeed, respective experiments have indicated that purified SePP elicits phospholipid hydroperoxide peroxidase activity with thioredoxin as a preferred cofactor in vitro [44]. In order to delineate the significance of the two domains in a physiological model, transgenic mice with a shortened SePP isoform lacking the C-terminal Sec-rich domain were generated and compared to wild-type and classical Sepp −/− mice [45]. Again, testis and brain selenium concentrations were strongly reduced in this mouse model, only slightly higher than in Sepp −/− mice. These findings corroborate that the C-terminus is important for selenium supply to the hierarchically preferred target tissues. Selenium transport limited to the single N-terminal Sec residue is thus not sufficient to maintain normal selenium homeostasis. Shorter SePP isoforms, which might prematurely terminate at the initial Sec residues, have been described in rat and mouse serum, but their physiological function and regulation remain to be studied (1).
3.3 SePP in the Liver
Liver is the central organ for selenium organification and selenium metabolism. Several studies with labeled selenocompounds have indicated that liver is the organ converting dietary selenium into circulating SePP for supply of other tissues [12, 46]. This interpretation is in line with clinical data, e.g., the reduced serum selenium and SePP concentrations in patients with liver disease [47]. But SePP is expressed in most tissues [48]. In order to define the importance of hepatic SePP for regular selenium metabolism, mice carrying a conditional allele of tRNA[Ser]Sec (Trsp fl/fl) were crossed with a cell-specific Albumin-Cre strain abrogating selenoprotein biosynthesis specifically in hepatocytes [49]. The mice were viable and showed almost complete loss of hepatic Trsp at 3 weeks of age. As expected, residual expression of hepatic selenoproteins was minimal, including SePP, causing strongly reduced circulating selenium and SePP concentrations [49, 50].
When different tissues were compared with respect to their dependence on hepatically derived SePP, it appeared that kidney selenium and kidney-derived Gpx3 concentrations were strongly reduced in Alb-Cre; Trsp fl/fl mice, while brain selenium remained unaffected [50]. These findings lent further support to the importance of liver for regular selenium metabolism and suggested cerebral SePP to contribute to the local “SePP-cycle.” In how far hepatic SePP was sufficient to support kidney, brain, testes, and other organs with the essential trace element was studied in a complementary mouse model. Here, hepatocyte-specific expression of a human SEPP1 transgene was studied on a Sepp −/− background generating mice with SePP expression in liver only [33]. Compared to Sepp −/− mice, those with liver-specific expression of SEPP1 had increased selenium concentrations in most tissues, were less sensitive to selenium restriction in terms of neurological dysfunction, and had restored male fertility [33].
Collectively, these mouse models highlighted the importance of liver-derived SePP for regular selenium metabolism and tissue supply. Nevertheless, without locally expressed SePP, the brain was, e.g., still more sensitive to selenium restriction despite circulating SePP availability. This observation indicates that hepatic SePP was essential for regular selenium transport into brain but not fully sufficient to sustain the regular selenium homeostasis in all tissues, especially in the preferentially supplied central nervous system.
3.4 Selenoprotein Metabolism in the Brain
SePP is locally expressed in the human brain [51, 52]. In our current model, SePP is an endogenous device both to transport selenium into and within the brain. Lrp8, a neuronal SePP receptor, is important for selenium uptake by neurons [19], although Lrp8 may not represent the only SePP receptor in the brain (see Chap. 18 for a detailed discussion). Megalin likely contributes to selenium uptake along the blood–brain barrier [27]. The roles of various selenoproteins in brain development, function, and degeneration are treated in Chap. 18.
3.5 SePP in the Kidney
The importance of SePP for kidney selenium status and metabolism has not been addressed by tissue-specific knockout studies of SePP. Instead, the physiological role of SePP for kidney selenium can be deduced from a number of findings in the aforementioned SePP-specific mouse models. Sepp −/− mice showed strongly decreased kidney selenium concentrations. This finding implies that either hepatically derived circulating SePP transports selenium to the kidneys or renal SePP biosynthesis itself is crucially important for controlling local tissue selenium content [15, 16]. In order to solve this conundrum, hepatic or renal SePP biosynthesis needs to be specifically disrupted.
The former was achieved by hepatocyte-specific inactivation of Trsp impairing biosynthesis of all selenoproteins in hepatocytes [50]. Strongly reduced SePP levels in plasma were determined in parallel to reduced kidney selenium concentrations. Reduced renal selenoprotein expression in Sepp −/− mice was rescued by hepatic expression of the human SEPP1 transgene [33]. Yet, wild-type levels of kidney selenium were not completely restored, either because of the lower general selenium status of the animals or because of the missing renal SePP expression. Together, these data indicate that circulating SePP contributes to renal selenium levels, but do not completely rule out a role for local SePP biosynthesis controlling renal selenium concentrations.
Lrp2 is abundantly expressed in the kidneys [53]. Lrp2/megalin has been implicated as a renal SePP receptor [17], but Lrp2 −/− mice analyzed in this pioneering study did not survive birth, and thus a role of Lrp2 in renal SePP uptake could not be directly demonstrated. A tissue-specific mouse model has been generated by crossing Lrp2 fl/fl mice with renal tubule-specific ApoE-Cre mice. These mice were fertile and viable, but suffered from symptoms of osteomalacia secondary to vitamin D loss via the urine and hypocalcemia [54]. Urinary Se-loss and renal selenoprotein expression have not been analyzed in these mice.
We have taken advantage of another Lrp2 mutant mouse strain of which a significant fraction of megalin-deficient mice survive into adulthood. These mice carry a missense mutation in the extracellular domain of Lrp2 developing a less severe phenotype as compared to classical Lrp2 −/− mice [39]. When selenium metabolism was analyzed in these Lrp2-mutant mice, selenium status was low, GPx activities were decreased in kidney and serum, and SePP concentrations were reduced in serum [27]. Movement coordination deteriorated in Lrp2-mutant mice when challenged by feeding a low selenium diet. Interestingly, full-length SePP was detected in the urine of these mice indicating, on the one hand, that SePP is partially filtrated by the glomeruli into the primary urine and, on the other hand, that renal Lrp2/megalin recognizes, binds, and removes SePP from the primary urinary filtrate and prevents SePP loss in wild-type mice [27]. These findings provided the physiological support to the initial demonstration of specific SePP binding to the renal proximal tubule epithelium as seen in ligand blotting assays [17].
A reduction of immature SePP fragments in renal lysates prepared from Lrp2-mutant mice was also observed [27]. This finding suggests that SePP is synthesized in the kidney and may contribute to circulating SePP levels. However, to firmly make this point, kidney-specific Sepp-deficient mice need to be generated and analyzed. Activities of plasma GPx3 and renal GPx1 are reduced in Lrp2-mutant mice, suggesting that renal selenoprotein synthesis depends in part on selenium internalization from the primary urine via Lrp2. Whether patients with mutations in LRP2 also suffer urinary selenium loss has not been tested.
4 Integrated View on Selenium Metabolism via SePP–Lrp Interaction: The SePP-Cycle
Based on available data, the sequence of SePP biosynthesis, secretion, and reuptake can be envisaged as a SePP-cycle. It may underlie some aspects of the hierarchical retention of selenium in certain tissues (Fig. 16.3). This so-called SePP-cycle appears to protect brain from selenium loss during selenium deficiency, might be of central importance for kidney selenium metabolism protecting the organism from excess selenium loss by renal SePP biosynthesis, and is likely involved in testes selenium uptake and use.
5 Regulation of SePP Expression
SePP gene expression has been studied in several cell types and experimental models. Proinflammatory cytokines such as interleukin-1α, TNFα, and interferon-γ suppress gene expression in cell lines involving activation of nitric oxide synthase-2 [55, 56], and TGFβ represses SePP transcription by a SMAD-binding element in the proximal human promoter [57].
Recently, also positive effects on the human SePP promoter were demonstrated by the forkhead box transcription factor FoxO1a, and this effect was enhanced by overexpression of peroxisomal proliferator-activated receptor-γ coactivator 1α (PGC-1α) [58]. These observations link SePP expression in human hepatoma and neuroblastoma cells to repression by insulin, and can explain SePP stimulation by the glucocorticoid dexamethasone. In contrast, high SePP levels have been associated with insulin resistance/type 2 diabetes. However, high glucose levels augmented SePP expression and secretion in cultured hepatocytes [59]. Moreover, SePP is proposed to serve as an insulin-antagonistic hepatokine [60]. This study, unfortunately, has not addressed the established role of SePP as a selenium transport protein, and thus failed to consider SePP-dependent changes in selenoprotein expression in insulin target tissues. This would have been important, since enhanced expression of GPx1 is known to cause insulin resistance in mice [61].
6 Comparison of Experimental Concepts with Clinical Data
A systematic comparison of potential biomarkers of selenium status in humans has recently been compiled and published [62]. Plasma or red blood cell selenium concentrations or GPx activities in serum, plasma, or blood cells are often used as markers of selenium status. In comparison, SePP turned out to be another versatile endpoint in populations with low to moderate selenium supply reaching a plateau at higher intake levels than cell GPx1 or circulating GPx3 activities. Several groups have concluded that SePP serum concentration represents the best diagnostic indicator of adequate selenium status in humans [63–65], provided that underlying liver, kidney, or inflammatory diseases have been excluded as confounding factors.
Recent population-based studies on the associations between various cancer forms and SNPs of genes encoding for selenoproteins and enzymes involved in metabolism of ROS provided some evidence that SePP variants (Ala234Thr, rs3877899; G > A in 3′ UTR, rs7579) affect selenium availability to target tissues such as prostate or colon thereby modulating cancer risk in the context of other gene–gene (e.g., SOD2), gene–nutrient and life style interactions [66–69]. These associations and the postulated underlying SePP-dependent selenium uptake and supply mechanisms need to be confirmed by independent studies. Decreased expression of SePP mRNA and SePP protein has been reported for several preneoplastic and cancerous lesions, e.g., of the respiratory and the GI tracts (gastric, colorectal, and hepatic cancers) as well as for prostate [70–73]. Unfortunately, SePP status has not been monitored in several other relevant and large cancer, cardiovascular, and metabolic trials (e.g., SELECT, NPC, SU.VI.MAX, SETCAP, etc.) analyzing potential protective or therapeutic effects of supplementation with selenocompounds alone or in combination with other antioxidative compounds such as vitamin E [74–76].
The recent availability of several specific antibodies recognizing human SePP helped to clarify the picture of systemic SePP distribution vs. local production indicated by cellular expression of SePP transcripts. These studies confirmed previous hints that SePP reaches various tissues and cells via circulation, but also provided evidence for local SePP production and secretion, e.g., within the CSF and in ependymal cells in the brain [51, 52]. SePP expression and immunostaining showed specific spatial and temporal patterns during brain development and pathological alterations in brains from patients suffering from neurodegenerative diseases such as Alzheimer’s [1, 77]. Together, these observations suggest a strategic location of SePP in brain potentially protecting cell types of high activity and functional relevance from selenium deficiency thereby ensuring regular development, differentiation, and expression of Se-dependent antioxidative defense systems.
Patients on chronic hemodialysis and apheresis are known to have an impaired selenium status and frequently receive selenium supplements [78]. Currently, it is not clear, whether they lose SePP or its (shorter) isoforms during the filtration process or whether their damaged renal tissue expresses insufficient Lrp2/megalin for adequate reabsorption of filtrated SePP. Since a low selenium status is a negative prognostic factor for long-term survival of chronically ill patients, it appears mandatory to control the trace element status of hemodialysis patients in order to avoid severe selenium deficiency [79].
Besides cancer, chronic and degenerative diseases, the selenium status and SePP are implicated in male fertility, which is reviewed in detail in Chap. 32. A genetic inherited defect causing an impaired SePP biosynthesis and low circulating SePP levels has recently been described in humans. Individuals with certain mutations in SECISBP2 display very low or undetectable levels of SePP [80]. Interestingly, some of these subjects are reported with mental retardation and abnormal gait [81] or delayed neurological and motor skill milestones [82]. However, apparent SePP deficiency in patients carrying SECISBP2 mutations does not lead to a phenotype as severe as in Sepp −/− mice, indicating that brain selenium metabolism is not completely impaired in these individuals. In contrast, severe neurological symptoms involving brain atrophy and epilepsy were recently reported in patients carrying a mutation in another rate-limiting factor of selenoprotein biosynthesis, i.e., the selenocysteine synthase gene, SEPSECS [83]. However, selenium and SePP status in the circulation or the CSF have not been determined in SEPSECS-deficient patients, but are likely reduced and involved in the clinical phenotype.
7 Summary
There is a functional interaction of hepatically derived or tissue-derived SePP and SePP-receptors from the Lrp family, namely Lrp2 and Lrp8. This interaction ensures the hierarchical supply and retention of selenium in testes and brain, and the general retention of SePP in mammals by preventing its loss via the urine. Pharmacological intervention of these endocytic receptor/SePP interactions might become of importance in cases of certain forms of male infertility, neurodegenerative disorders, or in patients exposed to excess oxidative stress, e.g., during various forms of chemotherapy, systemic inflammation, and bacterial or viral infections.
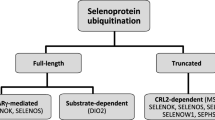
One of the important experimental tasks in the future will thus be the molecular characterization of the different SePP isoforms, their physiological functions, regulation, and interaction with the different SePP-receptors. Some evidence has been provided that Lrp8/apoER2 may be selective for full-length SePP, while Lrp2/megalin also accepts shorter SePP isoforms [1].
Of particular interest is also the relation between SePP-dependent delivery of selenium to the kidneys in comparison to the local recycling, biosynthesis, and secretion of renal-derived GPx3, which constitutes the second selenoprotein significantly contributing to the circulating blood selenium content. Our current knowledge is limited with regard to expression and regulation of SePP during development, selenium compartmentalization, and supply to tissues and cells not depending on SePP and devoid of the Lrp receptors. The molecular aspects of SePP downregulation in various cancer cells are not yet understood. Whether impaired expression and secretion of SePP during hepatic acute phase response and in various cancer cells can be overcome to improve the health status and better recovery from these diseases remains one prime challenge for future studies. Nevertheless, with the identification of SePP as the major transport, distribution, and storage protein for Se, and the characterization of specific receptor-mediated tissue-specific uptake processes, a number of previous enigmatic findings are now understood by a plausible molecular pathway. But given the promiscuity of both Lrp2 and Lrp8 for the alleged substrates to be recognized, bound, and internalized, future studies will also need to address specificity of the SePP/Lrp interactions in more detail.
References
Burk RF, Hill KE (2009) Biochim Biophys Acta 1790:1441
Flohé L (2009) Biochim Biophys Acta 1790:1389
Burk RF, Hill KE (2005) Annu Rev Nutr 25:215
Schomburg L, Schweizer U, Köhrle J (2004) Cell Mol Life Sci 61:1988
Moschos MP (2000) Cell Mol Life Sci 57:1836
Mostert V (2000) Arch Biochem Biophys 376:433
Motsenbocker MA, Tappel AL (1982) Biochim Biophys Acta 719:147
Gomez B Jr, Tappel AL (1989) Biochim Biophys Acta 979:20
Yang JG, Hill KE, Burk RF (1989) J Nutr 119:1010
Hill KE, Lloyd RS, Yang JG et al (1991) J Biol Chem 266:10050
Lobanov AV, Hatfield DL, Gladyshev VN (2008) Genome Biol 9:R62
Suzuki KT, Ishiwata K, Ogra Y (1999) Analyst 124:1749
Saito Y, Takahashi K (2002) Eur J Biochem 269:5746
Yan J, Barrett JN (1998) J Neurosci 18:8682
Hill KE, Zhou J, McMahan WJ et al (2003) J Biol Chem 278:13640
Schomburg L, Schweizer U, Holtmann B et al (2003) Biochem J 370:397
Olson GE, Winfrey VP, Hill KE et al (2008) J Biol Chem 283:6854
Olson GE, Winfrey VP, Nagdas SK et al (2007) J Biol Chem 282:12290
Burk RF, Hill KE, Olson GE et al (2007) J Neurosci 27:6207
Herz J, Bock HH (2002) Annu Rev Biochem 71:405
Willnow TE, Nykjaer A (2010) Mol Cell Endocrinol 316:93
Christensen EI, Birn H (2002) Nat Rev Mol Cell Biol 3:256
Andreassen TK (2006) Horm Metab Res 38:279
Negri AL (2006) Nephrology (Carlton) 11:510
Adams JS (2005) Cell 122:647
Homer 800BC Greek Epic Poetry 1
Chiu-Ugalde J, Theilig F, Behrends T et al (2010) Biochem J 431:103
Hirotsune S, Takahara T, Sasaki N et al (1995) Nat Genet 10:77
Trommsdorff M, Gotthardt M, Hiesberger T et al (1999) Cell 97:689
D’Arcangelo G, Miao GG, Chen SC et al (1995) Nature 374:719
Schweizer U, Michaelis M, Köhrle J et al (2004) Biochem J 378:21
Olson GE, Winfrey VP, Nagdas SK et al (2005) Biol Reprod 73:201
Renko K, Werner M, Renner-Müller I et al (2008) Biochem J 409:741
Hill KE, Zhou J, McMahan WJ et al (2004) J Nutr 134:157
Schweizer U, Schomburg L, Savaskan NE (2004) J Nutr 134:707
Burk RF, Hill KE, Motley AK et al (2006) Biochim Biophys Acta 1760:1789
Suzuki KT, Kurasaki K, Okazaki N et al (2005) Toxicol Appl Pharmacol 206:1
Willnow TE, Hilpert J, Armstrong SA et al (1996) Proc Natl Acad Sci USA 93:8460
Zarbalis K, May SR, Shen Y et al (2004) PLoS Biol 2:E219
Andersen OM, Yeung CH, Vorum H et al (2003) J Biol Chem 278:23989
Ursini F, Heim S, Kiess M et al (1999) Science 285:1393
Kehr S, Malinouski M, Finney L et al (2009) J Mol Biol 389:808
Saito Y, Sato N, Hirashima M et al (2004) Biochem J 381:841
Takebe G, Yarimizu J, Saito Y et al (2002) J Biol Chem 277:41254
Hill KE, Zhou J, Austin LM et al (2007) J Biol Chem 282:10972
Burk RF, Hill KE, Read R et al (1991) Am J Physiol 261:E26
Burk RF, Early DS, Hill KE et al (1998) Hepatology 27:794
Dreher I, Schmutzler C, Jakob F et al (1997) J Trace Elem Med Biol 11:83
Carlson BA, Novoselov SV, Kumaraswamy E et al (2004) J Biol Chem 279:8011
Schweizer U, Streckfuss F, Pelt P et al (2005) Biochem J 386:221
Scharpf M, Schweizer U, Arzberger T et al (2007) J Neural Transm 114:877
Bellinger FP, He QP, Bellinger MT et al (2008) J Alzheimers Dis 15:465
Willnow TE, Nykjaer A, Herz J (1999) Nat Cell Biol 1:E157
Leheste JR, Melsen F, Wellner M et al (2003) FASEB J 17:247
Dreher I, Jakobs TC, Köhrle J (1997) J Biol Chem 272:29364
Speckmann B, Pinto A, Winter M et al (2010) Free Radic Biol Med 49:777
Mostert V, Dreher I, Köhrle J et al (2001) Biofactors 14:135
Speckmann B, Walter PL, Alili L et al (2008) Hepatology 48:1998
Speckmann B, Sies H, Steinbrenner H (2009) Biochem Biophys Res Commun 387:158
Misu H, Takamura T, Takayama H et al (2010) Cell Metab 12:483
McClung JP, Roneker CA, Mu W et al (2004) Proc Natl Acad Sci USA 101:8852
Ashton K, Hooper L, Harvey LJ et al (2009) Am J Clin Nutr 89:2025S
Xia Y, Hill KE, Byrne DW et al (2005) Am J Clin Nutr 81:829
Burk RF, Norsworthy BK, Hill KE et al (2006) Cancer Epidemiol Biomarkers Prev 15:804
Méplan C, Crosley LK, Nicol F et al (2007) FASEB J 21:3063
Peters U, Chatterjee N, Hayes RB et al (2008) Cancer Epidemiol Biomarkers Prev 17:1144
Cooper ML, Adami HO, Gronberg H et al (2008) Cancer Res 68:10171
Méplan C, Hughes DJ, Pardini B et al (2010) Carcinogenesis 31:1074
Steinbrecher A, Méplan C, Hesketh J et al (2010) Cancer Epidemiol Biomarkers Prev
Mörk H, al-Taie OH, Bähr K et al (2000) Nutr Cancer 37:108
Calvo A, Xiao N, Kang J et al (2002) Cancer Res 62:5325
Al-Taie OH, Uceyler N, Eubner U et al (2004) Nutr Cancer 48:6
Li CL, Nan KJ, Tian T et al (2007) World J Gastroenterol 13:2363
Lippman SM, Klein EA, Goodman PJ et al (2009) JAMA 301:39
Hercberg S, Preziosi P, Briancon S et al (1998) Control Clin Trials 19:336
Schnabel R, Lubos E, Messow CM et al (2008) Am Heart J 156(1201):e1
Zhang S, Rocourt C, Cheng WH (2010) Mech Ageing Dev 131:253
Tonelli M, Wiebe N, Hemmelgarn B et al (2009) BMC Med 7:25
Geoghegan M, McAuley D, Eaton S et al (2006) Curr Opin Crit Care 12:136
Dumitrescu AM, Liao XH, Abdullah MS et al (2005) Nat Genet 37:1247
Azevedo MF, Barra GB, Naves LA et al (2010) J Clin Endocrinol Metab 95:4066
Schoenmakers E, Agostini M, Mitchell C et al (2010) J Clin Invest 120:4220
Agamy O, Ben Zeev B, Lev D et al (2010) Am J Hum Genet 87:538
Acknowledgements
Work in the authors’ labs is supported by the German Research Foundation (DFG: GraKo 1208/2, Scho 849/2-2) and German Cancer Aid (Deutsche Krebshilfe, 10-1792 Scho2, 108 426).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Köhrle, J., Schweizer, U., Schomburg, L. (2011). Selenium Transport in Mammals: Selenoprotein P and Its Receptors. In: Hatfield, D., Berry, M., Gladyshev, V. (eds) Selenium. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-1025-6_16
Download citation
DOI: https://doi.org/10.1007/978-1-4614-1025-6_16
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-1024-9
Online ISBN: 978-1-4614-1025-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)