
Abstract
To fully utilize the advantages of cardiac CTA, it is important to consider radiation exposure and to optimize scanning techniques. Recent advances in multidetector CT (MDCT) technology have revolutionized cardiovascular imaging in children with complex congenital heart disease. For infants with congenital heart disease, ECG-gated cardiac CTA is the modality of choice for imaging the coronary arteries, airway, and extracardiac vascular structures. Fast scanning times and high-quality evaluation of both complex cardiac and coronary anatomy have enabled CTA to aid in patient management and treatment planning. Currently, there are two accepted cardiac CTA scanning techniques for infants with congenital heart disease: retrospective and prospective ECG-gated scanning.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
To fully utilize the advantages of cardiac CTA, it is important to consider radiation exposure and to optimize scanning techniques. Recent advances in multidetector CT (MDCT) technology have revolutionized cardiovascular imaging in children with complex congenital heart disease. For infants with congenital heart disease, ECG-gated cardiac CTA is the modality of choice for imaging the coronary arteries, airway, and extracardiac vascular structures. Fast scanning times and high-quality evaluation of both complex cardiac and coronary anatomy have enabled CTA to aid in patient management and treatment planning. Currently, there are two accepted cardiac CTA scanning techniques for infants with congenital heart disease: retrospective and prospective ECG-gated scanning.
Technique
General anesthesia is administered routinely in infants less than 1 year of age to optimize the scans. All examinations are performed with multidetector scanners. The following parameters are given for a GE 64-slice MDCT: 4 cm detector length. Iodinated contrast medium is used at 1 mL/lb of body weight, with an injection speed of 0.7 mL/s. A weight-based protocol is used, with 80-kVp tube voltage and tube current adjusted according to body weight for prospective scanning. Tube current adjustment to body weight varies from institution to institution and may range from 10 to 40 mA/kg [1, 2]. The gantry speed is set at a 0.35-s rotation with a helical thickness of 0.6 mm and detector coverage of 40 mm. The technologist begins the scan when contrast fills the ventricle. The patient is scanned in a craniocaudal direction starting at the level of the subclavian artery and ending at the level of the diaphragm. The anesthesiologist assists with the breath hold. β-Blockers typically are not used to decrease the heart rate in children with congenital heart disease.
Retrospective Scanning
During retrospective scanning, the x-ray beam is turned on during the entire cardiac cycle and spiral scanning continues during table motion (Fig. 2.1). Retrospective gating uses a low pitch (0.2) to obtain attenuation measurements at all spatial locations in the heart and to scan during all phases of the cardiac cycle, including the entire R-R interval. The pitch in retrospective scanning depends on the heart rate. Pitch normally falls in the range of 0.2–0.24 for infants with heart rates above 100 bpm. The current in retrospective scanning is set at 250–300 mA.

Retrospective ECG-gated scan. The x-ray beam (in blue) is on through the entire cardiac cycle
Prospective Scanning
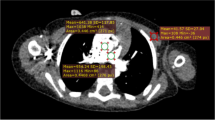
The vast majority of scanning can and should be done using the prospective ECG-triggered scanning technique, even in children and infants with very fast heart rates. This technique uses a nonspiral step-and-shoot axial scanning process in which the x-ray beam is on for a short time and is turned off as the table moves. The imaging window is approximately 50 % of the cardiac cycle. Because an infant’s heart rate is relatively high, short acquisition times with padding may be used to capture up to 50 % of the cardiac cycle to evaluate function (Fig. 2.2); when functional analysis is needed, 175 ms of padding should be used. The padding turns the tube on before the required acquisition time and leaves it on afterward, increasing the time the current is on to include more of the cardiac cycle (Fig. 2.3) for functional imaging. For prospective scanning, our tube current–body weight adjustment has three weight based settings. Typically, end systole is the time for imaging the coronary arteries in adults, with optimal visualization between 65 and 80 % of the cardiac cycle. In infants, the optimal time for imaging the coronary arteries typically is during systole, at 45–55 % of the cardiac cycle.

Prospective ECG-gated scan. The x-ray beam (in blue) is not on during the entire cardiac cycle. Notice the rapid heart rate of 140 bpm. The rapid heart rate is advantage as the scan time covers enough of the cardiac cycle so that functional information can be obtained with provided with postprocessing

Padding. Padding of 175 ms (yellow) is used to flank the acquisition time (green) to include more cardiac phases
Prospective Versus Retrospective Scanning (Table 2.1)
Radiation Dose
Children are more sensitive than adults to the effects of ionizing radiation; therefore, it is essential to balance image quality with radiation dose delivered when performing CTA in children. It is important to apply the ALARA (As Low As Reasonably Achievable) principle for infants and neonates by using low peak kilovoltage and adapting the milliamperes to the patient’s weight. Published studies comparing retrospective with prospective ECG-gated scanning techniques have reported radiation dose savings ranging from two to four times with prospective ECG-gated techniques [1–4]. Radiation doses estimated for prospective ECG-gated protocols have been reported to be less than 1 mSv in studies using low peak kilovoltage and low milliamperes per kilogram. On the contrary, retrospective ECG-gated scanning yields higher radiation doses, estimated to be around 3–10 mSv, even with the low-dose technique [5–10]. Another technique that may be used to lower the radiation dose for the patient is adaptive statistical iterative reconstruction, a unique CT reconstruction algorithm with matrix algebra used to selectively identify and subtract noise from the image. The result is less noise or the same amount of noise with less radiation [8–11].
CT Data Postprocessing and Analysis
At our institution, all images have a reconstruction section thickness of 0.625 mm and a section interval of 0.625 mm with use of a small cardiac field of view. The lung window is reconstructed at a 2.5-mm section. All images obtained are transferred to an external workstation, where they are reconstructed with multiplanar reformation, volume rendering, and maximum intensity projections. The protocol parameters used at our institution are described in detail in Table 2.2.
References
Jin KN, Park EA, Shin CI, Lee W, Chung JW, Park JH. Retrospective versus prospective ECG-gated dual-source CT in pediatric patients with congenital heart diseases: comparison of image quality and radiation dose. Int J Cardiovasc Imaging. 2010;26 Suppl 1:63–73.
Hollingsworth CL, Yoshizumi TT, Frush DP, Chan FP, Toncheva G, Nguyen G, et al. Pediatric cardiac-gated CT angiography: assessment of radiation dose. AJR Am J Roentgenol. 2007;189(1):12–8.
Paul JF, Rohnean A, Elfassy E, Sigal-Cinqualbre A. Radiation dose for thoracic and coronary step-and-shoot CT using a 128-slice dual-source machine in infants and small children with congenital heart disease. Pediatr Radiol. 2011;41(2):244–9.
Paul JF, Rohnean A, Sigal-Cinqualbre A. Multidetector CT for congenital heart patients: what a paediatric radiologist should know. Pediatr Radiol. 2010;40(6):869–75.
Hirai N, Horiguchi J, Fujioka C, Kiguchi M, Yamamoto H, Matsuura N, et al. Prospective versus retrospective ECG-gated 64 detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology. 2008;248(2):424–30.
Kuettner A, Gehann B, Spolnik J, Koch A, Achenbach S, Weyand M, et al. Strategies for dose-optimized imaging in pediatric cardiac dual source CT. Rofo. 2009;181(4):339–48.
Huang B, Law MW, Mak HK, Kwok SP, Khong PL. Pediatric 64-MDCT coronary angiography with ECG-modulated tube current: radiation dose and cancer risk. AJR Am J Roentgenol. 2009;193(2):539–44.
Al-Mousily F, Shifrin RY, Fricker FJ, Feranec N, Quinn NS, Chandran A. Use of 320-detector computed tomographic angiography for infants and young children with congenital heart disease. Pediatr Cardiol. 2011;32(4):426–32.
Pages J, Buls N, Osteaux M. CT doses in children: a multicentre study. Br J Radiol. 2003;76(911):803–11.
Deak PD, Smal Y, Kalender WA. Multisection CT protocols: sex- and age-specific conversion factors used to determine effective dose from dose-length product. Radiology. 2010;257(1):158–66.
Li X, Samei E, Segars WP, Sturgeon GM, Colsher JG, Frush DP. Patient-specific radiation dose and cancer risk for pediatric chest CT. Radiology. 2011;259(3):862–74.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Richardson, R.R., Chau, C. (2013). Scanning Technique for Cardiac CTA in Infants and Small Children. In: Atlas of Pediatric Cardiac CTA. Springer, New York, NY. https://doi.org/10.1007/978-1-4614-0088-2_2
Download citation
DOI: https://doi.org/10.1007/978-1-4614-0088-2_2
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4614-0087-5
Online ISBN: 978-1-4614-0088-2
eBook Packages: MedicineMedicine (R0)