
Abstract
Inefficient cooking with biomass fuels in poorly ventilated homes is a major source of exposure to indoor air pollution in developing countries. Household air pollution from cooking and heating with biomass fuels also is an important contributor to outdoor air pollution. The combustion of wood and other biomass is qualitatively similar to the burning of tobacco in terms of emissions of particulate matter and gases, and the mechanisms by which biomass smoke causes adverse health effects in humans are likely similar to those involved in tobacco smoke-induced disease processes. The public health impact of domestic cooking with biomass is great. The 2010 Global Burden of Disease comparative risk assessment found household air pollution from solid fuel (biomass and coal) use to be responsible for approximately 4.8 % of the total disability-adjusted life years and 3.9 million premature deaths per year. Household air pollution ranked third on the examined list of risk factors globally and was the most important environmental risk factor. The estimates are based on the strength of the evidence, primarily meta-analyses of epidemiological studies of acceptable scientific quality, although for cardiovascular disease the evidence is more inferential. The greatest burden of household air pollution–related premature deaths is in children with pneumonia exposed to biomass smoke. The greatest burden in adults is for cardiovascular disease, but for non-smoking women, chronic obstructive pulmonary disease (COPD) is an important cause of disability and death. Household air pollution also contributes to the burden of cataracts, the leading cause of blindness, and lung cancer, especially among women. Research gaps and opportunities for interventions to reduce impacts of biomass smoke on public health are identified.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
14.1 Introduction
Inefficient cooking with biomass fuels in poorly ventilated homes is a major source of exposure to indoor air pollution in the developing world. The levels of exposure to particulate matter (PM) from biomass smoke in such homes are often at least an order of magnitude higher than the highest concentrations that occur in the ambient air of the developed world (Bruce et al. 2000; Diette et al. 2012). Household air pollution from cooking and heating with biomass fuels also is an important contributor to outdoor air pollution, accounting for an estimated 10 % of ambient fine PM (PM2.5) (Smith et al. 2014).
Biomass fuel refers to any recently living plant- and/or animal-based material that is deliberately burned by humans as fuel, including wood, crop residues, and animal dung (Bruce et al. 2000). The number of people reliant on biomass fuels is projected to increase to 2.6 billion by 2030 (Smith et al. 2013). Most of these people live in rural areas of lesser-developed countries (LDCs), where some four-fifths of households rely on biomass fuels as their major or only source of domestic energy for cooking and sometimes space heating (World Health Organization 2009).
Cooking with biomass fuels is generally done on unvented stoves typically consisting of such simple arrangements as three rocks, a U-shaped hole in a block of clay, or a pit in the ground (Smith et al. 2013). Combustion under such conditions is inefficient and therefore incomplete products of combustion are generated. This typically leads to extremely high pollutant concentrations in the vicinity of the stove. Pollutant concentrations are further exacerbated by the lack of ventilation that characterizes many of the kitchens in rural areas of developing countries.
The high levels of smoke from cooking indoors with biomass fuels commonly contain up to 1,000 μg/m3 particulate matter with a diameter of 5 μm or less (PM5) and much higher values have been reported (Smith et al. 2013; Balakrishnan et al. 2013). These concentrations are orders of magnitude higher than either the U.S. Environmental Protection Agency national ambient air quality standard for PM10 or the World Health Organization (WHO) guideline. In addition to PM, carbon monoxide (CO), nitrogen oxides, formaldehyde, and a number of toxic organic compounds [e.g., benzene; 1,3 butadiene; benzo[α]pyrene and other polycyclic aromatic hydrocarbons (PAHs)] are present in biomass smoke, depending on the type of fuel that is burned (Warwick and Doig 2004). Readers are referred to Chap. 6 for details on potential carcinogenic effects of these constituents. The combustion of wood and other biomass is qualitatively similar to the burning of tobacco in terms of emissions of PM and gases, although without the nicotine.
In rural areas of lesser developed countries, women often spend many hours a day cooking so duration of exposure to biomass smoke is often considerable. The potential for exposure is further increased by common cultural practices. Infants and toddlers are often carried on the mother’s back while she cooks so that from early infancy children spend hours breathing smoke from cooking or heating fires (Armstrong and Campbell 2009). In temperate climates and highland areas, people spend more time indoors to protect themselves from the cold, and the cold temperatures that characterize these areas require fires that burn over extended periods and tighter house construction (i.e., less ventilation) for space heating (Smith et al. 2013). Thus, both pollution levels and exposure times increase.
The public health impact of the relatively high exposures to PM in homes where cooking is done with inefficient, poorly ventilated stoves using biomass fuels is great. The latest version of the Global Burden of Disease comparative risk assessment undertaken in 2010 found household air pollution from solid fuel use to be responsible for approximately 4.8 % of the total global burden of disease disability-adjusted life years and 3.9 million premature deaths per year (Lim et al. 2012; Smith et al. 2014). Household air pollution ranked third on the examined list of risk factors globally and was the most important environmental risk factor. The estimates are based on the strength of the evidence, primarily meta-analyses of epidemiological studies of acceptable scientific quality, although for cardiovascular disease the evidence is more inferential (see Sect. 14.8). The greatest burden of household air pollution-related premature deaths is in children with pneumonia exposed to biomass smoke. The greatest burden in adults is for cardiovascular disease, but for non-smoking women, chronic obstructive pulmonary disease (COPD) is also an important cause of disability and death. Household air pollution also contributes to the burden of cataracts, the leading cause of blindness, and lung cancer, especially among women. It is also worthy of note that an estimated 16 % of the global burden of disease attributed to ambient PM pollution comes from household combustion of solid fuel. The burden of disease due to household air pollution falls hardest on poor populations in Africa, Latin America, and Asia.
In some parts of the world, poorly burned solid fuels are commonly used for space heating and/or lighting, as well as cooking. The 2010 comparative risk assessment for household air pollution was explicitly limited to exposures related to cooking with solid fuels, and did not include other sources of exposure, largely because of lack of data. Because exposures to pollutants do occur from combustion for space heating and lighting as well as cooking with non-solid fuels, such as kerosene, future assessments will consider these sources as better data accumulate.
14.2 Mechanisms
The mechanisms by which biomass smoke causes adverse health effects in humans are likely similar to those involved in tobacco smoke and combustion-generated PM pathogenic processes. Oxidative stress in the airways and alveoli leads to stimulation of alveolar macrophages and injury to the epithelial lining, which in turn attracts inflammatory cells from the circulation. This local lung inflammatory reaction can spill over into the systemic circulation and contribute to adverse effects in other organs, such as the cardiovascular system, and the fetus in pregnant women. Alveolar macrophages laden with carbon particles from biomass smoke may contribute to increased risk of respiratory tract infections. The pathways involved in biomass smoke-induced lung carcinogenesis are probably identical to those by which tobacco smoke induces lung cancers.
Although the toxicological literature for biomass smoke is much less rich than for tobacco smoke and PM, a number of animal and in vitro studies have been reported and were referenced in a recent review paper (Migliaccio and Mauderly 2010). Pulmonary outcomes have been best studied in animal models, including airway responsiveness, lung function, effects on surfactant, epithelial damage, inflammation, edema, and antibacterial activity. Extrapulmonary outcomes have included effects on the cardiovascular system, adjuvant activity, p450 enzyme activity, glutathione depletion, and tumor/cancer growth.
A growing number of reports of controlled human exposure studies of wood smoke have been published. These studies are limited to acute effects and are specific to the fuels and burn conditions used, but evidence of systemic oxidative stress and inflammation, airway inflammation, and arterial stiffness has been observed after short-term exposure to wood smoke (Barregard et al. 2008; Sehlstedt et al. 2010; Stockfelt et al. 2012; Unosson et al. 2013). Not all studies, however, have found adverse effects (Riddervold et al. 2012; Forchhammer et al. 2012; Stockfelt et al. 2013).
14.3 Low Birth Weight
Low birth weight was not one of the conditions considered in the 2010 Global Burden of Disease effort because of lack of data from many countries. That said, there is considerable evidence of an association between biomass smoke exposure and low birth weight. A systematic review on the risk of low birth weight and solid fuel use was published in 2010 (Pope et al. 2010). The meta-analysis was updated in 2012 for a WHO report on indoor air quality. One randomized controlled trial (RCT) (Thompson et al. 2011) and six observational studies (Mavalankar et al. 1992; Boy et al. 2002; Mishra et al. 2004; Siddiqui et al. 2008; Tielsch et al. 2009; Abusalah et al. 2011) on the risk of low birth weight (<2,500 g at term) were reviewed. The pooled odds ratio (OR) was 1.40 [95 % confidence interval (CI): 1.26–1.54].
The biological plausibility of a biomass smoke effect on birth weight is supported by a similar and well-documented effect of in utero exposure to secondhand tobacco smoke (SHS) as well as mechanistic evidence of association between components of household air pollution (HAP) (CO, PM, and PAHs) and low birth weight. The range of reported estimates are consistent with those for related exposures, including outdoor air pollution, second hand smoking (SHS) and active smoking. The mean decrease in birth weight for biomass smoke exposure (90–100 g) lies between published estimates for SHS and active smoking, as would be expected from the relative levels of exposure to PM2.5 (Pope et al. 2010). The main deficiency of this literature is the lack of measurement of exposure to biomass smoke and thus the inability to demonstrate an exposure-response relationship. Nevertheless, the WHO report assessed the evidence of an association between biomass smoke exposure and low birth weight as moderately strong, applying Bradford Hill viewpoints, because of consistency, temporality, biological plausibility, and analogy. The one published RCT of a chimney stove provided some evidence in support of an intervention effect (Thompson et al. 2011).
14.4 Acute Lower Respiratory Infection (Childhood Pneumonia)
Acute lower respiratory infection (ALRI) is a leading contributor to the global burden of disease, accounting for 4.6 % of the total (Murray et al. 2012). Pneumonia is also the primary cause of death in children (1.4 million deaths in children younger than 5 years) and the incidence and mortality are generally highest in those countries and regions where solid fuel use is greatest (Nair et al. 2013). The relative risk of ALRIs for children exposed to household biomass smoke has been quantified in a number of studies, the majority from developing countries, but also from the United States (Torres-Duque et al. 2008). Most of these studies have used a case-control design, although several cohort studies have also been conducted. Taken together, these studies show a consistent association between solid fuel use and an increase in the risk of ALRI in exposed children. The overall estimate of the risk of ALRI from 24 studies selected for a meta-analysis conducted in preparation for the 2010 Global Burden of Disease comparative risk assessment (Dherani et al. 2008) was a pooled OR of 1.79 (CI: 1.26–2.21) for children younger than 5 years. The OR for children younger than 2 years was 1.96 (CI: 1.36–2.82). Only three studies included direct measurement of exposure, the remainder used proxies (fuel type, etc.). Outcome definitions varied from parental recall of WHO signs of ALRI to chest X-ray confirmation, and included severe and fatal outcomes; included studies had to distinguish upper from lower respiratory infections. Some evidence of an increased risk for more severe pneumonia was found. Impaired respiratory tract defense mechanisms, such as decreased mucociliary clearance and alveolar macrophage function, provide biological plausibility for the observed association between biomass smoke exposure and ALRI risk in children (Siddiqui et al. 2008; Zelikoff et al. 2002).
Only one RCT of an intervention to reduce exposure to biomass smoke to prevent childhood ALRI has been completed (Smith et al. 2011), involving 514 Guatemalan children aged <16 months, randomized to use a chimney wood stove or traditional three-stone fire. The primary outcome was physician diagnosis, with pulse oximetry to define severity. Exposure was assessed for all children using repeated CO measurements, together with co-located kitchen CO and PM2.5 measurements in a sub-sample to define the CO-PM2.5 relationship. In intention to treat analysis, child exposure was reduced by 50 %, associated with a relative risk of 0.78 (CI: 0.59, 1.06) for all physician-diagnosed pneumonia, and of 0.67 (CI: 0.45, 0.98) for severe pneumonia (defined by low oxygen saturation). Adjusted exposure-response analysis found significant relationships for both all and severe pneumonia.
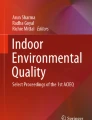
The randomized control trial to study the effect of reduction in household air pollution on childhood pneumonia in Guatemala (RESPIRE) results support a causal association between biomass smoke exposure and early childhood pneumonia and show that the greatest risk reduction occurs at lower exposure levels. The RESPIRE exposure-response data suggest that ALRI incidence would be reduced by around one-third with interventions that bring average PM2.5 down from several hundreds of μg/m3 to levels experienced by “unexposed” groups in the majority of epidemiological studies (Smith et al. 2014) (see Fig. 14.1). Reduction of exposure to biomass smoke levels at or below the WHO annual average guideline of 10 μg/m3 PM2.5 would theoretically result in larger risk benefit.

Exposure-response from the RESPIRE study for wood smoke exposure as assessed by average personal monitoring data and the rate of physician-diagnosed severe pneumonia as assessed by oxygen saturation (Reprinted from Smith et al. (2011) with permission from Elsevier)
14.5 Chronic Obstructive Pulmonary Disease
Chronic obstructive pulmonary disease is a leading cause of morbidity and mortality (~4 million deaths/year) worldwide and results in an economic and social burden that is both substantial and increasing, especially among women (Global Initiative for Chronic Obstructive Lung Disease 2014; Lozano et al. 2012). In less developed countries, a substantial proportion of COPD occurs in people who have never smoked tobacco products, especially among women cooking with stoves that emit high levels of a wide variety of pollutants similar to those present in tobacco smoke (Lim et al. 2012). Multiple case-control and cross-sectional studies have found an association between cooking with biomass fuel and chronic bronchitis or COPD when compared with lower exposure/cleaner fuels (Akhtar et al. 2007; Albalak et al. 1999; Caballero et al. 2008; Dutt et al. 1996; Ellegard 1996; Menezes et al. 1994; Qureshi 1994; Regalado et al. 2006; Saha et al. 2005; Dennis et al. 1996; Dossing et al. 1994; Ekici et al. 2005; Kiraz et al. 2003; Orozco-Levi et al. 2006; Perez-Padilla et al. 2006). Exposure was often assessed as present or absent or by daily hours spent by the stove. Most studies did not include direct measurements of specific pollutants. Studies that have measured kitchen particulate levels from biomass fuel use have confirmed very high concentrations (Albalak et al. 1999; Regalado et al. 2006), but personal measurements of exposure have not been used. Only a few cross-sectional studies have measured lung function and these studies have shown an association between biomass fuel use and chronic airflow obstruction (Caballero et al. 2008; Regalado et al. 2006). Taken together, the results of previous studies show a strong association between cooking with biomass fuel and COPD among women (Balmes 2010).
Several systematic reviews and meta-analyses have been published, including the one conducted for the 2010 Global Burden of Disease comparative risk assessment (Smith et al. 2014; Kurmi et al. 2010; Hu et al. 2010; Po et al. 2011). In the Smith et al. (2014) review 25 studies were included in the final analysis. All but seven included in the meta-analysis were cross-sectional in design. One study was a retrospective cohort (Chapman et al. 2005) and six were case-control (Dennis et al. 1996; Dossing and Khan 1994; Orozco-Levi et al. 2006; Perez-Padilla et al. 2006; Sezer et al. 2006; Xu et al. 2007). Case-control studies recruited controls from various sources, including visitors to the hospital, patients from other hospital services without presence of pulmonary disease, and population-based selection. Heterogeneous exposure measures were used in these studies, including rural-urban comparisons (where data supported the use of place of residence as a proxy for fuel use), outdoor versus indoor cooking, fuel type for cooking and/or heating, stove type and time-exposed to biomass fuel combustion. The pooled OR was 1.94 (CI: 1.62–2.33). Stratified analysis by gender showed a stronger association between exposure to biomass smoke and COPD in women [OR, 2.30 (CI: 1.73-3.06)] than in men [OR, 1.90 (CI: 1.15–3.13)]. The association in women remained significant even after adjusting for both age and smoking, while this was not the case for men.
Three other recently published systematic reviews and meta-analyses reported similar summary estimates for the effect of biomass smoke on risk of COPD. Kurmi et al. (2010) reported a summary OR (CI) for the use of solid fuels and COPD from 23 studies of 2.80 (CI: 1.85–4.0) and for biomass smoke and chronic bronchitis of 2.32 (1.92–2.80). Pooled estimates for different types of fuel showed that exposure to wood smoke carried a greater risk than coal (also seen in the Global Burden of Disease meta-analysis). Hu et al. (Hu et al. 2010) reported a summary OR from 15 studies of 2.44 (CI: 1.9–3.33) for the risk of developing COPD with biomass smoke exposure. Po et al. (Po et al. 2011) included data from 12 studies of female populations and reported a summary OR for chronic bronchitis of 2.52 (CI: 1.88–3.38) and for COPD of 2.40 (CI: 1.47–3.93). Applying the Bradford-Hill viewpoints (consistency, exposure-duration evidence, analogous evidence of the effect of smoking, and biological plausibility), the case for a causal association between biomass smoke and COPD is moderately strong, especially among women (Eisner et al. 2010).
Longitudinal studies of the impact of biomass smoke exposure on the development of COPD are lacking, but one study did follow women with COPD associated with biomass smoke exposure in terms of mortality risk (Ramirez-Venegas et al. 2006). Survival analysis over a 7-year follow-up period showed that women with COPD associated with biomass smoke exposure had mortality rates similar to those of men with COPD due to tobacco smoking.
Intervention studies to prevent COPD from biomass smoke exposure have been limited. A retrospective Chinese study found significant reductions in COPD incidence in homes where coal was used in improved stoves with chimneys, the effect increasing with time since adoption (Chapman et al. 2005). Two recently published studies of the efficacy of reducing wood smoke exposure with the use of an improved chimney stove were limited by short follow-up time (18 months) (Smith-Sivertsen et al. 2009; Romieu et al. 2009). Thus, although studies suggest lower biomass smoke exposure may be associated with lower COPD risk, several key questions remain, including can the development or progression of COPD be prevented by reducing biomass smoke exposure in these settings and what is the exposure-response relationship between biomass smoke and the rate of decline in lung function? Prospective cohort studies that have adequate statistical power, follow participants for sufficient duration to accurately measure rate of decline in lung function, and actual exposure measures are needed to answer these questions. Ideally, intervention studies with clean stoves will be conducted.
14.6 Lung Cancer
The emissions generated of combustion of the main solid fuels used for cooking and space heating, biomass and coal, may be associated with differential cancer risk because of differences in chemical composition. The International Agency for Research on Cancer (IARC) has concluded household use of coal is a Group 1 carcinogen, while biomass is classified as a Group 2(a) or probable carcinogen, due to more limited epidemiological evidence (International Agency for Research on Cancer 2010).
Two recent systematic reviews and meta-analyses of household use of coal and lung cancer risk have been conducted, including the one used as the basis for the 2010 Global Burden of Disease comparative risk assessment (Hosgood et al. 2011) and an additional effort by Kurmi et al. (2012). The Hosgood et al. review identified 25 case-control studies investigating household coal use with seven provided cooking-specific estimates. Exposure was assessed by fuel type, and lung cancer confirmed by pathology for most cases, otherwise by chest X-ray. Only five studies were conducted in countries other than mainland China and Taiwan. Household coal use for cooking and heating was associated with a pooled OR for lung cancer of 2.15 (CI: 1.61–2.89). The second review by Kurmi et al. pooled a total of 22 studies to generate an OR of 1.82 (CI: 1.60–2.06). In both reviews, the risk for women was somewhat greater than the risk for men.
Since the great majority of the 2.8 billion solid fuel users globally is exposed to biomass rather than coal smoke, the issue of the carcinogenic risk associated with the former is an important one. A systematic review for the 2010 Global Burden of Disease comparative risk assessment (Smith et al. 2014) identified 14 eligible studies of cooking and/or heating with biomass. Most of the studies conducted in Asia, although there were studies from Europe and North America as well. Biomass fuel was defined as including wood, straw, grass, crop waste, animal dung, and charcoal; only household use was considered, whether for cooking or heating. Exposure was determined by fuel type and no study directly measured exposure. One European study had exposure-response data available (Lissowska et al. 2005). Most cases of lung cancer were confirmed by pathology. The pooled OR for all 14 studies was 1.18 (CI: 1.03–1.35), but the most reliable estimate OR of 1.22 (CI: 1.08–1.37) from well-adjusted studies with clean fuel comparisons. The review by Kurmi et al. pooled seven studies and only used adjusted estimates to generate an OR that was somewhat higher, 1.50 (CI: 1.17–1.94). (Kurmi et al. 2012). In both the 2010 Global Burden of Disease and Kurmi et al. meta-analyses, women had somewhat higher risk than men. Applying the Bradford-Hill viewpoints (including consistency, exposure-response, biological plausibility), there does appear to be a moderately strong case for a causal association.
14.7 Cataracts
Cataract or severe lens opacification is one of the leading causes of blindness in the developing world. The 2010 Global Burden of Disease project (Murray et al. 2012) estimated that cataracts accounted for 0.2 % of the total disease burden, the majority of which is seen in the developing regions of sub-Saharan Africa and Southeast Asia alone where cooking with solid fuels is most common. The toxicological evidence from animal studies and epidemiological studies of other types of smoke (e.g., active smoking and secondhand smoke) suggest biological plausibility for an association between exposure to biomass smoke and risk of cataract. Condensates of both tobacco and biomass fuel smoke enhance the formation of superoxide radicals, which decrease antioxidants and cause lens discoloration and cataract. A component of biomass smoke is naphthalene, which has been shown to cause cataract in laboratory animal studies (van Heyningen and Pirie 1976).
The systematic review and meta-analysis for the 2010 Global Burden of Disease comparative risk assessment identified seven eligible studies, most of which had case-control designs, and all were from Southeast Asia (Smith et al. 2014). The pooled OR was 2.46 (CI: 1.74–3.50) and sensitivity analysis revealed no major confounding due to smoking or UV exposure. The results of the meta-analysis, the known risks from smoking, the consistency of results across studies, the toxicological data (especially regarding naphthalene), and some exposure-response evidence (Pokhrel et al. 2013) support causal inference.
14.8 Cardiovascular Disease
In contrast to the other health outcomes discussed above, at the time of writing this chapter, there were no epidemiological studies of the relationship between exposure to biomass smoke and cardiovascular disease. That said, a remarkably consistent, nonlinear relationship between estimated inhaled dose of combustion-sourced particles measured as PM2.5 (particulate matter with aerodynamic diameter ≤2.5 μm) and cardiovascular disease mortality was first demonstrated by Pope et al. (Pope et al. 2009). This dose-response relationship was remarkable for a non-cancer outcome in that it covered at least three orders of magnitude of dose from lowest to highest (exposure to ambient air pollution, exposure to secondhand tobacco smoke exposure, and active cigarette smoking). It then struck Peel and Smith that exposures to PM2.5 from solid fuel cooking lay in the range between those from secondhand smoke and active smoking (Smith and Peel 2010) and, given that tobacco is a kind of biomass, they postulated that the relative risk for CVD from biomass fuel smoke exposure would be in the order of 1.3–1.6 (Fig. 14.2).

Adjusted relative risks (95 % confidence intervals) of cardiovascular and cardiopulmonary mortality and estimated dose of PM2.5 across studies of outdoor air pollution, ETS, and active cigarette smoking (Adapted with permission from (Pope et al. 2009), their Fig. 2). Data on active smoking are from Pope et al. (Pope et al. 2009); on ETS are from the 2006 Surgeon General’s Report (U.S. Department of Health and Human Services 2006) and INTERHEART study (Teo et al. 2006); on air pollution are from the Women’s Health Initiative cohort (Miller et al. 2007), the American Cancer Society cohort (Pope et al. 1995, 2002, 2004), and the Harvard Six Cities cohort (Dockery et al. 1993; Laden et al. 2006). Exposure was measured as daily inhaled dose of PM2.5 (plotted on a log scale), calculated assuming 18 m3/day breathing rate. Active cigarette smoking was quantified as ≤3, 4–7, 8–12, 13–17, 18–22, and ≥23 cigarettes/day (relative to never-smokers). Also shown is the equivalent dose for the World Health Organization (WHO) (2006) Air Quality Guidelines (AQG) for PM2.5 (10 μg/m3 annual average) (Smith and Peel 2010)
Because the Global Burden of Disease project is designed to provide useful information for public health policy decisions regarding interventions to reduce important risks, the 2010 comparative risk assessment for household air pollution included identification of attributable risk for cardiovascular disease, the number one cause of death and disability on a global scale. If there were no available epidemiological studies that directly assessed the association between biomass smoke exposure and cardiovascular disease risk, then how could any risk be attributed to this exposure? An effort was made by an expert group to interpolate the risk due to biomass smoke by generating what has been termed an “integrated exposure-response curve.” The curve derived for risk of ischemic heart disease in relation to combustion-sourced fine particles is similar to that suggested by Pope et al 2011 (Pope et al. 2009), i.e., supralinear in shape from low exposures through the household air pollution exposure range, where it reaches a relative risk of 1.5 for high biomass fuel smoke exposure and a maximum of 2.5 for high active smoking exposure (Smith et al. 2014; Burnett et al. 2014). The integrated exposure-response curve for stroke is similar, but appears to flatten off at levels well within the household air pollution range at a maximum relative risk of just over 2.0.
Subsequent to the preparation of the 2010 Global Burden of Disease comparative risk assessment, the results of a cross-sectional Chinese study involving over 14,000 men and women aged 18 and over were reported (Lee et al. 2012). Solid fuel use (biomass and coal) for heating and/or cooking was assessed by questionnaire, and categorized according to ever use, duration, total amount and lifetime use. Outcomes, including ischemic heart disease, stroke and diabetes mellitus, were assessed by self-report of physician-diagnosed conditions, while blood pressure was measured during the study. The results showed elevated adjusted odds ratios for ischemic heart disease forever vs. never use of solid fuels, and significant trends across duration of use for stroke, hypertension and diabetes. The OR for ischemic heart disease 2.6 is somewhat higher than predicted from the integrated exposure–response curve; the OR for stroke, 1.6, was in the range expected from the curve although it was not statistically significant. Sex-stratified analysis found stronger effects for women, consistent with their higher exposure, and among non-smokers.
Although there is little epidemiological literature on the effect of biomass smoke exposure on cardiovascular disease risk, there are studies that show effects on blood pressure (McCracken et al. 2007; Baumgartner et al. 2011) and the ST-segment of the electrocardiogram (ECG) (McCracken et al. 2011). For blood pressure, there are five studies, four observational and one intervention (the latter with both RCT and before and after components). All have found that increased exposure was associated with higher systolic and/or diastolic blood pressure, with most findings being statistically significant. In the intervention trial (RESPIRE), McCracken et al. found the chimney stove intervention group to have statistically significant lower systolic (−3.7 mmHg) and diastolic (−3.0 mmHg) blood pressure in an intention-to-treat analysis, and similar sized effects when open-fire control subjects received the chimney stove at the end of follow-up (McCracken et al. 2007). In the same RESPIRE study subjects significant effects of the chimney stove intervention on subjects’ ECGs were demonstrated. During the trial, the stove intervention was associated with a significant protective effect (OR 0.26) for ST-segment depression and a similar effect with the before-and-after comparison (McCracken et al. 2011).
The population attributable risk for ischemic heart disease associated with biomass smoke exposure estimated by the integrated exposure-response curve method was 18 % compared to 53 % for hypertension, 29 % for hypercholesterolemia, and 31 % for tobacco smoke (both active smoking and secondhand exposure) (Lim SS et al. 1990). Despite the dearth of epidemiological studies, the overall evidence, including from the related combustion-sourced particles of smoking (active and second-hand) and outdoor air pollution, together with the observed blood pressure and electrocardiographic effects, suggests that exposure to biomass smoke can increase cardiovascular disease risk.
14.9 Other Diseases (Tuberculosis, Adult Pneumonia, Asthma)
Three other diseases for which the weight of evidence was judged not strong enough to attribute risk of disability-adjusted life years to household air pollution in the 2010 Global Burden of Disease comparative risk assessment are tuberculosis, adult pneumonia, and asthma. Nevertheless, there is some evidence and biological plausibility for an association between exposure to biomass smoke and increased risk for each of these diseases.
14.9.1 Tuberculosis
Tuberculosis (TB) was responsible for 1.4 million deaths in 2011, and over 80 % of the global burden of TB lies in the Western Pacific, South-East Asia and Africa; China and India together have 40 % of the world’s cases (Organization and Report 2013). The close association of tuberculosis with poverty, and use of solid fuel for cooking and heating in the home, makes the impact of exposure to household air pollution on risk of TB is a major concern. Because active tobacco smoking has been associated with increased risk for TB, it is again biologically plausible that exposure to biomass fuel smoke would also increase risk. Carbon particle–laden alveolar macrophages, for example, have been shown to be less effective in phagocytosis of microorganisms than those from subjects not exposed to smoke (Zhou and Kobzik 2007; Fick et al. 1984; Migliaccio et al. 2013).
Several reviews have been done over the past decade with the most recent, a systematic review and meta-analysis published in 2013 (Lin et al. 2007; Slama et al. 2010; Sumpter and Chandramohan 2013). In the 2013 review, 10 case-control and three cross-sectional studies were included. The outcome was sputum positive TB in all of the case-control studies, and two of the cross-sectional studies. None of the studies directly measured exposure to household air pollution so exposure assessment was only by survey of fuel type. Adjustment for smoking and crowding was done in most, but not all studies. Considerable study heterogeneity was found and study design issues were deemed problematic (e.g., hospital-based controls and over-representation of men). The pooled OR for the 10 case-control studies was 1.3. The six studies of women only had a pooled OR of 1.7.
A study by Pokhrel et al. also examined the risk of TB associated with the use of kerosene as well as solid biomass fuel (Pokhrel et al. 2010). Kerosene use was shown to have a much stronger effect on TB risk, for cooking with kerosene, the OR was 3.36 (CI: 1.01–11.22) and for lighting the OR was 9.43 (CI: 1.45–61.32). For cooking with a biomass fuel stove, the OR was a non-significant 1.21.
As noted above, the most up-to-date review and meta-analysis of the solid fuel-TB risk association reported a significantly increased pooled OR. However, both exposure-response evidence and intervention studies are lacking. Nevertheless, together with the well-established evidence that smoking increases risk of TB, findings from studies of animals exposed to solid fuel smoke (Zhou and Kobzik 2007; Fick et al. 1984; Migliaccio et al. 2013), and the plausible mechanism through impaired immunity from solid fuel exposure (Dutta et al. 2012), there is now a moderately strong case for a causal association between exposure to household air pollution and TB risk. Given the high prevalence of both exposure to household air pollution and TB across the developing world (and in the same geographic regions), reduction in household air pollution could make an important contribution to control of TB. Further research is needed to confirm that the association is causal rather than due to confounding by poverty-related factors, to better quantify exposure-response, and to assess potential interventions to reduce exposure.
14.9.2 Adult Acute Lower Respiratory Infection (Pneumonia)
In the 2010 Global Burden of Disease report, acute lower respiratory infections caused 2.8 million deaths annually (Lozano et al. 2012). Slightly over half of these deaths occur among adults (15 years and above), and most in those aged 60 years and over. While the majority of the adult deaths due to ALRI occur in developed countries, a substantial proportion of adult deaths in developing countries is due to ALRI/pneumonia. Given the strong evidence that exposure to biomass smoke causes ALRI in children (most probably through reducing immune defense mechanisms), as well as the established association between tobacco smoking and ALRI in adults, a biomass smoke-ALRI in adults is plausible.
A systematic review of adult ALRI was carried out for the 2010 Global Burden of Disease comparative risk assessment (Smith et al. 2014). From the many papers reviewed, only three were selected to have adequate data to assess the potential association of exposure to household air pollution and ALRI, and there is considerable heterogeneity among the three (Ezzati and Kammen 2001; Levesqu et al. 2001; Shen et al. 2009). The study by Ezzati and Kammen is a small cohort study in rural Kenya where various forms of biomass are used (wood, charcoal); home visits were used for assessment of community-acquired pneumonia (Ezzati and Kammen 2001). The data analysis also demonstrated a significant exposure-response relationship. The study by Levesque et al. is from Quebec, where biomass is used for household heating rather than cooking and exposure is much lower; the ALRI outcomes were self-reported and likely subject to some misclassification (Levesqu et al. 2001). The study by Shen et al. used a case–control design to assess risks for pneumonia deaths in a coal-using area of China (Shen et al. 2009). All three studies reported significant ORs for exposed groups in the range of 2.0–3.0. Because of differences in outcome definitions and assessment, pooling was not done.
Although the epidemiological data are limited, the exposure-response relationship from the study by Ezzati and Kammen (2001), strong evidence of a biomass smoke effect in children, and the known effects of other sources of combustion-sourced particle exposure (e.g., smoking and ambient air pollution), together suggest that exposure to solid fuel smoke increases the risk of adult ALRI. Further research is required to confirm and quantify this risk.
14.9.3 Asthma
Given the airway irritating effects of biomass smoke, it is reasonable to suspect that exposure might increase risk for asthma, especially because exposure to secondhand tobacco smoke has been associated with the development of asthma in children (Vork et al. 2007). On the other hand, there is a rural-urban gradient for asthma. The disease is generally much more prevalent in urban areas than in the largely rural areas where exposure to biomass smoke is more common (Addo-Yobo et al. 2007). The protective effect of living on a farm, especially with livestock, has been well documented (Ege et al. 2011). Because the evidence for an effect of biomass smoke on COPD is strong, and both asthma and COPD involve airway inflammation, the relationship between exposure to biomass smoke and risk of asthma remains a topic of considerable research interest.
A systematic review and meta-analysis of the association between exposure to biomass smoke and asthma in children and women was published in 2011 (Po et al. 2011). Nine studies were selected for the meta-analysis, four involving children and five involving women. The pooled OR for the four studies on asthma in children exposed to biomass smoke was 0.50 (CI: 0.12–1.98) (Fagbule and Ekanem 1994; Noorhassim et al. 1995; Behera et al. 2001; Melsom et al. 2001). For the five studies of women, the pooled OR was 1.34 (CI: 0.93–1.93) (Qureshi 1994; Behera et al. 2001; Golshan and Faghihi 2002; Uzun et al. 2003; Mishra 2003).
Since the Po et al. review was published, the results of several new studies have been reported. A survey of 508 adults in southeastern Kentucky found a significant association with asthma when wood and coal were burned for cooking (Barry et al. 2010). A much larger population survey from India found that adult women living in households using biomass and solid fuels had a significantly higher risk of asthma than those living in households using cleaner fuels, even after controlling for the effects of a number of potentially confounding factors (Agrawal 2012).
The most robust evidence supporting an increased risk of asthma from cooking with solid fuels was reported by the International Study of Asthma and Allergy in Children (ISAAC) which surveyed almost 513,000 children from 1999–2004 (Wong et al. 2013). The sole use of an open fire for cooking (assessed by questionnaire) was associated with an increased risk of wheeze in the past year in both young children (ages 6–7 years), OR 2.17 (CI: 1.64–2.87), and in older children (ages 13–14 years), OR 1.35 (CI: 1.11–1.64). The ORs for wheeze in the past year and the use of open fire in combination with other fuels for cooking were slightly lower, but still significant for both age groups.
Not all recent studies have reported positive associations between exposure to biomass smoke and asthma outcomes. For example, a recent study of 299 children from rural villages in Nigeria, reported smoke exposure was not associated with an increased risk of asthma symptoms or airway obstruction (Thacher et al. 2013). Because the published evidence is mixed, further research is needed to better understand the nature of the relationship between exposure to solid fuel smoke and asthma in both children and adults and for both new onset and exacerbations of disease. Studies that actually measure exposure and which are thus able to develop an exposure-response relationship would be particularly helpful.
14.10 Research Gaps
While one RCT of the efficacy of a chimney stove compared to an open fire for the prevention of early childhood pneumonia has been published (Smith et al. 2011) and related studies have suggested benefit regarding low birth weight, cognitive development, and respiratory symptoms in adult women, more studies of stove interventions are needed. In particular, the exposure-response data from the RESPIRE trial provide evidence that stoves which are cleaner than the chimney stove studied would provide greater reduction in childhood pneumonia. Several other ongoing RCTs of cleaner stove interventions in Nepal and Africa should contribute data to fill the gap in our knowledge about the added benefit of cleaner burning stoves beyond those with chimneys.
Another gap is the lack of a well-designed longitudinal study of the impact of improved stoves on the development of COPD in adults exposed to biomass smoke form cooking and heating. One published study from Mexico conducted in the context of a RCT designed to prevent childhood pneumonia found a protective effect of a chimney stove on rate of decline of lung function in women who actually used the stove (Romieu et al. 2009), but this study suffers from the limitation of too short of a follow-up period (1 year). Another paper from RESPIRE reports evidence that reduced exposure from use of a chimney stove is associated with decreased expression of metalloproteinase genes (Guarnieri et al. 2014).
Perhaps the greatest research gap involves the lack of epidemiological evidence to support the concept that biomass smoke exposure leads to increased risk of cardiovascular disease consistent with other combustion-sourced particle exposures, outdoor PM2.5, secondhand tobacco smoke, and active smoking.
More research is needed with regard to the associations between biomass smoke exposure and adult pneumonia, asthma, and tuberculosis, either because of paucity of data (adult pneumonia) or conflicting results. Another unresolved issue is the toxicity of kerosene as an alternative fuel, especially given the recently published evidence that it substantially increases the risk of tuberculosis (Pokhrel et al. 2010)
Because adoption of new stoves can be a difficult transition for households in the developing world due to both financial and cultural factors, more research is needed to improve our understanding of these potential barriers to the effectiveness of intervention programs.
Toxicological studies (in vitro, animal, and controlled human exposure) are needed to improve our mechanistic understanding of the pathways by which biomass smoke causes or contributes to disease pathogenesis. Such studies can also assist in the development of biomarkers of both exposure and effects (Rylance et al. 2013).
14.11 Opportunities for Intervention
For many years, the major obstacle to implementing programs to reduce biomass smoke exposure from domestic cooking and heating with inefficient, poorly ventilated stoves was lack of data proving benefit. Now that at least one RCT has proved efficacy in reduction of early childhood pneumonia, comparable to that of vaccination, with results from several other trials on the way, the major issues are cost and effectiveness of stoves that can substantially reduce biomass emissions. Improved stoves still cost more than many households in the developing world can afford, maintenance can be difficult, and many households may not be willing to adopt new stoves that require changes to traditional cooking styles.
An exciting program that was started with the help of Hillary Clinton when she was US Secretary of State is the Global Alliance for Clean Cookstoves (GACC), under the auspices of the United Nations Foundation. The GACC is a public-private partnership that “seeks to save lives, improve livelihoods, empower women, and protect the environment by creating a thriving global market for clean and efficient household cooking solutions.”(Global Alliance for Clean Cookstoves 2014) Its mission is to mobilize high-level national and donor commitments toward the goal of universal adoption of clean cookstoves and fuels. The primary goal of the GACC is to foster the adoption of clean cookstoves and fuels in 100 million households by 2020. Multiple demonstration and research projects have been funded by the organization since it was established in 2010. In 2012, the following countries were prioritized for immediate GACC engagement: Bangladesh, China, Ghana, Kenya, Nigeria, and Uganda.
Although the GACC represents a major breakthrough for efforts to improve the health of the 45 % of the world’s population that still cooks with solid fuel, even the most efficient stoves that burn biomass emit more PM2.5 than the gas and electric stoves that are used by developed world households. This has led some experts to suggest that electrification of developing countries and the use of relatively inexpensive induction cookers may be the most effective way to reduce exposure to household air pollution.
A final policy note is that black carbon generated from biomass combustion is an important short-lived climate-forcing agent (Jacobson 2001). Interventions to improve the efficiency of combustion of biomass fuels or better, that eliminate combustion of biomass fuels altogether, would provide a major climate change mitigation co-benefit in addition to the public health benefits described above.
References
Abusalah A, Gavana M, Haidich AB et al (2011) Low birth weight and prenatal exposure to indoor pollution from tobacco smoke and wood fuel smoke: a matched case–control study in Gaza Strip. Matern Child Health J 16:1718–1727
Addo-Yobo E, Woodcock A et al (2007) Exercise-induced bronchospasm and atopy in Ghana: two surveys ten years apart. PLoS Med 4:355–360
Agrawal S (2012) Effect of indoor air pollution from biomass and solid fuel combustion on prevalence of self-reported asthma among adult men and women in India: findings from a nationwide large-scale cross-sectional survey. J Asthma 49:355–365
Akhtar T, Ullah Z, Khan MH et al (2007) Chronic bronchitis in women using solid biomass fuel in rural Peshawar, Pakistan. Chest 132:1472–1475
Albalak R, Frisancho AR, Keeler GJ (1999) Domestic biomass fuel combustion and chronic bronchitis in two rural Bolivian villages. Thorax 54:1004–1008
Armstrong JR, Campbell H (2009) Indoor air pollution exposure and lower respiratory infections in young Gambian children. Int J Epidemiol 20:424–429
Balakrishnan K, Ghosh S, Ganguli B et al (2013) State and national household concentrations of PM2.5 from solid cookfuel use: results from measurements and modeling in India for estimation of the global burden of disease. Environ Health 12:77
Balmes JR (2010) When smoke gets in your lungs. Proc Am Thorac Soc 7:98–101
Barregard L, Sällsten G, Andersson L et al (2008) Experimental exposure to wood smoke: effects on airway inflammation and oxidative stress. Occup Environ Med 65:319–324
Barry AC, Mannino DM, Hopenhayn C, Bush H (2010) Exposure to indoor biomass fuel pollutants and asthma prevalence in Southeastern Kentucky: results from the Burden of Lung Disease (BOLD) study. J Asthma 47:735–741
Baumgartner J, Schauer JJ, Ezzati M et al (2011) Indoor air pollution and blood pressure in adult women living in rural China. Environ Health Perspect 119:1390–1395
Behera D, Chakrabarti T et al (2001) Effect of exposure to domestic cooking fuels on bronchial asthma. Indian J Chest Dis Allied Sci 43:27–31
Boy E, Bruce N, Delgado H (2002) Birth weight and exposure to kitchen wood smoke during pregnancy in rural Guatemala. Environ Health Perspect 10:109–114
Bruce N, Perez-Padilla R, Albalak R (2000) Indoor air pollution in developing countries: a major environmental and public health challenge. Bull World Health Organ 78:1078–1092
Burnett RT, Pope CA 3rd, Ezzati M et al (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect 122:397–403
Caballero A, Torres-Duque CA, Jaramillo C et al (2008) Prevalence of COPD in five Colombian cities situated at low, medium, and high altitude (PREPOCOL study). Chest 133:343–349
Chapman RS, He X, Blair AE et al (2005) Improvement in household stoves and risk of chronic obstructive pulmonary disease in Xuanwei, China: retrospective cohort study. BMJ 331:1050–1055
Dennis RJ, Maldonado D, Norman S et al (1996) Woodsmoke exposure and risk for obstructive airways disease among women. Chest 109:115–119
Dherani M, Pope D, Mascarenhas M et al (2008) Indoor air pollution from unprocessed solid fuel use and pneumonia risk in children aged under five years: a systematic review and meta-analysis. Bull World Health Organ 86:390–398C
Diette GB, Accinelli RA, Balmes JR et al (2012) Obstructive lung disease and exposure to burning biomass fuel in the indoor environment. Glob Heart 7:265–270
Dockery DW, Pope CA III, Xu X, Spengler JD, Ware JH, Fay ME et al (1993) An association between air pollution and mortality in six U.S. cities. N Engl J Med 329:1753–1759
Dossing M, Khan J, al-Rabiah F (1994) Risk factors for chronic obstructive lung disease in Saudi Arabia. Respir Med 88:519–522
Dutt D, Srinivasa DK, Rotti SB et al (1996) Effect of indoor air pollution on the respiratory system of women using different fuels for cooking in an urban slum of Pondicherry. Natl Med J India 9:113–117
Dutta A, Bhattacharya P, Lahiri T, Ray MR (2012) Immune cells and cardiovascular health in premenopausal women of rural India chronically exposed to biomass smoke during daily household cooking. Sci Total Environ 438:293–298
Ege M, Mayer M et al (2011) Exposure to environmental microorganisms and childhood asthma. N Engl J Med 364:701–709
Eisner MD, Anthonisen N, Coultas D et al (2010) An official American Thoracic Society public policy statement: Novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 82:693–718
Ekici A, Ekici M, Kurtipek E et al (2005) Obstructive airway diseases in women exposed to biomass smoke. Environ Res 99:93–98
Ellegard A (1996) Cooking fuel smoke and respiratory symptoms among women in low-income areas in Maputo. Environ Health Perspect 104:980–985
Ezzati M, Kammen DM (2001) Quantifying the effects of exposure to indoor air pollution from biomass combustion on acute respiratory infections in developing countries. Environ Health Perspect 109:481–488
Fagbule D, Ekanem E (1994) Some environmental risk factors for childhood asthma: a case-control study. Ann Trop Paediatr 14:15–19
Fick RB Jr, Paul ES, Merrill WW et al (1984) Alterations in the antibacterial properties of rabbit pulmonary macrophages exposed to wood smoke. Am Rev Respir Dis 129:76–81
Forchhammer L, Møller P, Riddervold IS et al (2012) Controlled human wood smoke exposure: oxidative stress, inflammation and microvascular function. Part Fibre Toxicol 9:7
Global Alliance for Clean Cookstoves (2014) Washington, DC http://www.cleancookstoves.org/the-alliance/. Accessed 26 Jan 2014
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for diagnosis, management, and prevention of COPD. http://www.goldcopd.org/Guidelines/guidelines-resources.html Accessed 20 Jan 2014
Golshan M, Faghihi M (2002) Indoor women jobs and pulmonary risks in rural areas of Isfahan, Iran. Respir Med 96:382–388
Guarnieri MJ, Diaz JV, Basu C et al (2014) Effects of woodsmoke exposure on airway inflammation in rural Guatemalan women. PLoS One 9:e88455
Hosgood HD 3rd, Wei H, Sapkota A et al (2011) Household coal use and lung cancer: systematic review and meta-analysis of case control studies, with emphasis on geographic variation. Int J Epidemiol 40:719–728
Hu G, Zhou Y, Tian J et al (2010) Risk of COPD from exposure to biomass smoke: a metaanalysis. Chest 138:20–31
International Agency for Research on Cancer (2010) Household use of solid fuels and high-temperature frying: evaluation of carcinogenic risks to humans. International Agency for Research on Cancer, Lyon
Jacobson MZ (2001) Strong radiative heating due to the mixing state of black carbon in atmospheric aerosols. Nature 409:695–697
Kiraz K, Kart L, Demir R et al (2003) Chronic pulmonary disease in rural women exposed to biomass fumes. Clin Invest Med 26:243–248
Kurmi OP, Semple S, Simkhada P et al (2010) COPD and chronic bronchitis risk of indoor air pollution from solid fuel: a systematic review and meta-analysis. Thorax 65:221–228
Kurmi OP, Arya PH, Lam KB et al (2012) Lung cancer risk of solid fuel smoke exposure: a systematic review and meta-analysis. Eur Respir J 40:1228–1237
Laden F, Schwartz J, Speizer FE, Dockery DW (2006) Reduction in fine particulate air pollution and mortality: extended follow-up of the Harvard Six Cities Study. Am J Respir Crit Care Med 173:667–672
Lee MS, Hang JQ, Zhang FY et al (2012) In-home solid fuel use and cardiovascular disease: a cross-sectional analysis of the Shanghai Putuo study. Environ Heal 11:18
Levesqu B, Allaire S, Gauvin D et al (2001) Wood-burning appliances and indoor air quality. Sci Total Environ 281:47–62
Lim SS, Vos T, Flaxman AD et al (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2224–2260
Lin H-H, Ezzati M, Murray M (2007) Tobacco smoke, indoor air pollution and tuberculosis: a systematic review and meta-analysis. PLoS Med 4(1):e20
Lissowska J, Bardin-Mikolajczak A, Fletcher T et al (2005) Lung cancer and indoor pollution from heating and cooking with solid fuels: the IARC International Multicenter Case-control Study in Eastern/Central Europe and the United Kingdom. Am J Epidemiol 162:326–333
Lozano R, Naghavi M, Foreman K et al (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2095–2128
Mavalankar DV, Gray RH, Trivedi CR (1992) Risk factors for preterm and term low birth weight in Ahmedabad, India. Int J Epidemiol 21:263–272
McCracken JP, Smith KR, Mittleman M et al (2007) Chimney stove intervention to reduce long-term woodsmoke exposure lowers blood pressure among Guatemalan women. Environ Health Perspect 115:996–1001
McCracken J, Smith K, Stone P et al (2011) Intervention to lower household woodsmoke exposure in Guatemala reduces ST-segment depression on electrocardiograms. Environ Health Perspect 119:1562–1568
Melsom T, Brinch L et al (2001) Asthma and indoor environment in Nepal. Thorax 56:477–481
Menezes AM, Victora CG, Rigatto M (1994) Prevalence and risk factors for chronic bronchitis in Pelotas, RS, Brazil: a population-based study. Thorax 49:1217–1221
Migliaccio CT, Mauderly JL (2010) Biomass smoke exposures: toxicology and animal study design. Inhal Toxicol 22:104–107
Migliaccio CT, Kobos E, King QO et al (2013) Adverse effects of wood smoke PM(2.5) exposure on macrophage functions. Inhal Toxicol 25:67–76
Miller KA, Siscovick DS, Sheppard L, Shepherd K, Sullivan JH, Anderson GL et al (2007) Longterm exposure to air pollution and incidence of cardiovascular events in women. N Engl J Med 356:447–458
Mishra V (2003) Effect of indoor air pollution from biomass combustion on prevalence of asthma in the elderly. Environ Health Perspect 111:71–78
Mishra V, Dai X, Smith KR et al (2004) Maternal exposure to biomass smoke and reduced birth weight in Zimbabwe. Ann Epidemiol 14:740–747
Murray CJ, Vos T, Lozano R et al (2012) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380(9859):2197–2223
Nair H, Simões EA, Rudan I et al (2013) Global and regional burden of hospital admissions for severe acute lower respiratory infections in young children in 2010: a systematic analysis. Lancet 381(9875):1380–1390
Noorhassim I, Rampal K et al (1995) The relationship between prevalence of asthma and environmental factors in rural households. Med J Malaysia 50:263–267
Orozco-Levi M, Garcia-Aymerich J, Villar J et al (2006) Wood smoke exposure and risk of chronic obstructive pulmonary disease. Eur Respir J 27:542–546
Perez-Padilla R, Regalado J, Vedal S et al (2006) Exposure to biomass smoke and chronic airway disease in Mexican women. A case-control study. Am J Respir Crit Care Med 154:701–706
Po J, FitzGerald J, Carlsten C (2011) Respiratory disease associated with solid biomass fuel exposure in rural women and children: systematic review and meta-analysis. Thorax 66:232–239
Pokhrel AK, Bates MN et al (2010) Tuberculosis and indoor biomass and kerosene use in Nepal: a case–control study. Environ Health Perspect 118:558–564
Pokhrel AK, Bates MN, Shrestha SP et al (2013) Biomass stoves and lens opacity and cataract in Nepalese women. Optom Vis Sci 90:257–268
Pope CA III, Thun MJ, Namboodiri MM, Dockery DW, Evans JS, Speizer FE et al (1995) Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am J Respir Crit Care Med 151:669–674
Pope CA III, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K et al (2002) Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 287:1132–1141
Pope CA III, Burnett RT, Thurston GD, Thun MJ, Calle EE, Krewski D et al (2004) Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation 109:71–77
Pope CA 3rd, Burnett RT, Krewski D et al (2009) Cardiovascular mortality and exposure to airborne fine particulate matter and cigarette smoke: shape of the exposure-response relationship. Circulation 120:941–948
Pope DP, Mishra V, Thompson L et al (2010) Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries. Epidemiol Rev 32:70–81
Qureshi KA (1994) Domestic smoke pollution and prevalence of chronic bronchitis/asthma in a rural area of Kashmir. Indian J Chest Dis Allied Sci 36:61–72
Ramirez-Venegas A, Sansores RH, Pérez-Padilla R et al (2006) Survival of patients with chronic obstructive pulmonary disease due to biomass smoke and tobacco. Am J Respir Crit Care Med 173:393–397
Regalado J, Pérez-Padilla R, Sansores R et al (2006) The effect of biomass burning on respiratory symptoms and lung function in rural Mexican women. Am J Respir Crit Care Med 174:901–905
Riddervold IS, Bønløkke JH, Olin AC et al (2012) Effects of wood smoke particles from wood-burning stoves on the respiratory health of atopic humans. Part Fibre Toxicol 9:12
Romieu I, Riojas-Rodríguez H, Marrón-Mares AT et al (2009) Improved biomass stove intervention in rural Mexico: impact on the respiratory health of women. Am J Respir Crit Care Med 180:649–656
Rylance J, Gordon SB, Naeher LP et al (2013) Household air pollution: a call for studies into biomarkers of exposure and predictors of respiratory disease. Am J Physiol Lung Cell Mol Physiol 304:L571–578
Saha A, Rao NM, Kulkarni PK et al (2005) Pulmonary function and fuel use: a population survey. Respir Res 6:127
Sehlstedt M, Dove R, Boman C et al (2010) Antioxidant airway responses following experimental exposure to wood smoke in man. Part Fibre Toxicol 7:21
Sezer H, Akkurt I, Guler N et al (2006) A case–control study on the effect of exposure to different substances on the development of COPD. Ann Epidemiol 16:59–62
Shen M, Chapman RS et al (2009) Coal use, stove improvement and adult pneumonia mortality in Xuanwei, China: a retrospective cohort study. Environ Health Perspect 117:261–266
Siddiqui AR, Gold EB, Yang X et al (2008) Prenatal exposure to wood fuel smoke and low birth weight. Environ Health Perspect 116:543–549
Slama K, Chiang CY et al (2010) Indoor solid fuel combustion and tuberculosis: is there an association? Int J Tuberc Lung Dis 14:6–14
Smith KR, Peel JL (2010) Mind the gap. Environ Health Perspect 118:1643–1645
Smith KR, McCracken JP, Weber MW et al (2011) Effect of reduction in household air pollution on childhood pneumonia in Guatemala (RESPIRE): a randomised controlled trial. Lancet 378:1717–1726
Smith KR, Frumkin H, Butler CD, Chafe Z et al (2013) Energy and human health. Annu Rev Public Health 34:1–30
Smith KR, Bruce N, Balakrishnan K et al (2014) Millions dead: how do we know and what does it mean? Methods used in the comparative risk assessment of household air pollution. Annu Rev Public Health 35:185–206
Smith-Sivertsen T, Díaz E, Pope D et al (2009) Effect of reducing indoor air pollution on women’s respiratory symptoms and lung function: the RESPIRE Randomized Trial, Guatemala. Am J Epidemiol 170:211–220
Stockfelt L, Sallsten G, Olin AC et al (2012) Effects on airways of short-term exposure to two kinds of wood smoke in a chamber study of healthy humans. Inhal Toxicol 24:47–59
Stockfelt L, Sallsten G, Almerud P et al (2013) Short-term chamber exposure to low doses of two kinds of wood smoke does not induce systemic inflammation, coagulation or oxidative stress in healthy humans. Inhal Toxicol 25:417–425
Sumpter C, Chandramohan D (2013) Systematic review and meta-analysis of the associations between indoor air pollution and tuberculosis. Trop Med Int Health 18:101–108
Teo KK, Ounpuu S, Hawken S, Pandey MR, Valentin V, Hunt D et al (2006) Tobacco use and risk of myocardial infarction in 52 countries in the INTERHEART study: a case–control study. Lancet 368:647–658
Thacher JD, Emmelin A, Madaki AJ, Thacher TD (2013) Biomass fuel use and the risk of asthma in Nigerian children. Respir Med 107:1845–1851
Thompson LM, Bruce N, Eskenazi B et al (2011) Impact of reduced maternal exposures to wood smoke from an introduced chimney stove on newborn birth weight in rural Guatemala. Environ Health Perspect 119:1489–1494
Tielsch JM, Katz J, Thulasiraj RD et al (2009) Exposure to indoor biomass fuel and tobacco smoke and risk of adverse reproductive outcomes, mortality, respiratory morbidity and growth among newborn infants in south India. Int J Epidemiol 38:1351–1363
Torres-Duque C, Maldonado D, Pérez-Padilla R et al (2008) Biomass fuels and respiratory diseases: a review of the evidence. Proc Am Thorac Soc 5:577–590
Unosson J, Blomberg A, Sandström T et al (2013) Exposure to wood smoke increases arterial stiffness and decreases heart rate variability in humans. Part Fibre Toxicol 10:20
U.S. Department of Health and Human Services (2006) The health consequences of involuntary exposure to tobacco smoke: a report of the surgeon general. Centers for Disease Control and Prevention, Atlanta
Uzun K, Ozbay B et al (2003) Prevalence of chronic bronchitis-asthma symptoms in biomass fuel exposed females. Environ Health Prev Med 8:13–17
van Heyningen R, Pirie A (1976) Naphthalene cataract in pigmented and albino rabbits. Exp Eye Res 22:393–394
Vork K, Broadwin R et al (2007) Developing asthma in childhood from exposure to secondhand tobacco smoke: insights from a meta-regression. Environ Health Perspect 115:1394–1400
Warwick H, Doig A (2004) Smoke – the killer in the kitchen. ITDG Publishing, London
Wong GW, Brunekreef B, Ellwood P, ISAAC Phase Three Study Group et al (2013) Cooking fuels and prevalence of asthma: a global analysis of phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Lancet 1:386–394
World Health Organization (2006) WHO air quality guidelines: global update for 2005. World Health Organization Regional Office for Europe, Copenhagen
World Health Organization (2009) Quantifying environmental health impacts. Global estimates of burden of disease caused by environmental risks. World Health Organization, Geneva
World Health Organization (2013) Global tuberculosis report 2013. World Health Organization, Geneva
Xu F, Yin X, Shen H et al (2007) Better understanding the influence of cigarette smoking and indoor air pollution on chronic obstructive pulmonary disease: a case-control study in Mainland China. Respirology 12:891–897
Zelikoff JT, Chen LC, Cohen MD et al (2002) The toxicology of inhaled woodsmoke. J Toxicol Environ Health 5:269–282
Zhou H, Kobzik L (2007) Effect of concentrated ambient particles on macrophage phagocytosis and killing of Streptococcus pneumoniae. Am J Respir Cell Mol Biol 36:460–465
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer-Verlag London
About this chapter
Cite this chapter
Balmes, J.R. (2015). Indoor Biomass Burning and Health Consequences. In: Nadadur, S., Hollingsworth, J. (eds) Air Pollution and Health Effects. Molecular and Integrative Toxicology. Springer, London. https://doi.org/10.1007/978-1-4471-6669-6_14
Download citation
DOI: https://doi.org/10.1007/978-1-4471-6669-6_14
Publisher Name: Springer, London
Print ISBN: 978-1-4471-6668-9
Online ISBN: 978-1-4471-6669-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)