
Abstract
The need for a total knee arthroplasty (TKA) after a high tibial osteotomy (HTO) presents several difficulties. The osteotomy induces a bony deformity that can lead to unbalanced bone cuts if the resection is based on ligament balancing techniques. This potential difficulty should be considered before surgery, anticipated, and planned for with a thorough clinical and radiologic examination. Specifically, radiographs should include:
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
The need for a total knee arthroplasty (TKA) after a high tibial osteotomy (HTO) presents several difficulties. The osteotomy induces a bony deformity that can lead to unbalanced bone cuts if the resection is based on ligament balancing techniques. This potential difficulty should be considered before surgery, anticipated, and planned for with a thorough clinical and radiologic examination. Specifically, radiographs should include:
-
AP and lateral single leg stance views
-
Axial view of the patella at 30° of knee flexion
-
Stress views (varus and valgus)
-
Full leg views (weight bearing)
Analysis of the tibial shape includes assessment of the translation and angulation of the epiphysis. This is quantified by measuring the mechanical tibial angle (MTA) and the tibiofemoral mechanical angle (AFTM) in the frontal plane and the tibial slope in the sagittal plane (Fig. 27.1). The angle of the previous osteotomy is of lesser importance. The mechanical axis at the knee is critical. Preoperative planning of the procedure is important. Templating of the implant, position of the implant, anticipated mismatch of the bone and the implant, estimated cuts, induced spaces, and the joint level are all essential to make the right choice of prosthesis (type of prosthesis – constrained or not, custom prosthesis, keel offset, associated osteotomy) and intraoperative technique (ligament release, sliding osteotomy of the lateral condyle of Burdin, etc.).

Assessment of the translation and angulation of the epiphysis
In practice, there are two preoperative situations that need to be understood: undercorrection (AFTM ≤180°) or overcorrection (AFTM >182°).
Surgical Technique
Typical setup for a TKA is employed.
-
1.
Incision
The choice of surgical approach is essential because it facilitates the releases and ligament balancing.
The previous vertical incision can be used and extended, if necessary, since it is close to the midline.
A previous horizontal incision cannot be reused. The new incision is created vertically in the midline, crossing the previous scar at right angles (Fig. 27.2).
Fig. 27.2 
Case of previous horizontal incision. The new incision crosses the previous scar at right angles
The location of the incision does not influence the choice of whether a medial or lateral arthrotomy is used.
-
In cases of undercorrection (varus knee), a medial parapatellar arthrotomy is preferred.
-
In case of overcorrection (valgus knee), a lateral parapatellar arthrotomy is preferred (Fig. 27.3).
Fig. 27.3 
Lateral parapatellar arthrotomy in case of overcorrection (valgus knee)
In cases with multiple scars where there is a possibility of skin necrosis, the opinion of the plastic surgeons is sometimes needed.
-
-
2.
Removal of equipment
Previous hardware is not routinely removed. When hardware removal is required, we remove it during the TKA procedure when possible in order to avoid two interventions and hospitalizations.
Nevertheless, a two-stage surgery is preferable when there is a question about infection. Microbiology advice is required if there is a positive history of infection.
The previous scar from the osteotomy may be used independently to remove the hardware, but there is a risk of skin necrosis.
-
3.
Exposure
If there is a patella baja or significant knee stiffness (flexion ≤90°), there is a risk of avulsion of the patellar tendon whilst flexing the knee to dislocate the patella. Osteotomy of the tibial tuberosity is sometimes necessary. However, one must attempt to avoid this by initially performing an arthrolysis. When performed, the tubercle osteotomy has the advantage of allowing a proximal transfer of the tibial tubercle when the patella is low. It is necessary to osteotomize a piece of tibial tubercle long enough (≥6 cm) and deep enough (it must reach the cancellous metaphyseal bone) and perform the fixation with two screws in order to avoid a nonunion (Fig. 27.4).
Fig. 27.4 
Tibial tubercle osteotomy
The exposure is completed by the release of the condylar gutters.
A lateral retinacular release is not routinely performed. If necessary, this release is performed from within the joint to limit undermining in the prepatellar region.
In some cases, putting a 2 mm pin as an artificial constraint in the patella tendon once the patella is dislocated (Deschamps) will strengthen its attachment and avoid avulsion during flexion and anterior dislocation of the tibia.
The posterior femoral cut can be made at this time to facilitate the exposure and the dislocation of the tibia (Fig. 27.5).
Fig. 27.5 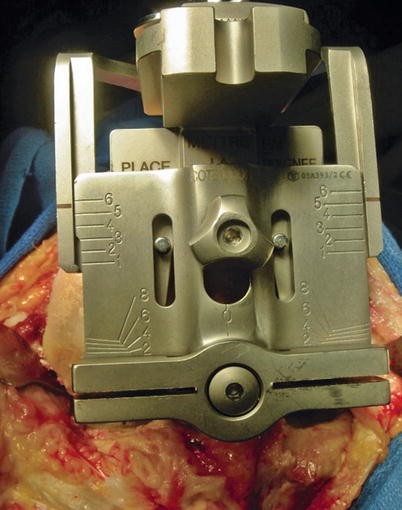
The posterior femoral cut can be made first to facilitate the exposure of the tibia
-
4.
Tibial cut
The objective is to obtain a mechanical tibial angle of 90°, cutting perpendicular to the mechanical axis of the tibia in the frontal and sagittal planes. We use intra- and extramedullary guides as a double check to determine the correct cutting angle on the tibia (the extramedullary guide gives the varus-valgus alignment). Two difficulties are then encountered: restoration of the joint line and compromise between coverage and conflict between the tibial stem and the tibial cortex.
This must be planned preoperatively when templating to ensure that there is no conflict between the tibial stem and tibial metaphysis. Similarly, one must draw the proposed cuts and evaluate their asymmetry.
The cutting height is difficult to determine. Due to the tibial shape, it is difficult to use the plateau to determine the cutting level and space height. The lateral compartment has been “reduced” by the osteotomy and now also has unusual cartilage wear. The medial compartment also has osteoarthritis but with bone loss.
-
In the case of undercorrection, the tibial cut is perpendicular to the long axis of the tibia and 6 mm is taken from the lateral tibial plateau (this is for an insert of 9 mm). Multiple drill holes in the medial tibial plateau may be necessary, to help with cement fixation (Fig. 27.6).
Fig. 27.6 
Tibial cut of 6 mm from the lateral tibial plateau in case of undercorrection
-
In the case of overcorrection, the tibial cut is perpendicular to the long axis of the tibia and 6 mm is taken from the medial tibial plateau (always for an insert of 9 mm) (Fig. 27.7).
Fig. 27.7 
Tibial cut of 6 mm from the medial tibial plateau in case of overcorrection
The translation created by the epiphyseal osteotomy may require a compromise between good tibial coverage and conflict between the keel or stem and the tibial cortex. Sometimes an offset tibial keel or a custom-made prosthesis is necessary (Fig. 27.8). Preoperative planning is therefore important so that these implants may be ordered if required (Fig. 27.9a, b).
Fig. 27.8 
Case of important tibial translation. A tibial component overhang or a conflict between the keel and the tibial cortex may occur. An offset tibial keel or a custom-made prosthesis should be discussed
Fig. 27.9 
Custom-made prosthesis with an offset tibial keel. (a) Preoperative view; (b) postoperative X-ray
We recommend using a long tibial stem (75 mm or 100 mm) in cases of opening wedge osteotomy especially when synthetic bone substitute was used.
The concept of tibial slope in total knee arthroplasty is important because increased tibial slope can lead to anterior tibial translation and anterior subluxation of the tibia when weight bearing. It is for this reason that we want a postoperative tibial slope of 0°. The problems found with asymmetric bone cuts in the coronal plane can also be found in the sagittal plane. Tibial slope should be carefully evaluated before surgery. We measure the angle between the axis of the diaphysis and the medial tibial plateau, which is less variable than using the medial tibial plateau and the anterior tibial cortex (this is affected by rotation on the radiographic films).
Soft tissue balancing precedes the distal femoral cut. Resection of osteophytes and a lateral release will help to balance the ligaments. We perform our lateral release in the following order:
-
Loosening of the IT band insertion on Gerdy’s tubercle during the lateral parapatellar approach
-
Pie crusting of the IT band (extended release)
-
Osteotomy of the lateral condyle (of Burdin) if there is contracture in flexion and extension (see previous chapters for the surgical technique) (Fig. 27.10a–c)
Fig. 27.10 
(a–c) Osteotomy of the lateral condyle providing balancing in extension and in flexion
-
Rarely, a femoral release of the popliteus and LCL in extreme cases (Fig. 27.11)
Fig. 27.11 
Subperiosteal femoral release of the popliteus tendon and LCL
Finally, in cases of severe overcorrection (malunion >100°), a corrective osteotomy is performed prior to the TKA, so that the definitive procedure can be performed under the best conditions. We try to avoid doing the corrective osteotomy and the TKA in a single surgery. We also usually do a sliding osteotomy of the lateral condyle in these cases.
The distal femoral cut is performed with a 5° valgus angle. The three components, femoral, tibial, and patella, are then cemented in place.
The closure is unremarkable.
-
-
5.
Postoperative
Weight bearing and crutches from day 1. Flexion is limited to 95° for 60 days and then without limitation. An extension splint is used for walking until the quadriceps is able to lock the knee in extension. If a proximalization of the tibial tubercle is done, the extension splint is kept for 2 months and the patient is reviewed at day 60.










Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
Demey, G., Hobbs, H. (2014). Total Knee Prosthesis After Valgus Osteotomy of the Tibia. In: Neyret, P., Demey, G. (eds) Surgery of the Knee. Springer, London. https://doi.org/10.1007/978-1-4471-5631-4_27
Download citation
DOI: https://doi.org/10.1007/978-1-4471-5631-4_27
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-5630-7
Online ISBN: 978-1-4471-5631-4
eBook Packages: MedicineMedicine (R0)