
Abstract
Continent lower urinary tract reconstruction is an invaluable tool to treat urinary incontinence, allow accessible intermittent catheterization, and protect the upper urinary tracts from high bladder pressures in children with neuropathic bladders. It has been used extensively in the past few decades around the world, and a large body of evidence has been accumulated as to its surgical outcomes and complications. The majority of these complications are manageable with a combination of medical and minimally invasive surgical interventions. This chapter will outline minimally invasive and injection techniques in the approach to complications such as stomal stenosis, acute inability to catheterize a channel, urinary incontinence, and bladder stones.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Continent urinary reconstruction
- Mitrofanoff appendicovesicostomy
- Malone appendicocecostomy
- Stomal stenosis
- Urinary incontinence
- Bladder stones
- Urinary retention
Introduction
Children with neuropathic voiding dysfunction who continue to have urinary incontinence and/or hostile bladder dynamics despite maximal medical therapy with clean intermittent catheterization and anticholinergic medication are considered for continent lower urinary tract reconstruction. The goal is to achieve a large capacity, low-pressure urinary reservoir that empties completely, is free of infection, and does not lead to renal deterioration. This can entail lengthening and tightening of the bladder neck to prevent urinary leakage from the native urethra as well as creation of a continent catheterizable channel to the abdominal wall to allow for accessible and efficient drainage. On occasion, the bladder will have to be enlarged with an enteric segment due to poor compliance and/or elevated detrusor filling pressures not responsive to medical management. In addition, many children with underlying conditions such as myelomeningocele, anorectal malformations, and tethered cord will have debilitating fecal incontinence and constipation. At the time of the major urologic reconstruction, an appendicocecostomy (antegrade continence enema, Malone ACE) can be performed to allow for more effective bowel management [1, 2]. Complications of these complex reconstructive procedures are not uncommon, however. They can range from minor difficulties such as stomal stenosis to serious life-threatening complications such as bladder perforation [3–6]. In addition, due to the mucus production from bowel tissue used in enterocystoplasty, bladder stones may form in the reservoir and lead to decreased capacity and recurrent urinary tract infections [7, 8]. This chapter will review the more common complications after these procedures and focus on minimally invasive and injection techniques to address these issues.
Stomal Stenosis
Since Mitrofanoff first described his procedure to facilitate clean intermittent catheterization via an abdominal wall stoma in 1980, the continent appendicovesicostomy has been used worldwide by reconstructive surgeons with great success [4, 5, 9–12]. Multiple series have documented its utility and the principle has been expanded to include detubularized and reconfigured intestinal segments (i.e., Yang-Monti, Casale modification), defunctionalized ureters, and even the fallopian tube [13–16]. Stomal stenosis at the cutaneous aspect of the channel is one of the more common complications of these channels (including those used for performing antegrade continence enemas). Contemporary series report a prevalence of up to 10–20 % (see Table 30.1) [4, 5, 17–19].
Most surgeons attempt to prevent stomal stenosis at the time of the creation of the channel by employing a U or V-shaped cutaneous flap to the spatulated end of the appendix. Despite these efforts as well as the continual ongoing passage of a catheter through the channel on a daily basis to gently dilate the stoma and theoretically minimize stenosis, scarring and tightness of the orifice can occur. The likely culprit is poor vascularity of the distal tip of the appendix resulting in ischemia and scarring. Sometimes hypertrophic scarring (e.g., keloids) can result in difficulty passing the catheter.
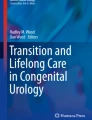
When stomal stenosis occurs the patients may report some difficulty or pain passing the catheter into the main part of the channel in mild cases but be unable to engage the catheter into the stoma at all in severe situations. This can also lead to forced attempts to place the catheter resulting in a false passage of the channel and rupture of the appendix and even loss of the conduit. In our experience, the stomal stenosis rate seems to be higher in the appendicocecostomy channel used to perform the antegrade continence enema when both channels are created concomitantly using a split appendix technique. This could be due to the fact that the ACE stoma is only accessed once a day to once every other day, as opposed to the Mitrofanoff neourethra that is accessed multiple times a day). Figure 30.1 shows two separated stomas created with this technique with the well-vascularized Mitrofanoff channel compared to the stenotic appendicocecostomy channel.

Continent catheterizable channels in the right lower quadrant with a healthy Mitrofanoff appendicovesicostomy (left) and a stenotic Malone appendicocecostomy (right)
Initial Intervention
When patients or caregivers begin to report difficulty with catheterization at the skin level, physical examination of the stoma may reveal a contraction of the orifice or sometimes a whitish circumferential scar with no visible mucosa. Simple initial interventions include placing a warm washcloth over the stoma for a few moments to soften the orifice prior to catheterizing the stoma and avoid further trauma to the tissues. Topical steroid cream such as 1 % triamcinolone may be applied 2–3 times daily (or with each catheterization) for a period of 4 weeks (or longer if needed) to soften the cicatrix [20]. We will often give a caregiver a slightly smaller catheter to keep at home in case the usual size catheter will not pass easily. For appendicocecostomies (ACE) that are not generally cannulated but once a day or every other day for bowel irrigations, the single-use catheter used for clean intermittent catheterization can subsequently be used to gently dilate the ACE stoma 4–5 times a day after emptying the bladder.
In severe cases the stomal stenosis can be managed with intradermal injection of Kenalog 40 (1 mL = 40 mg of triamcinolone) with concomitant dilation with urethral sounds. If using this technique, it is helpful to leave an indwelling catheter in place for 72 h after the injection to allow for any inflammation to subside.
Endoscopic Management
In cases where simple topical interventions are not sufficient, inspection of the channel with a pediatric cystoscope with concomitant dilation of the channel can be employed. This can be helpful in umbilical stomas where surgical revision may be somewhat technically challenging. A guidewire can be passed into the bladder under direct cystoscopic guidance (and even manipulated out the native urethra if no bladder neck reconstruction has been performed). The cystoscope is removed and sequential dilators (Amplatz Renal Dilator Set, Cook Medical) can be passed over the wire, safely dilating the orifice. Attention should be maintained to avoid passing the rigid dilator across the continence mechanism to avoid causing iatrogenic urinary incontinence. Mid-channel strictures are less common but could be a result of an old false passage or traumatic catheterization. These can be managed in a similar fashion with careful maintenance of guidewire access. In both situations, leaving a silicone Council tip catheter (placed over the guidewire) for 1–2 weeks may facilitate healing and avoid recurrence. We have found daily gentamicin bladder irrigations to be helpful in avoiding infection with temporary catheter drainage of reconstructed bladders and catheterizable channels.
Surgical Revision
There is a relative high rate of recurrent stomal stenosis and at times, formal surgical revision becomes necessary when conservative measures have failed. A variety of techniques exist to revise a stoma at the skin surface, but in general, raising a U-shaped flap of uninvolved skin and re-spatulating the appendix through the cicatrix down to healthier tissue for anastomosis to the flap is successful. In more severe cases, the appendix can be circumferentially mobilized even down to the fascia and then the diseased portion excised. Generous double U-shaped flaps can be employed to reach the appendix for anastomosis.
Treatment Failure
In rare cases where dilation and then surgical revision have failed to prevent recurrence of stomal stenosis and major surgical revision or replacement of the channel is not ideal or desired by the patient, an indwelling tube can be employed to at least maintain the access. This would not be ideal for bladder channels but we have used them for ACE stomas in difficult cases [21]. Options include a MIC-KEY gastrostomy button (Kimberly Clark Worldwide, Inc.) or a Chait Trapdoor cecostomy catheter (Cook Medical). Both can be easily accessed to perform bowel irrigations. The former is held in with a balloon and is somewhat more protuberant from the abdominal wall. The latter features a small, soft access port that lies flat against the skin. A hinged cap opens for access to the internal part of the tube. The caregiver has to grasp and pull the tube slightly upward to open the trapdoor and engage the connector for the tubing from the enema bag. The tube is held in place by internal coils of the catheter. Both the gastrostomy button and Chait tube can be worn under clothing without any large, noticeable bulges. The gastrostomy button generally can be placed in the office setting after using a measuring device to assess the length of the channel. We have found that the Chait tube should be initially placed and subsequently exchanged in the operating room setting due to the stiffness of the coils and the need for a superstiff guidewire or rigid metal straightener. The need for exchanging the tubes is variable but in our practice is performed generally every 6–12 months or when they become heavily soiled. Complications of these chronic tubes are generally related to inadvertent displacement or granulation tissue around the catheter. The former can be managed temporarily by the caregiver at home by promptly placing and then taping in a standard catheter until a tube can be replaced electively by the provider. Granulation tissue may be treated with cauterization if symptomatic or causing troublesome bleeding.
Another alternative to stomal stenosis is to place an ACE stopper (Medicina Medical). This device is a 100 % silicone short plug with a circular 15 mm disc to keep the stopper in place and help maintain patency of the channel. They come in a variety of lengths and diameters to accommodate different size stomas (Fig. 30.2). It doesn’t pass completely through the continence mechanism so it doesn’t lead to leakage of fecal contents or erosion of the flap mechanism. The use of the stopper has been shown to decrease the rate of stomal stenosis when used prophylactically after creation of the channel [22].

Several available sizes of the ACE stopper (Printed with permission from Medicina Medical)
Urinary Incontinence
One of the more frustrating complications of an appendicovesicostomy is urinary leakage from the stoma. This is typically reported as rare in most series ranging from 5 to 10 % [16]. However, this can be problematic for patients as the leakage is more noticeable and difficult to contain as compared to urethral leakage that may be managed with a diaper or pad. The etiology for the leakage may be technical with an inadequate or too short of a flap valve continence mechanism. Other possibilities may include underlying detrusor decompensation with disruption of the continence mechanism from elevated filling pressures. The initial evaluation should include a fluoroscopic voiding cystourethrogram as well as urodynamic testing to assess bladder anatomy, functional capacity, and bladder compliance.
Medical Management
Although an insufficient sphincter mechanism can be the culprit in channel leakage, the initial intervention, however, should be focused on maximizing the medical management. In addition, an index of suspicion for bladder deterioration or spinal cord tethering should be maintained. In a relatively small number of patients treated with an outlet procedure and a catheterizable channel without bladder augmentation, hostile bladder dynamics may result. A recent review of our experience showed that a very low outlet resistance preoperatively (in other words, a bladder never exposed to high or even normal storage pressures) and a postoperative tethered cord were independent risk factors for bladder deterioration [23]. Aggressive intervention with more frequent catheterizations, maximally tolerated doses of anticholinergics (including combinations of oral medications, intravesical preparations, and/or topical patches), and control of urinary tract infections with gentamicin irrigations are all reasonable to employ.
Botulinum A toxin injected into the detrusor muscle has been described as a treatment option in the management of high filling pressures, although the long-term durability is unknown, and thus the treatment may have to be repeated periodically. The procedure can be performed using a pediatric cystoscope and a long dextranomer-hyaluronic acid injection needle. The dosage is typically 10 IU per kg up to a maximum dose of 200 IU. In our practice, methylene blue is mixed into the solution to allow for tracking of previous injection sites.
Endoscopic Intervention
If there are no new neurological symptoms and a filling cystometrogram shows a compliant, low-pressure reservoir with a low outlet resistance, then treatments based on augmenting or revising the continence mechanism are appropriate. Initial endoscopic approaches with injection therapy can be quite helpful in these situations. With the introduction of the sterile biodegradable gel, dextranomer-hyaluronic acid, in the United States in 2001, for the injectable treatment of vesicoureteral reflux, many reconstructive surgeons have employed it “off label” for the treatment of stress urinary incontinence or fecal leakage in catheterizable channels. The procedure can be scheduled as an outpatient in the operating room under general anesthesia. It can be performed by using a 9 Fr off-set or 10 Fr all-in-one pediatric cystoscope and a long injection needle. The continence mechanism is visualized in an antegrade fashion, and the dextranomer-hyaluronic acid injection is performed circumferentially to better coapt the mucosa. Catheterization is performed after the injection prior to emergence from general anesthesia to ensure it still proceeds smoothly. The bladder can be filled and if there is leakage with gentle suprapubic pressure, more of the gel can be injected. A temporary indwelling catheter is typically not necessary. Complications are rare but can include transient difficulty catheterizing the channel as well as persistent incontinence. Bladder neck incontinence can be treated in a similar fashion through the channel combined with a retrograde approach through the native urethra. Our short-term results with injection techniques for channel incontinence have been encouraging [24]. We have also performed a suprapubic cystotomy for the sole purpose of injecting a patient’s bladder neck.
Surgical Intervention
If optimization of the anticholinergic and catheterization regimen has been performed, and endoscopic injection with a bulking agent is not successful, major surgical revision may be required. This can be approached through the original laparotomy incision. It is often helpful when revising a Mitrofanoff or ACE channel to dismember the stoma from the skin to gain more mobility. Careful attention needs to be maintained to the preservation of the vascularized pedicle. We have found that a long extravesical detrussorraphy (akin to an extravesical ureteral reimplantation) gives excellent continence outcomes along with assurance of a smooth, straight course for catheterization. It is helpful to have the bladder full when choosing the site of implantation along the sidewall of the bladder.
When the channel is completely incompetent and has to be reimplanted again, the detrusor muscle is incised with the bladder full along the expected location of the submucosal tunnel. The tunnel to appendiceal diameter ratio is typically 5:1 or more. Detrusor flaps are created in the plane between the muscle and the underlying mucosa. A small mucosotomy is created distally for the sutured appendicovesical anastomosis with 4-0 or 5-0 polyglactin sutures. The serosa at the distal end of the appendix is anchored to the detrusor flaps in a “vest” fashion and hitched into place to prevent the tunnel from becoming foreshortened during the healing process. The detrusor flaps are then closed with simple interrupted 3-0 polyglactin sutures ensuring that the neohiatus is not constrictive. Each suture incorporates a small bite of the serosa of the appendix to keep it from sliding in the detrusor tunnel. The continence of the channel and its catheterizability can be checked with each suture placed in the detrusor flaps. It is helpful to hitch the sidewall of the bladder to the overlying abdominal wall to keep the channel from being angulated when the bladder is partially full or empty. Our practice has been to leave the channel intubated for 4 weeks if appendix is used but 6 weeks if reconfigured ileum (Monti-Mitrofanoff) was necessary. An endoscopic inspection under anesthesia is performed and then an overnight stay is arranged for catheterization teaching with our team of urology nurse practitioners.
With the increasing usage of laparoscopic techniques in urinary reconstruction, it is feasible to consider approaching a revision of either a Mitrofanoff of ACE channel with a minimally invasive technique. Single-center series of primary channel creation laparoscopically with or without robotic assistance have been described with safe and effective results [25–28]. While a replication of a leaking appendicocecostomy (ACE) may not require extensive dissection, a re-operative reimplantation of a failed Mitrofanoff appendicovesicostomy may be more technically challenging, particularly with obtaining laparoscopic access and dealing with intestinal adhesions after a major laparotomy. No series of channel revisions have been described in the literature as of yet; however, with the advance of technology, these techniques will most certainly be adapted to the reconstruction surgeon’s armamentarium.
Acute Inability to Catheterize
A difficult situation in the care of these patients arises when there is acute difficulty passing the catheter into the channel. It is typically not a dire emergency to address an appendicocecostomy (ACE) that is acutely difficult to catheterize. In contrast, a Mitrofanoff channel that cannot be accessed puts the patient at risk of life-threatening sequelae if the bladder were to perforate, particularly when there is no leakage from the bladder neck, and the patient has a history of a bladder augmentation.
Risk factors for difficulty with catheterization also include a history of nonadherence with the prescribed regimen. In our series of bladder perforations, most patients had documented noncompliance issues as well as a history of bladder stones, possibly suggesting poor drainage habits [3]. Our office has a long-standing habit of checking with our home health care companies to ensure that the appropriate numbers of catheters are being ordered on a monthly basis. While this does not ensure that the catheter is actually being used as ordered, it does raise a red flag when the patient claims that they are dutifully performing the procedure but no refills have been ordered for several months. In addition, obesity is becoming a major public health concern in pediatrics and as patients with myelomeningocele age into adolescence and young adulthood, this can lead to difficulty with passing catheters into their channels and can complicate any surgical attempts to revise a continent reconstruction. Finally, female patients who become pregnant can be assured of increasing difficulty with catheterizations as the uterus enlarges progressively through the pregnancy and puts pressure on the bladder and channel [29, 30].
The acute management includes advising the patient to promptly present to be evaluated. If the patient is in distress and lives a considerable distance from the treating physician, the patient can be referred to the closest community hospital to have a suprapubic aspiration performed or even a percutaneous suprapubic cystostomy placed under ultrasound guidance. If the urologist cannot catheterize the channel in the office or emergency department, the patient must be taken to the operating room for endoscopic evaluation and management. One gentle pass of the catheter under anesthesia is appropriate but if unsuccessful, then inspection of the channel with a small (7 or 10 Fr) pediatric cystoscope is necessary
When treating a false passage, the cystoscope should be advanced into the channel and then withdrawn very slowly from the extent of the false passage back to the cutaneous stoma. The channel can be gently probed with a guidewire to find the true lumen. It can sometimes be difficult due to bleeding and poor visualization if multiple bedside attempts have already been made to drain the bladder. Often the true lumen is just under the surface of the stoma and may appear to be a slit-like opening of mucosa. Once guidewire access is obtained across the true lumen, the scope can be gently advanced over the wire to confirm that the wire is truly in the lumen of the bladder or cecum. The channel can be gently dilated and a Council tip catheter left indwelling for 2–4 weeks. A second-look endoscopy under anesthesia can be helpful to ensure that the lumen has healed and is catheterizable. In the unique case of an appendicocecostomy false passage, an antegrade contrast study either on the operating room table or in the radiology suite can rule out contrast extravasation from an unrecognized intestinal injury [31].
If the reason for the difficulty with catheterization was secondary to stomal stenosis, then steps can be taken as described previously in this chapter. Other possible causes include angulation of the channel when the bladder is extremely full. In some patients with nocturnal polyuria from gastrostomy tube feeds or renal insufficiency, an overnight catheter taped in to the stoma can be helpful to prevent difficulties in the morning when the bladder is full. We have also anecdotally noticed that children that are primarily gastrostomy tube fed can absorb a good deal of their ACE irrigation leading to excessive urine output after their bowel cleanout and thus their catheterization regimen may need to be adjusted in light of the higher volumes.
Bladder Stones
Another common complication of enterocystoplasty is the formation of reservoir stones. In some series, the prevalence has been reported as high as 50 % depending on the predominant intestinal segment used for augmentation [7, 8]. The predominant stone composition is magnesium ammonium phosphate (“triple phosphate” or “struvite”). Struvite stones are potentiated by bacterial infections that hydrolyze urea to ammonium and raise urine pH to neutral or alkaline values. Urea-splitting organisms include Proteus, Pseudomonas, Klebsiella, Staphylococcus, and Mycoplasma. The possible causes for the calculi include mucus production, recurrent urinary tract infections (UTI) with urea-splitting bacteria, as well as nondependent bladder drainage through an abdominal wall stoma rather than the native urethra. The mucus may facilitate the growth of bladder calculi directly by heterogeneous nucleation or indirectly by allowing bacterial growth.
Typical clinical presentations include recurrent UTIs and urinary incontinence but typically not suprapubic pain or renal colic. They can also be incidental findings on routine follow-up ultrasound or radiographic imaging. New bladder instability on a filling cystometrography study in the absence of an active infection may also raise the suspicion for bladder stones. Recurrence rates are high thus an index of suspicion should be maintained in the long-term follow-up of these patients.
Medical Management
Other than uric acid stones which are rare in reconstructed bladders, none of the usual stone types are amenable to medical dissolution. Patients with high mucus loads in the urine or a previous history of bladder stones may benefit from prophylactic high-volume saline irrigations once or twice daily. Irrigation with 4 % urea solutions can be helpful in difficult situations. Recurrent urinary tract infections are initially treated with a switch from “clean” to “sterile” technique including single-use catheters. This may have to be authorized from third-party payers in the United States. Oral antibiotic suppression can be helpful as well as education of other caregivers not to treat asymptomatic bacteriuria unless it is one of the aforementioned urea-splitting organisms. A reassessment of the bowel management protocol is important to rule out chronic fecal retention and overgrowth of bowel flora. Finally, daily gentamicin bladder irrigations have been shown to safely instill the medication directly to the needed area without concern for absorption, even in patients with bladder augmentation and renal allografts [32]. This can minimize the bacterial load when combined with an irrigation regimen to decrease mucus in the reservoir.
Surgical Intervention
Once a bladder stone has been diagnosed, it is reasonable to schedule an elective procedure for stone ablation and removal. For large stone burdens a simple cystotomy through a small suprapubic incision is a rapid and efficient method for complete stone extraction. A short overnight stay with an indwelling catheter will typically suffice for convalescence. For most stone burdens, however, an initial endoscopic treatment is appropriate. Controversy exists whether access through the appendicovesicostomy to treat the stones is safe, but in our experience, short treatments with a 10 Fr panendoscope through the existing channel have not resulted in iatrogenic incontinence or stomal injury. It is important not to attempt to basket out large fragments, however, as they may cause injury to the mucosal lining. Typically, a Holmium laser fiber is employed through a small pediatric cystoscope to break the stone into very small fragments. Suction tubing attached to one of the ports can be used to aspirate the residual fragments. Constant attention to the distension of the bladder is important to maintain during the treatment but temporary drainage after the procedure is usually not necessary.
For larger stone burdens being treated endoscopically, a suprapubic access is quite helpful [33]. A spinal needle can be placed under direct cystoscopic guidance through the previous suprapubic tube scar (or with ultrasound if there is concern about the proximity of intestinal tissue). A guidewire is passed through the spinal needle and the tract can be dilated up sequentially to accommodate an Amplatz sheath (Cook Medical). Another option is to use a smaller “peel-away” vascular access sheath that can be passed over the guidewire. The sheaths are made by several manufacturers and come in various sizes just large enough to accommodate the typical pediatric cystoscopes. The sheath can be used to pass a larger scope that can be allowed by a catheterizable channel and thus result in more efficient stone extraction. It is advisable to place a catheter in the appendicovesicostomy to vent the bladder during the procedure and avoid overdistension of an augmented bladder.
Conversely, a small cystoscope can be placed in the Mitrofanoff channel and then attach suction tubing to the percutaneous sheath. An assistant can then manipulate the sheath along the base of the bladder under direct cystoscopic vision to aspirate all the fragments. Stone extraction rates can be very high with these techniques with minimal morbidity and minimal residual fragments, which is important to decrease recurrent stones. A balloon catheter can then be placed through the sheath and the sheath removed. Our practice has been to leave the suprapubic tract intubated temporarily for at least 72 h with subsequent removal in the office.
Conclusions
Continent lower urinary tract reconstruction is an invaluable tool to treat urinary incontinence, allow accessible intermittent catheterization, and protect the upper urinary tracts from high bladder pressures in children with neuropathic bladders. It has been used extensively in the past few decades around the world and a large body of evidence has been accumulated as to its surgical outcomes and complications. The majority of these complications are manageable with a combination of medical and minimally invasive surgical interventions as outlined in this chapter.
References
Griffiths DM, Malone PS. The Malone antegrade continence enema. J Pediatr Surg. 1995;30(1):68–71.
Wheeler RA, Malone PS. Use of the appendix in reconstructive surgery: a case against incidental appendicectomy. Br J Surg. 1991;78(11):1283–5.
DeFoor W, Tackett L, Minevich E, Wacksman J, Sheldon C. Risk factors for spontaneous bladder perforation after augmentation cystoplasty. Urology. 2003;62(4):737–41.
Sumfest JM, Burns MW, Mitchell ME. The Mitrofanoff principle in urinary reconstruction. J Urol. 1993;150(6):1875–7; discussion 7–8.
Harris CF, Cooper CS, Hutcheson JC, Snyder 3rd HM. Appendicovesicostomy: the mitrofanoff procedure-a 15-year perspective. J Urol. 2000;163(6):1922–6.
Kaefer M, Tobin MS, Hendren WH, Bauer SB, Peters CA, Atala A, et al. Continent urinary diversion: the Children’s Hospital experience. J Urol. 1997;157(4):1394–9.
DeFoor W, Minevich E, Reddy P, Sekhon D, Polsky E, Wacksman J, et al. Bladder calculi after augmentation cystoplasty: risk factors and prevention strategies. J Urol. 2004;172(5 Pt 1):1964–6.
Woodhouse CR, Lennon GN. Management and aetiology of stones in intestinal urinary reservoirs in adolescents. Eur Urol. 2001;39(3):253–9.
Basavaraj DR, Harrison SC. The Mitrofanoff procedure in the management of intractable incontinence: a critical appraisal. Curr Opin Urol. 2006;16(4):244–7.
Fishwick JE, Gough DC, O’Flynn KJ. The Mitrofanoff procedure: does it last? BJU Int. 2000;85(4):496–7.
Liard A, Seguier-Lipszyc E, Mathiot A, Mitrofanoff P. The Mitrofanoff procedure: 20 years later. J Urol. 2001;165(6 Pt 2):2394–8.
Woodhouse CR. The Mitrofanoff principle for continent urinary diversion. World J Urol. 1996;14(2):99–104.
Lemelle JL, Simo AK, Schmitt M. Comparative study of the Yang-Monti channel and appendix for continent diversion in the Mitrofanoff and Malone principles. J Urol. 2004;172(5 Pt 1):1907–10.
Mor Y, Kajbafzadeh AM, German K, Mouriquand PD, Duffy PG, Ransley PG. The role of ureter in the creation of Mitrofanoff channels in children. J Urol. 1997;157(2):635–7.
Sugarman ID, Malone PS, Terry TR, Koyle MA. Transversely tubularized ileal segments for the Mitrofanoff or Malone antegrade colonic enema procedures: the Monti principle. Br J Urol. 1998;81(2):253–6.
Farrugia MK, Malone PS. Educational article: the Mitrofanoff procedure. J Pediatr Urol. 2010;6(4):330–7.
Cain MP, Casale AJ, King SJ, Rink RC. Appendicovesicostomy and newer alternatives for the Mitrofanoff procedure: results in the last 100 patients at Riley Children’s Hospital. J Urol. 1999;162(5):1749–52.
Thomas JC, Dietrich MS, Trusler L, DeMarco RT, Pope JC, Brock 3rd JW, et al. Continent catheterizable channels and the timing of their complications. J Urol. 2006;176(4 Pt 2):1816–20; discussion 20.
Welk BK, Afshar K, Rapoport D, MacNeily AE. Complications of the catheterizable channel following continent urinary diversion: their nature and timing. J Urol. 2008;180(4 Suppl):1856–60.
Snodgrass W. Triamcinolone to prevent stenosis in Mitrofanoff stomas. J Urol. 1999;161(3):928.
Heshmat S, DeFoor W, Minevich E, Reddy P, Reeves D, Sheldon C. Use of customized MIC-KEY gastrostomy button for management of MACE stomal complications. Urology. 2008;72(5):1026–9.
Subramaniam R, Taylor C. The use of an antegrade continence enema stopper in catheterizable channels virtually eliminates the incidence of stomal stenosis: preliminary experience. J Urol. 2009;181(1):299–301.
DeFoor W. Bladder decompensation after continent urinary reconstruction in children with neurogenic bladder. Atlanta: American Urological Association; 2012.
Minevich E. Endoscopic treatment with dextranomer-hyaluronic acid of persistent incontinence following continent urinary reconstruction. London: Joint Congress of the International Children’s Continence Society; 2012.
Wille MA, Jayram G, Gundeti MS. Feasibility and early outcomes of robotic-assisted laparoscopic Mitrofanoff appendicovesicostomy in patients with prune belly syndrome. BJU Int. 2012;109(1):125–9.
Nerli RB, Reddy M, Devraju S, Prabha V, Hiremath MB, Jali S. Laparoscopic mitrofanoff appendicovesicostomy: our experience in children. Indian J Urol. 2012;28(1):28–31.
Badawy H, Eid A, Dawood W, Hanno A. Safety and feasibility of laparoscopic appendicovesicostomy in children. J Pediatr Urol. 2013;9(4):427–31.
Nguyen HT, Passerotti CC, Penna FJ, Retik AB, Peters CA. Robotic assisted laparoscopic Mitrofanoff appendicovesicostomy: preliminary experience in a pediatric population. J Urol. 2009;182(4):1528–34.
Fillingham S. Managing pregnancy in women with urinary diversion. Br J Nurs. 2008;17(18):1154–8.
Greenwell TJ, Venn SN, Creighton S, Leaver RB, Woodhouse CR. Pregnancy after lower urinary tract reconstruction for congenital abnormalities. BJU Int. 2003;92(7):773–7.
Defoor W, Minevich E, Reddy P, Barqawi A, Kitchens D, Sheldon C, et al. Perforation of Malone antegrade continence enema: diagnosis and management. J Urol. 2005;174(4 Pt 2):1644–6.
Defoor W, Ferguson D, Mashni S, Creelman L, Reeves D, Minevich E, et al. Safety of gentamicin bladder irrigations in complex urological cases. J Urol. 2006;175(5):1861–4.
Paez E, Reay E, Murthy LN, Pickard RS, Thomas DJ. Percutaneous treatment of calculi in reconstructed bladder. J Endourol/Endourol Soc. 2007;21(3):334–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer-Verlag London
About this chapter
Cite this chapter
DeFoor, W.R., Reddy, P.P. (2014). Minimally Invasive Techniques to Approach Complications of Enterocystoplasty and Continent Catheterizable Channels. In: Godbole, P., Koyle, M., Wilcox, D. (eds) Pediatric Endourology Techniques. Springer, London. https://doi.org/10.1007/978-1-4471-5394-8_30
Download citation
DOI: https://doi.org/10.1007/978-1-4471-5394-8_30
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-4471-5393-1
Online ISBN: 978-1-4471-5394-8
eBook Packages: MedicineMedicine (R0)