
Abstract
T helper type 17 (TH17) cells are a recently discovered lineage of T cells that produce several effector molecules including IL-17A, IL-17F, IL-21, and IL-22. Scientific evidence to date strongly implicates that this arm of the immune system plays a critical role in mucosal immunity to many extracellular pathogens as well as coordinate adaptive immunity to some intracellular pathogens. In this paper, recent progress in our understanding of these cytokines, their cellular or sources and mechanism of their effector function in the mucosa in various infections is reviewed.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
CD4+ T helper cells are critical mediators of adaptive immune responses. Following interaction with antigen presenting cells, T cells receive signals by engagement of the T cell receptor (signal 1), co-stimulatory molecules (signal 2), and a complex network of cytokine signals (signal 3), then undergo activation and differentiation into effector CD4+ T cells. The critical role these cells play in mucosal immunity was clearly evidenced by the HIV epidemic that leads to the depletion of these cells from the mucosa and periphery (Kader et al. 2009; Mattapallil et al. 2005; Li et al. 2005), leading to the acquired immuno-deficiency syndrome (AIDS).
Five years after the initial clinical description of AIDS in 1981, Mossmann and Coffman described the first two CD4+ T-cells subsets based on discrete cytokine profiles (Mosmann et al. 1986). TH1 effectors produce Interferon-gamma (IFN-γ) and regulate cellular immunity against intracellular infections, whereas TH2 cells produce Interleukin (IL)-4, IL-5, and IL-13 and mediate humoral immunity against parasite infections.
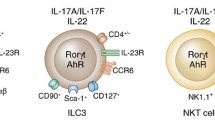
However, these two T-cell subsets do not completely account for the opportunistic infections seen in congenital or acquired absence of CD4+ T-cells such as mucosal candidiasis, Pneumocystis carinii pneumonia, or some bacterial pneumonias. Mice deficient in TH1 or TH2 responses (or both) are not permissive for P. carinii pneumonia (Garvy et al. 1997a, b), a hallmark infection in AIDS patients with low CD4+ T-cell counts. This data suggests that other CD4+ T-cell lineages are critical for host defenses against opportunistic infections. IL-17 was cloned from CD4+ memory cells in 1993 (Rouvier et al. 1993) and Infante-Duarte demonstrated that IL-17 cells could be produced in response to bacterial lipopeptides (Infante-Duarte et al. 2000). This early study showed that IL-17 producing cells were distinct from TH1 cells and thus provided the first evidence that T-cell derived IL-17 may have unique effector functions in host resistance against pathogens (Infante-Duarte et al. 2000). Recent evidence has shown that a major subset of cells that produce IL-17 are distinct from TH1 and TH2 cells and consist of a third subset of T cells referred to as TH17 cells (Langrish et al. 2005; Harrington et al. 2005; Park et al. 2005). TH17 cells produce the cytokines IL-17A (IL-17) (Harrington et al. 2005; Park et al. 2005) and IL-17F (Langrish et al. 2005), as well as the cytokines IL-21 (Nurieva et al. 2007; Korn et al. 2007) and IL-22 (Chung et al. 2006; Liang et al. 2006) (Fig. 1). This new TH17 cell lineage fills in some of the missing gaps in host immunity not fully explained by the TH1/TH2 paradigm.

Overview of Th17 cytokines and immunity at the mucosa. IL-17 and IL-22 can be produced by several immune cells found at mucosal sites in response to a variety of infectious stimuli. IL-17 and IL-22 and signal to the mucosal epithelium, where IL-17 induces G-CSF and CXC chemokine production. These two factors together result in neutrophil recruitment, which is required for bacterial and fungal clearance at mucosal sites. IL-22 and IL-17 can also augment the expression of antimicrobial peptides. IL-22, likely through the activation of STAT3 can also mediate epithelial repair, which is critical to control of extracellular bacterial pathogens. In the setting of vaccine-induced immunity, Th17 cells can induce the production of ligands for CXCR3 and augment the recruitment of IFNγ-producing Th1 cells to control intracellular pathogen growth
IL-17 is the prototype of TH17 cytokines and is the best studied of the TH17 cytokines. The first identified receptor for IL-17, IL-17RA is a Type I trans-membrane protein and is ubiquitously expressed on various organs including lung, kidney, and spleen (Yao et al. 1995). This receptor can bind three members of the IL-17 family including IL-17A, the closely related IL-17F, as well as the most distally related IL-17 family member, IL-17E (Gaffen 2009). The best studied examples of cells that express the receptor for IL-17 are leukocytes, epithelial cells, mesothelial cells, vascular endothelial cells, keratinocytes, and fibroblasts. They respond to IL-17R-mediated signaling by production of granulocyte colony-stimulating factor (G-CSF), IL-6, and IL-8 and mediate granulopoiesis, neutrophil recruitment, and inflammatory responses (Ouyang et al. 2008) (Fig. 1). Recently it has been shown that macrophages (Ishigame et al. 2009) and dendritic cells (Bai et al. 2009; Lin et al. 2009) also respond to IL-17 and produce cytokines and chemokines. Over-expression of IL-17 in mice results in massive extra-medullary hematopoiesis (Schwarzenberger et al. 1998) via the induction of G-CSF and stem cell factor (Schwarzenberger et al. 2000). IL-17RA KO mice can develop spontaneous infection with S. aureus infection around the eyes and nares (Schwarzenberger and Kolls 2002) and this phenotype is also observed in mice deficient in two of the three ligands for this receptor (Ishigame et al. 2009). Interestingly, this phenotype is not observed in IL-17A or IL-17F single KO mice (Ishigame et al. 2009), suggesting that these two cytokines can compensate for each other in this model. Both IL-17A and IL-17RA KO mice show susceptibility to pulmonary infection with the extracellular gram negative bacteria K. pneumoniae, and again with IL-17RA KO mice showing greater susceptibility than IL-17A KO mice (Aujla et al. 2008). In this model, IL-17RA KO mice fail to recruit neutrophils into the lung, in part due to reduced CXC chemokine production (Ye et al. 2001), but also reduced granulopoiesis through reduced G-CSF production (Ye et al. 2001). Through its effects on dendritic cells, IL-17 has been shown to regulate IL-12p70 production by dendritic cells, thereby regulating TH1 response to the intracellular pathogen Francisella tularensis (Lin et al. 2009) and Chlamydia muridarum (Bai et al. 2009). In contrast, IL-17 appears to be dispensable for TH1 immunity to Mycobacterium tuberculosis and Listeria. Thus, data strongly implicates TH17 cytokines in host immunity to both extracellular pathogens and certain intracellular pathogens.
2 Regulation of IL-17 and IL-22 in the Lung
The differentiation of TH17 cells is determined by the exposure to TGF-β, IL-6, and IL-21, while IL-23 further stabilizes the commitment of TH17 cells to this lineage (reviewed in (Korn et al. 2009)). These polarizing cytokines act on newly primed cells to induce the expression of the transcription factor RORγT and RORα which induces TH17 differentiation (Ivanov et al. 2006; Yang et al. 2008). RORγT also controls the expression of IL-23-inducible receptors on newly primed T cells, further expanding their responsiveness to IL-23 in order to sustain the T lineage-specific responses. The gp-130-Stat3 pathway is essential for expression of RORγT and TH17 development. Recently, it has been shown that IL-21 acts downstream of these events to further amplify TH17 cell generation in an autocrine manner. TH17 cells also express high levels of IL-R1 (Chung et al. 2009) and TLR2 (Reynolds et al. 2010), and both IL-1β and TLR2 ligands can activate these cells to produce IL-17 and IL-22. Cellular sources of IL-17 in acute primary pulmonary infection with K. pneumoniae (Happel et al. 2003), M. tuberculosis (Lockhart et al. 2006), or Influenza (Crowe et al. 2009) include γδ T-cells, iNKT cells, and possibly LTi cells (Takatori et al. 2009). In many infections, the γδ T-cell response can be the predominant source, plus the cellular production of IL-17 by these cells is critically regulated by both IL-23 and IL-1β (Sutton et al. 2009; Martin et al. 2009). What remains unclear is the cellular sources of IL-23 and IL-1β in vivo and the γδ T-cell subsets that respond to these signals. In a pulmonary model of Aspergillus infection, Vγ1 T-cells are the dominant source of IL-17 (Romani et al. 2008). However, in a model of chronic Bacillus subtilis infection, the Vγ6 subset dominates (Simonian et al. 2009), while in a pulmonary model of M.bovis BCG, both Vγ6 and Vγ4 dominate (Umemura et al. 2007).
Since over-induction of TH17 cells can impact tissue damage due to induction of inflammatory pathways, the generation of TH17 cells is strictly regulated. For example, cytokines such as IL-27 (Batten et al. 2006; Stumhofer et al. 2006), those belonging to TH1 (IFNγ) and TH2 (IL-4) (Harrington et al. 2005; Park et al. 2005), and IL-2 (Laurence et al. 2007) tightly regulate the induction of TH17 cells. Endogenous lipid mediators like prostaglandin E2 (PGE2) released under inflammatory conditions promote TH17 cells differentiation, suggesting that external infection-induced mediators can also influence the decision between a TH1/TH2/TH17 and T regulatory cell responses.
Several of these TH17 polarizing cytokines such as IL-23, TGF-β, IL-6, and IL-1β are induced in dendritic cells activated by components of microbes. Several bacteria and its products such as Kleibsiella pneumoniae (Happel et al. 2003, 2005), Mycobacterium tuberculosis (Gerosa et al. 2008; Khader et al. 2005), Helicobacter pylori (Mitchell et al. 2007), Francisella tularensis (Butchar et al. 2007), Salmonella enterica (Siegemund et al. 2007), and Bordetella pertussis (Fedele et al. 2005) induce these cytokines through TLR signaling. Further bacterial peptidoglycans can induce the generation of TH17 cells through nucleotide oligomerization domain 2 (NOD2) receptor signaling in dendritic cells (van Beelen et al. 2007). Viruses such as Herpes simplex virus (Kim et al. 2008) and fungus and fungal components such as β-glucans (Gerosa et al. 2008; LeibundGut-Landmann et al. 2007), mannans (Saijo et al. 2010; van de Veerdonk et al. 2009), Cryptococcus (Siegemund and Alber 2008), Candida albicans (LeibundGut-Landmann et al. 2007) and Aspergillus fumigatus (Zelante et al. 2007) can all induce some or all of these polarizing cytokines from dendritic cells and play a role in differentiation of TH17 cells. These studies suggest that relative amounts of the polarizing cytokines induced by the pathogen will define the final outcome of differentiation of naïve T cells to TH1, TH2, TH17, or T regulatory cells during infection.
3 TH17 Effector Responses in the Mucosa
Human bronchial lung epithelial (HBE) cells express both IL-17RA, IL-17RC, IL-22R, and IL-10R2 and thus can respond to IL-17A, IL-17F, and IL-22 (McAllister et al. 2005; Kuestner et al. 2007; Aujla et al. 2008; Huang et al. 2007, Fig. 1). The expression of IL-17RA and IL-17RC also appears in a basolateral dominant fashion (McAllister et al. 2005; Huang et al. 2007) such that signaling only occurs in polarized epithelial cells which are exposed to ligands provided by the basolateral surface (Uesugi et al. 2001; Huang et al. 2007). Treatment of HBE cells with IL-17 induces CXC chemokines such as IL-8 (McAllister et al. 2005; Jones and Chan 2002), G-CSF (McAllister et al. 2005), and antimicrobial proteins such as human β-defensin 2 (Kao et al. 2004). IL-17 treatment also induces IL-19 (Huang et al. 2008), which may be important in regulating TH2 responses in the mucosa. IL-17 also induced the expression of the polymeric immunoglobulin receptor (Aujla et al. 2008) and indeed TH17 cytokines have been shown to be critical in generating mucosal IgA responses (Jaffar et al. 2009). IL-22 can activate STAT3 (Wolk et al. 2010) in both murine and human lung epithelial cells and synergizes with IL-17 to increases the expression of human antimicrobial genes such as HBD2, lipocalin (Aujla et al. 2008), and the calgranulins (Aujla et al. 2008). An activity that is unique to IL-22 and not shared by IL-17A or IL-17F in human lung epithelial cells is the fact that IL-22 can augment the clonogenic potential of these cells and accelerate wound repair (Aujla et al. 2008). In skin keratinocytes, IL-22 can also cause acanthosis and hyper-proliferation (Zheng et al. 2007). Thus, IL-22 may be important to epithelial repair in infection, as well as augmenting barrier function (Fig. 1). Neutralizing IL-22 in vivo leads to rapid dissemination of bacteria from the lung during K. pneumoniae infection (Aujla et al. 2008). Mucosal IL-22 administration can reduce local bacterial growth as well as prevent dissemination in this model (Aujla et al. 2008). The cellular source of IL-22 in the model is unclear, as IL-22 producing cells are present in Rag 2−/− mice but not Rag 2−/−, and γC double KO mice demonstrate that IL-22 producers are γC dependent.
4 TH17 Cytokines and Bacterial Infections at the Mucosa
As mentioned above, early work in IL-17RA KO mice demonstrates increased sensitivity to cutaneous S. aureus (Schwarzenberger and Kolls 2002; Ishigame et al. 2009; Cho et al. 2010) and pulmonary K. pneumoniae (Ye et al. 2001) infection and established a critical role for IL-17 in protective immunity against extracellular bacteria. Further studies show that TH17 cells play a protective role against extracellular bacterial infections in the gut mucosa. Citrobacter rodentum, a naturally occurring mouse pathogen, requires the generation of IL-23-dependent TH17 cells in the lamina propria for protection (Mangan et al. 2006; Ishigame et al. 2009). Also, IL-22 contributes to the early host defense against C.rodentium through the direct induction of the Reg family of antimicrobial proteins in colonic epithelial cells (Zheng et al. 2008). IL-17 signaling also appears to be host-protective in the oral mucosa, as IL-17R-deficient mice are highly susceptible to infection by the gram-negative anaerobic periodontal pathogen, Porphyromonas gingivalis, due to reduced neutrophil mobilization and recruitment (Yu et al. 2008).
Although these studies strongly suggest that TH17 cytokine responses are protective against most extracellular pathogens, in some cases, TH17 responses contribute to tissue pathology. This was first shown in response to chronic biofilm infection with Pseudomonas aeruginosa where IL-23 deficient mice had markedly reduced IL-17 responses and less tissue pathology in response to chronic mucoid P. aeruginosa infection. Furthermore, in whooping cough, an infection caused by B. pertussis, a gram negative extracellular bacterial infection in the respiratory tract resulted in persistent cough as one of the hallmarks of the clinical disease. Accumulating evidence suggests that the B. pertussis infection may bias the host response towards the production of TH17 cytokines (Siciliano et al. 2006; Fedele et al. 2008) by preferentially inhibiting IL-12 and inducing IL-23 (Fedele et al. 2008). B. pertussis causes severe respiratory pathology including bronchiectasis, while B. parapertussis causes less severe disease pathology (Carbonetti 2007). Interestingly, B. pertussis lipooligosaccharide induces potent production of IL-23, IL-1β, and IL-6 from DCs and drives a more robust differentiation of naïve CD4 T cells to TH17 cells when compared to DCs activated with LPS from B. parapertussis (Fedele et al. 2008). The current emerging hypothesis is that host bias towards TH17 following B. pertussis infection results in inflammation and destruction of the airways, leading to bronchiectasis and persistent cough. This hypothesis is further supported by another cause of bronchiectasis, cystic fibrosis, which is highly associated with bronchiectasis due to chronic biofilm infection with P. aeruginosa and elevated IL-17 and IL-22 responses in draining lung lymph node cells (Aujla et al. 2008). Following M. tuberculosis infection, the lung inflammation was caused by repeated vaccinations with BCG and resulted in pathological consequences that were IL-17 dependent (Cruz et al. 2010). These disease models may serve as an example for the role of IL-17 in mediating pathology while conferring protection against extracellular bacterial infections in the respiratory mucosa. These findings are not confined to the lung. In H.pylori infection in the gastrointestinal tract, the TH17 response may culminate in a pathogenic inflammatory response in the gut mucosa (Luzza et al. 2000; Caruso et al. 2008). In contrast, certain intracellular pathogens that may require both TH1 cells and neutrophils for protection at mucosal sites may be dependent on IL-23/IL-17 for pathogen control. For example, the induction of IL-17 and IL-17F production following acute Mycoplasma pneumonia pulmonary infection is IL-23-dependent and contributes to neutrophil recruitment and mediates protection against the infection (Wu et al. 2007). Also, infection with Salmonella typhimurium, which can exist as an intracellular pathogen, results in induction of IL-17 and IL-22 in the ileal mucosa. The absence of IL-17R signaling results in increased translocation of the bacteria to the mesenteric lymph nodes, reduced induction of chemokines, anti-microbials, and reduced neutrophilic recruitment to the ileal mucosa (Raffatellu et al. 2008). Using a macaque model of Simian Immuno-deficiency Virus (SIV) to study HIV human disease and related complications arising due to bacterial co-infections such as S.typhimurium, it was found that SIV co-infection selectively inhibits TH17 responses elicited by S. typhimurium, probably due to depletion of CD4+ T cells in the ileal mucosa (Raffatellu et al. 2008). This results in an inability of SIV-infected macaques to mount normal mucosal inflammatory response to S. typhimurium infection and allows dissemination of bacteria into the mesenteric lymph node. This data may provides a basis for the observation that people with HIV are at a increased risk of developing bacteremia due to dissemination of bacteria resulting from reduced CD4 TH17 responses. HIV-infected individuals that receive anti-retroviral therapy undergo effective CD4 T-cell restoration and this is usually associated with enhanced CD4 TH17-cell accumulation (Macal et al. 2008).
5 TH17 Cytokines and Fungal Infections at the Mucosa
The role of TH17 cytokines in fungal infection has been controversial, but emerging evidence in both animal and human models shows that these cytokines play a critical role in mucosal infections. Initial observations suggested that TH17 cytokines, particularly IL-17, contribute to tissue pathology in invasive aspergillus infections in the lung, predominantly in the setting of NADPH oxidase deficiency (Romani et al. 2008). However, IL-17 and IL-17RA signaling are critical for host resistance to oro-pharyngeal candidiasis and for the expression of mouse β-defensin 3 that has anti-Candicidal activity (Conti et al. 2009). Patients with Hyper IgE syndrome (HIES) that frequently suffer from oro-pharyngeal candidiasis have mutations in STAT3 (Holland et al. 2007; Minegishi et al. 2007). They fail to generate Candida specific TH17 cells, adding further evidence that this phenotype is tightly linked to TH17 immunity (Milner et al. 2008; de et al. 2008). Treatment of skin keratinocytes with TH17 cytokines markedly increases anti-Candicidal activity in vitro, while activated T-cells from HIES patients are unable to induce this anti-Candicidal activity. It has recently been shown that patients with chronic mucocutaneous candidiasis also have antibodies that can block IL-17 and/or IL-22 which may also explain the susceptibility of these patients to mucosal Candida infection (Puel et al. 2010). In respiratory tract models of fungal infections using Pneumocytis carnii (Rudner et al. 2007) and Aspergillus fumigatus (Werner et al. 2009), induction of IL-23 and IL-17 following pathogen challenge is protective, since IL-23KO mice or neutralization of the IL-23/IL-17 axis resulted in impaired clearance of the pathogen.
6 TH17 Cytokines and Viral Infection
The role of TH17 cytokines in viral infection is a rapidly emerging area of research. Herpes simplex virus (HSV-1) infection of the cornea results in early induction of both IL-23 (Kim et al. 2008) and IL-17 (Molesworth-Kenyon et al. 2008). IL-17RA KO mice have also reduced early infiltration of neutrophils and corneal opacity following HSV infection (Molesworth-Kenyon et al. 2008). In contrast, IL-23KO mice have exacerbated disease and pathology possibly due to HSV increased IL-12 responses and increased IFNγ producing cells (Kim et al. 2008). In pulmonary influenza infection, IL-17R KO mice had record tissue pathology and weight loss suggesting that in this model, IL-17 contributes to tissue pathology as well (Crowe et al. 2009). In a heterotypic influenza model, CD8+ cells that produce IL-17 can mediate protection against influenza challenge (Hamada et al. 2009). Thus, the role of the IL-17 response to primary influenza infection versus heterotypic infection appears to differ. Human rhinovirus (HRV) infections are associated with exacerbations of asthma and chronic obstructive pulmonary infiltration. IL-17 was shown to function synergistically with HRV to induce IL-8 from epithelial cells and may contribute to the recruitment of neutrophils, immature DCs, and memory T cells to the lung; contributing to severe inflammatory profiles seen during viral exacerbations of airway disease (Wiehler and Proud 2007).
7 Conclusions
We specifically did not address the role of TH17 cytokines vaccine-induced immunity as this has been recently reviewed (Khader et al. 2009). Current data suggests that TH17 cells have evolved to mediate protective immunity against a variety of pathogens at different mucosal sites. Moreover, deficient TH17 responses explain in part, the increased susceptibility to certain infections such as mucocutaneous in HIES patients and the depletion of TH17 cells by HIV. Taken together, strategies to augment these cells or recover these cell populations will be important for improved vaccine or therapeutic efficacy in these patients. It is important to remember that IL-17 is evolutionary conserved and that the gene exists in mollusks and Ciona intestinalis. This predates the development of adaptive T-cell immunity, and this cytokine likely bridged innate and adaptive immunity. What remains unclear is how evolutionary pressure forced this gene to be expressed in memory CD4+ T-cells in mammals. This will be an important area of future investigation.
References
Aujla, S.J., Chan, Y.R., Zheng, M., Fei, M., Askew, D.J., Pociask, D.A., Reinhart, T.A., McAllister, F., Edeal, J., Gaus, K., Husain, S., Kreindler, J.L., Dubin, P.J., Pilewski, J.M., Myerburg, M.M., Mason, C.A., Iwakura, Y., and Kolls, J.K. (2008). IL-22 mediates mucosal host defense against Gram-negative bacterial pneumonia. Nat. Med. 14, 275–281.
Bai, H., Cheng, J., Gao, X., Joyee, A.G., Fan, Y., Wang, S., Jiao, L., Yao, Z., and Yang, X. (2009). IL-17/Th17 promotes type 1 T cell immunity against pulmonary intracellular bacterial infection through modulating dendritic cell function. J. Immunol. 183, 5886–5895.
Batten, M., Li, J., Yi, S., Kljavin, N.M., Danilenko, D.M., Lucas, S., Lee, J., De Sauvage, F.J., and Ghilardi, N. (2006). Interleukin 27 limits auto-immune encephalomyelitis by suppressing the development of interleukin 17-producing T cells. Nat. Immunol. 7, 929–936.
Butchar, J.P., Rajaram, M.V., Ganesan, L.P., Parsa, K.V., Clay, C.D., Schlesinger, L.S., and Tridandapani, S. (2007). Francisella tularensis induces IL-23 production in human monocytes. J. Immunol. 178, 4445–4454.
Carbonetti, N.H. (2007). Immuno-modulation in the pathogenesis of Bordetella pertussis infection and disease. Curr. Opin. Pharmacol. 7, 272–278.
Caruso, R., Fina, D., Paoluzi, O.A., Del Vecchio, B.G., Stolfi, C., Rizzo, A., Caprioli, F., Sarra, M., Andrei, F., Fantini, M.C., Macdonald, T.T., Pallone, F., and Monteleone, G. (2008). IL-23-mediated regulation of IL-17 production in Helicobacter pylori-infected gastric mucosa. Eur. J. Immunol. 38, 470–478.
Cho, J.S., Pietras, E.M., Garcia, N.C., Ramos, R.I., Farzam, D.M., Monroe, H.R., Magorien, J.E., Blauvelt, A., Kolls, J.K., Cheung, A.L., Cheng, G., Modlin, R.L., and Miller, L.S. (2010). IL-17 is essential for host defense against cutaneous Staphylococcus aureus infection in mice. J. Clin. Invest 120, 1762–1773.
Chung, Y., Chang, S.H., Martinez, G.J., Yang, X.O., Nurieva, R., Kang, H.S., Ma, L., Watowich, S.S., Jetten, A.M., Tian, Q., and Dong, C. (2009). Critical regulation of early Th17 cell differentiation by interleukin-1 signaling. Immunity 30, 576–587.
Chung, Y., Yang, X., Chang, S.H., Ma, L., Tian, Q., and Dong, C. (2006). Expression and regulation of IL-22 in the IL-17-producing CD4+ T lymphocytes. Cell. Res. 16, 902–907.
Conti, H.R., Shen, F., Nayyar, N., Stocum, E., Sun, J.N., Lindemann, M.J., Ho, A.W., Hai, J.H., Yu, J.J., Jung, J.W., Filler, S.G., Masso-Welch, P., Edgerton, M., and Gaffen, S.L. (2009). Th17 cells and IL-17 receptor signaling are essential for mucosal host defense against oral candidiasis. J. Exp. Med. 206, 299–311.
Crowe, C.R., Chen, K., Pociask, D.A., Alcorn, J.F., Krivich, C., Enelow, R.I., Ross, T.M., Witztum, J.L., and Kolls, J.K. (2009). Critical role of IL-17RA in immuno-pathology of influenza infection. J. Immunol. 183, 5301–5310.
Cruz, A., Fraga, A.G., Fountain, J.J., Rangel-Moreno, J., Torrado, E., Saraiva, M., Pereira, D.R., Randall, T.D., Pedrosa, J., Cooper, A.M., and Castro, A.G. (2010). Pathological role of interleukin 17 in mice subjected to repeated BCG vaccination after infection with Mycobacterium tuberculosis. J. Exp. Med. 207, 1609–1616.
de, B.L., Puel, A., Filipe-Santos, O., Cobat, A., Ghandil, P., Chrabieh, M., Feinberg, J., von, B.H., Samarina, A., Janniere, L., Fieschi, C., Stephan, J.L., Boileau, C., Lyonnet, S., Jondeau, G., Cormier-Daire,V., Le,M.M., Hoarau,C., Lebranchu,Y., Lortholary,O., Chandesris,M.O., Tron, F., Gambineri, E., Bianchi, L., Rodriguez-Gallego, C., Zitnik, S.E., Vasconcelos, J., Guedes, M., Vitor, A.B., Marodi, L., Chapel, H., Reid, B., Roifman, C., Nadal, D., Reichenbach, J., Caragol, I., Garty, B.Z., Dogu, F., Camcioglu, Y., Gulle, S., Sanal, O., Fischer, A., Abel, L., Stockinger, B., Picard, C., and Casanova, J.L. (2008). Mutations in STAT3 and IL12RB1 impair the development of human IL-17-producing T cells. J. Exp. Med. 205, 1543–1550.
Fedele, G., Nasso, M., Spensieri, F., Palazzo, R., Frasca, L., Watanabe, M., and Ausiello, C.M. (2008). Lipopolysaccharides from Bordetella pertussis and Bordetella parapertussis differently modulate human dendritic cell functions resulting in divergent prevalence of Th17-polarized responses. J. Immunol. 181, 208–216.
Fedele, G., Stefanelli, P., Spensieri, F., Fazio, C., Mastrantonio, P., and Ausiello, C.M. (2005). Bordetella pertussis infected human monocyte-derived dendritic cells undergo maturation and induce Th1 polarization and interleukin-23 expression. Infect. Immun. 73, 1590–1597.
Gaffen, S.L. (2009). Structure and signaling in the IL-17 receptor family. Nat. Rev. Immunol. 9, 556–567.
Garvy, B.A., Ezekowitz, R.A., and Harmsen, A.G. (1997a). Role of gamma interferon in the host immune and inflammatory responses to Pneumocystis carinii infection. Infect. Immun. 65, 373–379.
Garvy, B.A., Wiley, J.A., Gigliotti, F., and Harmsen, A.G. (1997b). Protection against Pneumocystis carinii pneumonia by antibodies generated from either T helper 1 or T helper 2 responses. Infection & Immunity 65, 5052–5056.
Gerosa, F., Baldani-Guerra, B., Lyakh, L.A., Batoni, G., Esin, S., Winkler-Pickett, R.T., Consolaro, M.R., De, M.M., Giachino, D., Robbiano, A., Astegiano, M., Sambataro, A., Kastelein, R.A., Carra, G., and Trinchieri, G. (2008). Differential regulation of interleukin 12 and interleukin 23 production in human dendritic cells. J. Exp. Med. 205, 1447–1461.
Hamada, H., Garcia-Hernandez, M.L., Reome, J.B., Misra, S.K., Strutt, T.M., McKinstry, K.K., Cooper, A.M., Swain, S.L., and Dutton, R.W. (2009). Tc17, a unique subset of CD8 T cells that can protect against lethal influenza challenge. J. Immunol. 182, 3469–3481.
Happel, K.I., Dubin, P.J., Zheng, M., Ghilardi, N., Lockhart, C., Quinton, L.J., Odden, A.R., Shellito, J.E., Bagby, G.J., Nelson, S., and Kolls, J.K. (2005). Divergent roles of IL-23 and IL-12 in host defense against Klebsiella pneumoniae. J. Exp. Med. 202, 761–769.
Happel, K.I., Zheng, M., Young, E., Quinton, L.J., Lockhart, E., Ramsay, A.J., Shellito, J.E., Schurr, J.R., Bagby, G.J., Nelson, S., and Kolls, J.K. (2003). Cutting Edge: Roles of Toll-Like Receptor 4 and IL-23 in IL-17 Expression in Response to Klebsiella pneumoniae Infection. J. Immunol. 170, 4432–4436.
Harrington, L.E., Hatton, R.D., Mangan, P.R., Turner, H., Murphy, T.L., Murphy, K.M., and Weaver,C.T. (2005). Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat. Immunol. 6, 1123–1132.
Holland, S.M., DeLeo, F.R., Elloumi, H.Z., Hsu, A.P., Uzel, G., Brodsky, N., Freeman, A.F., Demidowich, A., Davis, J., Turner, M.L., Anderson, V.L., Darnell, D.N., Welch, P.A., Kuhns, D.B., Frucht, D.M., Malech, H.L., Gallin, J.I., Kobayashi, S.D., Whitney, A.R., Voyich, J.M., Musser, J.M., Woellner, C., Schaffer, A.A., Puck, J.M., and Grimbacher, B. (2007). STAT3 mutations in the hyper-IgE syndrome. N. Engl. J. Med. 357, 1608–1619.
Huang, F., Kao, C.Y., Wachi, S., Thai, P., Ryu, J., and Wu, R. (2007). Requirement for both JAK-mediated PI3K signaling and ACT1/TRAF6/TAK1-dependent NF-kappaB activation by IL-17A in enhancing cytokine expression in human airway epithelial cells. J. Immunol. 179, 6504–6513.
Huang, F., Wachi, S., Thai, P., Loukoianov, A., Tan, K.H., Forteza, R.M., and Wu, R. (2008). Potentiation of IL-19 expression in airway epithelia by IL-17A and IL-4/IL-13: important implications in asthma. J. Allergy Clin. Immunol. 121, 1415–21, 1421.
Infante-Duarte, C., Horton, H.F., Byrne, M.C., and Kamradt, T. (2000). Microbial lipopeptides induce the production of IL-17 in Th cells. J. Immunol. 165, 6107–6115.
Ishigame, H., Kakuta, S., Nagai, T., Kadoki, M., Nambu, A., Komiyama, Y., Fujikado, N., Tanahashi, Y., Akitsu, A., Kotaki, H., Sudo, K., Nakae, S., Sasakawa, C., and Iwakura,Y. (2009). Differential roles of interleukin-17A and -17F in host defense against mucoepithelial bacterial infection and allergic responses. Immunity 30, 108–119.
Ivanov, I.I., McKenzie, B.S., Zhou, L., Tadokoro, C.E., Lepelley, A., Lafaille, J.J., Cua, D.J., and Littman, D.R. (2006). The orphan nuclear receptor RORgammat directs the differentiation program of pro-inflammatory IL-17+ T helper cells. Cell. 126, 1121–1133.
Jaffar, Z., Ferrini, M.E., Herritt, L.A., and Roberts, K. (2009). Cutting edge: Lung mucosal Th17-mediated responses induce polymeric Ig receptor expression by the airway epithelium and elevate secretory IgA levels. J. Immunol. 182, 4507–4511.
Jones, C.E. and Chan, K. (2002). Interleukin-17 stimulates the expression of interleukin-8, growth-related oncogene-alpha, and granulocyte-colony-stimulating factor by human airway epithelial cells. Am. J. Respir. Cell Mol. Biol. 26, 748–753.
Kader, M., Wang, X., Piatak, M., Lifson, J., Roederer, M., Veazey, R., and Mattapallil, J.J. (2009). Alpha4(+)beta7(hi)CD4(+) memory T cells harbor most Th-17 cells and are preferentially infected during acute SIV infection. Mucosal. Immunol. 2, 439–449.
Kao, C.Y., Chen, Y., Thai, P., Wachi, S., Huang, F., Kim, C., Harper, R.W., and Wu,R. (2004). IL-17 markedly up-regulates beta-defensin-2 expression in human airway epithelium via JAK and NF-kappaB signaling pathways. J. Immunol. 173, 3482–3491.
Khader, S.A., Gaffen, S.L., and Kolls, J.K. (2009). Th17 cells at the crossroads of innate and adaptive immunity against infectious diseases at the mucosa. Mucosal. Immunol. 2, 403–411.
Khader, S.A., Pearl, J.E., Sakamoto, K., Gilmartin, L., Bell, G.K., Jelley-Gibbs, D.M., Ghilardi, N., deSauvage, F., and Cooper, A.M. (2005). IL-23 compensates for the absence of IL-12p70 and is essential for the IL-17 response during tuberculosis but is dispensable for protection and antigen-specific IFN-gamma responses if IL-12p70 is available. J. Immunol. 175, 788–795.
Kim, B., Sarangi, P.P., Azkur, A.K., Kaistha, S.D., and Rouse, B.T. (2008). Enhanced viral immuno-inflammatory lesions in mice lacking IL-23 responses. Microbes. Infect. 10, 302–312.
Korn, T., Bettelli, E., Gao, W., Awasthi, A., Jager, A., Strom, T.B., Oukka, M., and Kuchroo, V.K. (2007). IL-21 initiates an alternative pathway to induce pro-inflammatory T(H)17 cells. Nature 448, 484–487.
Korn, T., Bettelli, E., Oukka, M., and Kuchroo, V.K. (2009). IL-17 and Th17 Cells. Annu. Rev. Immunol. 27, 485–517.
Kuestner, R.E., Taft, D.W., Haran, A., Brandt, C.S., Brender, T., Lum, K., Harder, B., Okada, S., Ostrander, C.D., Kreindler, J.L., Aujla, S.J., Reardon, B., Moore, M., Shea, P., Schreckhise, R., Bukowski, T.R., Presnell, S., Guerra-Lewis, P., Parrish-Novak, J., Ellsworth, J.L., Jaspers, S., Lewis, K.E., Appleby, M., Kolls, J.K., Rixon, M., West, J.W., Gao, Z., and Levin, S.D. (2007). Identification of the IL-17 receptor related molecule IL-17RC as the receptor for IL-17F. J. Immunol. 179, 5462–5473.
Langrish, C.L., Chen, Y., Blumenschein, W.M., Mattson, J., Basham, B., Sedgwick, J.D., McClanahan, T., Kastelein, R.A., and Cua, D.J. (2005). IL-23 drives a pathogenic T cell population that induces auto-immune inflammation. J. Exp. Med. 201, 233–240.
Laurence, A., Tato, C.M., Davidson, T.S., Kanno, Y., Chen, Z., Yao, Z., Blank, R.B., Meylan, F., Siegel, R., Hennighausen, L., Shevach, E.M., and O’Shea, J.J. (2007). Interleukin-2 signaling via STAT5 constrains T helper 17 cell generation. Immunity. 26, 371–381.
LeibundGut-Landmann, S., Gross, O., Robinson, M.J., Osorio, F., Slack, E.C., Tsoni, S.V., Schweighoffer, E., Tybulewicz, V., Brown, G.D., Ruland, J., and Reis E Sousa (2007). Syk- and CARD9-dependent coupling of innate immunity to the induction of T helper cells that produce interleukin 17. Nat. Immunol. 8, 630–638.
Li, Q., Duan, L., Estes, J.D., Ma, Z.M., Rourke, T., Wang, Y., Reilly, C., Carlis, J., Miller, C.J., and Haase, A.T. (2005). Peak SIV replication in resting memory CD4+ T cells depletes gut lamina propria CD4+ T cells. Nature 434, 1148–1152.
Liang, S.C., Tan, X.Y., Luxenberg, D.P., Karim, R., Dunussi-Joannopoulos, K., Collins, M., and Fouser, L.A. (2006). Interleukin (IL)-22 and IL-17 are co-expressed by Th17 cells and cooperatively enhance expression of antimicrobial peptides. J. Exp. Med. 203, 2271–2279.
Lin, Y., Ritchea, S., Logar, A., Slight, S., Messmer, M., Rangel-Moreno, J., Guglani, L., Alcorn, J.F., Strawbridge, H., Park, S.M., Onishi, R., Nyugen, N., Walter, M.J., Pociask, D., Randall, T.D., Gaffen, S.L., Iwakura, Y., Kolls, J.K., and Khader, S.A. (2009). Interleukin-17 is required for T helper 1 cell immunity and host resistance to the intracellular pathogen Francisella tularensis. Immunity 31, 799–810.
Lockhart, E., Green, A.M., and Flynn, J.L. (2006). IL-17 production is dominated by gammadelta T cells rather than CD4 T cells during Mycobacterium tuberculosis infection. J. Immunol. 177, 4662–4669.
Luzza, F., Parrello, T., Monteleone, G., Sebkova, L., Romano, M., Zarrilli, R., Imeneo, M., and Pallone, F. (2000). Up-regulation of IL-17 is associated with bioactive IL-8 expression in Helicobacter pylori-infected human gastric mucosa. J. Immunol. 165, 5332–5337.
Macal, M., Sankaran, S., Chun, T.W., Reay, E., Flamm, J., Prindiville, T.J., and Dandekar, S. (2008). Effective CD4+ T-cell restoration in gut-associated lymphoid tissue of HIV-infected patients is associated with enhanced Th17 cells and polyfunctional HIV-specific T-cell responses. Mucosal. Immunol. 1, 475–488.
Mangan, P.R., Harrington, L.E., O’Quinn, D.B., Helms, W.S., Bullard, D.C., Elson, C.O., Hatton, R.D., Wahl, S.M., Schoeb, T.R., and Weaver, C.T. (2006). Transforming growth factor-β induces development of the TH17 lineage. Nature 441, 231–234.
Martin, B., Hirota, K., Cua, D.J., Stockinger, B., and Veldhoen, M. (2009). Interleukin-17-producing gammadelta T cells selectively expand in response to pathogen products and environmental signals. Immunity 31, 321–330.
Mattapallil, J.J., Douek, D.C., Hill, B., Nishimura, Y., Martin, M., and Roederer,M. (2005). Massive infection and loss of memory CD4+ T cells in multiple tissues during acute SIV infection. Nature 434, 1093–1097.
McAllister, F., Henry, A., Kreindler, J.L., Dubin, P.J., Ulrich, L., Steele, C., Finder, J.D., Pilewski, J.M., Carreno, B.M., Goldman, S.J., Pirhonen, J., and Kolls, J.K. (2005). Role of IL-17A, IL-17F, and the IL-17 Receptor in Regulating Growth-Related Oncogene-{alpha} and Granulocyte Colony-Stimulating Factor in Bronchial Epithelium: Implications for Airway Inflammation in Cystic Fibrosis. J. Immunol. 175, 404–412.
Milner,J.D., Brenchley,J.M., Laurence,A., Freeman,A.F., Hill,B.J., Elias,K.M., Kanno,Y., Spalding,C., Elloumi,H.Z., Paulson,M.L., Davis,J., Hsu,A., Asher,A.I., O’Shea,J., Holland,S.M., Paul,W.E., and Douek,D.C. (2008). Impaired T(H)17 cell differentiation in subjects with autosomal dominant hyper-IgE syndrome. Nature 452, 773–776.
Minegishi,Y., Saito,M., Tsuchiya,S., Tsuge,I., Takada,H., Hara,T., Kawamura,N., Ariga,T., Pasic,S., Stojkovic,O., Metin,A., and Karasuyama,H. (2007). Dominant-negative mutations in the DNA-binding domain of STAT3 cause hyper-IgE syndrome. Nature 448, 1058–1062.
Mitchell, P., Germain, C., Fiori, P.L., Khamri, W., Foster, G.R., Ghosh, S., Lechler, R.I., Bamford, K.B., and Lombardi, G. (2007). Chronic exposure to Helicobacter pylori impairs dendritic cell function and inhibits Th1 development. Infect. Immun. 75, 810–819.
Molesworth-Kenyon, S.J., Yin, R., Oakes, J.E., and Lausch, R.N. (2008). IL-17 receptor signaling influences virus-induced corneal inflammation. J. Leukoc. Biol. 83, 401–408.
Mosmann, T.R., Cherwinski, H., Bond, M.W., Giedlin, M.A., and Coffman, R.L. (1986). Two types of murine helper T cell clone. I. Definition according to profiles of lymphokine activities and secreted proteins. J. Immunol. 136, 2348–2357.
Nurieva, R., Yang, X.O., Martinez, G., Zhang, Y., Panopoulos, A.D., Ma, L., Schluns, K., Tian, Q., Watowich, S.S., Jetten, A.M., and Dong, C. (2007). Essential autocrine regulation by IL-21 in the generation of inflammatory T cells. Nature 448, 480–483.
Ouyang, W., Kolls, J.K., and Zheng, Y. (2008). The biological functions of T helper 17 cell effector cytokines in inflammation. Immunity 28, 454–467.
Park, H., Li, Z., Yang, X.O., Chang, S.H., Nurieva, R., Wang, Y.H., Wang, Y., Hood, L., Zhu, Z., Tian, Q., and Dong, C. (2005). A distinct lineage of CD4 T cells regulates tissue inflammation by producing interleukin 17. Nat. Immunol. 6, 1133–1141.
Puel, A., Doffinger, R., Natividad, A., Chrabieh, M., Barcenas-Morales, G., Picard, C., Cobat, A., Ouachee-Chardin, M., Toulon, A., Bustamante, J., Al-Muhsen, S., Al-Owain, M., Arkwright, P.D., Costigan, C., McConnell, V., Cant, A.J., Abinun, M., Polak, M., Bougneres, P.F., Kumararatne, D., Marodi, L., Nahum, A., Roifman, C., Blanche, S., Fischer, A., Bodemer, C., Abel, L., Lilic, D., and Casanova, J.L. (2010). Auto-antibodies against IL-17A, IL-17F, and IL-22 in patients with chronic mucocutaneous candidiasis and auto-immune polyendocrine syndrome type I. J. Exp. Med. 207, 291–297.
Raffatellu, M., Santos, R.L., Verhoeven, D.E., George, M.D., Wilson, R.P., Winter, S.E., Godinez, I., Sankaran, S., Paixao, T.A., Gordon, M.A., Kolls, J.K., Dandekar, S., and Baumler, A.J. (2008). Simian immunodeficiency virus-induced mucosal interleukin-17 deficiency promotes Salmonella dissemination from the gut. Nat. Med. 14, 421–428.
Reynolds, J.M., Pappu, B.P., Peng, J., Martinez, G.J., Zhang, Y., Chung, Y., Ma, L., Yang, X.O., Nurieva, R.I., Tian, Q., and Dong, C. (2010). Toll-like receptor 2 signaling in CD4(+) T lymphocytes promotes T helper 17 responses and regulates the pathogenesis of auto-immune disease. Immunity 32, 692–702.
Romani, L., Fallarino, F., De Luca, A., Montagnoli, C., D’Angelo, C., Zelante, T., Vacca, C., Bistoni, F., Fioretti, M.C., Grohmann, U., Segal, B.H., and Puccetti, P. (2008). Defective tryptophan catabolism underlies inflammation in mouse chronic granulomatous disease. Nature 451, 211–215.
Rouvier, E., Luciani, M.F., Mattei, M.G., Denizot, F., and Golstein, P. (1993). CTLA-8, cloned from an activated T cell, bearing AU-rich messenger RNA instability sequences, and homologous to a herpes virus saimiri gene. J. Immunol. 150, 5445–5456.
Rudner, X.L., Happel, K.I., Young, E.A., and Shellito, J.E. (2007). Interleukin-23 (IL-23)-IL-17 cytokine axis in murine Pneumocystis carinii infection. Infect. Immun. 75, 3055–3061.
Saijo, S., Ikeda, S., Yamabe, K., Kakuta, S., Ishigame, H., Akitsu, A., Fujikado, N., Kusaka, T., Kubo, S., Chung, S.H., Komatsu, R., Miura, N., Adachi, Y., Ohno, N., Shibuya, K., Yamamoto, N., Kawakami, K., Yamasaki, S., Saito, T., Akira, S., and Iwakura, Y. (2010). Dectin-2 recognition of alpha-mannans and induction of Th17 cell differentiation is essential for host defense against Candida albicans. Immunity 32, 681–691.
Schwarzenberger, P., Huang, W., Ye, P., Oliver, P., Manuel, M., Zhang, Z., Bagby, G., Nelson, S., and Kolls, J.K. (2000). Requirement of Endogenous Stem Cell Factor and Granulocyte-Colony- Stimulating Factor for IL-17-Mediated Granulopoiesis. J. Immunol. 164, 4783–4789.
Schwarzenberger,P. and Kolls,J.K. (2002). Interleukin 17: an example for gene therapy as a tool to study cytokine mediated regulation of hematopoiesis. J. Cell Biochem. Suppl Suppl 38, 88–95.
Schwarzenberger, P., La, R., V, Miller, A., Ye, P., Huang, W., Zieske, A., Nelson, S., Bagby, G.J., Stoltz, D., Mynatt, R.L., Spriggs, M., and Kolls, J.K. (1998). IL-17 stimulates granulopoiesis in mice: use of an alternate, novel gene therapy-derived method for in vivo evaluation of cytokines. J. Immunol. 161, 6383–6389.
Siciliano, N.A., Skinner, J.A., and Yuk, M.H. (2006). Bordetella bronchiseptica modulates macrophage phenotype leading to the inhibition of CD4+ T cell proliferation and the initiation of a Th17 immune response. J. Immunol. 177, 7131–7138.
Siegemund, S. and Alber, G. (2008). Cryptococcus neoformans activates bone marrow-derived conventional dendritic cells rather than plasmacytoid dendritic cells and down-regulates macrophages. FEMS Immunol. Med. Microbiol. 52, 417–427.
Siegemund, S., Schutze, N., Freudenberg, M.A., Lutz, M.B., Straubinger, R.K., and Alber, G. (2007). Production of IL-12, IL-23 and IL-27p28 by bone marrow-derived conventional dendritic cells rather than macrophages after LPS/TLR4-dependent induction by Salmonella Enteritidis. Immunobiology 212, 739–750.
Simonian, P.L., Roark, C.L., Born, W.K., O’Brien, R.L., and Fontenot, A.P. (2009). Gammadelta T cells and Th17 cytokines in hypersensitivity pneumonitis and lung fibrosis. Transl. Res. 154, 222–227.
Stumhofer, J.S., Laurence, A., Wilson, E.H., Huang, E., Tato, C.M., Johnson, L.M., Villarino, A.V., Huang, Q., Yoshimura, A., Sehy, D., Saris, C.J., O’Shea, J.J., Hennighausen, L., Ernst, M., and Hunter, C.A. (2006). Interleukin 27 negatively regulates the development of interleukin 17-producing T helper cells during chronic inflammation of the central nervous system. Nat. Immunol. 7, 937–945.
Sutton, C.E., Lalor, S.J., Sweeney, C.M., Brereton, C.F., Lavelle, E.C., and Mills, K.H. (2009). Interleukin-1 and IL-23 induce innate IL-17 production from gammadelta T cells, amplifying Th17 responses and auto-immunity. Immunity 31, 331–341.
Takatori, H., Kanno, Y., Watford, W.T., Tato, C.M., Weiss, G., Ivanov, I.I., Littman, D.R., and O’Shea, J.J. (2009). Lymphoid tissue inducer-like cells are an innate source of IL-17 and IL-22. J. Exp. Med. 206, 35–41.
Uesugi, T., Froh, M., Arteel, G.E., Bradford, B.U., Gabele, E., Wheeler, M.D., and Thurman, R.G. (2001). Delivery of IkappaB superrepressor gene with adenovirus reduces early alcohol-induced liver injury in rats. Hepatology 34, 1149–1157.
Umemura, M., Yahagi, A., Hamada, S., Begum, M.D., Watanabe, H., Kawakami, K., Suda, T., Sudo, K., Nakae, S., Iwakura, Y., and Matsuzaki, G. (2007). IL-17-mediated regulation of innate and acquired immune response against pulmonary Mycobacterium bovis bacille Calmette-Guerin infection. J. Immunol. 178, 3786–3796.
van Beelen, A.J., Zelinkova, Z., Taanman-Kueter, E.W., Muller, F.J., Hommes, D.W., Zaat, S.A., Kapsenberg, M.L., and de Jong, E.C. (2007). Stimulation of the intracellular bacterial sensor NOD2 programs dendritic cells to promote interleukin-17 production in human memory T cells. Immunity 27, 660–669.
van de Veerdonk, F.L., Marijnissen, R.J., Kullberg, B.J., Koenen, H.J., Cheng, S.C., Joosten, I., Van den Berg, W.B., Williams, D.L., van der Meer, J.W., Joosten, L.A., and Netea, M.G. (2009). The macrophage mannose receptor induces IL-17 in response to Candida albicans. Cell Host. Microbe 5, 329–340.
Werner, J.L., Metz, A.E., Horn, D., Schoeb, T.R., Hewitt, M.M., Schwiebert, L.M., Faro-Trindade, I., Brown, G.D., and Steele,C. (2009). Requisite role for the dectin-1 beta-glucan receptor in pulmonary defense against Aspergillus fumigatus. J. Immunol. 182, 4938–4946.
Wiehler, S. and Proud, D. (2007). Interleukin-17A modulates human airway epithelial responses to human rhinovirus infection. Am. J. Physiol Lung Cell Mol. Physiol 293, L505–L515.
Wolk, K., Witte, E., Witte, K., Warszawska, K., and Sabat, R. (2010). Biology of interleukin-22. Semin. Immunopathol. 32, 17–31.
Wu, Q., Martin, R.J., Rino, J.G., Breed, R., Torres, R.M., and Chu, H.W. (2007). IL-23-dependent IL-17 production is essential in neutrophil recruitment and activity in mouse lung defense against respiratory Mycoplasma pneumoniae infection. Microbes. Infect. 9, 78–86.
Yang, X.O., Pappu, B.P., Nurieva, R., Akimzhanov, A., Kang, H.S., Chung, Y., Ma, L., Shah, B., Panopoulos, A.D., Schluns, K.S., Watowich, S.S., Tian, Q., Jetten, A.M., and Dong, C. (2008). T helper 17 lineage differentiation is programmed by orphan nuclear receptors ROR alpha and ROR gamma. Immunity 28, 29–39.
Yao, Z., Fanslow, W.C., Seldin, M.F., Rousseau, A.-M., Painter, S.L., Comeau, M.R., Cohen, J.I., and Spriggs, M.K. (1995). Herpes virus saimiri encodes a new cytokine, IL-17, which binds to novel cytokine receptor. Immunity 3, 811–821.
Ye, P., Rodriguez, F.H., Kanaly, S., Stocking, K.L., Schurr, J., Schwarzenberger, P., Oliver, P., Huang, W., Zhang, P., Zhang, J., Shellito, J.E., Bagby, G.J., Nelson, S., Charrier, K., Peschon, J.J., and Kolls, J.K. (2001). Requirement of interleukin 17 receptor signaling for lung CXC chemokine and granulocyte colony-stimulating factor expression, neutrophil recruitment, and host defense. J. Exp. Med. 194, 519–527.
Yu, J.J., Ruddy, M.J., Conti, H.R., Boonanantanasarn, K., and Gaffen, S.L. (2008). The interleukin-17 receptor plays a gender-dependent role in host protection against Porphyromonas gingivalis-induced periodontal bone loss. Infect. Immun. 76, 4206–4213.
Zelante, T., De Luca, A., Bonifazi, P., Montagnoli, C., Bozza, S., Moretti, S., Belladonna, M.L., Vacca, C., Conte, C., Mosci, P., Bistoni, F., Puccetti, P., Kastelein, R.A., Kopf, M., and Romani,L. (2007). IL-23 and the Th17 pathway promote inflammation and impair antifungal immune resistance. Eur. J. Immunol. 37, 2695–2706.
Zheng, Y., Danilenko, D.M., Valdez, P., Kasman, I., Eastham-Anderson, J., Wu, J., and Ouyang, W. (2007). Interleukin-22, a T(H)17 cytokine, mediates IL-23-induced dermal inflammation and acanthosis. Nature 445, 648–651.
Zheng, Y., Valdez, P.A., Danilenko, D.M., Hu, Y., Sa, S.M., Gong, Q., Abbas, A.R., Modrusan, Z., Ghilardi, N., De Sauvage, F.J., and Ouyang, W. (2008). Interleukin-22 mediates early host defense against attaching and effacing bacterial pathogens. Nat. Med. 14, 282–289.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Kolls, J.K., Khader, S.A. (2011). TH17 Cytokines in Primary Mucosal Immunity. In: Jiang, S. (eds) TH17 Cells in Health and Disease. Springer, New York, NY. https://doi.org/10.1007/978-1-4419-9371-7_13
Download citation
DOI: https://doi.org/10.1007/978-1-4419-9371-7_13
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4419-9370-0
Online ISBN: 978-1-4419-9371-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)