
Abstract
Mumps has been recognized as a common childhood illness since the time of Hippocrates in the fifth century BC. In 1790, central nervous system involvement was described by Hamilton and, in 1860, sensorineural deafness by Toynebee.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
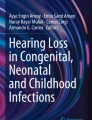
Mumps has been recognized as a common childhood illness since the time of Hippocrates in the fifth century BC. In 1790, central nervous system involvement was described by Hamilton and, in 1860, sensorineural deafness by Toynebee. By the 1940s, mumps was garnering mounting concern as a cause of painful orchitis, aseptic meningitis, and encephalitis that was substantially affecting troop mobilization. Cultivation of the mumps virus in chick embryos in 1945 led to the development of inactivated vaccine, but killed mumps vaccine only induced short-term memory with low efficacy [1, 2]. Subsequently, effective live-attenuated vaccines have been developed. These were introduced into many industrialized countries heralding a major step forward in prevention with annual rates of mumps cases plummeting by 90%. The effect was so dramatic that by 1992, mumps disease was delineated as one of six potentially eradicable diseases by the International Task Force for Disease Eradication [3]. Despite this optimism, indigenous mumps has not disappeared from all countries that have introduced routine mumps vaccine. Indeed, mumps has made a comeback in many countries in the past decade with numerous outbreaks including a very large one in the United Kingdom (Fig. 1) [4], outbreaks in Sweden [5], the Netherlands [6], Canada [7], Australia [8], the United States [9], Belgium [10], and a number of other countries. In contrast, Finland, which lies close to many of these European countries, has not had any recent outbreaks [11, 12].

Mumps notifications in England and Wales: 2004–2009 (Reproduced with permission from Health Protection Report. 2009;3(14) 9 April 2009. Health Protection Agency. http://www.hpa.org.uk.hpr/archives/2009/news1409.htm) [4]
What has gone wrong with the mumps vaccine eradication plan? Why have mumps outbreaks occurred in populations with high rates of mumps vaccine coverage? Why might Finland have been spared so far? What are the lessons learned and how might the control of mumps be improved?
The clinical presentation of mumps, the virus and its pathogenesis, mumps epidemiology, diagnostic tools, and vaccines will be reviewed briefly to provide a background for discussion of the outbreaks, lessons learned, and questions still arising.
2 Mumps: The Clinical Presentation
Mumps illness is generally mild, typically beginning with a prodrome of nonspecific symptoms including low-grade fever, headache, malaise, and myalgia [13, 14]. However, up to 20% of infections are asymptomatic. The well-recognized parotid gland swelling (either unilateral or bilateral) occurs in only 30–40% of cases while 40–50% of patients may have respiratory symptoms, particularly children younger than 5 years of age who may develop lower respiratory illnesses. Parotid gland swelling is more common in school-aged children with parotitis occurring in 60–70%, with submandibular swelling in 10% and suprasternal swelling in 6% (See Fig. 2) but can occur, albeit rarely, in infants [15]. As shown in Table 1, mumps infection is often associated with complications [13, 14]. The rates of complications such as orchitis, oophoritis, and encephalitis increase with age and are more prominent in adults [9]. Previous estimates of sensorineural hearing loss may have been on the low side at 0.5–5/100,000 [13] given that a more recent prospective office-based study in Japan, a country where mumps vaccine is not used, found a rate of severe mumps hearing loss of 1/1,000 [16]. Mumps infection in pregnancy appears to increase embryonic and fetal death and spontaneous abortion but the mumps virus does not appear to be teratogenic [19]. There might be a relationship between mumps in pregnancy and endocardial fibroelastosis but data are limited. Little is known about mumps in immunocompromised patients, although mumps has been recently reported as a cause of kidney rejection in an adult renal transplant patient [17]. Hospitalizations due to mumps are uncommon [9] and death from mumps is rare, occurring in only about one to three cases per 10,000, usually due to encephalitis [13].

Child with mumps (Courtesy of CDC/NIP/Barbara Rice. Public Health Image Library. Centers for Disease Control and Prevention. http://www.cdc.gov/vaccines/vpd-vac/mumps/photos.htm)
3 Mumps: The Virus
Mumps virus is an enveloped, negative-strand RNA virus in the family Paramyxoviridae, genus Rubulavirus (Fig. 3) and is a close cousin of human Parainfluenza virus [18]. The mumps genome encodes for eight proteins including two glycoproteins: hemagglutinin-neuraminidase (HN) and fusion protein (F); five other structural proteins: nucleocapsid (NP), phosphoprotein (P), large polymerase protein (L), matrix protein (M), and small hydrophobic (SH) protein; and two nonstructural proteins V and I encoded within the P protein gene [20]. No single gene mutation appears to be wholly responsible for the overall virulence of a specific mumps strain but rather requires gene mutations leading to changes in several proteins [21]. While monkeys were originally used for testing neurovirulence, a neonatal rat-based assay has now been developed [22].

Negative stained transmission electron micrograph depicting the ultrastructural features displayed by the mumps virus (Courtesy of CDC/ Dr. F. A. Murphy. Public Health Image Library. Centers for Disease Control and Prevention. http://www.cdc.gov/vaccines/vpd-vac/mumps/photos.htm)
Prior to the development of monoclonal antibodies, mumps was declared to be serologically monotypic. However, mumps is now recognized to have multiple genotypes with 12 detected to date based upon variation in the SH gene, the most variable gene in mumps with intra-genomic variation of 2–4% and inter-genomic variation ≥ 6% [20, 23]. Although the SH gene does not play a role in protective immunity, sequence variation in this gene reflects the virus’ overall genetic and antigenic variability, including the HN gene that codes for the major target of neutralizing antibody [24].
The NP protein is the antigen (S antigen) used in the IgM assays for acute infection while the F and HN proteins are known to be important for inducing protective antibody. To further complicate serological testing, due to some homology between mumps virus F and HN proteins with those of other paramyxoviruses, some serologic cross-reactivity can occur [18].
The mumps virus can replicate in a variety of cell tissue cultures such as primary rhesus monkey kidney cells and HeLa cells as well as in embryonated hens’ eggs. In tissue culture, the cytopathic effect is indistinguishable from that of respiratory syncytial virus. Given that mumps has an envelop, it is sensitive to ether. Mumps virus is stable at 4°C for several days, and can be kept at –65°C for years but is sensitive to repeated thawing and freezing.
4 Mumps: The Pathogenesis and Transmission
Mumps is a respiratory infection transmitted through close contact by inhalation of infectious droplet nuclei, by direct contact, or by autoinoculation after hands contact virus-contaminated fomites and touch the nose or mouth. Infection can remain localized in the respiratory tract but viremia frequently occurs, usually late in the incubation period [25, 26]. Spread within the body can also occur through infected mononuclear cells. The virus has a predilection for glandular (e.g., parotid glands, ovaries, testes, and pancreas) and nerve tissue [14]. The virus enters the central nervous system through the vasculature of the choroid plexus [18]. The incubation period for mumps is 14–18 days but maybe as long as 25 days. Based upon studies of household contacts, mumps is less infectious than measles or varicella [27]. The period of peak contagion is from 3 days prior to the onset of symptoms until 5 days afterwards [20]. However, the mumps virus can be isolated from saliva from as early as 7 days before to 9 days after onset of clinical symptoms [14]. Those with subclinical infection can spread the virus while the respiratory tract and salivary glands are involved. Salivary secretion of virus correlates inversely with local virus-specific IgA secretory antibody levels [25, 26]. With respect to prevention, mumps virus is most accessible and susceptible to immune attack during the period of viremia when it is cell free [18]. Humoral antibodies appear to restrict plasma viremia. The role that cell-mediated immunity plays is not well understood.
5 Mumps: The Diagnosis
The clinical diagnosis of mumps rests upon the standard case definition: acute onset of unilateral or bilateral swelling of the parotid or other salivary glands lasting 2 or more days without any other apparent cause [28]. This will miss cases where parotid gland swelling either is not prominent or does not occur. Use of the clinical diagnosis is most effective in countries without routine mumps immunization programs where outbreaks regularly occur but is more problematic for sporadic cases or in countries where mumps vaccine is widely used. Similar presentations (parotid swelling and low-grade fever) can occur in infections with other viruses such as Epstein-Barr, parainfluenza types 1, 2, or 3, adenovirus, Human herpesvirus 6, enteroviruses, influenza A, and lymphocytic choriomeningitis virus [29–31]. In a study in Alberta, Canada, before the introduction of mumps vaccine, about one-third of cases of sporadic mumps reported by family physicians could not be confirmed by serology suggesting that causes other than mumps to be the etiology [32]. A further problem in countries with routine mumps immunization programs is that mumps may be misdiagnosed or missed completely due to lack of clinical familiarity with the presentation of mumps in different age groups and the expectation that all cases have parotitis.
5.1 Mumps: Laboratory Diagnosis for Mumps Infection
Laboratory-confirmed mumps is defined by the United States Centers for Disease Control and Prevention and the Public Health Agency of Canada as a patient with clinical symptoms compatible with mumps who has positive mumps IgM antibody (without previous immunization in the last 6 weeks), or seroconversion as defined by a fourfold rise in IgG titer to mumps, or isolation of mumps virus, or detection of mumps RNA in saliva, urine, or CSF [33]. However, laboratory confirmation of mumps infection can be difficult, particularly in recent outbreaks that have affected partially immune populations.
5.1.1 Specimen Collection
As with any other diagnostic test, the accuracy of the results will be influenced by the type of specimen collected, the timing of specimen collection, and the conditions under which the specimen is transported to the laboratory. As indicated previously, mumps virus can be detected for 5 days after the onset of symptoms in buccal specimens and up to 13 days in urine specimens in non-vaccinated individuals [34]. Buccal swabs are the ideal specimen for the diagnosis of acute mumps infection and generally have a higher sensitivity than urine [35, 36]. To collect a buccal sample, the patient should first have their parotid gland massaged to express infected saliva. A swab should be rubbed along the buccal mucosa near stenson’s duct, placed in appropriate viral transport media and shipped to the laboratory at 4°C [37] (Fig. 4). Due to the labile nature of the virus, the specimen should not be frozen at –20°C.

Collection of buccal specimen for detection of mumps virus by culture and polymerase chain reaction (PCR). Swab the buccal cavity, i.e, the space near the upper rear molars between the cheek and the teeth. Swab the area between the cheek and gum by sweeping the swab near the upper molar to the lower molar area (adapted from the Illinois Dept. of Public Health – Div. of Laboratories (Chicago Virology Section) Courtesy of CDC http://www.cdc.gov/vaccines/vpd-vac/mumps/downloads/detection_IL.pdf)
5.1.2 Tissue Culture
The mumps virus can replicate in a variety of cell tissue cultures such as primary rhesus monkey kidney cells, HeLa cells, Vero cells, human neonatal kidney cells, as well as in embryonated hens’ eggs. In tissue culture, the cytopathic effect usually occurs 6–8 days post-inoculation and is characterized by the formation of syncycia which may be indistinguishable from that of respiratory syncytial virus. Confirmation of a positive culture is done using mumps-specific immunofluorescence. Methods using centrifugation enhanced inoculation of shell vial tissue cultures offer more rapid results (2–5 days) than traditional culture [38]. Mumps virus is stable at 4°C for several days and can be kept at –70°C for years but is sensitive to repeated thawing and freezing [34, 39].
5.1.3 Molecular Testing
Nucleic acid-based tests (NAT), such as reverse transcriptase PCR, have been developed to detect mumps virus in clinical samples. Both conventional hemi-nested RT-PCR and real-time RT-PCR methods directed at the SH and F genes have been validated for clinical use [39–42]. NAT methods are more rapid and can generate a result in 4–8 h compared to 5 days for tissue culture. In addition, NAT has superior sensitivity compared to culture. The sensitivity of culture for identification of mumps from oral specimens collected from patients with suspect mumps is 73% compared to real-time RT-PCR methods [35, 39]. NAT methods have the ability to detect as little as 0.01 TCID50 of virus or ten copies of RNA [34, 41, 43]. Faster turnaround time to results (often in as little as 4 h), reduced potential for amplicon contamination, and in some cases further enhancement of sensitivity, are all advantages to real-time methods compared to the conventional nested RT-PCR. As these molecular methods become more common, and protocols become more standardized, NAT methods will likely become the new standard in the diagnosis of acute mumps infection.
5.1.4 IgM Serology
The identification of an IgM response to a specific pathogen is often used as a way to diagnose acute infection. However, experience with the use of IgM-specific serology in the most recent mumps outbreaks in North America and the United Kingdom suggest that IgM serology is a very insensitive test. Studies from Canada and Europe demonstrated that the sensitivity of different commercially available kits for the detection of IgM antibodies to the mumps virus ranged from 24 to 51% [36, 44]. Why these assays perform poorly is likely a reflection of the population being tested. These assays were originally developed to test the primary immune response individuals without pre-existing immunity to mumps. In the recent North American outbreaks many of the cases had only received a single dose of mumps-containing vaccine or had two doses with waning immunity [24]. This partial immunity did not prevent re-infection but could alter the natural history of the immune response where the IgM response is blunted and below the limit of detection of the commercially available assays.
5.1.5 IgG Serology
Many commercial assays are available to document the presence of anti-mumps IgG in patients’ specimens. A positive result is often used as a surrogate marker of immunity. However, data from the United States have shown that many of those infected with mumps in the recent outbreak had two doses of MMR and IgG antibodies at the time of presentation, which questions whether these assays are a reliable measure of immunity [45].
The serologic response to mumps can be measured using neutralization assays, hemagglutination inhibition (HI) assays, and enzyme immunoassays (EIA); however, there is poor correlation between these different methods [46]. When a person is exposed to a live virus (wild or attenuated vaccine strains), both neutralizing and non-neutralizing antibodies are generated. Antibody titers are commonly measured using commercial EIAs which are simple to perform compared to the more technically demanding neutralization assays. However, these EIA methods do not distinguish between neutralizing and non-neutralizing antibodies. The gold standard method of testing for protective immunity is to measure neutralizing antibodies by a neutralization assay. In this assay a patient’s serum is mixed with a known concentration mumps virus and put on a cell line that is permissive to infection with the mumps virus. If there are antibodies in the patients serum that are effective at preventing infection, they will bind to the mumps virus and “neutralize” it so that the cell line does not get infected [47].
Unlike measles and rubella in which a protective titer has been established using an internationally recognized reference standard, no such benchmark exists for mumps, making determination of who is truly immune difficult.
Documentation of a fourfold rise in IgG titer is also a criterion for laboratory confirmation. However, this rise may be difficult to document in infected individuals who have had previous vaccination. The purpose of vaccination is to prime the immune response to respond rapidly to a pathogen. The IgG response in these individuals may be so rapid that a fourfold rise could be missed.
The laboratory confirmation of mumps infection can be challenging, particularly in a partially immunized population. Although newer molecular detection methods such as real-time reverse transcriptase PCR are becoming the standard in mumps diagnostics, no diagnostic testing is 100% sensitive, and as such mumps infection cannot be absolutely ruled out by a negative diagnostic test, particularly in a partially immunized population [48].
6 Mumps: The Epidemiology
Mumps occurs worldwide but only in humans; there are no natural animal reservoirs. A carrier state is not known to exist in humans and mumps infection is thought to confer lifelong immunity. In the pre-vaccine era, more than 50% of reported cases of mumps were in children aged 5–9 years, and over 90% of reported cases were in those under 14 years of age. This may have been related both to the ease of spread in this age group and to the high frequency of clinically apparent parotitis, and thus increased probability of considering the diagnosis. Within a household, the secondary attack rate is estimated to be 80–90%. Mumps is uncommon in infants under one year of age likely due to the presence of maternal antibodies as well as limited exposure if both parents are immune either through natural infection or through childhood immunization.
Mumps commonly occurs in the winter and spring in temperate climates but does not show seasonality in tropical climes [18]. In countries without routine mumps immunization programs, mumps epidemics occur approximately every 3–4 years. Mumps rates vary by country with an average of 300/100,000 in countries without immunization programs [18]; however, the rates have dropped dramatically in countries where routine mumps immunization has been introduced as shown in Table 2 [13, 18]. While single-dose routine programs led to a marked decrease in cases, two-dose programs were even more effective (Table 2).
By 2000, mumps appeared to be well controlled in many countries with routine mumps immunization programs such as the United Kingdom, the United States, Canada, and Australia. However, in the past 5 years, each of these countries has experienced major outbreaks predominately in older adolescents and young adults but not in young age children as occurs in countries without immunization programs [7–9, 49]. These outbreaks were unexpected and have raised concerns about the effectiveness of mumps vaccine and mumps vaccine programs.
Mumps virus, based upon SH region variation, shows distinct geographic clustering by genotype and redistribution may occur over time [50]. More than one genotype may circulate simultaneously in a geographic region. In the Western Hemispheres, genotypes C, D, E, G, and H predominate while in Asia, genotypes B, F, and I are more common [14]. The mumps strains that caused the outbreaks in the United Kingdom, United States, and Canada were G and all related genetically [7] and different from the genotype A found in Jeryl Lynn vaccine.
7 Mumps: The Vaccines
Although effective live-attenuated mumps vaccines have been available for more than 30 years [18], use has not been widespread until recently. By 2007, 114 countries, plus parts of China, had introduced mumps vaccine. All commercially available mumps vaccines contain live-attenuated mumps virus that is lyophilized and must be reconstituted before use. Mumps vaccines may be monovalent but more often are given in combination with measles and rubella vaccine (MMR) or, more recently, with added varicella vaccine (MMR-V).
At present, there are at least 11 different attenuated mumps vaccine strains in use throughout the world, but only Jeryl Lynn (developed in the United States), UrabeAm9 (developed in Japan), and Leningrad-3 (developed in the former Soviet Union) and their derivatives (RIT 4385: viral clone of Jeryl Lynn; Leningrad–Zabreg: further attenuated Leningrad-3) are used widely [14, 51]. Vaccine preparations using the attenuated parent vaccine strain may differ by manufacturer because of differences in passage history, cell substrates, or manufacturing processes [52]. The currently used attenuated vaccine strains belong to different genotypes, i.e., Jeryl Lynn genotype A and Urabe Am9 genotype B [50]. Each of the vaccines also differs in their immunogenicity, efficacy, effectiveness, and associated adverse events. For example, Urabe Am9 has been associated with enhanced neurovirulence compared to Jeryl Lynn, while Jeryl Lynn (genotype A) has been shown to have reduced cross-neutralization capacity with genotype D [24, 50].
Mumps vaccines are considered very safe. In large field trials before licensure, no serious adverse events were reported with the Jeryl Lynn vaccine [53]. Overall, adverse reactions to mumps vaccination are uncommon and usually mild, i.e., slight injection site local soreness and swelling; occasionally mild parotitis and low-grade fever may occur. More serious adverse events such as sensorineural deafness have been reported albeit at a reporting rate of one case per 6–8 million doses of mumps vaccine with causality not fully established [54]. The more common serious adverse event attributable to mumps vaccine is aseptic meningitis reported at widely varying frequencies as high as one case per 1,000 vaccinations (Leningrad-3 and Urabe Am-9) to as low as 1/1,800,000 vaccinations (Jeryl Lynn) [51, 52]. Causality has been proven through isolation of the vaccine mumps strain from the cerebrospinal fluid. The difference in frequency of vaccine-associated aseptic meningitis reflects both differences in vaccine strains and vaccine preparation, as well as variation in study design, diagnostic criteria, and clinical practice [51, 52]. As with wild mumps, asymptomatic pleocytosis in the cerebrospinal fluid may occur. Of note, there are reports of horizontal transmission of mumps vaccine virus (Leningrad-Zagreb and Leningrad-3) to family contacts [55–57].
Mumps vaccines are immunogenic but less so than natural disease; with Jeryl Lynn, the mean neutralizing titers in children are 1:9 vs. 1:60 with natural disease [58]. There is variation in immunogenicity by strain. Urabe not only has a higher rate of aseptic meningitis than does Jeryl Lynn [59], but also has consistently reported higher seroconversion rates although both are very immunogenic [51]. Antibodies persist for at least 10 years after immunization with two doses being more effective than one, but immunity does wane significantly over time [18, 60]. Based upon titers, there does not seem to be any advantage to delaying the second dose from 4–6 to 9–11 years [60]. Antibodies appear to decline more quickly with Jeryl Lynn than with Urabe. In a study in the United Kingdom, 4 years after receipt of MMR, the rate of seronegativity was 19% with Jeryl Lynn compared to 15% with Urabe [61]. In a study from Finland, 21 years after last dose of MMR, 24% had no measurable mumps antibody using enzymoimmunoassay [62]; however, given that there are no accepted surrogate serological markers for protection, extrapolation of these immunogenicity studies to the real world is difficult. Cellular immunity may also be important. Of note, all (n=14) of the seronegative group noted above in the Finnish study had evidence of cell-mediated immunity (mumps antigen-specific lymphoproliferative responses) and only one of the seropositive vaccinees (n=36) had none after 20 years. This suggests that cell-mediated immunity may persist for a very long time but the clinical importance of this is still unclear [63].
With respect to efficacy, most trials done in the 1960s and 1970s were short-term only and showed efficacy for Jeryl Lynn of 95–96% and for Leningrad-3 of 91–99% [18]. However, studies of effectiveness in outbreaks have noted consistently lower ranges (61–91% for Jeryl Lynn and Urabe) [18, 64, 65]. Of note, Leningrad–Zagreb vaccine, at only a fraction of the cost of Jeryl Lynn vaccine, has been shown to be very effective – 95% in one study [66]. Single-dose vaccine is only effective in decreasing mumps by 80–90%: for elimination, two doses are a must [13]. Furthermore, very high coverage rates are needed (first dose >95% and second dose ≥80%) to interrupt indigenous mumps transmission in a country [67]. Low to moderate levels of mumps vaccine coverage may actually increase the number of susceptibles and the number of cases in older age groups.
8 Mumps: Recent Resurgence
Mumps has made a resurgence in a number of countries in the past 5–10 years. Outbreaks in countries that previously had reported good mumps control, such as the United States, Australia, and Canada, are especially concerning. In each of the outbreaks, the clinical presentation of mumps whether in an immunized or a non-immunized cohort has not differed from that described earlier [7, 65]. Parotitis, orchitis, aseptic meningitis, pancreatitis, and encephalitis have all occurred [68]. The hospitalization rates have remained low with only 85 patients out of 6584 (<2%) hospitalized in the 2006 outbreak in the United States [9]. Deaths have not been reported [7–9, 69]. The epidemiology and underlying contributing factors differ in these outbreaks with some due to vaccine program problems while others suggest vaccine problems. Five patterns are seen (Table 3).
8.1 Vaccine Program: Refusal to Accept Immunization: 2007–2008 Outbreak in the Netherlands
In the Netherlands, mumps vaccination using Jeryl Lynn was introduced in 1987. The routine childhood immunization program includes mumps vaccine as part of MMR at 14 months and a second dose at 9 years. This regimen appeared to be bringing mumps under good control leading to fewer than 50 cases reported each year and dropping to less than 10 cases per year by 2005 [8], although there was an outbreak in an international school in 2004 [6] with a 12% attack rate among students immunized according to the Dutch schedule. In 2007, 87 cases of mumps were reported in less than a year; median age 13 years (range 2–56 years) [6]. The geographic distribution coincided with areas with low immunization rates (Fig. 5a, b). Of the 87 cases, only 29 were vaccinated. Mumps may have occurred due to the reduced cross-neutralization capacity of Jeryl Lynn for Group D [8, 70], the most frequently isolated genotype in this outbreak. In the 58 who were unvaccinated, the main reason given in 36 was religion – Orthodox Reformed Christians. The geographic distribution of cases coincided with the “Bible belt.” Even with high rates of immunization in surrounding areas (90–95% vaccine coverage) [70], mumps still readily infected the non-immunized population with some spread to the immunized. Herd immunity did not protect the non-immune population. Similar outbreaks in non-immunized populations within well-immunized communities have occurred elsewhere [71].

a Geographical distribution of notified mumps cases in the Netherlands from August 1, 2007 to May 15, 2008 [6]. b Geographical distribution of measles–mumps–rubella vaccination coverage by municipality at the age of 2 years in the Netherlands, 2008 [6]. Source: Centre for Infectious Disease Control, Rijkinstituut voor Volksgenzonheid en Milieu (RIVM), The Netherlands. With permission Eurosurveillance
8.2 Vaccine Program: Failure to Immunize an Age Group: “Lost Cohort”: 2004–2006 Outbreak in United Kingdom
Routine immunization for mumps was introduced into the United Kingdom in 1988 as MMR vaccine. The vaccine was recommended for children 12–15 months of age. Cases of mumps declined as did mumps hospitalizations [72]. Initial modeling done at that time suggested that the critical level of mumps vaccine uptake needed to eliminate transmission of mumps was approximately 85% of each cohort by the age of 2 years [73]. Both Jeryl Lynn and Urabe Am-9 vaccine strains were used until the early 1990s when the decision was made to no longer purchase Urabe Am-9 [74] due to concerns about the associated high rates of aseptic meningitis [59]. In 1994, an outbreak of measles prompted a national catch-up campaign for 5- to 16-year olds, but due to a world shortage of MMR, measles–rubella vaccine was used [75]. Modeling of efficacy data for mumps vaccine at that time indicated that mumps was unlikely to be eliminated with a single-dose program [72] so this led to the introduction of a two-dose MMR childhood regimen in 1996. Of note, by 1999, cases of mumps in adolescents began to rise [76] although major outbreaks were not occurring. A catch-up MMR campaign was started in early 2004 primarily aimed at those older than 19 years [49], but this is a difficult age group to reach [49, 77].
During 2004–2006, the United Kingdom experienced a major nationwide outbreak of mumps with over 50,000 cases reported in 2005. As shown in Fig. 6, the majority of cases represented a “lost cohort” – too young to have had natural disease at school when mumps was spreading widely, too old when routine MMR vaccine was introduced in 1988 (no catch-up), no mumps vaccine in the MR catch-up program in 1994, and too old for the two-dose program that started in 1996 [76]. In 2004, almost 79% of the confirmed cases were persons 15–24 years of age and only 3.3% reported having received two doses of vaccine and another 30% had received one dose only [75]. By 2005, most of the cases were 19- to 23-year olds in college or universities [75]. Although mumps vaccine (MMR) uptake had been declining in the England since 2000 following adverse publicity about possible (since discredited) links to autism and Crohn’s disease [78], this was not the cause of this large outbreak as only 2.4% of the confirmed mumps cases in 2004 were in persons who would have been eligible for two doses of MMR [75]. The vaccine effectiveness in this large outbreak was estimated to be 87.8% for one dose and 94.6% for two doses of vaccine [79].

For England and Wales, confirmed mumps cases in 2004 by year of birth (1970–2001) per 100,000 population and opportunity for MMR vaccination [76]. Reproduced from (Mumps outbreaks across England and Wales in 2004: observational study. Savage E, Ramsay M, White J, Beard S, Lawson H, Hunjan R, et al. BMJ 330(7500):1119–20 copyright notice 2005) with permission from BMJ Publishing Group
This was not an outbreak primarily due to vaccine failure but rather an outbreak due to vaccine program failure to fully immunize a cohort resulting in a “lost cohort.” Furthermore, given that not all members of this lost cohort had mumps during this outbreak, the potential continues for more mumps cases to occur in adults as this “lost cohort” ages. Given that mumps continues to be a problem in some European Union countries where endemo-epidemics continue [68, 80], the potential for further mumps outbreaks in the United Kingdom remains. This “lost cohort” shows that a susceptible group who are not fully immunized nor exposed to mumps as children can fuel a huge outbreak when mumps is introduced.
Besides the “lost cohort” in these large United Kingdom outbreaks, there was also evidence that waning immunity may have played a role [79]. Of the over 300 cases reported in children in 2004–2005, close to 17% had received one dose of MMR and 31% two doses. Vaccine effectiveness was 88% for one dose and 95% for two doses but the effectiveness of one dose declined from 96% in 2-year olds to 66% in 11- to 12-year olds while the effectiveness of two doses declined from 99% in 5- to 6-year olds to 86% in 11- to 12-year olds [79]. This illustrates that these outbreaks have multi-factorial underpinnings albeit with one major factor – the “lost cohort” – predominating.
8.3 Vaccine Program: Single Dose: Forgotten Cohort 2004–2007 Outbreaks in Canada, 2005–2007 in Australia
In both Canada and Australia, mumps vaccine (Jeryl Lynn or a derivative) has been given routinely (MMR) for 30 years or so, with two-dose MMR regimens introduced in Canada in the mid 1990s (second dose at age 18 months or at 4–5 years of age depending upon the province) and in Australia in 1994 for children aged 10–16 years [7, 8]. In both countries, mumps outbreaks occurred in the past 5 years (2004–2007 in Canada; 2005–2007 in Australia). In Canada, the major outbreaks, involving over 1,200 cases, occurred in 2007 initially in Nova Scotia and then in Alberta (Fig. 7) [81]. Young adults were especially prominent with 58% of the cases occurring in those 20–29 years of age and 5% in those 30–39 years of age [81]. This age group represents a “forgotten cohort” in Canada. Those over 40 years of age at the time were likely immune to mumps due to natural exposure and infection as children. Those aged 12–17 years of age and younger in 2007 had received two doses of MMR vaccine due to the introduction of a second dose of measles–mumps–rubella (MMR) vaccine for measles control in 1996–1997 in most provinces and territories. This left the “forgotten” cohort – those born predominately between 1970 and 1990 who had only received one dose of MMR vaccine [81]. The outbreak in Australia followed an eerily similar pattern – 41% of cases in young adults aged 20–29 years of age with cases concentrated in the birth cohort 1978–1982 [8]. This age group was too old for the two-dose program and too young for natural immunity through mumps infection as a child – a “forgotten cohort” again. Of note, in Canada the genotype of the mumps virus was G, similar to the wild mumps virus causing the major outbreak in the United Kingdom, suggesting spread from there [7]. The outbreaks in the “forgotten – only one dose – cohorts” in both Canada and Australia emphasize the earlier observations that a single dose of mumps vaccine in early childhood is not effective in eliminating endemic mumps in a country [13] as some remain susceptible due to waning immunity, as has been noted in the United Kingdom outbreaks discussed above [79].

Mumps outbreaks in Canada by province in 2007 [81] (Courtesy of Public Health Agency of Canada. © Public Health Agency of Canada, 2009 http://www.phac-aspc.gc.ca/mumps-oreillons/prof-eng.php)
The young adults in these forgotten cohorts form an especially vulnerable group for mumps due to their very social and mobile lifestyles [77, 81]. They have limited interest in adhering to isolation procedures or participating in immunization catch-up programs, frequently share living accommodations, have large social networks (bars/pubs/nightclubs and sports) where secretions can easily be spread, as well as having a penchant for travel during college holidays and breaks where mumps can be picked up and brought back to campus or their workplace. The fairly long infectious period (up to 16 days), long incubation period (14–25 days), and high rate of asymptomatic illness make mumps an ideal microbe to spread in this age group if they are not well protected by immunization. Additional cases in this demographic group and possibly in other jurisdictions where forgotten cohorts exist would not be unexpected.
8.4 Vaccine Failure: Primary Vaccine Failure: Ineffective Vaccine – Rubini
Outbreaks of mumps in countries where Rubini vaccine was used provide excellent examples of primary mumps vaccine failure. Although a very safe vaccine, it has very low or no clinical efficacy. In Singapore, three different MMR vaccines were used since 1990 – Jeryl Lynn, Urabe, and Rubini. Disease surveillance showed that despite a robust two-dose MMR program, mumps cases continued to occur, mainly in children under 15 years of age (61% of the cases) [82]. Where known, almost 74% had received Rubini vaccine, 21% Jeryl Lynn, and 5% Urabe. The vaccine efficacy was –55.3% (yes minus) for Rubini [83]. Similar poor outcomes with Rubini vaccine have been shown in Switzerland with no evidence of protection compared to 70% effectiveness of Jeryl Lynn [84]. A review of the literature by Dayan and Rubin noted vaccine effectiveness for Rubini of 0–33% [24]. The outbreaks in these two countries were noticeably in younger populations with clear evidence of primary vaccine failure. Given that not every child who has received Rubini has now received two doses of a more effective vaccine, countries where Rubini has been used have an aging cohort where further outbreaks of mumps may occur.
8.5 Vaccine Failure: Two-dose Vaccine Failure: Waning Immunity: 2006 Outbreaks in the United States
The large mumps outbreak in the United States provides yet another pattern. In the 2006 outbreaks, 85% of the mumps cases lived in eight contiguous states in the Midwest and over 80% were enrolled in college [9]. Overall, 63 and 84% of those between 18 and 24 years of age had received two doses of mumps vaccine. These were neither “lost cohort” (no vaccine) nor “forgotten cohort” (one dose only) outbreaks as had occurred in the United Kingdom and in Canada and Australia. The high two-dose mumps vaccine coverage did protect many students in these Midwest outbreaks, as shown by the relatively low secondary attack rate for clinical mumps in roommates of only 2.2–7.7% [85]. As in the Canadian and Australian outbreaks, the age and college lifestyle of those most affected may have contributed to fueling the outbreaks [20].
The waning immunity noted to have played a factor in contributing to the rise of mumps in children during the United Kingdom outbreak [79] may also have been at play in these Midwest outbreaks [20, 65]. Support for this hypothesis comes from the observation that, compared to roommates without mumps, those with mumps were more likely to have received their second dose of MMR more than 10 years earlier [85]. Antibody induced by the Jeryl Lynn mumps vaccine was able to effectively neutralize this wild genotype G strain of mumps [86], albeit the geometric mean titers were only about one-half of those against the vaccine strain. While the G genotype did have antigenic differences, these were not so great as to make the antibody response from Jeryl Lynn ineffective. Earlier studies in Japan have shown that secondary vaccine failures in school children with exposure to wild mumps may be due to lower avidity antibody [87].
9 Mumps Elimination in Finland
While many countries have experienced a recrudescence of mumps in the past decade after periods of good control with two-dose regimens, Finland has a more than 25 year history of nationwide elimination of mumps [11] with the most recent outbreak occurring in 1987–1988 [88]. While incidental cases have occurred in the past 10 years (two to eight cases per year in 2003–2007), these have been predominately in non-immunized people and have not led to outbreaks [11]. Many cases had a connection to a foreign country often where epidemics were occurring. Only limited secondary vaccine failures were seen: of seven of 22 mumps cases, three cases had had one dose while four cases had had two doses, all with Jeryl Lynn [11]. Of note, when Finland undertook its program to eliminate indigenous mumps, it ensured that not only did children receive vaccine, but also young adults in schools and in the military. The attention to this age group and long-standing programs that ensure very high rates of MMR uptake (over 95%) means that neither a lost nor a forgotten cohort is present in Finland. This rate of uptake also far exceeds the uptake rates in the United States. However, Finland may be at risk for outbreaks given the potential for importation of mumps from countries where mumps is endemic combined with evidence of waning antibodies and no endemic mumps to boost response [11]. The clinical relevance of the demonstrated continued cell-mediated immunity in those who are antibody negative remains to be seen. Perhaps this will be protective.
10 Mumps: Public Health Control Strategies in Outbreaks
Public health units have employed a variety of strategies to limit the spread of mumps once an outbreak is occurring. Table 4 summarizes similarities and differences in isolation strategies used in Canada, the United Kingdom, and the United States [9, 75, 81, 89, 90]. Of note, the data to support these differences are limited and suggest that more work needs to be done to evaluate the effectiveness and cost of these strategies.
11 Mumps Outbreaks: Lessons Learned
There are many important lessons to be learned from these mumps outbreaks. In countries where mumps is uncommon, health-care providers may need reminders of how mumps can present in different age groups. These outbreaks have shown that single-dose mumps vaccine programs are inadequate for the control of endemic mumps. Even with two-dose programs, very high rates of uptake are required (95% first dose; >80% second dose) if control is to be established. Herd immunity will not protect non-immunized pockets. Incomplete and low immunization rates among older adolescents and young adults can lead to large outbreaks. This is an age group where mumps can be easily spread and can be hard to control. Waning immunity, as measured by antibody titers, may be an underlying factor in mumps outbreaks in fairly well-immunized groups. The role of persistent cell-mediated immunity in long-term protection from mumps is unknown. Mumps vaccines vary in terms of adverse event rates and effectiveness. Leningrad-3, which is only a fraction of the cost of Jeryl Lynn [3, 91], is not only associated with more aseptic meningitis but also has higher effectiveness. Reliable laboratory diagnostic tests for mumps in a highly immunized population beyond detection by culture or PCR are needed. Lastly, these outbreaks suggest that long-term control of mumps with two doses of vaccine given in early childhood may not lead to control even with very high uptake rates if cell-mediated immunity and not antibody is the key to long-term protection. Additional booster doses may need to be considered in the future. This leads to the conclusion that ongoing surveillance for mumps is crucial as is further research into control.
12 Mumps Control: Unanswered Questions
A number of unanswered questions arise from observation of these outbreaks.
-
How does mumps behave in a population with very high immunization rates over the long term? What will happen over time in Finland?
-
Does eliminating cases of mumps in childhood through infant and preschool immunization lead to an increased number of older susceptible adults due to waning immunity and missed immunizations?
-
Will booster doses of mumps vaccine be needed in older youth or young adults immunized in early childhood? If so, what vaccine would be best?
-
Given the effectiveness and cost of Leningrad-3, is it time to reassess its use against Jeryl Lynn despite its rate of aseptic meningitis?
-
Why has mumps now disappeared in Canada, Australia, and the United States?
-
Does enzyme immunoassay correlate well with measured neutralizing antibodies?
-
How do we measure protection against mumps? What level of antibody is protective? Is testing for cell-mediated immunity required to determine protection?
-
What are the best strategies for controlling mumps in developing and developed countries that have no or poor mumps immunization programs? How can barriers to mumps vaccine be overcome?
-
As the mumps viruses causing outbreaks change, do the vaccines need to change?
-
Are catch-up programs needed for the lost and forgotten cohorts as well as those who have been immunized with ineffective vaccines such as Rubini?
-
What are effective public health strategies for dealing with outbreaks of vaccine preventable disease like mumps in older youths and young adults?
13 Summary
This decade has seen an unprecedented resurgence of mumps in countries where mumps had previously been well controlled. The factors contributing to these mumps outbreaks have included vaccine program failures including failure to accept immunization by a select group, failure to immunize a cohort, and failure to provide a second dose to a cohort, as well as examples of primary and secondary vaccine failures. The Finnish data suggesting that for good control first dose uptake rates of 95% and second dose uptake rates of over 80% are required are sobering. Many industrialized countries have past uptake rates below this and in some, recent MMR uptake has fallen [78, 92] leaving a wider swath at risk for mumps. Mumps outbreaks are highly likely to re-occur. Mumps is indeed back.
References
Habel K. Vaccination of human beings against mumps; vaccine administered at the start of an epidemic. I. Incidence and severity of mumps in vaccinated and control groups. Am J Hyg. 1951;54(3):295–311.
World Health Organization. Mumps virus vaccines. Wkly Epidemiol Rec. 2007;82(7):51-60.
Fullerton KE, Reef SE. Commentary Ongoing debate over the safety of the different mumps vaccine strains impacts mumps disease control. Int J Epidemiol. 2002;31(5):983–4.
Health Protection Agency. Continued increase in mumps in universities 2008/2009 News; 2009 April. http://www.hpa.org.uk/hpr/archives/2009/news1409.htm
Sartorius B, Penttinen P, Nilsson J, Johansen K, Jonsson K, Arneborn M et al. An outbreak of mumps in Sweden, Feb–Apr 2004. Euro Surveill. 2005;10(9):191–3. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=559.
Karagiannis I, van Lier A, van Binnendijk R, Ruijs H, Ruijs H, Fanoy E et al. Mumps in a community with low vaccination coverage in the Netherlands. Euro Surveill. 2008;13(24). http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=18901.
Watson-Creed G, Saunders A, Scott J, Lowe L, Pettipas J, Hatchette TF. Two successive outbreaks of mumps in Nova Scotia among vaccinated adolescents and young adults. CMAJ. 2006;175(5):483–8.
Aratchige PE, McIntyre PB, Quinn HE, Gilbert GL. Recent increases in mumps incidence in Australia: the “forgotten” age group in the 1998 Australian measles control campaign. Med J Aust. 2008;189(8):434–7.
Dayan GH, Quinlisk MP, Parker AA, Barskey AE, Harris ML, Schwartz JM et al. Recent resurgence of mumps in the United States. N Engl J Med. 2008;358(15):1580–9.
Vandermeulen C, Roelants M, Vermoere M, Roseeuw K, Goubau P, Hoppenbrouwers K. Outbreak of mumps in a vaccinated child population: a question of vaccine failure? Vaccine. 2004;22(21–22):2713–16.
Peltola H, Jokinen S, Paunio M, Hovi T, Davidkin I. Measles, mumps, and rubella in Finland: 25 years of a nationwide elimination programme. Lancet Infect Dis. 2008;8(12):796–803.
Vandermeulen C, Leroux-Roels G, Hoppenbrouwers K. Mumps outbreaks in highly vaccinated populations: What makes good even better?. Hum Vaccin. 2009;5(7):494–6.
Galazka AM, Robertson SE, Kraigher A. Mumps and mumps vaccine: a global review. Bull World Health Organ. 1999;77(1):3–14.
Hviid A, Rubin S, Muhlemann K. Mumps. Lancet. 2008;371(9616):932–44.
Agarwal T, Rahman N, Abel R. Down in the mumps. J Pediatr Surg. 2006;41(12):e17–18.
Hashimoto H, Fujioka M, Kinumaki H. An office-based prospective study of deafness in mumps. Pediatr Infect Dis J. 2009;28(3):173–5.
Baas MC, van Donselaar KA, Florquin S, van Binnendijk RS, ten Berge IJ, Bemelman FJ. Mumps: not an innocent bystander in solid organ transplantation. Am J Transplant. 2009;9(9):2186–9.
Plotkin SA, Rubin SA. Mumps vaccine. In: SA Plotkin WA Orenstein, PA Offit editors. Vaccines. 5th ed. Philadelphia, PA: Elsevier; 2008. p. 435–65.
Ornoy A, Tenenbaum A. Pregnancy outcome following infections by coxsackie, echo, measles, mumps, hepatitis, polio and encephalitis viruses. Reprod Toxicol. 2006;21(4):446–57.
Anderson LJ, Seward JF. Mumps epidemiology and immunity: the anatomy of a modern epidemic. Pediatr Infect Dis J. 2008;27(10 Suppl):S75–S79.
Rubin SA, Amexis G, Pletnikov M, Li Z, Vanderzanden J, Mauldin J et al. . Changes in mumps virus gene sequence associated with variability in neurovirulent phenotype. J Virol. 2003;77(21):11616–24.
Rubin SA, Afzal MA, Powell CL, Bentley ML, Auda GR, Taffs RE et al. The rat-based neurovirulence safety test for the assessment of mumps virus neurovirulence in humans: an international collaborative study. J Infect Dis. 2005;191(7):1123–8.
Johansson B, Tecle T, Orvell C. Proposed criteria for classification of new genotypes of mumps virus. Scand J Infect Dis. 2002;34(5):355–7.
Dayan GH, Rubin S. Mumps outbreaks in vaccinated populations: are available mumps vaccines effective enough to prevent outbreaks?. Clin Infect Dis. 2008;47(11):1458–67.
Friedman M, Hadari I, Goldstein V, Sarov I. Virus-specific secretory IgA antibodies as a means of rapid diagnosis of measles and mumps infection. Isr J Med Sci. 1983;19(10):881–4.
Friedman MG. Radioimmunoassay for the detection of virus-specific IgA antibodies in saliva. J Immunol Methods. 1982;54(2):203–11.
Simpson RE. Infectiousness of communicable diseases in the household (measles, chickenpox, and mumps). Lancet. 1952;2(6734):549–54.
World Health Organization. WHO-recommended standards for surveillance of selected vaccine-preventable diseases Geneva; 2003. http://www.who.int/immunization_monitoring/diseases/mumps_surveillance/en/
Davidkin I, Jokinen S, Paananen A, Leinikki P, Peltola H. Etiology of mumps-like illnesses in children and adolescents vaccinated for measles, mumps, and rubella. J Infect Dis. 2005;191(5):719–23.
Brook I. Diagnosis and management of parotitis. Arch Otolaryngol Head Neck Surg. 1992;118(5):469–71.
Bastien N, Bowness D, Burton L, Bontovics E, Winter AL, Tipples G et al. Parotitis in a child infected with triple-reassortant influenza A virus in Canada in 2007. J Clin Microbiol. 2009;47(6):1896–8.
Falk WA, Buchan K, Dow M, Garson JZ, Hill E, Nosal M et al. The epidemiology of mumps in southern Alberta 1980-1982. Am J Epidemiol. 1989;130(4):736–49.
CDC (Atlanta) http://www.cdc.gov/ncphi/disss/nndss/casedef/mumps_2008.htm last accessed 10 Sep, 2009.
Leland DS. Parainfluenza and mumps viruses. In: PR Murray, EJ Baron, JH Jorgensen, ML Landry and MA Pfaller (ed.). Manual of Clinical Microbiology. 2007; 9:1352–60; Washington, DC: ASM Press.
Krause CH, Eastick K, Ogilvie MM. Real-time PCR for mumps diagnosis on clinical specimens–comparison with results of conventional methods of virus detection and nested PCR. J Clin Virol. 2006;37:184–9.
Hatchette TF, Davidson R, Clay S, Pettipas J, LeBlanc J, Sarwal S, Smieja M, Forward KR. Laboratory diagnosis of mumps in a partially immunized population: The Nova Scotia Experience. Can J Infect Dis Med Microbiol. 2009;20(4):e157–e162.
CDC (Atlanta) http://www.cdc.gov/ncphi/disss/nndss/casedef/mumps_2008.htm last accessed 10 Sep 2009.
Germann D, Gorgievski A, Strohle A, Matter L. Detection of mumps virus in clinical specimens by rapid centrifugation culture and conventional tube cell culture. J Virol Methods. 1998;73:59–64.
Uchida K, Shinohara M, Shimada S, Segawa Y, Doi R, Gotoh A, Hondo R. Rapid and sensitive detection of mumps virus RNA directly from clinical samples by real-time PCR. J Med Virol. 2005;75:470–4.
Jin L, Beard S, Brown DW. Genetic heterogeneity of mumps virus in the United Kingdom: identification of two new genotypes. J Infect Dis. 1999;180:829–33.
Boddicker JD, Rota PA, Kreman T, Wangeman A, Lowe L, Hummel KB, Thompson R, Bellini WJ, Pentella M, Desjardin LE. Real-time reverse transcription-PCR assay for detection of mumps virus RNA in clinical specimens. J Clin Microbiol. 2007;45:2902–8.
Leblanc JJ, Pettipas J, Davidson RJ, Tipples GA, Hiebert J, Hatchette TF. Detection of mumps virus RNA by real-time one-step reverse transcriptase PCR using the LightCycler platform. J Clin Microbiol. 2008;46:4049–51.
Jin L, Feng Y, Parry R, Cui A, Real-time LuY. PCR and its application to mumps rapid diagnosis. J Med Virol. 2007;79:1761–7.
Krause CH, Molyneaux PJ, Ho-Yen DO, McIntyre P, Carman WE, Templeton. KE. J Clin Virol. 2007;38:153.
Rota JS, Turner JC, Yost-Daljev MK, Freeman M, Toney DM, Meisel E, Williams N, Sowers SB, Lowe L, Rota PA, Nicolai LA, Peake L, Bellini WJ. Investigation of a mumps outbreak among university students with two measles-mumps-rubella (MMR) vaccinations, Virginia, September-December 2006. J Med Virol. 2009;81:1819–25.
Pipkin PA, Afzal MA, Heath AB, Minor PD. Assay of humoral immunity to mumps virus. J Virol Methods. 1999;79:219–25.
Ballew HC. In: S Specter, RL Hodinka, SA Young editors. Neutralization in: clinical virology manual, 3rd ed. Washington, DC. ASM Press, 2000. p. 127–34.
Tipples GA, Beirnes J, Hiebert J, Hatchette T, Pettipas J, Macey J, Deeks S, Lipskie T, Bellini W, Rota P, Rota J Laboratory Guidelines for the diagnosis of mumps v.3 (3 Apr 2008) http://www.nml-lnm.gc.ca/guide/guideview-eng.asp?key=186 (Last accessed 10 Sep 2009:1352–1360).
Jick H, Chamberlin DP, Hagberg KW. The origin and spread of a mumps epidemic: United kingdom, 2003–2006. Epidemiology. 2009;20(5):656–61.
Muhlemann K. The molecular epidemiology of mumps virus. Infect Genet Evol. 2004;4(3):215–19.
Bonnet MC, Dutta A, Weinberger C, Plotkin SA. Mumps vaccine virus strains and aseptic meningitis. Vaccine. 2006;24(49–50):7037–45.
World Health Organization. Mumps virus vaccines. Wkly Epidemiol Rec. 2007;82(7):51–60.
Stokes J Jr, Weibel RE, Buynak EB, Hilleman MR. Live attenuated mumps virus vaccine. II. Early clinical studies. Pediatrics. 1967;39(3):363–71.
Asatryan A, Pool V, Chen RT, Kohl KS, Davis RL, Iskander JK. Live attenuated measles and mumps viral strain-containing vaccines and hearing loss: Vaccine Adverse Event Reporting System (VAERS), United States, 1990–2003. Vaccine. 2008;26(9):1166–72.
Kaic B, Gjenero-Margan I, Aleraj B, Ljubin-Sternak S, Vilibic-Cavlek T, Kilvain S et al. Transmission of the L-Zagreb mumps vaccine virus, Croatia, 2005–2008. Euro Surveill. 2008;13(16). http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=18843.
Tesovic G, Poljak M, Lunar MM, Kocjan BJ, Seme K, Vukic BT et al. Horizontal transmission of the Leningrad-Zagreb mumps vaccine strain: a report of three cases. Vaccine. 2008;26(16):1922–5.
Atrasheuskaya AV, Neverov AA, Rubin S, Ignatyev GM. Horizontal transmission of the Leningrad-3 live attenuated mumps vaccine virus. Vaccine. 2006;24(10):1530–6.
Weibel RE, Stokes J Jr, Buynak EB, Whitman JE Jr, Hilleman MR. Live attenuated mumps-virus vaccine. 3. Clinical and serologic aspects in a field evaluation. N Engl J Med. 1967;276(5):245–51.
Miller E, Goldacre M, Pugh S, Colville A, Farrington P, Flower A et al. Risk of aseptic meningitis after measles, mumps, and rubella vaccine in UK children. Lancet. 1993;341(8851):979–82.
LeBaron CW, Forghani B, Beck C, Brown C, Bi D, Cossen C et al. Persistence of mumps antibodies after 2 doses of measles-mumps-rubella vaccine. J Infect Dis. 2009;199(4):552–60.
Miller E, Hill A, Morgan-Capner P, Forsey T, Rush M. Antibodies to measles, mumps and rubella in UK children 4 years after vaccination with different MMR vaccines. Vaccine. 1995;13(9):799–802.
Davidkin I, Jokinen S, Broman M, Leinikki P, Peltola H. Persistence of measles, mumps, and rubella antibodies in an MMR-vaccinated cohort: a 20-year follow-up. J Infect Dis. 2008;197(7):950–6.
Jokinen S, Osterlund P, Julkunen I, Davidkin I. Cellular immunity to mumps virus in young adults 21 years after measles-mumps-rubella vaccination. J Infect Dis. 2007;196(6):861–7.
Harling R, White JM, Ramsay ME, Macsween KF, van den Bosch C. The effectiveness of the mumps component of the MMR vaccine: a case control study. Vaccine. 2005;23(31):4070–4.
Peltola H, Kulkarni PS, Kapre SV, Paunio M, Jadhav SS, Dhere RM. Mumps outbreaks in Canada and the United States: time for new thinking on mumps vaccines. Clin Infect Dis. 2007;45(4):459–66.
Beck M, Welsz-Malecek R, Mesko-Prejac M, Radman V, Juzbasic M, Rajninger-Miholic M et al. . Mumps vaccine L-Zagreb, prepared in chick fibroblasts. I. Production and field trials. J Biol Stand. 1989;17(1):85–90.
Vesikari T, Sadzot-Delvaux C, Rentier B, Gershon A. Increasing coverage and efficiency of measles, mumps, and rubella vaccine and introducing universal varicella vaccination in Europe: a role for the combined vaccine. Pediatr Infect Dis J. 2007;26(7):632–8.
Boxall N, Kubinyiova M, Prikazsky V, Benes C, Castkova J. An increase in the number of mumps cases in the Czech Republic, 2005–2006. Euro Surveill. 2008;13(16). http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=18842.
Bernard H, Schwarz NG, Melnic A, Bucov V, Caterinciuc N, Pebody RG et al. . Mumps outbreak ongoing since October 2007 in the Republic of Moldova. Euro Surveill. 2008;13(13). http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=8079.
Kaaijk P, van der Zeijst B, Boog M, Hoitink C. Increased mumps incidence in the Netherlands: review on the possible role of vaccine strain and genotype. Euro Surveill. 2008;13(26). http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=18914.
Public Health Agency of Canada. Canadian National Report on Immunization, 2006. http://www.phac-aspc.gc.ca/publicat/ccdr-rmtc/06vol32/32s3/4epi-eng.php
Gay N, Miller E, Hesketh L, Morgan-Capner P, Ramsay M, Cohen B et al. Mumps surveillance in England and Wales supports introduction of two dose vaccination schedule. Commun Dis Rep CDR Rev. 1997;7(2):R21–R26.
Anderson RM, Crombie JA, Grenfell BT. The epidemiology of mumps in the UK: a preliminary study of virus transmission, herd immunity and the potential impact of immunization. Epidemiol Infect. 1987;99(1):65–84.
Colville A, Pugh S, Miller E. Withdrawal of a mumps vaccine. Eur J Pediatr. 1994;153(6):467–8.
Centers for Disease Control and Prevention. Mumps epidemic–United kingdom, 2004–2005. MMWR Morb Mortal Wkly Rep. 2006;55(7):173–5.
Savage E, Ramsay M, White J, Beard S, Lawson H, Hunjan R et al. Mumps outbreaks across England and Wales in 2004: observational study. BMJ. 2005;330(7500):1119–20.
MacDonald N, Flegel K. Mumps in young adults: the canary in the coal mine. CMAJ. 2007;177(2):121, 3.
Wright JA, Polack C. Understanding variation in measles-mumps-rubella immunization coverage–a population-based study. Eur J Public Health. 2006;16(2):137–42.
Cohen C, White JM, Savage EJ, Glynn JR, Choi Y, Andrews N et al. . Vaccine effectiveness estimates, 2004–2005 mumps outbreak, England. Emerg Infect Dis. 2007;13(1):12–17.
Gabutti G, Guido M, Rota MC, De Donno A, Ciofi Degli Atti ML, Crovari P. The epidemiology of mumps in Italy. Vaccine. 2008;26(23):2906–11.
Public Health Agency of Canada. Mumps in Canada, 2007. 2009. http://www.phac-aspc.gc.ca/mumps-oreillons/prof-eng.php
Goh KT. Resurgence of mumps in Singapore caused by the Rubini mumps virus vaccine strain. Lancet. 1999;354(9187):1355–6.
Ong G, Goh KT, Ma S, Chew SK. Comparative efficacy of Rubini, Jeryl-Lynn and Urabe mumps vaccine in an Asian population. J Infect. 2005;51(4):294–8.
Richard JL, Zwahlen M, Feuz M, Matter HC. Comparison of the effectiveness of two mumps vaccines during an outbreak in Switzerland in 1999 and 2000: a case-cohort study. Eur J Epidemiol. 2003;18(6):569–77.
Cortese MM, Jordan HT, Curns AT, Quinlan PA, Ens KA, Denning PM et al. Mumps vaccine performance among university students during a mumps outbreak. Clin Infect Dis. 2008;46(8):1172–80.
Rubin SA, Qi L, Audet SA, Sullivan B, Carbone KM, Bellini WJ et al. Antibody induced by immunization with the Jeryl Lynn mumps vaccine strain effectively neutralizes a heterologous wild-type mumps virus associated with a large outbreak. J Infect Dis. 2008;198(4):508–15.
Narita M, Matsuzono Y, Takekoshi Y, Yamada S, Itakura O, Kubota M et al. Analysis of mumps vaccine failure by means of avidity testing for mumps virus-specific immunoglobulin G. Clin Diagn Lab Immunol. 1998;5(6):799–803.
Peltola H, Davidkin I, Paunio M, Valle M, Leinikki P, Heinonen OP. Mumps and rubella eliminated from Finland. JAMA. 2000;284(20):2643–7.
Centers for Disease Control and Prevention. Updated recommendations for isolation of persons with mumps. MMWR Morb Mortal Wkly Rep. 2008;57(40):1103–5.
Marienau KJ, Averhoff F, Redd S. The role of air travel in the spread of mumps. Clin Infect Dis. 2008;47(9):1237.
Centers for Disease Control and Prevention. Vaccines & Immunizations. Programs & Tools. CDC Vaccine Price List. 2009. http://www.cdc.gov/vaccines/programs/vfc/cdc-vac-price-list.htm
Kamerow D. Yankee doodling: jabbering about jabs. BMJ. 2008;337:a1517.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
MacDonald, N., Hatchette, T., Elkout, L., Sarwal, S. (2011). Mumps is Back: Why is Mumps Eradication Not Working?. In: Curtis, N., Finn, A., Pollard, A. (eds) Hot Topics in Infection and Immunity in Children VII. Advances in Experimental Medicine and Biology, vol 697. Springer, New York, NY. https://doi.org/10.1007/978-1-4419-7185-2_14
Download citation
DOI: https://doi.org/10.1007/978-1-4419-7185-2_14
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4419-7184-5
Online ISBN: 978-1-4419-7185-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)