
Abstract
Ms. Jones is an 82-year-old F who was in her usual state of good health when she developed a fever and cough. A chest X-ray revealed left upper lobe pneumonia and she was successfully treated with a course of antibiotics. Three months later her pneumonia recurred, and at that time a chest CT showed a left upper lobe nodule. A biopsy of the nodule was consistent with adenocarcinoma, and she was referred for thoracic surgery evaluation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Postoperative Delirium
- Limited Resection
- Postoperative Atrial Fibrillation
- Typical Carcinoid
- Pulmonary Carcinoid
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Case Study
Ms. Jones is an 82-year-old F who was in her usual state of good health when she developed a fever and cough. A chest X-ray revealed left upper lobe pneumonia and she was successfully treated with a course of antibiotics. Three months later her pneumonia recurred, and at that time a chest CT showed a left upper lobe nodule. A biopsy of the nodule was consistent with adenocarcinoma, and she was referred for thoracic surgery evaluation.
On evaluation Ms. Jones is found to be healthy and active, despite recent flares of arthritis in her hands. Her family refers to her as “well preserved.” She walks daily for a quarter mile with her family, shops for her own groceries and enjoys gardening. She carries a basket of laundry up two flights of stairs every day, and carries two bags of groceries at a time into the kitchen from her car. She had a myocardial infarction 17 years ago and 2 years ago had a cardiac stent placed. She has a history of reflux disease which seems to be worsening over the past year. She has osteoarthritis and the kyphosis in her back has become quite obvious. She has a distant 27-pack year smoking history. She has extensive social supports and is viewed as the matriarch of a family that includes 6 children and 21 grandchildren. Her first great grandchild is expected this fall. She is active in her church and volunteers at a shelter serving meals once a month.
Pulmonary function tests are notable for good lung function with an FEV1 of 1.8 L (81% predicted) and an FVC of 2.6 L (88% predicted). She is able to walk 1,400 feet in 6 min without hypoxia. She is able to climb two flights of stairs without difficulty. A brain MRI, bronchoscopy, and mediastinoscopy are all negative. How does Ms. Jones advanced age affect her management?
Introduction
With the aging of the baby boomer population, the number of people in the USA over 65 is expected to nearly double by 2040. Currently 12.5% of the US population is over the age of 65, and this percentage is projected to increase to 20% by the year 2050. The average life expectancy in the USA is 77.8 and projected to increase to over 80 by 2050 [1–4].
Older patients increasingly present for consideration of thoracic surgery, and determining the optimal management for this group of patients will be a more frequent challenge in the future. While elderly patients present with a spectrum of thoracic disease, both benign and malignant, patients with cancer comprise the largest and most studied subset of this population.
Lung cancer is a disease of the elderly. The median age of diagnosis for lung cancer in the USA is 71 years and over 65% of patients are diagnosed after age 65. National Cancer Institute statistics indicate that lung cancer is the leading cause of cancer mortality in men and women [5, 6]. In 2008 an estimated 215,020 Americans will be diagnosed and 161,840 people will die of lung cancer. Over 100,000 lung cancer deaths will be in patients over the age of 65 [7].
Non-small cell lung cancer (NSCLC) comprises 80–85% of primary lung tumors, small cell lung cancer (SCLC) makes up 15–20% and 1–2% are pulmonary carcinoid [8–10]. SCLC is usually widely metastatic at time of diagnosis, and rarely under the purview of the surgeon; however, the percentage of lung cancer patients with SCLC histology falls with age [10]. Surgical resection of NSCLC and pulmonary carcinoid offers the best chance for oncologic cure. Additionally, retrospective evidence suggests that resection of isolated metastases to the lung may improve survival.
The decision to undergo surgical resection for malignant disease should not be based on age alone. An understanding of the unique qualities of this patient population has lead to improved surgical outcomes for the elderly over the last several decades. Patient evaluation, selection, and peri-operative management must all be adapted to provide best possible care for the increasing numbers of aged patients undergoing surgery for cancer. Management of an elderly lung cancer patient requires a global consideration of the characteristics of aging, differences in tumor presentation and histology, and co-morbidities that tend to accumulate over time. The initial interview with a patient and family members is used to elucidate important variables that may impact operative risk and expectations of the recovery process. These questions should elucidate the current independent status of the patient, social supports, mood, and signs of reduced activity or physical limitations. After all, the elderly population is a heterogeneous group of patients ranging in functional reserve from the surprisingly well preserved to the wheelchair bound.
Physiologic Changes of Age
Physiologic changes of the respiratory system associated with aging include reduced chest wall compliance with stiffening of calcified costal cartilages and narrowing of the intervertebral disc space. A progressively restricted ribcage is accompanied by decreased diaphragmatic excursion. Postoperative weakness of the hemi-diaphragm in this group can lead to otherwise unexplained respiratory failure. There is a reduction of lung elastic recoil with loss of alveolar architecture producing a decreased alveolar gas exchange surface. The loss of lung elastic recoil and decreased lung compliance diminishes negative intrapleural pressure, which then prevents reopening of the small airways, resulting in air trapping and inadequate ventilation. Functionally this manifests in a gradual decline of vital capacity and partial pressure of oxygen (Po2), with an increase in residual volume. Progressive atrophy creates weakness of the respiratory musculature. Decline in motor power of the accessory muscles and a stiffening of the chest wall also result in a declining forced expiratory volume in 1 s (FEV1). Changes in lung compliance are not uniformly distributed. Higher respiratory rates therefore increase ventilation–perfusion mismatch. Additionally, there is a decrease in central nervous system responsiveness. The elderly exhibit a blunted ventilatory response to both hypoxic and hypercapneic insults [11, 12].
Physiologic changes in lung mechanics make elderly patients particularly sensitive to narcotics and muscle relaxants, as well as to supine positioning. Elderly patients are also at increased risk for respiratory tract infections, due to waning immune responses [13]. Smoking in particular has been shown to cause bronchial mucociliary dysfunction [14]. which has been associated with increased susceptibility to infection [15]. Finally, elderly patients with marked kyphosis and accompanying paraesophageal diaphragmatic hernias are at particular risk for postoperative aspiration.
Increasing age is associated with declines in other organ systems as well. There is a decline in glomerular filtration rate, an increasing incidence of heart disease, and an increasing incidence of cognitive dysfunction. Changes in body composition decrease the volume of distribution of water-soluble drugs [16]. Additionally, elderly patients take more medications than younger patients and are vulnerable to adverse drug effects.
Preoperative Evaluation
Elderly patients are at increased risk for preoperative morbidity and mortality due to both decreased ability to recover physiologic homeostasis after surgical stress and co-morbid conditions. Older patients represent a heterogeneous population, and should be offered surgery based on physiologic rather than chronological age. A thorough preoperative assessment is imperative to determine whether a patient is an appropriate surgical candidate and to predict and avoid postoperative complications. Numerous risk assessment tools have been created to define preoperative variables that correlate with poor outcomes; however, an easy to use, strongly predictive tool, has been elusive. Geriatric assessment tools aimed at predicting outcomes in the specific elderly surgical population remain under study.
All patients in consideration for lung cancer resection surgery require a complete history and physical exam with particular attention to characterization of symptoms, smoking history, and weight loss. At a minimum, patients should undergo a chest X-ray, electrocardiogram, a room air arterial blood gas, pulmonary function tests for patients undergoing lung resection, basic laboratory work, and a complete staging evaluation. Further workup can be determined based on symptoms or the status of co-morbid conditions.
Accurate diagnosis and staging is of utmost importance to ensure that patients are appropriately chosen for operative resection. Elderly patients should have radiographic and surgical staging of suspected lung cancers in the same manner as younger counterparts. Only after the exact stage is known can rational treatment decisions be made. Therefore, elderly patients should have chest CT scans to image suspected lung nodules, PET scans to look for metastatic disease, brain scans to look for occult metastases and, if indicated, cervical mediastinoscopy to stage mediastinal nodes. Elderly patients with suspected lung nodules should not be denied this standard workup unless their functional status is so impaired that treatment is not possible.
Cardiac Risk Assessment
The American Heart Association (AHA) and American College of Cardiology (ACC) developed consensus practice guideline for peri-operative cardiovascular evaluation for noncardiac surgery that provides a template for assessing patients of all ages [17]. The AHA/ACC guidelines describe a stepwise approach to preoperative surgery with risk stratification and further imaging determined by utilizing symptoms, clinical predictors, and functional capacity. Clinical history should focus on assessment for coronary risk factors and physical capacity including the ability to climb two flights of stairs or walk one block. In general, patients with poor functional status, or patients with a history of angina or claudication should undergo noninvasive testing. In thoracic surgery patients it may be difficult to determine if symptom etiology is the result of cardiac or pulmonary pathology, thus it is appropriate to have a low threshold for additional cardiac imaging and assessment by a cardiologist to assist with risk stratification.
Supraventricular tachycardias are very common after thoracic surgery, with increased risk for older patients or those with a faster preoperative heart rate [18]. The risk of postoperative atrial fibrillation is 19% in patients undergoing lung resection for cancer [19]. Randomized trials of thoracic surgery patients have determined that calcium channel blockers or beta-blockers can reduce the incidence of postoperative atrial fibrillation by 50–60%; however, beta-blockers were associated with an increased risk of pulmonary edema. Neither class of medication reduced mortality. Three trials showed that digitalis increased the risk of atrial arrhythmias [20]. Beta-blockers and calcium channel blockers will both reduce postoperative atrial fibrillation; however, beta-blockers are preferred by some due to their broader benefits of cardiac risk reduction. On the other hand, up to half the doses of postoperative beta-blocker may have to be held due to transient hypotension or bradycardia, leading others to recommend the use of calcium channel blockers.
Pulmonary Risk Assessment
All patients under consideration for lung resection surgery should have pulmonary function tests performed. FEV1 by spirometry is the most common measured value used to determine a patient’s suitability for surgery. In the 1970s, data obtained from over 2,000 patients showed a <5% mortality rate for patients with an FEV1 >1.5 L for lobectomy and >2 L for pneumonectomy [21, 22]. Absolute values for FEV1 may create a bias against older people; however, a value of >80% of predicted has been quoted by some as sufficient for a patient to undergo pneumonectomy without further pulmonary testing [23]. In reviewing more recent spirometry studies performed from NSCLC patients in 1994–2000, Datta and Lahiri concluded that increased postoperative morbidity and mortality were predicted by an FEV1 of <2 L or <60% predicted for pneumonectomy, an FEV1 of <1.6 L for lobectomy, and <0.6 L for wedge or segmentectomy [24].
Lung resections have been undertaken in patients with much poorer lung function. In 2005, Linden et al. published data from a series of 100 consecutive patients with preoperative FEV1 of <35% predicted undergoing lung tumor resection. In this series, there was a 1% mortality rate (single case of perforated colonic diverticulum) and a 36% complication rate. Morbidity was dominated by 22% of patients with prolonged air leaks. Eleven patients were discharged with a new oxygen requirement, and four patients developed pneumonia. Only one patient was discharged on a ventilator and three other patients required intubation for >48 h [25].
In a study of 237 patients, Ferguson et al. found preoperative diffusion capacity for carbon monoxide (DLCO) to be more predictive of postoperative mortality than FEV1. In this study, a DLCO of <60% predicted was associated with increased mortality and a DLCO of <80% predicted was predictive of increased pulmonary complications [26]. Other studies, however, have not found this parameter to be a significant predictor of postoperative complications [27, 28]. DLCO and spirometry may be used as complimentary tests, particularly in patients with diffuse parenchymal disease or dyspnea that is out of proportion to the FEV1, with a low DLCO prompting further evaluation [22].
Formal and simple exercise testing evaluates the cardiopulmonary system under induced physiological stress and also has been found to be predictive of postoperative complications. Girish et al. prospectively studied symptom-limited stair climbing in thoracic and upper abdominal surgery patients. No complications occurred in patients who could climb seven flights of stairs, while 89% of patients unable to climb one flight of stairs had complications. Inability to climb two flights of stairs had a positive predictive value of 80%. The ability of patients to climb stairs was found to be inversely related to the length of postoperative hospital stay [29]. The 6-min walk test (6MWT) measures the distanced walked over a period of 6 min. A normal patient is able to cover at least 1,400 feet in 6 min. In a qualitative review, Solway concluded that the 6MWT was easy to administer and more reflective of activities of daily living than other walk tests [30]. While stair climbing and 6MWT are easy to perform, their use in elderly patients may be limited by orthopedic impairments, peripheral vascular insufficiency or neurological impairments.
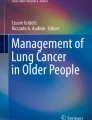
As published previously [31], a recommended preoperative pulmonary evaluation for an elderly patient should consist of spirometry, pulmonary diffusion capacity of the lung for carbon monoxide (DLCO), room air ABG, and exercise tolerance tests including stair climbing and 6-min walk. Patients with an FEV1 >1 L and no major abnormality of other tests (FEV1/FVC >50%, DLCO >50% predicted, ABG paO2 >45 mm Hg, tolerance of exercise tests) may safely proceed with surgery, including pneumonectomy (Fig. 48.1).

Recommended pulmonary evaluation for patients undergoing lung resection surgery. DLCO diffusion capacity for carbon monoxide, ABG arterial blood gas, FEV1 forced expiratory volume in 1 s, FVC forced vital capacity, VO 2 Max maximal oxygen consumption, PPO predicted postoperative.
Further evaluation for patients who fall outside these criteria include ventilation/perfusion scans to calculate predicted postoperative (PPO) lung function and VO2 max testing. A PPO FEV1 threshold of 0.8 L [32] or 0.7 L [33] has been suggested as a lower limit value for proceeding with lung resection. Absolute values of PPO FEV1 can underestimate postoperative lung function in people with small stature or the elderly, and can thus be converted into percent-predicted postoperative (% PPO) lung function. Multiple studies have suggested that morbidity increases at a threshold % PPO FEV1 of <40%, or a % PPO DLCO of <40% [26, 34–37].
Measurement of maximal oxygen consumption (VO2 max) by formal cardiopulmonary exercise testing is helpful to further risk stratify patients with borderline lung function. A VO2 max of <10 ml/kg/min had a very high operative morbidity (26% total in combined data) in several small case series. VO2 max values of 10–15 ml/kg/min had an intermediate peri-operative morbidity (8.3% total) whereas patients with >15 mg/kg/min can proceed with lung resection surgery with an acceptable mortality rate [22].
Cognitive Assessment
The likelihood of returning to baseline physical and mental function after surgery is one of the most important outcomes for an elderly patient. While patients and their families accept that there will be a postoperative recovery time in the hospital or rehabilitation setting, it is difficult to assess the magnitude of this functional decline and predict the risk of permanent loss of independence. There is a paucity of data assessing changes in quality of life after thoracic surgery in the elderly, and few studies that assess whether surgery triggers postoperative loss of independence, or change in need for assistance or living requirements. A study of 68 octogenarians undergoing pulmonary resections at Johns Hopkins Medical Institutions showed that 80% of patients were discharged directly to home from the hospital rather than to rehab, offering some proxy information regarding immediate postoperative return to function [38]. Moller et al. published a study in 1998 that showed a 25% rate of cognitive dysfunction at 1 week postop from major noncardiac surgery in elderly patients (average age 68), with continued dysfunction in 9% at 3 months [39]. Data from many studies verify a high incidence of postoperative cognitive dysfunction in the first week after surgery, and dysfunction does tend to increase with age. Only one other study has substantiated long-term declines over controls, and some have suggested that declines found in these studies may be due to random variation [40, 41]. Karneko et al. determined that preoperative dementia was a risk factor for postoperative delirium [42]. Furthermore, Fukuse et al. found that thoracic surgery patients with preoperative dementia, as estimated by the mini-mental status exam (MMS), were fourfold more likely to have postoperative complications [43].
Geriatric Assessments
There are multiple assessment indices that have been applied to elderly patients to link preoperative function with risk for poor outcome. Functional status describes the ability to perform self-care, self-maintenance, and physical activities. Traditional measures used to assess functional status are activities of daily living (ADLs) and instrumental activities of daily living (IADLs). ADLs are six basic self-care skills, including the ability to bathe, dress, go to the toilet, transfer from a bed to chair, maintain continence, and feed one’s self. IADLs include higher functioning skills that are used to maintain independence in the community. This scale assesses ability to use the telephone, go shopping, prepare food, perform housekeeping and laundry, use various modes of transportation, assume responsibility for medications, and the ability to handle finances. Need for assistance in these tasks has been predictive of prolonged hospital stay, nursing home placement and home-care requirements [44, 45]. Poor nutritional status, defined as a BMI <22 kg/m2 has been associated with increased need for assistance with ADLs and a decreased 1-year survival [46]. A lower ADL score is associated with postoperative complications [47]. The information source reporting a patient’s functional status biases the results, with self-reported scores rating higher than scores reported by a significant other or nurse [48].
Performance status is a standardized scale designed to measure the ability of a cancer patient to perform ordinary tasks. There are two scales, the Karnofsky performance scale, which ranges from 0 (dead) to 100 (normal) and the ECOG scale that ranges from 0 (asymptomatic) to 5 (dead). Comparisons of the two scales have been validated with a large sample of patients [49]. Performance status has been used to select patients for entry into chemotherapy trials; however, it is also well accepted to be associated with postoperative morbidity [50–52].
Postoperative Care
Postoperative management must be optimized specifically for the elderly population. Narcotic use should be minimized whenever possible to prevent delirium, and appropriate elderly patients should be assessed for preoperative placement of a thoracic epidural catheter for analgesia. Benzodiazapines and medications for sleep should also be minimized. Excellent pulmonary hygiene must be maintained with frequent chest physiotherapy and early ambulation. At our institution, thoracic ambulation carts, as shown in Fig. 48.2, are used to facilitate walking patients who require oxygen, and are otherwise tethered with multiple lines and catheters. Forearms are supported by pads while hands wrap around a handbrake. Oxygen tanks and ambulatory saturation monitors are stored along the sides. Pleural drainage systems can be suspended from the side rails. A cloth strap is used to secure the patient to the cart during ambulation.

Thoracic ambulation cart used to facilitate early postoperative ambulation (artwork by Marcia Williams).
Non-small Cell Lung Cancer
Stage at Presentation
Elderly patients more frequently have early-stage disease, compared to younger patients with lung cancer. O’Rourke et al. used a database of 22,874 patients to demonstrate that percentage of patients with surgically resectable disease at diagnosis increases with age. The percent of lung cancer patients with local stage NSCLC increased from 15.3% of those aged 54 years or younger, to 19.2% of those aged 55–64 years, to 21.9% of those aged 65–74 years, and to 25.4% of those aged 75 years or older [53]. Data published from the Surveillance, epidemiology, and end results (SEER) database in 2005 analyzing a cohort of 14,555 patients with early-stage NSCLC showed that the frequency of stage I disease increased from 79% in patients <65 to 87% in patients age 75 or greater [54]. Thus, although the elderly are at higher risk of developing lung cancer, a higher proportion present with potentially curable disease.
Histology
Elderly patients are more likely to be diagnosed with squamous cell carcinoma (SCC) over other histology types [10, 55, 56]. Mery et al.’s analysis of the SEER database showed that the frequency of SCC increased from 27% in patients <65 years old, to 38% in patients 75 and older, with parallel decreases in frequency of adenocarcinoma from 61 to 50% in corresponding age groups [54]. SCCs are associated with a higher incidence of local disease [53], tend to have lower recurrence rates and may have longer survival times than non-squamous cell cancers [57–59]. Squamous cell tumors are more likely to be centrally located however, and thus are more likely to require pneumonectomy for curative resection.
Extent of Resection
Surgical resection for NSCLC offers the best chance for cure. The extent of NSCLC resection in elderly patients has been extensively debated, with advocates for limited resections for the aged. Lobectomy, removal of one of the five lobes of the lung and associated lymph nodes within a single pleural membrane, is considered standard of care for surgical resection of early-stage NSCLC [60]. Unfortunately there are multiple studies that substantiate age as a risk factor for death after thoracotomy. Using data from the 1960s and 1970s, several small single institution studies published operative mortality rates of 14–27% for the elderly depending on age and type of surgery [61–64]. These findings were confirmed by a multiinstitution study by the Lung Cancer Study Group in 1983. Ginsberg et al. reviewed 2,200 cases of lung resection for cancer and found that operative mortality increased proportionally with age. Patients with age <60 had a 1.3% 30-day mortality rate, with increasing rates of 4.1, 7.0, and 8.1% mortality rates for the 60–69, 70–79, and 80 or greater age groups, respectively [65].
More recently, Mery et al. determined a 30-day postoperative mortality rate of 14,555 patients who had undergone curative resections for treating stage I or II NSCLC over the period of 1992–1997. In an analysis of patients undergoing all types of surgery, there was a 0.45% mortality rate for those under age 65 years old, 0.6% for ages 65–74, and 1.2% for patients age 75 or older ( p = 0.001). Mortality differences were found to be primarily due to differences in survival of patient undergoing lobectomy, with 0.3, 0.5, and 1.5% mortality, respectively, for these corresponding age groups ( p = 0.0001). The difference in peri-operative mortality was statistically similar for patients undergoing limited resection [66]. Prior published reports likewise did not identify a difference in expected operative mortality after thoracotomy if lung-sparing operations were performed [67–69].
The American College of Surgeons Oncology Group (ACOSOG) Z0030 Study published morbidity and mortality data in 2006 for 1,023 clinically resectable T1 or T2, N0 or non-hilar N1 NSCLC patients randomized over a period from 1999 to 2004 to undergo pulmonary resection with lymph node sampling vs. mediastinal lymph node dissection. Their age-stratified morbidity and mortality data is shown in Table 48.1. Notably, overall mortality was 1.4%, improved from Ginsberg’s reported 3.8%, and was not statistically associated with age [70]. Ninety percent of patients in the ACOSOG Z0030 study underwent resection via a thoracotomy, with the remaining procedures performed as video-assisted thoracic surgery (VATS) or VATS-assisted resections. Operative mortality reported by Ginsberg for pneumonectomy and lobectomy was 6.2 and 2.9%, respectively, compared with 0 and 1.3%, in the ACOSOG study. Notably the pneumonectomy rate of the earlier study was 25.6 vs. 4% in ACOSOG, likely partially explaining the higher mortality rate of the earlier study. The complication rate did rise as age increased, with 49% of patients in the 80 and over age group experiencing one or more complication.
The operative risk of death after pulmonary resections is largely attributable to two anatomical disruptions. First there is the loss of functional lung tissue, and secondly there is the morbidity and mortality introduced by the access thoracotomy. Operative strategies particular to the elderly population addresses both of these fronts, with use of video-assisted thoracoscopic surgery (VATS) to minimize the chest wall disruption of a thoracotomy and by consideration of limited resections for the most elderly. Figure 48.3 illustrates the difference in the disruption of chest wall musculature between thoracotomy and VATS approaches.

Lung resection surgery via (a) posteriolateral thoracotomy (b) video-assisted thoracoscopic surgery (artwork by Marcia Williams).
VATS is defined as surgery performed through two or three incisions that are 2 cm in length. A utility incision <10 cm long may be used, without spreading of the ribs. VATS procedures in the elderly have been shown to have lower morbidity, lower rates of postoperative delirium and result in earlier ambulation, a lower narcotic requirement, and a quicker recovery time [71–75].
Limited resections, consisting of either a sementectomy or wedge resection, remove less lung tissue and are usually performed via VATS. These operations are associated with less peri-operative morbidity and mortality; however, do not completely remove draining lymphatics and may be associated with poorer oncologic outcomes. A randomized trial by the Lung Cancer Study Group of limited resection vs. lobectomy for T1 N0 disease revealed a tripling of locoregional recurrence with limited resection, and a trend toward improved survival in the lobectomy group [76]. Divergence of the survival curves between lobectomy and limited resection did not occur until 3 years after surgery, however, indicating a potential role for limited resection in patients with a shorter expected life span. Additional studies have concluded that limited resection remains a “compromise” treatment for elderly patients or those with limited cardiopulmonary reserve [77]. An age-stratified analysis of 14,555 patients in the SEER database, showed no benefit for lobectomy over limited resection in patients over age 71 [54]. Figure 48.4 shows a schematic of the range of lung resections. The decision to perform a limited resection vs. a lobectomy must take into account the patient’s ability to tolerate a larger surgery and potential associated complications vs. a smaller resection with less durable oncologic outcomes.

Extent of resection, (a) wedge resection, (b) lobectomy, (c) and pneumonectomy (artwork by Marcia Williams).
Pulmonary Carcinoid
Pulmonary carcinoids represent 1–2% of lung tumors. They consist of a spectrum of neuroendocrine tumors that are divided into those with typical (TC) or atypical (AC) histological features. While carcinoids tend to present in younger patients, atypical tumors are often diagnosed about 10 years later than typical carcinoid, occurring in the sixth decade. Atypical carcinoids tend to be larger, are usually localized to the peripheral lung fields, and are more aggressive than typical carcinoids. The 5-year survival is 40–60 vs. 90% for indolent typical carcinoids [78]. Limited resection with wedge or segmentectomy is the preferred treatment for localized carcinoids. More extensive resection has been advocated for atypical carcinoids, with extent of resection mirroring recommendations for NSCLC [79, 80].
Surgical Resection for Pulmonary Metastases
Metastasis to the lungs is a common oncologic problem. Pulmonary metastases tend to be an indicator of widely metastatic disease; however, in some patients metastases to the lungs may occur in isolation. Retrospective evidence suggests that highly selected patients may have improved survival after resection of pulmonary metastases. Indications for the procedure include (1) control of the primary site, (2) metastatic disease isolated to the thorax, (3) resectable disease, and (4) sufficient cardiopulmonary reserve for the operation [81]. Most studies have found that age does not have a prognostic influence on overall survival [82–87].
The largest evaluation of outcomes after lung metastasectomy comes from the International Registry of Lung Metastases. Established in 1990, the registry enrolls all patients who have undergone resection of lung metastases with curative intent. Of the 5,206 patients enrolled between 1991 and 1995, 43% of lung metastases were epithelial in origin, 42% were sarcomas, 7% were germ cell tumors, 6% were melanomas, and 2% were other types. Single metastases accounted for 46% and multiple metastases 52%. Germ cell tumors had the best survival and melanoma the poorest survival at 5 and 10 years (68% at 5 years and 63% at 10 years vs. 21 and 14%, respectively). The survival rates for epithelial tumors and sarcomas did not differ significantly (37% at 5 years and 21% at 10 years vs. 31 and 26%, respectively). Rates of recurrence also varied by histology type, with 64% for sarcomas and melanoma, 46% for epithelial and 26% for germ cell tumors with a median time to recurrence of 10 months. In a multivariate analysis, disease-free interval (DFI), number of metastases and tumor type were highly prognostic of long-term survival. Based on these findings, Pastorino et al. proposed four prognostic groupings to provide a framework for management. Group I consisted of patients with resectable metastases, a DFI ≥ 36 months and a single metastasis. Group II patients had resectable metastases, and a DFI of <36 months or multiple metastases. Group III again had resectable lesions and both a DFI of <36 months and multiple metastases. Patients with unresectable metastases made up group IV. Median survival for these four groups were 61, 34, 24, and 14 months for groups I–IV, respectively [87].
The use of VATS over thoracotomy for lung metastasectomy is controversial, as the surgeon is not able to palpate the lung for additional lesions. In 1994, Collie et al. reported that conventional CT missed up to 50% of pulmonary metastases found at surgery [88]. Furthermore, McCormack et al. found additional malignant lesions at thoracotomy in 56% of patients after initial VATS exploration, and thus concluded that thoracotomy with manual palpation was the gold standard for metastasectomy [89]. Preoperative evaluation with PET has a reported sensitivity of up to 94% for lesions 1.1–1.9 cm; however, it has limited ability to detect smaller lesions [90]. Other investigators, however, found no difference in rates of recurrence or survival between VATS and thoracotomy [91, 92]. As advances in imaging technology increase the ability to detect smaller lesions, it is likely that the use of VATS will become more commonplace, particularly in older patients. Elderly patients with isolated pulmonary metastases and adequate cardiopulmonary reserve should be considered for surgical resection.
Treatment Patterns of Elderly Cancer Patients
There are multiple studies that point to the under-treatment of cancer in the elderly, for both lung cancer and other diseases [93]. Published data from the SEER database showed that the frequency of limited resections increased with age, with a decline of pneumonectomies and lobectomies with age. Approximately, 30% of the most elderly patients in the database were denied surgery or were offered only palliative surgery, in contrast with only 8% of the youngest patients [54]. Age is associated with declines in functional reserve and organ function, and optimal treatment is often affected by co-morbid conditions. Adding to the complexity involved in treatment, the elderly have often not participated in clinical trials, often forcing clinicians to rely primarily on retrospective data for treatment decisions [94].
Using 2004 data, the life expectancy of an 80-year-old in the USA is 9.1 years (8.2 years for males, 9.8 years for females), whereas the median survival for elderly patients with untreated early-stage lung cancer is only 14 months [95]. This suggests that life limitation for an 80-year-old with lung cancer is likely to be cancer related [96]. Table 48.2 [97] shows life table data from 2004 for patients older than 65.
Case Study Update
Given Ms. Jones’ relatively good health and performance status, her expected life expectancy was felt to be at least 5 years, and that this would be shortened without resection of her cancer. As an octogenarian, a limited VATS resection was chosen over thoracotomy to reduce peri-operative morbidity and mortality. She underwent a VATS left upper lobe wedge resection and mediastinal nodal sampling without event, and was discharged home on postoperative day 4. Her pathology returned as T1 N0 Mx bronchioalveolar carcinoma (BAC). Ms. Jones continued to do well until 18 months after her surgery when a new contralateral right upper lobe spiculated mass was detected on follow-up chest CT scan. Interval follow-up CT showed slow growth of this nodule and a lack of lymphadenopathy. A bone scan and head CT was negative for metastatic disease. Diagnostically, it was unclear if this was a metastasis, a new primary tumor, or a benign nodule. She otherwise remained in good health and elected to proceed with VATS wedge resection of this second nodule. Pathology from this resection again proved to be BAC.
Two years after her second resection her chest CT showed evidence of recurrence of BAC, now in the left lower lobe, and she developed a left pulmonary effusion. She began to have progressive shortness of breath and was started on gefitinib. This stabilized her disease and her symptoms for another 12 months. She eventually succumbed to her disease, 5 years after her initial diagnosis. Her functional status remained excellent for four and a half of those years.
Summary Recommendations
Resection of pulmonary malignancies has been shown to be safe in selected elderly patients. Age alone should not be a contraindication to a therapy that offers the best chance for cure for early-stage cancer patients. A thorough preoperative assessment can help individualize the morbidity and mortality risk of surgery for each patient, and thus provide both surgeon and patient with the information needed for operative decision-making. Operative interventions in the elderly require coordinated attention to the specific requirements of the aged. Efforts must be made to balance complete oncologic resection with the elderly’s limited tolerance for homeostatic insult. Specialized multidisciplinary care provided by primary-care physicians, geriatric specialists, cardiologists, oncologists, surgeons, anesthesia, nursing, physical therapy, and nutrition optimize care for the elderly thoracic surgery patient.
References
Kung HC, Hoyery DL, Xu J (2008) Deaths: final data for 2005. Center for Disease Control. Natl Vital Stat Rep 56(10):1–124
US Census Bureau, Population Division (2008) Table 2. Projections of the population by selected age groups and sex for the United States: 2010 to 2050 (NP2008-T2). Release Date 14 Aug 2008
US Census Bureau, Population Division (2008) Table 3. Percent distribution of the projected population by selected age groups and sex for the United States: 2010 to 2050 (NP2008-T3). Release Date 14 Aug 2008
National Projections Program, Population Division (2000) NP-T7-B projected life expectancy at birth by race and Hispanic origin, 1999–2100. U.S. Census Bureau, Washington, DC
American Cancer Society, Cancer Facts & Figures (2008) Age-adjusted cancer death rates, males by site. http://www.cancer.org/docroot/MED/content/MED_1_1_Most_Requested_Graphs_and_Figures_2008.asp
American Cancer Society, Cancer Facts & Figures (2008) Age-adjusted cancer death rates, females by site. http://www.cancer.org/docroot/MED/content/MED_1_1_Most_Requested_Graphs_and_Figures_2008.asp
Ries LAG, Melbert D, Krapcho M et al (2008) SEER cancer statistics review, 1975–2005. National Cancer Institute, Bethesda, MD, http://seer.cancer.gov/csr/1975_2005/, based on November 2007 SEER data submission, posted to the SEER web site
Gridelli C, Langer C, Maione P, Rossi A, Schild SE (2007) Lung cancer in the elderly. J Clin Oncol 25(14):1898–1907
Hage R, de la Riviere AB, Seldenrijk C, van den Bosch JM (2003) Update in pulmonary carcinoid tumors: a review article. Ann Surg Oncol 10(6):697–704
Teeter SM, Holmes FF, McFarlane MJ (1987) Lung carcinoma in the elderly population. Influence of histology on the inverse relationship of stage to age. Cancer 60(6):1331–1336
Rossi A, Ganassini A, Tantucci C et al (1996) Aging and the respiratory system. Aging (Milano) 8(3):143–161
Janssens JP, Pache JC, Nicod LP (1999) Physiological changes in respiratory function associated with ageing. Eur Respir J 13:197–205
Meyer KC (2004) Lung infections and aging. Ageing Res Rev 3(1):55–67
Verra F, Escudier E, Lebargy F et al (1995) Ciliary abnormalities in bronchial epithelium of smokers, ex-smokers, and nonsmokers. Am J Respir Crit Care Med 151(3):630–634
Salathe M, O’Riordan TG, Wanner A (1996) Treatment of mucociliary dysfunction. Chest 110:1048–1057
McLesky CH (1992) Anesthesia for the geriatric patient. In: Barash PG, Cullen BF, Staelting RK (eds) Clinical anasthesia, 2nd edn. JB Lippincott, Philadelphia, pp 1353–1383
Eagle KA, Berger PB, Calkins H et al (2002) ACC/AHA guideline update for perioperative cardiovascular evaulation for noncardiac surgery. Circulation 105:1257–1267
Passman RS, Gingold DS, Amar D et al (2005) Prediction rule for atrial fibrillation after major noncardiac thoracic surgery. Ann Thorac Surg 79:1698–1703
Roselli EE, Murthy SC, Rice TW et al (2005) Atrial fibrillation complicating lung cancer resection. J Thorac Cardiovasc Surg 130:438–444
Sedrakyan A, Treasure T, Browne J et al (2005) Pharmacologic prophylaxis for postoperative atrial tachyarrhythmia in general thoracic surgery: evidence from randomized clinical trials. J Thorac Cardiovasc Surg 129:997–1005
British Thoracic Sociert (2001) Society of cardiothoracic surgeons of Great Britain and Ireland working party. Guidelines on the selection of patients with lung cancer for surgery. Thorax 56:89–108
Colice GL, Shafazand S, Griffin JP et al (2007) Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: ACCP evidence-based clinical practice guidelines (2nd ed). Chest 132:161–177
Wyser C, Stulz P, Soler M et al (1999) Prospective evaluation of an algorithm for the functional assessment of lung resection candidates. Am J Respir Crit Care Med 159:1450–1456
Datta D, Lahiri B (2003) Preoperative evaluation of patients undergoing lung resection surgery. Chest 123:2096–2103
Linden PA, Bueno R, Colson YL et al (2005) Lung resection in patients with preoperative FEV1 < 35% predicted. Chest 127:1984–1990
Ferguson MK, Little L, Rizzo L et al (1988) Diffusing capacity predicts morbidity and mortality after pulmonary resection. J Thorac Cardiovasc Surg 96:894–900
Stephan F, Boucheseiche S, Hollande J et al (2000) Pulmonary complications following lung resection: a comprehensive analysis of incidence and possible risk factors. Chest 118:1263–1270
Botsen PC, Block AJ, Moulder PC (1981) Relationship between preoperative pulmonary function tests and complications after thoracotomy. Surg Gynecol Obstet 52:813–815
Girish M, Trayner E, Dammann O et al (2001) Symptom-limited stair climbing as a predictor of postoperative cardiopulmonary complications after high risk surgery. Chest 120:1147–1151
Solway S, Brooks D, Lacasses Y et al (2001) A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest 119(1):256–270
Jaklitsch MT, Mery CM, Audisio RA (2003) The use of surgery to treat lung cancer in elderly patients. Lancet Oncol 4:463–471
Olsen GN, Block AJ, Tobias JA (1974) Prediction of postpnemonectomy pulmonary function using quantitative macroaggregate lung scanning. Chest 66:13–16
Pate P, Tenholder MF, Griffin JP et al (1996) Preoperative assessment of the high-risk patient for lung resection. Ann Thorac Surg 61:1494–1500
Markos J, Mullan BP, Hillman DR et al (1989) Preoperative assessment as a predictor of mortality and morbidity after lung resection. Am Rev Respir Dis 139:902–910
Bolliger CT, Wyser C, Boser H et al (1995) Lung scanning and exercise testing for the prediction of postoperative peformance in lung resection candidates at increased risk of complications. Chest 108:341–348
Holden DA, Rice TW, Stefmach K et al (1992) Exercise testing, 6-min walk, and stair climb in the evaluation of patients at high risk for pulmonary resection. Chest 102:1774–1779
Wahi R, McMurtry MJ, DeCaro LF et al (1989) Determinants of perioperative morbidity and mortality after pneumonectomy. Ann Thorac Surg 48:33–37
Brock MV, Kim MP, Hooker CM et al (2004) Pulmonary resection in octogenarians with stage I nonsmall cell lung cancer: a 22-year experience. Ann Thorac Surg 77:271–277
Moller JT, Cluitmans P, Rasmussen LS et al (1998) Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet 351:857–861
Rasmussen LS, Siersma VD (2004) ISPOCD Group: postoperative cognitive dysfunction: true deterioration versus random variation. Acta Anaesthesiol Scand 48:1137–1143
Newman S, Stygall J, Shaefi S et al (2007) Postoperative cognitive dysfunction after noncardiac surgery. Anesthesiology 106:572–590
Kaneko T, Takahashi S, Naka T et al (1997) Postoperative delirium following gastrointestinal surgery in elderly patients. Surg Today 27:107–111
Fukuse T, Satoda N, Hijiya K et al (2005) Importance of a comprehensive geriatric assessment in prediction of complications following thoracic surgery in elderly patients. Chest 127:886–891
Narian O, Rubenstein L et al (1988) Predictors of immediate and 6 month outcomes in hospitalized elderly patients. The importance of functional status. J Am Geriatr Society 36:775–783
Reuben D, Rubenstein L et al (1992) Value of functional staus as a predictor of mortality: results of a prospective study. Am J Med 93(6):663–669
Landi F, Giuseppe G et al (1999) Body mass index and mortality among older people living in the community. J Am Geriatr Soc 47:1072
Audisio RA, Ramesh H, Longo W et al (2005) Preoperative assessment of surgical risk in oncogeriatric patients. Oncologist 10:262–268
Rubenstein LZ, Schairer C, Wieland GD, Kane R (1984) Systematic biases in functional status assessment of elderly adults: effects of different data sources. J Gerontol 39(6):686–691
Buccheri G, Ferrigno D, Tamburini M (1996) Karnofsky and ECOG performance status scoring in lung cancer: a prospective, longitudinal study of 536 patients from a single institution. Eur J Cancer 32A(7):1135–1141
Harpole DH Jr, Herndon JF 2nd, Young WG Jr et al (1995) Stage I nonsmall cell lung cancer: a multivariate analysis of treatment methods and patterns of recurrence. Cancer 76:787–796
Stamatis G, Djuric D, Eberhardt W et al (2002) Postoperative morbidity and mortality after induction chemoradiotherapy for locally advancer lung cancer: an analysis of 350 operated patients. Eur J Cardiothorac Surg 22:292–297
Ferguson MK, Vigneswaran WT (2008) Diffusing capacity predicts morbidity after lung resection in patients without obstructive lung disease. Ann Thorac Surg 85(4):1158–1164
O’Rourke MA, Feussner JR, Feigl P et al (1987) Age trends of lung cancer stage at diagnosis: implications for lung cancer screening in the elderly. JAMA 258:921–926
Mery CM, Pappas AN, Bueno R et al (2005) Similar long-term survival of elderly patients with non-small cell lung cancer treated with lobectomy or wedge resection within the Surveillance, Epidemiology, and End Results database. Chest 128:237–245
Weinmann M, Jeremie B, Toomes H et al (2003) Treatment of lung cancer in the elderly. Part I. Non-small cell lung cancer. Lung Cancer 39:233–253
Morandi U, Stefani A, Golinelli M et al (1997) Results of surgical resection in patients over the age of 70 years with non small-cell lung cancer. Eur J Cardiothorac Surg 11:432–439
Gail MH, Eagan RT, Feld R et al (1984) Prognostic factors in patients with resected state I non-small cell lung cancer: a report from the Lung Cancer Study Group. Cancer 54:1802–1813
Mountain CF, Lukeman JM, Hammar SP et al (1987) Lung cancer classification: the relationship of disease extent and cell type to survival in a clinical trials population. J Surg Oncol 35:147–156
Deslauriers J, Gregoire J (2000) Surgical therapy of early non-small cell lung cancer. Chest 117(suppl):104S–109S
Faulkner SL (2000) Is lobectomy the “gold standard” for stage I lung cancer in year 2000? Chest 118(suppl):119S
Bates M (1970) Results of surgery for bronchial carcinoma in patients aged 70 and over. Thorax 25:77–78
Evans EW (1973) Resection of bronchial carcinoma in the elderly. Thorax 28:86–88
Kirsh MM, Rotman H, Bove E et al (1976) Major pulmonary resection for bronchial carcinoma in the elderly. Ann Thorac Surg 22:369–373
Harviel JD, McNamara JJ, Straehley CJ (1978) Surgical treatment of lung cancer in patients over the age of 70 years. J Thorac Cardiovasc Surg 75:802–805
Ginsberg RJ, Hill LD, Eagan RT et al (1983) Modern thirty-day operative mortality for surgical resections in lung cancer. J Thorac Cardiovasc Surg 86:654–658
Mery CM, Jaklitch MT (2006) Lung resection in the elderly, correspondence. Chest 129:496–497
Albano WA (1977) Should elderly patients undergo surgery for cancer. Geriatrics 32:105–108
Breyer RH, Zippe C, Pharr WF et al (1981) Thoracotomy in patients over age seventy years: ten-year experience. J Thorac Cardiovasc Surg 81:187–193
Zapatero J, Madrigal L, Lago J et al (1990) Thoracic surgery in the elderly: review of 100 cases. Acta Chir Hung 31:227–234
Allen MS, Darling GE, Pechet TT et al (2006) ACOSOG Z0030 Study Group. Morbidity and mortality of major pulmonary resections in patients with early-stage lung cancer: initial results of the randomized, prospective ACOSOG Z0030 trial. Ann Thorac Surg 81(3):1013–1019
Decamp MM Jr, Jaklitsch MT, Mentzer SJ et al (1995) The safety and versatility of video-thoracoscopy: a prospective analysis of 895 cases. J Am Coll Surg 181:113–120
McKenna R (1994) Thoracoscopic lobectomy with mediastinal sampling in 80 year-old patients. Chest 106:1902–1904
Landreneau RL, Sugarbaker DJ, Mack MJ et al (1993) Postoperative pain-related morbidity: video-assisted thoracic surgery versus thoracotomy. Ann Thorac Surg 56:1285–1289
Jaklitsch MT, Bueno R, Swanson SJ et al (1996) Video-assisted thoracic surgery in the elderly: a review of 307 cases. Chest 110:751–758
Cattaneo SM, Park BJ, Wilton AS et al (2008) Use of video-assisted thoracic surgery for lobectomy in the elderly results in fewer complications. Ann Thorac Surg 85:231–236
Ginsberg RJ, Rubinstein LV (1995) Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann Thorac Surg 60(3):615–622, discussion 622–623
Landreneau RJ, Sugarbaker DJ, Mack MJ et al (1997) Wedge resection versus lobectomy for stage I (T1 N0 M0) non-small-cell lung cancer. J Thorac Cardiovasc Surg 113(4):691–700
Kulke MH, Mayer RJ (1999) Carcinoid tumors. N Engl J Med 340(11):858–868
Marty-Ane C, Costes V, Pujol J et al (1995) Carcinoid tumors of the lung: do atypical features require aggressive management? Ann Thorac Surg 59(1):78–83
Mezzetti M, Raveglia F, Panigalli T et al (2003) Assessment of outcomes in typical and atypical carcinoids according to latest WHO classification. Ann Thorac Surg 76(6):1838–1842
Jaklitsch MT, Mery CM, Lukanich JM et al (2001) Sequential thoracic metastasectomy prolongs survival by re-establishing local control within the chest. J Thorac Cardiovasc Surg 121(4):657–667
Inoue M, Ohta M, Iuchi K et al (2004) Benefits of surgery for patients with pulmonary metastases from colorectal carcinoma. Ann Thorac Surg 78(1):238–244
Weiser MR, Downey RJ, Leung DH, Brennan MF (2000) Repeat resection of pulmonary metastases in patients with soft-tissue sarcoma. J Am Coll Surg 191(2):184–190, discussion 190–191
Saito Y, Omiya H, Kohno K et al (2002) Pulmonary metastasectomy for 165 patients with colorectal carcinoma: A prognostic assessment. J Thorac Cardiovasc Surg 124(5):1007–1013
Pfannschmidt J (2003) Prognostic factors and survival after complete resection of pulmonary metastases from colorectal carcinoma: experiences in 167 patients. J Thorac Cardiovasc Surg 126(3):732–739
Carballo M, Maish M, Jaroszewski D, Holmes C (2009) Video-assisted thoracic surgery (VATS) as a safe alternative for the resection of pulmonary metastases: a retrospective cohort study. J Cardiothorac Surg 4(1):13
The International Registry of Lung Metastases, Writing Committee, Pastorino U et al (1997) Long-term results of lung metastasectomy: prognostic analyses based on 5206 cases. J Thorac Cardiovasc Surg 113(1):37–49
Collie DA, Wright AR, Williams JR et al (1994) Comparison of spiral-acquisition computed tomography and conventional computed tomography in the assessment of pulmonary metastatic disease. Br J Radiol 67(797):436–444
McCormack PM, Bains MS, Begg CB et al (1996) Role of video-assisted thoracic surgery in the treatment of pulmonary metastases: results of a prospective trial. Ann Thorac Surg 62(1):213–216
Reinhardt M, Wiethoelter N, Matthies A et al (2006) PET recognition of pulmonary metastases on PET/CT imaging: impact of attenuation-corrected and non-attenuation-corrected PET images. Eur J Nucl Med Mol Imaging 33(2):134–139
Nakajima J, Takamoto S, Tanaka M et al (2001) Thoracoscopic surgery and conventional open thoracotomy in metastatic lung cancer. Surg Endosc 15(8):849–853
Mutsaerts E, Zoetmulder F, Meijer S et al (2002) Long term survival of thoracoscopic metastasectomy vs metastasectomy by thoracotomy in patients with a solitary pulmonary lesion. Eur J Surg Oncol 28(8):864–868
Samet J, Hunt WC, Key C et al (1986) Choice of cancer therapy varies with age of patient. JAMA 255:3385–3390
Gridelli C, Langer C, Maione P et al (2007) Lung cancer in the elderly. J Clin Oncol 25(14):1898–1907
McGarry RC, Song G, des Rosiers P et al (2002) Observation-only management of early stage, medically inoperable lung cancer: poor outcome. Chest 121:1155–1158
Yellin A, Brenfield JR (1985) Surgery for bronchogenic carcinoma in the elderly. Am Rev Respir Dis 131:197
Arias E (2007) United States life tables, 2004. Natl Vital Stat Rep 56(9):1–39.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Billmeier, S.E., Jaklitsch, M.T. (2011). Pulmonary Surgery for Malignant Disease in the Elderly. In: Rosenthal, R., Zenilman, M., Katlic, M. (eds) Principles and Practice of Geriatric Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4419-6999-6_48
Download citation
DOI: https://doi.org/10.1007/978-1-4419-6999-6_48
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4419-6998-9
Online ISBN: 978-1-4419-6999-6
eBook Packages: MedicineMedicine (R0)