
Abstract
Over the past three decades, China, the world’s most populous country whose population accounts for one-fifth of the global population, has enjoyed impressive economic developments. People in China have experienced many dramatic changes in their lifestyles thanks to the increases in family income and availability of food as a result of China’s economic reform and the growing global trade (CSSB 2008). Meanwhile, people’s lifestyles are becoming more sedentary compared to decades ago. Compared to other groups, children and adolescents are likely to be affected to a greater extent by these changes, partially due to China’s family planning policy, the so called “one child policy” initiated in the later 1970s, which enables parents and grandparents to provide their children with more resources and care.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Gross Domestic Product
- Childhood Obesity
- Total Medical Cost
- Gross Domestic Product Growth Rate
- Combine Prevalence
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Over the past three decades, China, the world’s most populous country whose population accounts for one-fifth of the global population, has enjoyed impressive economic developments. People in China have experienced many dramatic changes in their lifestyles thanks to the increases in family income and availability of food as a result of China’s economic reform and the growing global trade (CSSB 2008). Meanwhile, people’s lifestyles are becoming more sedentary compared to decades ago. Compared to other groups, children and adolescents are likely to be affected to a greater extent by these changes, partially due to China’s family planning policy, the so called “one child policy” initiated in the later 1970s, which enables parents and grandparents to provide their children with more resources and care.
Some recent studies, predominately published in Chinese, suggest that the prevalence of obesity has increased in China both in children and adults as well as the related chronic diseases (Ji and Working group on Obesity in China (WGOC) 2007; Ma et al. 2005; Mi et al. 2006; Wang et al. 2007). Nationally representative survey data show that between 1992 and 2002, the prevalence of overweight and obesity increased in all sex and age groups, and in all geographic areas. Using the World Health Organization (WHO) body mass index (BMI) cut points, among adults in China, the combined prevalence of overweight and obesity (BMI ≥ 25 kg/m2) increased from 14.6 to 21.8% during this period, while based on the Chinese standard (BMI ≥ 24 kg/m2), it increased from 20.0 to 29.9%. With the increase in obesity, obesity- and diet-related chronic diseases such as hypertension, Cardiovascular disease (CVD), and type 2 diabetes also increased over the past decade and became the most important preventable cause of death. For example, the prevalence of hypertension increased from 14.4% in 1991 to 18.8% in 2002 in adults (Wang et al. 2007). On the other hand, data collected from pre-school children show that undernutrition remains a major public health concern, particularly in poor and rural areas (Liu et al. 2008). Therefore, China is facing a double burden of both, an overnutrition and an undernutrition problem.
This chapter describes the current situation and the time trends of overweight and obesity among children and adolescents in China. We focused on representative data collected in large national surveys and results that are based on the recently released Chinese BMI reference (Ji and Working Group on Obesity in China (WGOC) 2005).
China’s Socio-demographic and Economic Characteristics
China is the largest developing country with the fastest growing economy in the world (World Bank 2009; Wikipedia 2009) (see Table 11.1). China has about one-fifth of the global population. China’s economy during the past 30 years has changed from a centrally planned system that was largely closed to international trade to a more market-oriented economy that has a rapidly growing private sector. China’s Gross Domestic Product (GDP) has increased by more than tenfold since 1978, and China contributed one-third of global economic growth in 2004. In 2008, China’s economy is the second largest in the world after that of the United States with a GDP of $7.8 trillion when measured on a purchasing power parity (PPP) basis. China has been the fastest-growing major nation for the past three decades with an average annual GDP growth rate above 10% since China initiated its economic reform in the late 1970s. Nevertheless, at present, China remains a low-to-medium income country.
Thanks to China’s fast per capita income increase, an average annual rate of more than 8% over the last three decades, and the government’s strong support for poverty reduction programs, poverty rate in China has drastically decreased. China alone accounted for over 75% of poverty reduction in the developing world over the last 20 years. On the other hand, this rapid economic growth has been accompanied by rising income inequalities.
China’s economic reforms and development over the last three decades have also resulted in substantial improvements in people’s daily life and in human development indicators. Adult illiteracy rate fell from 37% in 1978 to less than 10% in 2005; and, indicative of health indices, the infant mortality rate fell from 41 per 1,000 live births in 1978 to 23 in 2005. Life expectancy has increased to 73.2 years by 2008. China enforced its “one child” policy since the late 1970s, as a result, Chinese children are enjoying more family resources and care than their early counterparts, and China is now one of the most rapidly aging countries in the world.
The two most important sectors of the Chinese economy have traditionally been agriculture and industry, which together employ more than 70% of the labor force and produce more than 60% of GDP. The two sectors have differed in many respects, and affect people’s life differently. For example, technology, labor productivity, and incomes have advanced much more rapidly in industry than in agriculture. These disparities between the two sectors have resulted in an economic-cultural-social gap between the rural and urban areas, a major division in Chinese society, where in general, most urban residents have enjoyed better living standards and further improvements over the past two decades. It is estimated that more than 204 million Chinese, many in remote and resource-poor areas in the western and interior regions, still suffer from poverty, often without access to clean water, arable land, or adequate health and education services.
Classification of Obesity in Children and Adolescents in China
BMI is a simple and widely used method for estimating body fat mass and has been widely accepted as a useful measurement for overweight and obesity classification in both adult and child population (WHO 2000, 2004). However, different cut points for the classification of childhood obesity have been used across populations and studies and several international references have been developed and recommended for use (Cole et al. 2000; Kuczmarski et al. 2002). It is argued that the WHO BMI cut points are developed primarily based on data collected in Western populations, and may not be appropriate for some population groups such as some in the Asia Pacific areas (Misra 2003; WHO 2004; WHO, IASO, & IOTF 2000).
In China, for adults, BMI cut points of 24 (for overweight) and 28 (for obesity), lower than the WHO standard, have been recommended and used (Wang et al. 2007; Zhou and Cooperative Meta-Analysis Group of the Working Group on Obesity in China 2002). These Chinese BMI cut points were developed based on analysis of data collected from 239,972 Chinese adults in the 1990s. A BMI cut point of 24 was found having the best sensitivity (=62.07% for men and 63.15% for women) and specificity (=63.85% for men and 62.13% for women) for identifying health conditions including hypertension, diabetes and dyslipidaemia, while a BMI of 28 had a specificity around 90% (Zhou and Cooperative Meta-Analysis Group of the Working Group on Obesity in China 2002).
To define childhood obesity and for screening overweight and obesity in school-age children (7–18 years old), in 2004, the Working Group on Obesity in China (WGOC) published a national reference, which is a set of sex-age-specific BMI cut points (Table 11.2 and Fig. 11.1) (Ji and Working Group on Obesity in China (WGOC) 2005). Overall these BMI cut points are lower than those in the US CDC 2000 Growth Charts. The WGOC BMI reference was developed based on anthropometric data (height and weight) collected in the 2000 Chinese National Survey on Students Constitution and Health (CNSSCH) from 216,620 subjects aged 7–18 years old in 30 of China’s 31 provinces (except for Taiwan). For children younger than 7 years old, the WGOC recommended to use the WHO’s weight-for-height z-score (WHZ) standard 2 ≤ WHZ < 3 for overweight and ≥3 for obesity. Figure 11.1 shows that compared to their US counterparts, Chinese children and adolescents remain thinner; and the BMI cut points recommended in China are lower that the US 2000 CDC Growth Charts, but the differences become greater at older ages. The present chapter focused on results based on the Chinese WGOC BMI reference.

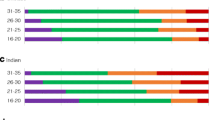
Comparison of age-specific BMI percentiles in China (the 2002 national survey [The 2002 China National Health and Nutrition Survey, the 85th percentile was not provided.]), the US CDC 2000 Growth Chart, and the Chinese/WGOC BMI reference for classification of overweight and obesity in girls. ^The Chinese reference only covers school age children aged 7–17 years old. WGOC Working Group on Obesity in China (Ji and Working Group on Obesity in China (WGOC) 2005)
The Prevalence and Trends of Childhood Obesity in China
Good nationally representative data have been collected in China allowing for examining the time trend in childhood obesity. Many additional nationwide, regional and local surveys have been conducted recently and provide additional important information. The 2002 China National Health and Nutrition Survey provides the best, most recent national estimates, and shows that the combined prevalence of overweight and obesity in children aged 0–18 years was 4.1 and 2.1%, respectively. While in urban areas, among school-age children (≥7 years), the combined prevalence was 12.9%. A most recent study shows that in northern coastal big cities, the combined prevalence had reached 32.5% in boys and 17.6% in girls (both ≥7 years) in 2005 (Ji and Cheng 2008), which is similar to that in some industrialized countries (Wang and Lobstein 2007).
Time Trends in the Prevalence of Childhood Obesity
Table 11.3 shows that the prevalence of obesity and overweight has increased between 1992 and 2002 in all sex and age groups. The nationwide combined prevalence increased by 31.7% from 3.9% in 1992 to 5.4% in 2002 in pre-school children (up to age 6), and increased by 17.9% from 5.7% in 1992 to 6.6% in 2002 in school-age children (7–17 years).
Table 11.4 shows the trends based on data collected in another series of representative cross-sectional surveys in metropolitan areas in China, the health examination data collected among elementary and secondary school students. The surveys have been conducted every 5 years since 1985 by the Chinese National Survey on Students Constitution and Health Association. In the metropolitan areas, the prevalence of overweight and obesity in boys and girls have increased remarkably, approximately by 10 times. The combined prevalence increased from 1.4% in 1985 to 17.1 in 2000 in boys, more rapidly than that in girls (from 1.5 to 9.7%).
The available data show large disparities between regions and groups, even among urban areas. In major cities, during recent years, the prevalence of childhood obesity has increased more dramatically than in inland cities. For example, in Shanghai and Beijing, the two largest cities in China, the prevalence has more than tripled between 1985 and 1995. The prevalence in 7–12-year-old boys in these two cities increased from 5.4 to 5.8 to 29.0% in 2000. In inland cities, the figure increased from 0.6 to 11.8% (see Table 11.5).
Sex and Age Differences
Overall, the national average prevalence was comparable in boys and girls among pre-school age children, but was higher in boys than in girls in school-age children (e.g., Table 11.3). Similarly, in metropolitan areas, it was much higher (almost doubled) in boys than that in girls in these age groups (e.g., Tables 11.4 and 11.5).
Urban and Rural Differences
Similar to the situation in some other developing countries, there are large urban-rural differences in the prevalence of overweight and obesity in China, and the prevalence in urban areas is higher, in particular in school-age children (Table 11.6). Our calculated urban to rural ratio indicates that almost all of the prevalence is higher in urban than rural areas, except for the prevalence of obesity in pre-school girls. In addition, urban boys and girls have higher mean BMI compared to their rural counterparts (Fig. 11.2). These are based on the 2002 China Nutrition and Health Survey data. Note that most major cities in China have both urban and rural residents. For example, Beijing includes urban (inside the city) and rural areas (city surrounding areas). In China, usually people living in urban areas have better living standards, higher income, and more government-supported benefits such as retirement and healthcare than rural residents.

Mean BMI in children aged 2–18 years old, by sex and urban-rural residence: the 2002 China Health and Nutrition Survey (data sources: Ma et al. 2005)
The Main Factors That Have Contributed to the Increase in Obesity in China
Obesity is believed to be the result of a number of biological, behavioral, cultural, social, and environmental factors and the complex interactions between them that promote a positive energy balance (Bray 1998; Davison and Birch 2001; WHO 2000). It is argued that the rapid increase in the prevalence of obesity worldwide over the past two decades probably suggests that environmental factors, but not genetic factors, are the major risk factors, because genetic factors cannot change so dramatically within such a short period (Hill and Peters 1998).
The rapid increase in the prevalence of overweight and obesity and the large disparities between population groups and regions in the prevalence and secular trends in China are particular a result of the rapid economic development and shifts in people’s lifestyles and the differences in these shifts over the past two decades. Higher levels of parental education and family income have been found as significant risk factors for childhood obesity in China (Xie et al. 2007). The following highlights several such indicators and gives examples. China’s per capita GDP has increased dramatically in the past two decades (Fig. 11.3). On one hand, this results in a steady increase in family income and improvements in people’s living standards. On the other hand, this may have a number of unintended consequences such as shift in people’s lifestyles.

Time trends in per capita gross domestic product (GDP, Chinese yuan) in China: 1978–2006 (data sources: CSSB 2008)
Chinese citizens have experienced many dramatic changes in their lifestyles, including dietary intake and physical activity. The Chinese diet has shifted from a traditional dietary pattern, which typically contains quantities of plant foods including grains and vegetables, to the Western dietary pattern characterized by high intakes of meats, fat, and sugar (Du et al. 2004; Zhai et al. 2007). Nationally representative data show that the consumption of animal foods and dairy products have increased, while plant foods, including grains, fruit, and vegetable has steadily decreased, especially in urban areas. Consumption of cooking oil increased dramatically, especially of plant cooking oil (Fig. 11.4). The Western fast food industry has marketed aggressively in China, and Western fast food (which remains much more expensive than local food) and locally marketed and produced similar high-fat and energy-dense food are becoming an important part of urban children’s diet. Often, parents and grandparents reward their children with meals at McDonald’s (e.g., Jing 2000). Based on a recent report, by 2008, KFC has more than 2,200 outlets in some 450 cities and McDonald’s has 950 outlets in China. Other Western fast food companies are entering the Chinese market more aggressively. For example, in April 2008 Burger King had just 12 outlets in mainland China, but soon the company announced plans to open between 250 and 300 outlets in China over the next 5 years (Economist 2008).

Trends in food consumption (g/day per reference man) in China: 1982, 1992 and 2002. The 1982, 1992, and 2002 China National Health and Nutrition Survey. Reference man refers to adult men with light to medium physical activity (data source: Zhai et al. 2007)
Changes in China have also contributed to the growing sedentary lifestyle among children in China. Among these changes, the major shifts include: first, children’s greatly declined involvement in household work or farm work for children living in rural areas compared to the older cohorts, which are contributed by the one-child policy, shifts in parents’ occupation, parents’ higher expectation and the growing competition for students’ academic performance, and the increasing availability and use of labor-saving devices at home such as washing machines (Fig. 11.5). For example, increased household ownership of a washing machine leads to less energy expenditure in housework. Second, children’s screen time, such as time spent on watching television, playing computer and video games, has increased. For example, the television ownership increased from 17.2 per 100 urban households in 1985 to 134.8 to 2005 (Fig. 11.5). Third, changes in the means and options of transportation. For example, during recent years, much fewer young people ride bicycles or walk to schools, while more enjoy more convenient public transportation system, taxi, family-owned motorcycles and automobiles when travel. China’s Bureau of Statistics started to include urban household automobile ownership in its yearly statistical books published since 1999. Urban household automobile ownership had increased by 1,160 times between 1999 and 2006 (Fig. 11.5). One study shows that 14% of the Chinese households acquired a motorized vehicle between 1989 and 1997. Another study shows that the odds of being obese were 80% higher for adults in households that own a motorized vehicle, compared to those that do not (Bell et al. 2002).

Trends in household ownership of color television, washing machine, automobile (in urban areas) in China: sets/per 100 households (data sources: CSSB 2008)
Discussion and Conclusions
China has experienced many rapid economic and social developments and changes over the past three decades. These have resulted in a number of major shifts in people’s lifestyles, most of which have contributed to overconsumption of foods but reduced physical activity. Thus, no wonder, we are seeing a rapidly growing obesity epidemic in China. Recent data show that nationwide the average prevalence of overweight and obesity has reached 30% in adults, approximately 6–7% in children, while in major cities, the prevalence has reached over 50% in adults and approximately 20% in children (Ji and Working group on Obesity in China (WGOC) 2007; Mi et al. 2006; Wang et al. 2007).
Childhood obesity could track into adulthood and has a lot of health and financial consequences, for example, to increase the risks for hypertension, type 2 diabetes, coronary heart disease, and stroke, and increase healthcare costs. A recent study estimated that the total medical cost attributable to overweight and obesity was estimated at 21.11 billion Chinese Yuan (RMB, approximately US$2.74 billion), which accounted for 25.5% of the total medical costs for the four major obesity-related chronic diseases namely hypertension, type 2 diabetes, coronary heart disease and stroke, or 3.7% of China’s national total medical costs in 2003 (Zhao et al. 2008). The researchers warned that the medical cost associated with overweight and obesity could increase to 37 billion Chinese Yuan (RMB, approximately US$4.8 billion), a 75% increase, if the epidemic developed speedily and the ratio of the prevalence of overweight to obesity approached 1.1:1. The study was based on the 2003 Third National Health Services Survey data from a large sample of 143,521 subjects, to derive direct medical costs including costs for outpatient visits, physician services, inpatient stays, rehabilitation services, nursing fees and medications. Recently another study warned that the economic costs related to the nutrition transition, in particular, the changing dietary and physical activity patterns and increase in obesity and overweight in China, may represent 4 to 8% of China’s economy (Popkin 2008).
The United States can serve as an example to indicate the seriousness of the financial consequences of the obesity epidemic, and to show that the warnings made recently for China can become true if its growing obesity epidemic could not be controlled effectively. One of our recent studies projected that in the United States, medical costs attributable to overweight and obesity have already reached 72 to 82 billion US dollars and accounted for 12 to 13% of total US healthcare costs. The total healthcare costs attributable to obesity/overweight would double every decade to 860.7 to 956.9 billion US dollars by 2030, accounting for 16 to 18% of total US healthcare costs, if the obesity trend continues in the US (Wang et al. 2008a, b).
China already has had the largest number of overweight and obese people on earth. Timely attention and adequate effort should be made to prevent childhood obesity and to address the rapidly growing obesity epidemic in China. Comprehensive, national programs should be developed, in particular, while today China is making great effort and investing heavily to improve her citizen’s health and access to healthcare service (e.g., the Healthy China 2020 Program). Multiple parties such as parents, children, health professionals, schools, media, food industry, and the central and local government agencies should all be involved for promoting healthy lifestyles and for the prevention of obesity. China should learn from the failure and successful experience of other countries in combating the obesity epidemic. Although there are many challenges for obesity prevention in China as the nation is facing many other public health challenges, there are emerging promising signs in this effort. For example, the work of the Working Group on Obesity in China has increased the attention of the general public and related health professionals on the obesity problem, the importance of using standardized references for classification as well as the screening of overweight and obesity among children and adults in China. Recently, in 2007 the Chinese State Council endorsed a report for child and adolescent health improvement, which recommended that every student should have at least 1h of physical activity each day in school.
References
Bell, A.C., Ge, K., & Popkin, B.M. (2002). The road to obesity or the path to prevention: motorized transportation and obesity in China. Obesity Research, 10, 277–283.
Bray, G.A. (1998). Obesity: a time bomb to be defused. Lancet, 352, 160–161.
Central Intelligence Agency (CIA) (2009). People’s Republic of China. https://www.cia.gov/library/publications/the-world-factbook/geos/ch.html (assessed March 9, 2009).
China State Statistics Bureau (CSSB) (2008). China statistical yearbook 2002 to 2008. Beijing: China Statistics Press (in Chinese).
Cole, T.J., Bellizzi, M.C., Flegal, K.M., & Dietz, W.H. (2000). Establishing a standard definition for child overweight and obesity worldwide: international survey. British Medical Journal, 320, 1240–1243.
Davison, K.K., & Birch, L.L. (2001). Childhood overweight: a contextual model and recommendations for future research. Obesity Reviews, 2, 159–171.
Du, S., Mroz, T.A., Zhai, F., & Popkin, B.M. (2004). Rapid income growth adversely affects diet quality in China – particularly for the poor! Social Science & Medicine, 59, 1505–1515.
Economist (2008). Fast food in China: here comes a whopper – the world’s second largest burger chain is gearing up in China (February 10, 2009); http://www.economist.com/business/displaystory.cfm?story_id=12488790.
Hill, J.O., & Peters, J.C. (1998). Environmental contributions to the obesity epidemic. Science, 280, 1371–1374.
Ji, C.Y., & Cheng, T.O. (2008). Prevalence and geographic distribution of childhood obesity in China in 2005. International Journal of Cardiology, 131, 1–8.
Ji, C.Y., & Working Group on Obesity in China (WGOC). (2005). Report on childhood obesity in China (1): body mass index reference for screening overweight and obesity in Chinese school-age children. Biomedical and Environmental Sciences, 18, 390–400.
Ji, C.Y., & Working group on Obesity in China (WGOC). (2007). Report on childhood obesity in China (4) prevalence and trends of overweight and obesity in Chinese urban school-age children and adolescents, 1985–2000. Biomedical and Environmental Sciences, 20, 1–10.
Ji, C.Y., & Working Group on Obesity in China (WGOC). (2008). The prevalence of childhood overweight/obesity and the epidemic changes in 1985–2000 for Chinese school-age children and adolescents. Obesity Reviews, 9, Suppl 1, 78–81.
Jing, J. (2000). Feeding China’s little emperors: food, children, and social change. Stanford: Stanford University Press.
Kuczmarski, R.J., Ogden, C.L., & Guo, S.S. (2002). 2000 CDC growth charts for the United States: methods and development. National Center for Health Statistics. Vital and Health Statistics, Series 11, 246, 1–190.
Liu, A., Zhao, L., Yu, D., & Yu, W. (2008). Study on malnutrition status and changing trend of children under 5 years old in China. Wei Sheng Yan Jiu, 37, 324–326 (in Chinese).
Ma, G.S., Li, Y.P., Wu, Y.F., Zhai, F.Y., Cui, Z.H., Hu, X.Q., Luan, D.C., Hu, Y,H., & Yang, X.G. (2005). The prevalence of body overweight and obesity and its changes among Chinese people during 1992 to 2002. Chinese Journal of Preventive Medicine, 39, 311–315 (in Chinese).
Mi, J., Cheng, H., Hou, D.Q., Duan, J.L., Teng, H.H., & Wang, Y.F. (2006). Prevalence of overweight obesity among children and adolescents in Beijing in 2004. Zhonghua Liu Xing Bing Xue Za Zhi, 27, 469–474 (in Chinese).
Misra, A. (2003). Revisions of cutoffs of body mass index to define overweight and obesity are needed for the Asian-ethnic groups. International Journal of Obesity and Related Metabolic Disorders, 27, 1294–1296.
Ng, S.W., Zhai, F., & Popkin, B.M. (2008). Impacts of China’s edible oil pricing policy on nutrition. Social Science & Medicine, 66, 414–426.
Popkin, B.M. (2008). Will China’s nutrition transition overwhelm its health care system and slow economic growth? Health Affairs, 27, 1064–1076.
Wang, Y. (2004). Epidemiology of childhood obesity – methodological aspects and guidelines: what’s new? International Journal of Obesity, 28, 21–28.
Wang, Y., & Lobstein, T. (2007). Worldwide trends in childhood obesity. International Journal of Pediatric Obesity, 1, 11–25.
Wang, Y., Beydoun, M.A., Liang, L., Caballero, B., & Kumanyika, S.K. (2008a). Will all Americans become overweight or obese? Estimating the progression and cost of the US obesity epidemic. Obesity, 16, 2323–2330.
Wang, Z., Zhai, F., Du, S., & Popkin, B. (2008b). Dynamic shifts in Chinese eating behaviors. Asia-Pacific Journal of Clinical Nutrition, 17, 123–130.
WHO (2000). Obesity: preventing and managing the global epidemic. Report of a WHO consultation. WHO Technical Report Series, No. 894, Geneva.
WHO (2004). WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet, 363, 157–163.
WHO, IADO, & IOTF (2000). The Asia-Pacific perspective: redefining obesity and its treatment (December 20, 2001); http://www.asso.org.au/profiles/profs/reportsguides/obesity/371.
Wikipedia (2009). Economy of the People’s Republic of China. http://en.wikipedia.org/wiki/Economy_of_the_People’s_Republic_of_China (assessed March 9, 2009).
World Bank (2009). Country brief – China. http://web.worldbank.org/WBSITE/EXTERNAL/COUNTRIES/EASTASIAPACIFICEXT/CHINAEXTN/0,,menuPK:318960∼pagePK:141132∼piPK:141107∼theSitePK:318950,00.html (assessed March 9, 2009).
Xie, B., Chou, C., Spruijt-Metz, D., Reynolds, K., Clark, F., Palmer, P.H., Gallaher, P., Sun, P., Guo, Q., & Johnson, C.A. (2007). Socio-demographic and economic correlates of overweight status in Chinese adolescents. American Journal of Health Behavior, 31, 339–352.
Yang, G., Kong, L., Zhao, W., Wan, X., Zhai, Y., Chen, L.C., & Koplan, J.P. (2008). Emergence of chronic non-communicable diseases in China. Lancet, 372, 1697–1705.
Yang, X., & Zhai, F. (2006). Report of the 2002 Chinese National Nutrition and Health Survey (3rd Report) (pp. 87–88). Beijing: People’s Health Press.
Zhai, F., Wang, H., Du, S., He, Y., Wang, Z., Ge, K., & Popkin, B.M. (2007). Lifespan nutrition and changing socio-economic conditions in China. Asia-Pacific Journal of Clinical Nutrition, 16, Suppl 1, 374–382.
Zhao, W., Zhai, F., Hu, J., Wang, J., Yang, Z., Kong, L., & Chen, C. (2008). Economic burden of obesity-related chronic diseases in Mainland China. Obesity Reviews, 9, Suppl 1, 62–67.
Zhou, B.F., & Cooperative Meta-Analysis Group of the Working Group on Obesity in China (2002). Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults – study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomedical and Environmental Sciences, 15, 83–96.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Wang, Y., Mi, J., Tao, Y., Chen, P. (2011). Epidemiology of Obesity in Children and Adolescents in China. In: Moreno, L., Pigeot, I., Ahrens, W. (eds) Epidemiology of Obesity in Children and Adolescents. Springer Series on Epidemiology and Public Health, vol 2. Springer, New York, NY. https://doi.org/10.1007/978-1-4419-6039-9_11
Download citation
DOI: https://doi.org/10.1007/978-1-4419-6039-9_11
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4419-6038-2
Online ISBN: 978-1-4419-6039-9
eBook Packages: MedicineMedicine (R0)