
Abstract
Although the routes of transmission and infectivity differ, the three blood borne infections with most impact on public health are caused by viruses that can cause chronic asymptomatic infections. Human immunodeficiency virus (HIV) is discussed in Chapter 3.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Although the routes of transmission and infectivity differ, the three blood borne infections with most impact on public health are caused by viruses that can cause chronic asymptomatic infections. Human immunodeficiency virus (HIV) is discussed in Chapter 3. Here we discuss hepatitis B virus (HBV) and hepatitis C virus (HCV). HBV and HCV are grouped together for certain similarities (both causing hepatitis , hence the name, both caused by a virus , and both can lead to chronic asymptomatic infections and liver disease ) but the differences are prominent enough to warrant separate presentations. Some of the main similarities and differences are listed in Table 19.1. Other hepatitis viruses include hepatitis A virus and hepatitis E virus that are both feco-orally transmitted. The hepatitis D virus, commonly called deltavirus, occurs only as a superinfection in persons with active HBV infection. Without laboratory testing, different causes of hepatitis cannot be distinguished.
1.1 Prevalence
A single blood borne exposure (e.g., through a needle stick injury) to HBV leads to acute infection in an estimated 3–30% of cases and exposure to HCV in 1–10% of cases as compared to HIV where the proportion of infections is 0.3%. Sexually, HBV is transmitted ten times more effectively than HIV (Kingsley et al. 1990). For HBV countries are classified as areas of low, middle, and high endemicity, whereas the distribution of HCV equally shows regional variations but these are more focal. In areas of low endemicity for HBV import through migration is the major contributor to prevalence. For HCV in low-endemic countries, injecting drug use (IDU) is the major mode of HCV transmission , and migration contributes to a lesser extent to HCV prevalence.
For both HBV and HCV, the overall prevalence can be ascertained by population-based sero-epidemiological studies. Data of donor screening is often used to estimate the overall prevalence. However, as high-risk groups are excluded from donating blood and donor inclusion criteria differ across countries, this data refers to a highly selected subpopulation. Some countries have antenatal screening for HBV in order to identify newborns at increased risk. Although pregnant women are a selected subpopulation as well, this screening may provide a more representative source. Incidence data on reported acute infections are of limited value for assessing the prevalence as most HBV and practically all HCV infections in the acute phase are asymptomatic and therefore undiagnosed. Moreover, using the long-term sequelae of HBV and HCV (i.e., liver cirrhosis, fibrosis, and carcinoma) based on clinical data to estimate the prevalence is difficult as the results of serological tests are often not included in morbidity and mortality registries.
These factors hinder efforts in determining HBV and HCV prevalence. However, for both infections valid data are needed as they should guide public health measures, either directed at specific high-risk groups (e.g., screening and early treatment) or the population (e.g., universal vaccination against HBV).
1.2 Prevention
As for most blood borne infections, undiagnosed individuals are a reservoir and a predominant source of new infections. Primary prevention of HBV and HCV is therefore directed at hygienic precautions in all percutaneous procedures and, for HBV, at promoting condom use and less risky sexual behavior. As there is a safe and effective vaccine available against HBV, vaccination is the most important public health measure in primary prevention. There is no vaccine available that prevents HCV infection. For both HBV and HCV, early diagnosis (only established through blood tests) and treatment of infectious individuals reduce the background prevalence of chronic infections and thus contribute to primary prevention. Concomitant source and contact tracing has additional benefits in the case of the 30% symptomatic acute HBV infections (identifying asymptomatic sources and preventing new symptomatic infections), but has limited value in HCV where new infections often go undiagnosed and infection is identified long after exposure.
Whilst treatment of HBV and HCV previously relied only on immune modulation, in the last decade new antivirals have been developed against both viruses. Treatment success has increased and will further increase when new and combined antiviral drugs become available.
In this chapter, we will describe the public health importance of these two silent killers HBV and HCV, which annually cause more deaths than HIV in high-income countries. We clarify the main epidemiological methods and obstacles in public health prevention and control of these infections.
2 Hepatitis B
2.1 Epidemiology
2.1.1 Global Patterns and Transmission Routes
HBV is of major public health importance due to its high burden of disease and its preventability. An estimated 360 million people worldwide have chronic HBV infection , and 600,000 deaths occur each year due to HBV-related liver disease or hepatocellular carcinoma (Shepard et al. 2006). HBV is transmitted by percutaneous or permucosal exposure to blood or body fluids from infected persons. Transmission usually takes place either through sexual contact , blood contact, or perinatally. Perinatal transmission is highly efficient (the major route in Southeast Asia), with the highest risk in children born to HBeAg positive mothers (Beasley et al. 1977). HBV is also transmitted within households to young children through close non-sexual contact (the major route in Africa) (Davis et al. 1989).
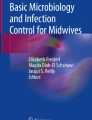
Since the age of HBV acquisition is inversely associated with the risk of becoming chronically infected, infections acquired in infancy or childhood contribute disproportionally to the pool of chronic carriers . The lifetime infection risk varies dramatically between 0.4% in Western Europe to 90% in East Asia , and is usually described in three groups (Fig. 19.1) (Shepard et al. 2006).

Geographical distribution of HBV endemicity. Source: World Health Organization (2001) Introduction of hepatitis B vaccine into childhood immunization services, Geneva, WHO, WHO/V&B/01.31
2.1.2 Risk Groups
The prevalence of HBV in a country is associated with its predominant transmission modes and the duration and quality of its vaccination strategy. In countries with high prevalence (HBsAg seroprevalence ≥8%), most infections are acquired perinatally or in early childhood (Shepard et al. 2006). In these countries, health-care associated HBV transmission is also frequent (Hauri et al. 2004). In low prevalence countries (HBsAg seroprevalence <2%) most infections are acquired through adult risk behavior including IDU and male homosexual contact (Hahné et al. 2004). Other groups with increased risk for acquiring HBV include infants born to infectious mothers, health-care workers , children with developmental disabilities , patients undergoing hemodialysis, and close contacts of infected people. Long-term travelers to endemic areas are generally also advised to be vaccinated (Salisbury et al. 2006).
Within low prevalence countries, one can distinguish subgroups with relatively high prevalence and incidence, with associated transmission patterns including frequent perinatal and household transmission (Aweis et al. 2001; Hahné et al. 2003; Hurie et al. 1992). These subgroups can be indigenous or arise through migration from endemic areas . For public health management of HBV, it is important that surveillance distinguishes between transmission occurring within a country (local transmission) and infections imported by immigration of carriers (imported infections). Whereas the former can be influenced by a country’s vaccination policy, the latter cannot.
2.2 Molecular Epidemiology
Hepatitis B virus belongs to the family of hepadnaviridae . It has a small double-stranded circular DNA genome of around 3200 base pairs , which encodes seven viral proteins . HBV is an unusual DNA virus as it replicates through an RNA intermediate which is transcribed back into cDNA using reverse transcriptase . This process is prone to errors, leading to a higher than usual mutation rate for DNA viruses and to diversification of the virus. However, as over half of the genome consists of overlapping open reading frames ; most errors result in viruses with reduced fitness. The diversification does allow tracking of virus transmission. In addition, it also has consequences for the prevention, diagnostic methods, natural history, and treatment of HBV infections (Echevarria and Avellon 2006; Lok and McMahon 2007).
The earliest grouping of HBV types made was based on variants of its surface protein (HBsAg), determined by the antigens present in the HBsAg (Courouce et al. 1976). Antigen a is common to all known HBsAg subtypes. Since it is the main epitope recognized by neutralizing antibodies arising through infection or vaccination, vaccine protection is not subtype specific. Next to a, there are two pairs of mutually exclusive antigens (d/y and w/r ), whereby w can exist in four forms (1–4). This results in subtypes such as “adw4” and “ayr.”
Subsequent to the description of HBsAg subtypes, eight genotypes (A–H) have been identified based on genome sequencing of HBV strains (Norder et al. 2004). The genotype grouping does not overlap with the HBsAg subtype grouping, although some correlations can be found. Within genotypes A, B, C, D, and F, but not (yet) in E, G, and H, subgenotypes have been identified. The occurrence of the HBsAg- and geno(sub)types varies geographically, which allows tracking virus transmission and population movement between regions (Echevarria and Avellon 2006; Norder et al. 2004).
Within almost all groups of hepatitis B virus (sub)types, mutants have been described according to where the mutation has occurred (pre-Core, Core, HBsAg). These mutations can have important implications for public health: They can interfere with the effectiveness of (passive and active) immunization and treatment, and can also affect the sensitivity of diagnostic assays (Echevarria and Avellon 2006). For example, a viable one point mutation in the pre-core region results in virus that cannot produce a particular protein that is traditionally used as a marker for viral load (the HBe protein ). This can result in infectious individuals at risk of severe disease being missed (Omata et al. 1991). Although this is a diagnostic challenge, its public health impact has (so far) been limited.
Surveillance of HBV’s diversity and its implications is therefore a key component of the public health response to HBV.
In addition to the study of subgroups of HBV and their characteristics, the relatedness of individual viruses can be studied in more detail using phylogenetics (see Chapter 7). The phylogenetic resolution depends on the length and specific part of the HBV genome that is sequenced (Boot et al. 2008). Phylogenetic analyses that integrate epidemiological information (such as risk behavior, country of origin) have become a powerful tool to assess the intensity of HBV transmission within and between high-risk groups (van Steenbergen et al. 2002), to identify outbreaks (Fisker et al. 2006), and to evaluate the effectiveness of vaccination programs (van Houdt et al. 2007).
Recent molecular epidemiological analysis suggests that in the Netherlands men who have sex with men (MSM) are the predominant high-risk group, with ongoing local transmission reflected by the very close relatedness of genotype A strains from MSM. In contrast, among heterosexually acquired HBV, sequences show a wide variation suggesting that they result from multiple introductions (by chronic carriers that moved from endemic areas and, to a lesser extent, by returning travelers) rather than from sustained transmission in a core-group of high-risk individuals. Based partly on these findings, it was decided, in the Netherlands, to intensify vaccination of MSM but to cease the free vaccination offer for heterosexuals with high rates of partner change. HBV transmission among heterosexuals may be prevented more effectively by screening (some groups of) immigrants and vaccination of their contacts. Since treatment of HBV has improved, secondary prevention is becoming more important (Hutton et al. 2007), not only to prevent morbidity for the individual patient but also to eliminate the patient as a source for others.
2.3 Clinical Course
2.3.1 Diagnostics
The immune reaction determines the clinical course of HBV infection. An inadequate, but persistent, immune response can lead to chronic infection. Testing of antibodies against hepatitis B proteins (anti-HBc, anti-HBs, anti-HBe) and antigens (HBsAg, HBeAg) are thus the means of diagnosing the stage of hepatitis B infection. Table 19.2 presents the most common course of occurrence of antigens and antibodies after infection. Additional testing of liver enzymes , with liver biopsy for histological classification, if justified, is required for clinical follow-up in chronic infection. HBV-DNA by PCR can quantify the viral load and classify infectiousness and therapeutical effect.
2.3.2 Immunological Reactions
There are important clinical differences (with epidemiological consequences) between acute and chronic HBV infection . Acute infection can lead to acute (infectious) disease, lasting several weeks or months. Acute hepatitis B in adults is usually self-limiting, but 5–10% of infections become chronic. In neonates acute infections usually are asymptomatic but the majority become chronic. Chronic infections cause the major burden of disease (and are a constant source of infection for others–“the reservoir ”-) due to the increased risk of liver cirrhosis and hepatocellular carcinoma after decades of chronic infection. There are various categories of chronic infection , with corresponding long-term risk differences. To better understand the disease process, four phases of infection are distinguished that consequently occur in all infected individuals, while the length of stay in each phase is highly variable (Lok 2002).
-
Phase 1: immuno-tolerant phase : “incubation period”. Tolerance with low immune response resulting in HBV replication (circulating viral proteins – antigens HBsAg, HBeAg and high viral load HBV-DNA, but normal liver function tests – “transaminases”) and antibodies against the HBcore protein (anti-HBc).
-
Phase 2: immuno-active phase : “symptomatic disease”. Enhanced immune response, leading to inflammation of liver cells (decreased viral load (HBV-DNA), increased transaminases). Over time, seroconversion of the viral e-antigen (HBeAg) to antibodies to the viral e-antigen (anti-HBe) might occur. Many years in phase 2 can show periods of increased immune activity, with symptomatic disease, and lead to serious liver damage.
-
Phase 3: inactive phase . Persistent anti-HBe, low HBV-DNA, normal transaminases. Occasionally, HBsAg seroconversion to low anti-HBs levels. However, persistent HBV-DNA in liver cells might result in liver cirrhosis and hepatocellular carcinoma (HCC). HBV-DNA integrates in liver cell-DNA and might disturb regulatory mechanisms in cell division and multiplication. There is no evidence that viral factors are important in development of chronic sequelae (as in HCV), but host factors (chronic necrosis, inflammation, and regeneration of liver cells) and external (e.g., smoking) factors contribute to HCC as is the case in HCV.
-
Phase 4: immune phase . High levels of anti-HBs and anti-HBc , absence of HBV-DNA. This is the preferred endpoint of infection: lifelong immunity. It is not excluded that HBV-DNA is integrated in the DNA of certain liver cells, but this does not lead to any chronic sequelae, unless there is a serious immunosuppression for other reasons (e.g., after organ transplant).
Adults most commonly proceed in a short (few months) time from phase 1–2 and 3–4 (asymptomatic, or with mild or seldom serious symptoms), resulting in complete recovery with lifelong immunity. In contrast, infected new born children might stay in phase 1 for many years and slowly progress over the years from phase 2 to 3 when, after several decades, serious liver disease might lead to early death (never reaching phase 4).
2.3.3 Clinical Spectrum
The incubation period (phase 1) varies depending on the host’s immunity, transmission route, and inoculum size. Symptoms are a sign of entering phase 2, and,if occurring, start 6 weeks to 6 months after exposure. Only one-third of infected adults, and an even smaller proportion of children, develops an icteric phase. Rarely, acute symptomatic HBV infection leads to fulminant liver failure (1%) and death (0.1%). HBV clearance is age dependent (Edmunds et al. 1993). Over 95% of adults spontaneously and completely recover (phase 4). However, in 95% of cases infection at birth leads to persistent infection (phase 3), as compared to 30% for those infected at age 0–6 years. Persons with persistent infection are at increased risk of developing cirrhosis and HCC over the ensuing decades.
The liver-related mortality rate for chronically infected HBV patients is estimated at around 1/1000 person years. In HIV co-infected individuals, the risk of HBV chronicity and liver-related mortality is increased (Thio et al. 2002).
2.3.4 Therapy
Acute hepatitis B is a self-limiting disease. However, in the rare cases of fulminant liver failure antiviral therapy might be beneficial (Tillmann et al. 2006) and ultimately liver transplantation is the only life saving treatment option (still an important reason for liver transplantation in the Western world).
Treatment of chronic hepatitis B is indicated if the viral load is high (HBV-DNA >105 IU/ml) and if there are also signs of disturbance of liver function (elevated transaminases –ALAT-) or the presence of liver inflammation and or fibrosis. Present treatment options include immune modulation with interferon alfa, peginterferon alfa, and direct antiviral treatment with nucleoside analogues (such as lamivudine, adefovir, entecavir, or telbivudine) (European Association for the Study of the Liver 2009).
Pegylated interferon alfa during 12 months leads to sustained viral response in 35% of patients and complete cure in 7% (Buster et al. 2008). However, inconvenient administration (subcutaneous) and frequent side effects hamper wider use. Antiviral nucleoside analogues can be given for prolonged periods: one year of treatment leads to reduction in viral load, lowering of transaminases, and improvement of the liver histology in almost all patients. After discontinuation of antiviral therapy the viral load might increase to pre-treatment values. Antiviral treatment can only pave the way for the patient’s immune reaction; complete cure relies on the patient’s immune system.
A serious drawback of long-term use of antivirals (especially lamivudine, but also adefovir and telbivudine) is the occurrence of viral resistance. Resistance against the newer entecavir is at present limited, but the follow-up period is still short.
2.4 Prevention and Control
2.4.1 Hygienic Precautions
For blood borne pathogens , hygienic precautions in the health-care setting are essential for control. This includes avoiding the use of contaminated instruments, universal precautions for invasive procedures, and screening of blood products, tissue and organs. Health-care workers and the public should be educated. Outside health care, the use of contaminated instruments by tattoo, piercing, nail studios, and IDU should be avoided, e.g., by offering needle exchange programs for IDUs. For prevention of sexual transmission condom use is effective.
2.4.2 HBV Notification and Post-exposure Prophylaxis
In areas of low endemicity notification remains important for HBV control. For reported patients, serological markers are evaluated and source and contacts are traced and vaccinated if susceptible. Needle stick injuries and other percutaneous and permucosal exposures, including sexual exposures, always warrant risk assessment for immediate post-exposure prophylaxis (with HBV vaccine and possibly hepatitis B immune globulin (HBIg)).
2.4.3 Universal HBV Vaccination
HBV vaccine (available since 1982) is safe and >95% effective in preventing HBV infection, and is thus the first vaccine against a virus that also causes human cancer. In 1992, the World Health Organization (WHO) called for all countries to implement universal vaccination , and 151 of 192 member states complied (Shepard et al. 2006). In areas with very low prevalence, the cost-effectiveness of universal vaccination is still under debate. Irrespective of universal immunization, selective targeted vaccination for those at highest risk remains important for the coming decades. Universal vaccination in high and medium incidence countries has led to a considerable reduction in prevalence, morbidity, and mortality (Ni et al. 2007; Bonanni et al. 2003). Costs are the major barrier for vaccine introduction in developing countries. Fortunately, the Global Alliance for Vaccines and Immunization (a coalition between public and private institutions) and the Global Fund for Children’s Vaccines is making HBV vaccine available for 74 low-income countries (Lavanchy 2004).
2.4.4 Selective Targeted HBV Vaccination
Low prevalence areas usually target only groups at increased risk for free vaccination: medical risk groups, babies of chronically infected women (requiring antenatal screening and subsequent administration of HBIg at birth, followed by HBV vaccine), IDUs, MSM, and heterosexuals with multiple partners (Salisbury et al. 2006). However, the vaccination coverage in these groups is often low, even among employees at increased risk for HBV that are obliged to be vaccinated, such as health-care workers (Ndiaye et al. 2005).
Travelers of low prevalence areas going to intermediate or high endemicity areas are also advised to have HBV vaccination depending on duration of stay and additional risk factors.
The impact of selective vaccination on the epidemiology of HBV in low incidence countries appears at present to be limited. In the UK and The Netherlands, transmission is ongoing in IDUs and MSM, respectively (Sutton et al. 2006a; van Houdt et al. 2007). This can be explained by low vaccination coverage, increase in the size and changes in behavior of high-risk populations, and enhanced testing and subsequent reporting of (anicteric) infections that previously went undetected. To better assess the effectiveness of selective vaccination, additional methods including behavioral and molecular surveillance are therefore needed. The impact of selective adult vaccination on the burden of disease is limited, as newly acquired infections in adulthood progress to chronic infection only in a minority of cases (5%) and the current disease burden mainly originates from chronic carriers who immigrated from higher prevalence countries.
2.5 Modeling
For HBV, mathematical models have broadly three aims: to study the epidemiology of HBV, to guide public health interventions, and to predict the future burden of disease.
Since the adverse health outcomes of HBV infection mostly take place years after infection, Markov models are used to estimate the effect of HBV screening (Hutton et al. 2007) and treatment of chronic HBV (Takeda et al. 2007).
Obtaining insight into the epidemiology of HBV and its determinants is complex since infection is often asymptomatic. Since the risk of acquiring chronic infection is age dependent and the average age of infection is influenced by the prevalence of carriage, a positive feedback mechanism exists. Mathematical models have been highly instrumental in explaining the extreme differences in levels of HBV endemicity between countries and populations (Medley et al. 2001). Models are also needed for estimating transmission parameters (e.g., the force of infection or basic reproductive ratio) from (sero)prevalence data obtained through surveys (Sutton et al. 2006a; Coleman et al. 1998). These quantities provide information about the prevention effort needed to eliminate the virus and the population groups best targeted by prevention measures.
For HBV, as for many other communicable diseases, interventions such as vaccination and treatment not only reduce the risk of infection and disease in the vaccinated or treated individual, but also in his or her close contacts. A comprehensive assessment of the impact of vaccination and treatment therefore requires that these indirect effects are quantified and taken into account. To do so, dynamic models have been used that simulate the transmission of HBV in a population given determinants such as age, sexual risk behavior, and vaccination coverage. These models have been used to inform decision making on the introduction of public health interventions by assessing the (cost)-effectiveness of HBV vaccination (Williams et al. 1996). Dynamic models have also been used to assess the short- and long-term impact of public health interventions subsequent to implementation, for example, the impact of high-risk group vaccination on the prevalence of chronic infections among MSM (Xiridou et al. 2008). These studies can provide realistic expectations of when the impact of a vaccination program can be expected, and to what extent, e.g., given different levels of sexual risk behavior in MSM. Lastly, dynamic models can guide intervention programs so that maximum impact is achieved. This can result in recommendations to prioritize vaccination of those with the highest levels of risk behavior or new IDUs (Sutton et al. 2006b; Sutton et al. 2006a).
As for other diseases, mathematical modeling has also been used to predict the future burden of disease due to chronic HBV infection (Goldstein et al. 2005). These estimates are relevant to demonstrate potential impact of vaccination, and also for health-care planning. As described in Chapter 12 mathematical models also have their limitations, and surveillance and (molecular) epidemiological studies remain important tools for generating data to support and validate models.
3 Hepatitis C
3.1 Epidemiology
3.1.1 Transmission Routes
HCV was first identified in 1989. It was the most common cause of post-transfusion non-A–non-B hepatitis , as it was especially recognized among individuals who had received contaminated blood products. In 1991, the first commercial HCV antibody test became available, leading to a dramatic decrease in the incidence of transfusion-acquired HCV in countries that introduced screening of donor blood (Memon and Memon 2002).
3.1.2 Global Pattern
HCV has infected an estimated 2.2% of the world’s population (The Global Burden of Hepatitis C Working Group 2004). The reported prevalence rates vary greatly per country. A serious limitation is the lack of reliable population-based studies. Overall, WHO estimates that the African and Eastern Mediterranean regions have the highest HCV prevalence, but for many countries reliable population-based studies are lacking (The Global Burden of Hepatitis C Working Group 2004). The world’s highest HCV prevalence has been reported in Egypt, as a result of mainly intravenous administered therapy against schistosomiasis. From the 1920 s till the 1980s multiple doses of therapeutic injections were administered in mass settings without sufficient sterilization of re-used injection materials, leading to a HCV prevalence of 15–20% in the general Egyptian population (Frank et al. 2000). Although in high-income countries health-care associated HCV transmission incidentally occurs, its contribution to the overall prevalence in these countries is low (Thompson et al. 2009). In contrast, in median- and low-income countries non-sterile injection practices, lack of HCV screening of donor blood, and other iatrogenic routes of transmission still account for significant HCV transmission and serve as a bridge to the general population (Madhava et al. 2002).
3.1.3 Risk Groups
IDUs are at high risk of HCV infection (prevalence 31–98%) (Memon and Memon 2002). Other risk groups for HCV infection are recipients of blood products before 1992 [i.e., hemophilia patients, prevalence ∼70% (Posthouwer et al. 2005)]; hemodialysis patients [prevalence 3–23% (Fissel et al. 2004)]; non-injection drug users (prevalence 2–35%), although the causal pathway to infection in the latter group remains unclear (Scheinmann et al. 2007); people who experienced a needle stick injury and health-care professionals dealing with blood and blood products (prevalence unknown) (Gerberding 1995); household contacts of HCV-infected individuals (possible transmission through the shared use of toothbrushes, razors, etc., prevalence 0–11% (Memon and Memon 2002)); and children born to HCV-infected mothers, with transmission rates of ∼4%, increasing in maternal HCV/HIV co-infection to ∼20% (Yeung et al. 2001). In contrast to HIV and HBV, so far no specific measures are available to prevent mother-to-child transmission for HCV. Mode of delivery and breastfeeding do not influence transmission rates significantly (Yeung et al. 2001).
Other activities that may cause blood–blood contact have been described as routes of HCV infection, such as tattooing, body piercing, and cultural/religious practices (e.g., scarification, circumcision, acupuncture). However, results are inconsistent and it is uncertain whether these risk factors make any measurable contribution to overall HCV transmission (Alter 2007).
Even in the presence of HIV co-infection , HCV is rarely transmitted by heterosexual intercourse (Vandelli et al. 2004). Since 2000, however, HCV emerges among HIV-infected MSM (Giraudon et al. 2007; van de Laar et al. 2009). Phylogenetic analyses showed clusters of MSM-specific HCV strains, indicating a sexual route of HCV transmission. Based on mainly case studies, it has been suggested that sexually acquired HCV is associated with HIV infection, the presence of ulcerative sexually transmitted diseases, sexual techniques causing mucosal damage, and sex under the influence of non-injecting drugs (Danta et al. 2007; van de Laar et al. 2009).
3.2 Virology and Molecular Epidemiology
3.2.1 Virology
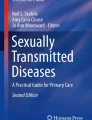
HCV is a single-stranded RNA virus, whose host range is confined to humans and closely related primates. It primarily targets hepatocytes. Due to its similarities in genome organization, structure and replication to a large group of vector borne diseases (e.g., yellow fever) and animal pestiviruses, HCV was added to the family of Flaviviridae. The viral genome codes for one single polyprotein, which is processed into three structural proteins and seven non-structural proteins that code for the viral enzymes (Simmonds 2001). The high viral turnover and the error-prone replication process result in rapid evolution of HCV within an infected host. The swarm of highly similar viral variants that develop within one host is called quasispecies and probably provide the mechanism by which HCV evades host immune surveillance and establishes and maintains chronic infection (Gale and Foy 2005) (Fig. 19.2).

HCV model structure and genome organization. Reproduced from reference Anzola and Burgos 2003 with permission from the author
3.2.2 Molecular Epidemiology
The high genetic variability of the HCV genome has led to a classification of the virus into seven major genotypes (1–7) which except for genotypes 5 and 7 are each further divided into more than 80 related subtypes (a, b, c,…) (Simmonds et al. 2005; Murphy et al. 2007). Genotypes have 65–70% similarity on the nucleotide level, subtypes 75–80%, and within a subtype sequence variability is below 10% (Simmonds et al. 2005). As HCV genotype distribution depends on geographic area, mode of transmission , and varies over time, it provides clues about the historical origin and the spread of the virus. Some HCV subtypes are found globally due to a swift spread in the 20th century through needle sharing among IDUs (types 1a and 3a) or contaminated blood products (types 1b, 2a, and 2b). These genotypes represent the majority of infections in Europe and Northern America. In contrast, the presence of numerous and highly diverse subtypes in Western/Central Africa and the Middle East (genotypes 1, 2, and 4) as well as Southeast Asia (genotypes 3 and 6) suggest that these genotypes originate from these areas where they have been endemic for a long time (Simmonds 2001).
Evolutionary relationships among genes and organisms can be illustrated by a phylogenetic tree, comparable to a pedigree showing which genes or organisms are most closely related. As the degree of diversity (or similarity) among HCV viral variants provides information on the likelihood that strains were acquired in the same transmission network, phylogenetic analysis can be used to investigate the spread of HCV. The high similarity of HCV isolates observed among MSM in Europe revealed a large transmission network of HIV-infected MSM in which HCV transmission was linked to high-risk sexual behavior (van de Laar et al. 2009). In contrast, the degree of diversity among HCV and HIV isolates obtained from children attending a hospital in Benghazi, Libya showed that four different HIV and HCV outbreaks in this hospital were due to a long-standing infection-control problem instead of the arrival of a foreign medical staff, who were found guilty in 2004 of deliberately infecting 426 children with HIV. Based on inferred nucleotide evolutionary rates, the date of origin of the four outbreaks proved to vary between 1985 and 1997, which is before the arrival of the foreign staff (de Oliveira et al. 2006).
3.2.3 HCV Superinfection and Reinfection
Molecular typing techniques have confirmed that both HCV reinfection and superinfection with a homologous or a heterologous HCV strain occur, suggesting that neither virological clearance nor ongoing HCV chronic infection provides full protection against new HCV infections (Blackard and Sherman 2007). Evidence for partial HCV protective immunity derives largely from chimpanzee studies. Chimpanzees that previously cleared HCV and subsequently were rechallenged with homologous HCV strains, generally show lower levels of HCV viremia and self-limited infection (Bassett et al. 2001). In humans, the presence of such partial protective immunity remains controversial. IDUs from Baltimore who spontaneously cleared their HCV infection were found to be less likely to develop new episodes of HCV viremia compared to IDUs without previous infection (Mehta et al. 2002). No such protection, however, was observed among a cohort of young Australian IDUs (Micallef et al. 2007). Moreover, as the generation of a recombinant virus requires that a cell must be infected simultaneously with two or more distinct HCV strains, the recent documentation of recombinant HCV strains is de facto evidence that dual HCV infections also occur (Kalinina et al. 2004). The reported frequency of such HCV superinfection in active IDUs varies between 0 and 20% (Herring et al. 2004; Dove et al. 2005). The true incidence, however, is hard to establish as current laboratory methodologies make characterization of superinfection cumbersome (Blackard and Sherman 2007).
3.2.4 Diagnostics
Standard HCV testing includes screening for HCV antibodies using an anti-HCV EIA confirmed by immunoblot. In a clinical setting, a positive HCV antibody test will be directly followed by RNA testing to establish the presence of ongoing infection. In order to diagnose the widest span of viral variants, HCV-RNA tests are generally based on the highly conserved 5ʹ untranslated region (UTR) of the HCV genome. Genotyping on the other hand requires viral heterogeneity, reference regions globally used for genotyping are structural proteins core/E1 and the non-structural NS5B protein that codes for the RNA polymerase (Simmonds et al. 2005).
The time between the infection and the appearance of HCV antibodies is estimated to be approximately 60 days (Busch 2001). Hence, the presence of active HCV-RNA in HCV antibody negative individuals indicates acute infection. However, prolonged seroconversion windows or complete failure to mount or maintain HCV antibodies have been observed among immunosuppressed individuals, e.g., those co-infected with HIV (Chamie et al. 2007). Once HCV antibody positive, current lab techniques are unable to provide information on the moment HCV was acquired. Loss of HCV antibodies (HCV seroreversion) has been described, but mainly among individuals that were able to clear the virus (Lannote et al. 1998).
3.3 Clinical Course of Infection
In the majority of cases acute HCV is asymptomatic. Less than one-third of individuals with an acute HCV infection experiences mostly mild and aspecific symptoms such as loss of appetite, fatigue and flu-like symptoms, and occasionally jaundice (Hoofnagle 2002). Natural viral clearance of HCV only occurs in a minority (∼25%) of patients (Micallef et al. 2006). Chronic infection is defined as the persistence of HCV-RNA for more than 6 months after infection. As the onset of the infection and the development of cirrhosis in chronically infected patients usually are asymptomatic, diagnosis often occurs late, limiting efforts to determine natural history of HCV (Seeff 2002). Depending on the study design and population, a large variation in progression rate has been found. Approximately 20 years after the onset of chronic infection, HCV leads to liver cirrhosis in 6–25% of patients, of whom per year 1–4% develop hepatocellular carcinoma (Seeff 2002; Sweeting et al. 2006; Patel et al. 2006). Next to viral factors, host and external factors such as male sex, older age at the time of infection, HBV or HIV-1 co-infection , and alcohol intake might accelerate disease progression (Seeff 2002; Patel et al. 2006). Some of these factors are also associated with viral persistence after acute infection and therapy outcome. New non-invasive methods have been developed that can be used for clinical decision making, including combined serological markers and liver scan techniques to establish the degree of fibrosis. However, until now liver histology is still considered to be the most reliable method to stage and grade the severity of liver disease (Patel et al. 2006).
3.3.1 Therapy
Recently, important advances in the treatment of chronic HCV infection have been made. Currently, the recommended therapy consists of the use of a modified form (pegylated) of interferon alpha (protein with immunomodularity and antiviral properties) in combination with ribavirin (a nucleoside analogue with antiviral activity). In the absence of HIV co-infection, HCV treatment duration is usually 24–48 weeks, depending on the HCV genotype. The aim of the treatment is to eradicate viral RNA and to reach a sustained virological response (SVR) , which is the absence of HCV-RNA at 24 weeks after the end of treatment (National Institutes of Health Consensus Development Conference Statement 2002). The most important predictor of SVR, which occurs in 42–80% of the cases, is HCV genotype (Weigand et al. 2007). Genotypes 1 and 4 are difficult-to-treat genotypes, with approximately 50% of treated patients achieving SVR, compared to an SVR up to 90% in patients with genotypes 2 and 3. Other predictors of therapeutic outcome that influence treatment duration include rapid viral response (RVR) (undetectable HCV-RNA levels at week 4) and early viral responses (EVR) (≤2 log decrease in viral load during the first 12 weeks) and low HCV-RNA level prior to treatment (Weigand et al. 2007).
All patients should be considered for treatment. However, patients with mild disease activity can be given the option of deferring therapy (Patel et al. 2006). Despite this, a high number of IDU still has limited access to HCV antiviral treatment, as cost-effectiveness of HCV treatment in this population is often questioned. Those successfully treated are at risk of HCV reinfection when sharing of injection equipment is continued (Micallef et al. 2007). Moreover, low treatment adherence with ongoing risk behavior, as well as the possibility of HCV superinfection at the start of treatment might negatively affect HCV treatment outcome itself (Blackard and Sherman 2007). However, recent studies suggest that when HCV care is integrated with methadone provision drug users can be successfully treated (Novick and Kreek 2008).
Approximately 10–14% of all patients discontinue treatment because of serious side effects (National Institutes of Health Consensus Development Conference Statement 2002). Some others experience viral relapses after the end of treatment. Currently new therapeutic concepts are being developed which directly target HCV-RNA and viral enzymes, or influence host–virus interactions (Takkenberg et al. 2008). Despite toxicity issues and rapid selection of resistance, which did restrain some of the initial enthusiasm, several of these new compounds are very promising and are expected to be registered within the next 3 years. Future treatment of chronic HCV infection will probably be more effective and shorter, and consist of a combination of peginterferon, ribavirin together with one or more new drugs (Takkenberg et al. 2008).
3.4 Prevention and Control
3.4.1 Prevention of Further Spread of HCV
In contrast to HBV, for HCV there is no vaccine available, nor are there drugs for post-exposure prophylaxis or prevention of mother-to-child-transmission. Prevention relies completely on precautionary measures preventing further spread, which are similar to those taken for HBV (e.g., hygienic measures, screening of donor blood). As effective treatment is available, creating awareness and stimulating testing behavior among HCV risk groups is of major importance.
As IDUs are at high risk of HIV and HCV due to the reuse and sharing of needles and/or injecting paraphernalia, in high-income countries many HIV harm reduction programs have been targeted at this population. These include needle exchange programs, social care, opioid replacement therapy (mainly methadone and buprenorphine), or a combination of these. Many interventions have shown to be cost-effective since they have reduced HIV prevalence (Wright and Tompkins 2006). Studies evaluating the effect of separate harm reduction programs on HCV incidence or prevalence show inconsistent results. Van den Berg et al. suggested that a combined comprehensive approach is effective (van den Berg et al. 2007).
Improvement of blood transfusion safety and health-care conditions are the main factors that will contribute to the control of HCV transmission in low- and medium-income countries.
3.4.2 Identifying Undiagnosed HCV Infections
Mass population screening for HCV in low prevalence countries is considered to be inappropriate as its cost-effectiveness is poor. Several targeted screening programs have been carried out aimed at risk groups for HCV infection. Screening policies are based on various considerations, including the prevalence of risk behavior (i.e., injecting drugs) or exposure (blood transfusion before HCV screening of donor blood started) in the population, the prevalence of HCV among those with the risk profile, and the need for persons with a recognized exposure to be evaluated for HCV (Alter 2002). Tracing HCV-infected individuals can lead to individual lifestyle adjustments (improving HCV prognosis), treatment, and prevention of further transmission (e.g., to household contacts).
As HCV had spread among individuals who received blood products before the introduction of the first HCV antibody test in 1991, various high-income countries introduced look-back programs in which recipients of blood from HCV-infected donors were notified and motivated for testing. As in other look-back programs, the Canadian HCV look-back experience successfully identified previously undiagnosed HCV-infected patients, but the costs were high and the yield relatively low (Bowker et al. 2004). Other interventions aimed at identifying undiagnosed HCV-infected individuals used targeted screening programs based on risk factors (Sypsa et al. 2001; Mallette et al. 2007), which may prove to be a more cost-effective screening policy. HCV information campaigns have been initiated in various high-income countries including Australia, the UK, the USA, and Canada, but data on the results of these campaigns have not been published so far.
Many medium- and low-income countries lack an active policy for identifying HCV-infected individuals or for raising awareness, as other health or economic problems have more urgency.
3.5 Modeling
Mathematical models have been used to reconstruct the spread of HCV. For example, using molecular evolutionary analysis and a logistic growth model (see Chapter 12) it has been estimated that the spread of HCV genotype 1 in Japan in the 1930 s took place before widespread dissemination of HCV in the United States in the 1960 s when IDU and transfusion of unscreened blood (products) were widespread (Tanaka et al. 2002). A coalescent approach estimated that the timing of the HCV epidemic in Egypt was between 1930 and 1950 (Pybus et al. 2003), whereas a back calculation model estimated that the epidemic exploded in 1970 in line with the massive use of parenteral anti-schistosomiasis treatment in this period (Deuffic-Burban et al. 2006). The discrepancy in the estimation of the timing of the epidemic might be due to the different methods applied and the assumptions made. It is hard to conclude which estimate is most likely because no serological data are available for that time period.
Because of the relatively long time from infection to disease outcome, Markov and other mathematical models (including forward projection models) have been developed to predict the future epidemic and burden of disease and to evaluate the effect of interventions. Based on these models it has been estimated that, for various medium- to high-income countries, HCV-related morbidity and mortality will at least double in the next two decades (Sypsa et al. 2005; Deuffic-Burban et al. 2006), and will exceed the number of deaths from HIV. The improvements of HCV therapy are too recent and the identification of infected individuals for treatment is too low to reverse the increase in mortality (Deuffic-Burban et al. 2007). Models have also been helpful in planning and evaluating the effect of interventions aimed at preventing new HCV infections. They have suggested that because of the high reproductive rate of HCV compared to HIV comprehensive harm reduction programs must complement syringe exchange to successfully prevent HCV. The interventions should also be sustained for many years to reduce HCV infections (Vickerman et al. 2007).
4 Conclusions
There are overlaps and differences in the (efficiency of) transmission routes of HBV and HCV. Although blood–blood transmissibility is higher for HBV than HCV, the higher rate of chronicity for HCV has resulted in a large number of chronic carriers for both viruses. These chronic infections have an increased risk for serious liver disease decades after initial infection and have therefore a significant impact on public health. Presently, in high-income countries, more people die from HBV and HCV than from HIV.
For HBV, effective public health intervention to prevent new infections is feasible with a safe and effective vaccine . Universal childhood vaccination can eradicate hepatitis B. However, this will not prevent serious liver disease and early death in the coming decades for the 350 millions that are already chronically infected with HBV. In the absence of a vaccine against HCV, HCV prevention relies completely on precautionary measures preventing its further spread.
For both HBV and HCV, molecular epidemiology and mathematical modeling have greatly contributed in clarifying routes of transmission, and in predicting the (impact of interventions on the) future burden of disease.
Besides development of public health interventions, future challenge exists of unraveling the specific mechanisms of spontaneous viral clearance, super-/co-infection, and viral resistance, and of gaining insight into determinants predicting therapy success. Further efforts will focus on advances in therapy which now show encouraging results for HCV in preclinical studies.
For both HBV and HCV, identification of asymptomatic chronically infected individuals is extremely important. In affluent societies effective (expensive) treatment is available for both, to improve individual long-term outcome. Additionally, effective treatment will eliminate the reservoir for new infections. Development of new drugs has to keep pace with inevitable development of viral resistance. Through various donor organizations universal HBV vaccination is made available in most low-income countries. Now, efforts should be made so that treatment is also available in developing countries where most of the burden of disease due to hepatitis B and C occurs. Infected individuals can take precautionary measures to prevent further spread (e.g., wound care, using condoms), and susceptible (household) contacts of HBV-infected individuals should be vaccinated. As the majority of acute HBV and HCV infections go unnoticed, educating the public about (differences in) the often mixed-up hepatitis viruses and their nature is of great importance to enhance awareness and facilitate early identification.
References
Alter MJ (2002) Prevention of spread of hepatitis C. Hepatology; 36(5):593–598
Alter MJ (2007) Epidemiology of hepatitis C virus infection. World J Gastroenterol; 13(17):2436–2441
Anzola M, Burgos JJ (2003) Hepatocellular carcinoma: molecular interactions between hepatitis C virus and p53 in hepatocarcinogenesis. Expert Rev Mol Med; 5(28):1–16
Aweis D, Cooper CD, Brabin B, Beeching N (2001) Serological evidence for Hepatitis B infection in the Somali population of Liverpool. Arch Dis Child; 84 (suppl I):A62
Bassett SE, Guerra B, Brasky K, Miskovsky E, Houghton M, Klimpel GR et al. (2001) Protective immune response to hepatitis C virus in chimpanzees rechallenged following clearance of primary infection. Hepatology; 33(6):1479–1487
Beasley RP, Trepo C, Stevens CE, Szmuness W (1977) The e antigen and vertical transmission of hepatitis B surface antigen. Am J Epidemiol; 105(2):94–98
Blackard JT, Sherman KE (2007) Hepatitis C virus coinfection and superinfection. J Infect Dis; 195(4):519–524
Bonanni P, Pesavento G, Bechini A, Tiscione E, Mannelli F, Benucci C et al. (2003) Impact of universal vaccination programmes on the epidemiology of hepatitis B: 10 years of experience in Italy. Vaccine; 21(7–8):685–691
Boot HJ, Cremer J, Koedijk F, Ballegooijen M, Op de Coul ELM (2008) Improved tracing of hepatitis B virus transmission chains by phylogenetic analysis based on C region sequences. J Med Virol; 80:233–241
Bowker SL, Smith LJ, Rosychuk RJ, Preiksaitis JK (2004) A review of general hepatitis C virus lookbacks in Canada. Vox Sang; 86(1):21–27
Busch MP (2001) Closing the window on viral transmission in blood transfusion. In: Stramer SL, ed. Blood safety in the new milennium. American Association of Blood Banks:Betehsda, MD; 33–54
Buster EH, Flink HJ, Cakaloglu Y, Simon K, Trojan J, Tabak F et al. (2008)Sustained HBeAg and HBsAg loss after long-term follow-up of HBeAg-positive patients treated with peginterferon alpha-2b. Gastroenterology; 135(2):459–467
Chamie G, Bonacini M, Bangsberg DR, Stapleton JT, Hall C, Overton ET et al. (2007) Factors associated with seronegative chronic hepatitis C virus infection in HIV infection. Clin Infect Dis; 44(4):577–583
Coleman PJ, McQuillan GM, Moyer LA, Lambert SB, Margolis HS (1998) Incidence of hepatitis B virus infection in the United States, 1976–1994: estimates from the National Health and Nutrition Examination Surveys. J Infect Dis; 178(4):954–959
Courouce AM, Drouet J, Muller JY (1976) Australia antigen subtypes identification. Results. Bibl Haematol; 42:89–127
Danta M, Brown D, Bhagani S, Pybus OG, Sabin CA, Nelson M et al. (2007) Recent epidemic of acute hepatitis C virus in HIV-positive men who have sex with men linked to high-risk sexual behaviours. AIDS; 21(8):983–991
Davis LG, Weber DJ, Lemon SM (1989) Horizontal transmission of hepatitis B virus. Lancet; 1(8643):889–893
de Oliveira T, Pybus OG, Rambaut A, Salemi M, Cassol S, Ciccozzi M et al. (2006) Molecular epidemiology: HIV-1 and HCV sequences from Libyan outbreak. Nature; 444(7121):836–837
Deuffic-Burban S, Mohamed MK, Larouze B, Carrat F, Valleron AJ (2006) Expected increase in hepatitis C-related mortality in Egypt due to pre-2000 infections. J Hepatol; 44(3):455–461
Deuffic-Burban S, Poynard T, Sulkowski MS, Wong JB (2007) Estimating the future health burden of chronic hepatitis C and human immunodeficiency virus infections in the United States. J Viral Hepat; 14(2):107–115
Dove L, Phung Y, Bzowej N, Kim M, Monto A, Wright TL (2005) Viral evolution of hepatitis C in injection drug users. J Viral Hepat; 12(6):574–583
Echevarria JM, Avellon A (2006) Hepatitis B virus genetic diversity. J Med Virol; 78 (Suppl 1):S36–S42
Edmunds WJ, Medley GF, Nokes DJ, Hall AJ, Whittle HC (1993) The influence of age on the development of the hepatitis B carrier state. Proc R Soc Lond B Biol Sci; 253(1337):197–201
European Association for the Study of the Liver (2009) EASL clinical practice guidelines: management of chronic hepatitis B. J Hepatol; 50:227–242
Fisker N, Carlsen NL, Kolmos HJ, Tonning-Sorensen L, Host A, Christensen PB (2006) Identifying a hepatitis B outbreak by molecular surveillance: a case study. BMJ; 332(7537):343–345
Fissell RB, Bragg-Gresham JL, Woods JD, Jadoul M, Gillespie B, Hedderwick SA et al. (2004) Patterns of hepatitis C prevalence and seroconversion in hemodialysis units from three continents: the DOPPS. Kidney Int; 65(6):2335–2342
Frank C, Mohamed MK, Strickland GT, Lavanchy D, Arthur RR, Magder LS et al. (2000) The role of parenteral antischistosomal therapy in the spread of hepatitis C virus in Egypt. Lancet; 355(9207):887–891
Gale M, Jr., Foy EM (2005) Evasion of intracellular host defence by hepatitis C virus. Nature; 436(7053):939–945
Gerberding JL (1995) Management of occupational exposures to blood-borne viruses. N Engl J Med; 332(7):444–451
Giraudon I, Ruf M, Maguire H, Charlett A, Ncube F, Turner J et al. (2007).Increase in newly acquired hepatitis C in HIV positive men who have sex with men across London and Brighton, 2002–2006. Is this an outbreak? Sex Transm Infect 84(2):111–115
Goldstein ST, Zhou F, Hadler SC, Bell BP, Mast EE, Margolis HS (2005) A mathematical model to estimate global hepatitis B disease burden and vaccination impact. Int J Epidemiol; 34(6):1329–1339
Hahné S, Ramsay M, Balogun K, Edmunds WJ, Mortimer P (2004) Incidence and routes of transmission of hepatitis B virus in England and Wales, 1995–2000: Implications for immunisation policy. J Clin Virol; 29:211–220
Hahné S, Ramsay M, Soldan K, Balogun K, Mortimer P (2003) Hepatitis B incidence among South Asian children in England and Wales: implications for immunisation policy. Arch Dis Child; 88:1082–1083
Hauri AM, Armstrong GL, Hutin YJ (2004) The global burden of disease attributable to contaminated injections given in health care settings. Int J STD AIDS; 15(1):7–16
Herring BL, Page-Shafer K, Tobler LH, Delwart EL (2004) Frequent hepatitis C virus superinfection in injection drug users. J Infect Dis; 190(8):1396–1403
Hoofnagle JH (2002) Course and outcome of hepatitis C. Hepatology; 36(5):521–529
Hurie MB, Mast EE, Davis JP (1992) Horizontal transmission of hepatitis B virus infection to United States- born children of Hmong refugees. Pediatrics; 89(2):269–273
Hutton DW, Tan D, So SK, Brandeau ML (2007) Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults for hepatitis B. Ann Intern Med; 147(7):460–469
Kalinina O, Norder H, Magnius LO (2004) Full-length open reading frame of a recombinant hepatitis C virus strain from St Petersburg: proposed mechanism for its formation. J Gen Virol; 85(7):1853–1857
Kingsley LA, Rinaldo CR Jr., Lyter DW, Valdiserri RO, Belle SH, Ho M (1990) Sexual transmission efficiency of hepatitis B virus and human immunodeficiency virus among homosexual men. JAMA; 264(2):230–234
Lanotte P, Dubois F, Le PS, Guerois C, Fimbel B, Bacq Y et al. (1998) The kinetics of antibodies against hepatitis C virus may predict viral clearance in exposed hemophiliacs. J Infect Dis; 178(2):556–559
Lavanchy D (2004) Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepat; 11(2):97–107
Lok AS (2002) Chronic hepatitis B. N Engl J Med; 346(22):1682–1683
Lok AS, McMahon BJ (2007) Chronic hepatitis B. Hepatology; 45(2):507–539
Madhava V, Burgess C, Drucker E (2002) Epidemiology of chronic hepatitis C virus infection in sub-Saharan Africa. Lancet Infect Dis; 2(5):293–302
Mallette C, Flynn MA, Promrat K (2007) Outcome of screening for hepatitis C virus infection based on risk factors. Am J Gastroenterol 103(1):131–137
Memon MI, Memon MA (2002) Hepatitis C: an epidemiological review. J Viral Hepat; 9(2):84–100
Medley GF, Lindop NA, Edmunds WJ, Nokes DJ (2001) Hepatitis-B virus endemicity: heterogeneity, catastrophic dynamics and control. Nat Med; 7(5):619–624
Mehta SH, Cox A, Hoover DR, Wang XH, Mao Q, Ray S et al. (2002) Protection against persistence of hepatitis C. Lancet; 359(9316):1478–1483
Micallef JM, Kaldor JM, Dore GJ (2006) Spontaneous viral clearance following acute hepatitis C infection: a systematic review of longitudinal studies. J Viral Hepat; 13(1):34–41
Micallef JM, Macdonald V, Jauncey M, Amin J, Rawlinson W, van Beek I et al. (2007) High incidence of hepatitis C virus reinfection within a cohort of injecting drug users. J Viral Hepat; 14(6):413–418
Murphy DG, Willems B, Deschenes M, Hilzenrat N, Mousseau R, Sabbah S (2007) Use of sequence analysis of the NS5B region for routine genotyping of hepatitis C virus with reference to C/E1 and 5' untranslated region sequences. J Clin Microbiol; 45(4):1102–1112
National Institutes of Health Consensus Development Conference Statement (2002) Management of hepatitis C: 2002-June 10–12, 2002. Hepatology; 36(5 Suppl 1):S3–20
Ndiaye SM, Hopkins DP, Shefer AM, Hinman AR, Briss PA, Rodewald L et al. (2005) Interventions to improve influenza, pneumococcal polysaccharide, and hepatitis B vaccination coverage among high-risk adults: a systematic review. Am J Prev Med; 28(5 Suppl):248–279
Ni YH, Huang LM, Chang MH, Yen CJ, Lu CY, You SL et al. (2007) Two decades of universal hepatitis B vaccination in Taiwan: impact and implication for future strategies. Gastroenterology; 132(4):1287–1293
Norder H, Courouce AM, Coursaget P, Echevarria JM, Lee SD, Mushahwar IK et al. (2004) Genetic diversity of hepatitis B virus strains derived worldwide: genotypes, subgenotypes, and HBsAg subtypes. Intervirology; 47(6):289–309
Novick DM, Kreek MJ (2008) Critical issues in the treatment of hepatitis C virus infection in methadone maintenance patients. Addiction; 103(6):905–918
Omata M, Ehata T, Yokosuka O, Hosoda K, Ohto M (1991) Mutations in the precore region of hepatitis B virus DNA in patients with fulminant and severe hepatitis. N Engl J Med; 324(24):1699–1704
Patel K, Muir AJ, McHutchison JG (2006) Diagnosis and treatment of chronic hepatitis C infection. BMJ; 332(7548):1013–1017
Posthouwer D, Plug I, van der Bom JG, Fischer K, Rosendaal FR, Mauser-Bunschoten EP (2005) Hepatitis C infection among Dutch haemophilia patients: a nationwide cross-sectional study of prevalence and antiviral treatment. Haemophilia; 11(3):270–275
Pybus OG, Drummond AJ, Nakano T, Robertson BH, Rambaut A (2003) The epidemiology and iatrogenic transmission of hepatitis C virus in Egypt: a Bayesian coalescent approach. Mol Biol Evol; 20(3):381–387
Salisbury D, Ramsay M, Noakes Keds. (2006) Immunisation against infectious disease. HMSO: London
Scheinmann R, Hagan H, Lelutiu-Weinberger C, Stern R, Des Jaklais D, Flom PL et al. (2007) Non-injection drug use and Hepatitis C Virus: a systematic review. Drug and Alcohol Dependence; 89(1):1–12
Seeff LB (2002) Natural history of chronic hepatitis C. Hepatology; 36(5):S35–S36
Shepard CW, Simard EP, Finelli L, Fiore AE, Bell BP (2006) Hepatitis B virus infection: epidemiology and vaccination. Epidemiol Rev; 28:112–125
Simmonds P (2001) The origin and evolution of hepatitis viruses in humans. J Gen Virol; 82(Pt 4):693–712
Simmonds P, Bukh J, Combet C, Deleage G, Enomoto N, Feinstone S et al. (2005) Consensus proposals for a unified system of nomenclature of hepatitis C virus genotypes. Hepatology; 42(4):962–973
Sutton AJ, Gay NJ, Edmunds WJ (2006b) Modelling the impact of prison vaccination on hepatitis B transmission within the injecting drug user population of England and Wales. Vaccine; 24(13):2377–2386
Sutton AJ, Gay NJ, Edmunds WJ, Hope VD, Gill ON, Hickman M (2006a) Modelling the force of infection for hepatitis B and hepatitis C in injecting drug users in England and Wales. BMC Infect Dis; 6:93
Sweeting MJ, de Angelis D, Neal KR, Ramsay ME, Irving WL, Wright M et al. (2006) Estimated progression rates in three United Kingdom hepatitis C cohorts differed according to method of recruitment. J Clin Epidemiol; 59(2):144–152
Sypsa V, Hadjipaschali E, Hatzakis A (2001) Prevalence, risk factors and evaluation of a screening strategy for chronic hepatitis C and B virus infections in healthy company employees. Eur J Epidemiol; 17(8):721–728
Sypsa V, Touloumi G, Papatheodoridis GV, Tassopoulos NC, Ketikoglou I, Vafiadis I et al. (2005) Future trends of HCV-related cirrhosis and hepatocellular carcinoma under the currently available treatments. J Viral Hepat; 12(5):543–550
Takeda A, Jones J, Shepherd J, Davidson P, Price A (2007) A systematic review and economic evaluation of adefovir dipivoxil and pegylated interferon-alpha-2a for the treatment of chronic hepatitis B. J Viral Hepat; 14(2):75–88
Takkenberg B, de Bruijne J, Weegink C, Jansen P, Reesink H (2008) Novel therapies in hepatitis B and C. Curr Gastroenterol Rep; 10(1):81–90
Tanaka Y, Hanada K, Mizokami M, Yeo AE, Shih JW, Gojobori T et al. (2002) Inaugural Article: A comparison of the molecular clock of hepatitis C virus in the United States and Japan predicts that hepatocellular carcinoma incidence in the United States will increase over the next two decades. Proc Natl Acad Sci USA; 99(24):15584–15589
The Global Burden Of Hepatitis C Working Group (2004) Global burden of disease (GBD) for hepatitis C. J Clin Pharmacol; 44(1):20–29
Thio CL, Seaberg EC, Skolasky R, Jr., Phair J, Visscher B, Munoz A et al. (2002) HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet; 360(9349):1921–1926
Thompson ND, Perz JF, Moorman AC, Holmberg SD (2009) Nonhospital health care-associated hepatitis B and C virus transmission: United States, 1998–2008. Ann Intern Med; 150(1):33–39
Tillmann HL, Hadem J, Leifeld L, Zachou K, Canbay A, Eisenbach C et al. (2006) Safety and efficacy of lamivudine in patients with severe acute or fulminant hepatitis B, a multicenter experience. J Viral Hepat; 13(4):256–263
van de Laar TJ, Pybus OG, Bruisten SM, Brown D, Nelson M, Bhagani S et al. (2009) Evidence of a large, international HCV transmission network in HIV-positive men who have sex with men. Gastroenterology 136(5):1609–1617
Vandelli C, Renzo F, Romano L, Tisminetzky S, De Palma M, Stroffolini T et al. (2004) Lack of evidence of sexual transmission of hepatitis C among monogamous couples: results of a 10-year prospective follow-up study. Am J Gastroenterol; 99(5):855–859
van den Berg C, Smit C, van Brussel G, Coutinho R, Prins M (2007) Full participation in harm reduction programmes is associated with decreased risk for human immunodeficiency virus and hepatitis C virus: evidence from the Amsterdam Cohort Studies among drug users. Addiction; 102(9):1454–1462
van Houdt R, Bruisten SM, Koedijk FD, Dukers NH, op de Coul EL, Mostert MC et al. (2007) Molecular epidemiology of acute hepatitis B in the Netherlands in 2004: nationwide survey. J Med Virol; 79(7):895–901
van Houdt R, Koedijk FDH, Bruisten SM, op de Coul EL, Heijnen MLA, Waldhober Q, et al. (2009) Hepatitis B vaccination targeted toward behavioral-risk groups in the Netherlands: does it work? Vaccine 27(27):3530–3535
van Steenbergen JE, Niesters HGM, Op de Coul ELM, van Doornum GJJ, Osterhaus ADME, Leentvaar-Kuijpers A et al. (2002) Molecular epidemiology of Hepatitis B Virus in Amsterdam 1992–1997. J Med Virol; 66:159–165
Vickerman P, Hickman M, Judd A (2007) Modelling the impact on Hepatitis C transmission of reducing syringe sharing: London case study. Int J Epidemiol; 36(2):396–405
Weigand K, Stremmel W, Encke J (2007) Treatment of hepatitis C virus infection. World J Gastroenterol; 13(13):1897–1905
Williams JR, Nokes DJ, Medley GF, Anderson RM (1996). The transmission dynamics of hepatitis B in the UK: a mathematical model for evaluating costs and effectiveness of immunization programmes. Epidemiol Infect; 116(1):71–89
Wright NM, Tompkins CN (2006) A review of the evidence for the effectiveness of primary prevention interventions for hepatitis C among injecting drug users. Harm Reduct J; 3:27
Xiridou M, Wallinga J, Dukers-Muijers N, Coutinho R (2008) Hepatitis B vaccination and changes in sexual risk behaviour among men who have sex with men in Amsterdam. Epidemiol Infect; 137(4):504–512
Yeung LT, King SM, Roberts EA (2001) Mother-to-infant transmission of hepatitis C virus. Hepatology; 34(2):223–229
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2009 Springer Science+Business Media, LLC
About this chapter
Cite this chapter
Zuure, F., Hahné, S., van de Laar, T., Prins, M., van Steenbergen, J. (2009). Blood Borne and Sexual Transmission: Hepatitis B and C. In: Krämer, A., Kretzschmar, M., Krickeberg, K. (eds) Modern Infectious Disease Epidemiology. Statistics for Biology and Health. Springer, New York, NY. https://doi.org/10.1007/978-0-387-93835-6_19
Download citation
DOI: https://doi.org/10.1007/978-0-387-93835-6_19
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-0-387-93834-9
Online ISBN: 978-0-387-93835-6
eBook Packages: Mathematics and StatisticsMathematics and Statistics (R0)