
Abstract
Larynx cancer is the most common cancer of the head and neck. Risk factors include tobacco, alcohol, betel and areca nuts, and deficiencies of iron, vitamin B12, and vitamin C. Larynx subsites: Supraglottis: suprahyoid and infrahyoid epiglottis, aryepiglottic folds, arytenoids, and false cords. Glottis: true vocal cords (TVCs) including the anterior and posterior commissures. Subglottis: extends from the lower boundary of the glottis to the inferior aspect of the cricoid cartilage.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Pearls
Larynx
-
Larynx cancer is the most common cancer of the head and neck.
-
Risk factors include tobacco, alcohol, betel and areca nuts, and deficiencies of iron, vitamin B12, and vitamin C.
-
Larynx subsites:
-
Supraglottis: suprahyoid and infrahyoid epiglottis, aryepiglottic folds, arytenoids, and false cords.
-
Glottis: true vocal cords (TVCs) including the anterior and posterior commissures.
-
Subglottis: extends from the lower boundary of the glottis to the inferior aspect of the cricoid cartilage.
-
-
TVCs attach to the thyroid cartilage at the center of the “figure of 8” on a lateral X-ray.
-
LN drainage is common from the supraglottis (to levels II–V) and subglottis [to pretracheal (Delphian), paratracheal, and inferior jugular nodes]. Glottic tumors rarely spread to LN when ≤T1–2 (<3%), but more commonly spread to LN when T3–4 (∼20–30%).
-
Superior laryngeal nerve innervates the cricothyroid muscles that produce tension and elongation of the vocal cords. All other laryngeal muscles are innervated by the recurrent laryngeal nerve.
Hypopharynx
-
Portion of the pharynx extending from the plane of the superior border of the hyoid bone to the inferior border of the cricoid cartilage.
-
Hypopharynx subsites:
-
Pyriform sinuses.
-
Posterior and lateral hypopharyngeal walls.
-
Postcricoid area.
-
-
LN drainage from the hypopharynx is to levels II–V, the retropharyngeal LN, and to paratracheal and paraesophageal LN (when tumor involves the lowest portion of the hypopharynx and the postcricoid area).
-
Ninety five percent of tumors of the larynx and hypopharynx are SCC.
-
External auditory canal pain may be referred via the superior laryngeal nerve through the auricular nerve of Arnold (branch of CN X).
-
A “hot potato” voice may be due to the involvement of the base of tongue.
Workup
-
H&P, including hoarseness, pain, dysphagia, odynophagia, otalgia, trismus.
-
All patients should have nasopharyngolaryngoscopy. Fixation of the true cord may be caused by invasion of the cricoarytenoid muscle or joint, or from recurrent laryngeal nerve injury.
-
Esophagoscopy for hypopharnx tumors or if clinically indicated for laryngeal tumors.
-
Bronchoscopy if clinically indicated.
-
Biopsy tumor and/or lymph node(s).
-
Labs include CBC, chemistries, BUN/Cr, LFTs, baseline TSH.
-
Imaging includes thin-cut CT and/or MRI of the head and neck and a CXR. PET scans may be informative for stage III–IV.
-
Preventive dental care and extractions should occur 10–14 days before RT.
-
Baseline speech, swallowing, and nutrition evaluations. If locally-advanced, consider baseline audiometry too.
Staging: Larynx And Hypopharynx Cancer
(AJCC 6th Ed., 2002)
Primary tumor (T) Larynx and hypopharynx TX:Primary tumor cannot be assessed T0:No evidence of primary tumor Tis:Carcinoma in situ Supraglottis T1:Tumor limited to one subsite of supraglottis with normal vocal cord mobility T2:Tumor invades mucosa of more than one adjacent subsite of supraglottis or glottis or region outside the supraglottis (e.g., mucosa of the base of tongue, vallecula, medial wall of pyriform sinus), without fixation of the larynx T3:Tumor limited to larynx with vocal cord fixation and/or invades any of the following: postcricoid area, preepiglottic tissues, paraglottic space, and/or minor thyroid cartilage erosion (e.g., inner cortex) T4a:Moderately advanced local disease. Tumor invades through the thyroid cartilage and/ or invades tissues beyond the larynx (e.g., trachea, soft tissues of neck including deep extrinsic muscle of the tongue, strap muscles, thyroid, or esophagus) T4b:Very advanced local disease. Tumor invades prevertebral space, encases carotid artery, or invades mediastinal structures Glottis T1:Tumor limited to the vocal cord(s) (may involve anterior or posterior commissure) with normal mobility T1a:Tumor limited to one vocal cord T1b:Tumor involves both vocal cords T2:Tumor extends to supraglottis and/or subglottis, and/or with impaired vocal cord mobility T3:Tumor limited to the larynx with vocal cord fixation and/or invasion of paraglottic space, and/or inner cortex of the thyroid cartilage T4a:Moderately advanced local disease. Tumor invades through the outer cortex of the thyroid cartilage and/or invades tissues beyond the larynx (e.g., trachea, soft tissues of neck including deep extrinsic muscle of the tongue, strap muscles, thyroid, or esophagus) T4b:Very advanced local disease. Tumor invades prevertebral space, encases carotid artery, or invades mediastinal structures Subglottis T1:Tumor limited to subglottis T2:Tumor extends to vocal cord(s) with normal or impaired mobility T3:Tumor limited to larynx with vocal cord fixation T4a:Moderately advanced local disease. Tumor invades cricoid or thyroid cartilage and/or invades tissues beyond the larynx (e.g., trachea, soft tissues of neck including deep extrinsic muscles of the tongue, strap muscles, thyroid, or esophagus) T4b:Very advanced local disease. Tumor invades prevertebral space, encases carotid artery, or invades mediastinal structures Hypopharynx T1:Tumor limited to one subsite of hypopharynx and/or 2 cm or less in greatest dimension T2:Tumor invades more than one subsite of hypopharynx or an adjacent site, or measures more than 2 cm, but not more than 4 cm in greatest dimension, without fixation of hemilarynx T3:Tumor more than 4 cm in greatest dimension or with fixation of hemilarynx or extension to esophagus T4a:Moderately advanced local disease. Tumor invades thyroid/cricoid cartilage, hyoid bone, thyroid gland, or central compartment soft tissue* T4b:Very advanced local disease. Tumor invades prevertebral fascia, encases carotid artery, or involves mediastinal structures. *Note: Central compartment soft tissue includes prelaryngeal strap muscles and subcutaneous fat. Regional lymph nodes (N) Larynx and hypopharynx NX:Regional lymph nodes cannot be assessed N0:No regional lymph node metastasis N1:Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension N2a:Metastasis in a single ipsilateral lymph node, more than 3 cm but not more than 6 cm in greatest dimension N2b:Metastasis in multiple ipsilateral lymph nodes, not more than 6 cm in greatest dimension N2c:Metastasis in bilateral or contralateral lymph nodes, not more than 6 cm in greatest dimension N3:Metastasis in a lymph node more than 6 cm in greatest dimension *Note: Metastases at level VII are considered regional lymph node metastases. Distant metastases (M) Larynx and hypopharynx M0:No distant metastasis M1:Distant metastasis | |||
Stage Grouping 0:TisN0M0 I:T1N0M0 II:T2N0M0 III:T3N0M0, T1-3N1M0 IVA:T4aN0-1M0, T1-4aN2M0 IVB:T4b any N M0, any T N3 M0 IVC:Any T, any N, M1 | ∼2/5-Year OS | ||
Larynx | Hypopharynx | ||
I: | 65/35% | 65/35% | |
II: | 80/60% | 60/30% | |
III: | 70/50% | 50/30% | |
IV: | 60/35% | 35/15% | |
Used with permission from the American Joint Committee on Cancer (AJCC), Chicago, IL. The original source for this material is the AJCC Cancer Staging Manual, Sixth Edition (2002), published by Springer Science + Business Media. | |||
Surgical Options
Operation | Indications | Removes | Contraindications/notes |
Limited surgery (stripping or CO2 laser) | Carcinoma in situ | Mucosa of cord | Can lead to thickened or harsh voice. Difficult to determine if invasive CA present |
Cordectomy | Early T1a lesions of middle 1/3 of one TVC | Transoral laser excision of part of one cord. Afterwards, pseudocord forms and patient has useful (but harsh) voice | |
Vertical partial (hemi) laryngectomy | Voice preservation for TVC lesions involving one and <1/3 (<5 mm) of other TVC | Bisects larynx and removes 1/2 of thyroid cartilage, a portion or all of one TVC and up to 1/3 (5 mm) of other TVC | Contraindicated if TVC fixation, >5 mm posterior or >10 mm anterior subglottic extension (because must preserve cricoid), or supraglottic extension to false cord or interarytenoid area |
Supraglottic (horizontal partial) laryngectomy (SGL) | Early supraglottic lesions for voice preservation | Removes epiglottis, aryepiglottic folds, false cords, upper 1/3–1/2 of thyroid cartilage, ± hyoid bone (if epiglottic space involvement). Preserves one or both arytenoids and both TVCs | Contraindicated if exolaryngeal spread, vocal cord fixation, involvement of arytenoids, <3 mm between tumor and anterior commissure, thyroid/cricoid cartilage invasion, and/or inadequate pulmonary function (due to high aspiration risk) |
Extended SGL | Supraglottic lesion with <1 cm base of tongue invasion | Same as SGL with removal of ipsilateral BOT up to circumvalate papillae | |
Total laryngectomy | Indicated for advanced lesions with transglottic or extensive subglottic extension, most pyriform sinus lesions, and/or cartilage invasion | Removes hyoid, thyroid, and cricoid cartilages, epiglottis, strap muscles. Patient left with a permanent tracheostoma and pharynx reconstruction (by suturing to the base of tongue) | Most frequent sites of failure include tracheal stoma, base of tongue, and neck nodes. Rehabilitation options include tracheoesophageal speech, artificial electronic larynx, esophageal speech |
Partial laryngopharyngectomy | Used for small medial and anterior pyriform sinus lesions | Removes false cords, epiglottis, aryepiglottic fold, and pyriform sinus, but TVCs are preserved | Contraindicated if transglottic extension, cartilage invasion, vocal fold paralysis, pyriform apex invasion (b/c below level of TVCs), postcricoid invasion, exolaryngeal spread, or poor pulmonary reserve |
Total laryngopharyngectomy | For more advanced hypopharyngeal lesions | TL plus removal of varying amount of pharyngeal wall | Requires flap or gut graft if total pharyngectomy |
Treatment Recommendations
2002 Stage | Larynx | |
Tis | Endoscopic removal (stripping/laser) or definitive RT | |
T1-2N0 glottic | Definitive RT. Advantage of RT is that failures can be salvaged with partial laryngectomy and still have third chance with salvage total laryngectomy. Alternative, cordectomy or partial laryngectomy ± selective neck dissection. Post-op RT for close/+ margin, PNI, LVSI | |
T1-2N0 supraglottic | Definitive RT. Or, partial supraglottic laryngectomy ± selective neck dissection. Post-op chemo-RT for + margin; post-op RT for close margin, PNI, LVSI | |
Resectable T1-2N+, T3N0/+ requiring total laryngectomy | Concurrent chemo-RT as in RTOG 91–11 (preferred). If < complete response, salvage surgery and neck dissection may be performed. If residual neck mass or initial N2-3, post-RT neck dissection considered Alternative is total laryngectomy, and ipsilateral or bilateral neck dissection (N0-1) or bilateral comprehensive neck dissection (N2-3). Post-op chemo-RT for + margin or nodal ECE. Post-op RT (or chemo-RT with multiple factors) for pT3-4, pN2-3, close margin, PNI, LVSI, ≥1 cm subglottic extension, and/or cartilage invasion Induction chemo × 3c may be considered. If CR or PR, proceed with concurrent chemo-RT as above. If < PR or progression, proceed to surgery and neck dissection as indicated | |
Resectable T4N0/+ | Total laryngectomy and ipsilateral or bilateral neck dissection followed by post-op chemo-RT Alternative for selected patients is definitive concurrent chemo-RT as in RTOG 91–11. Induction chemotherapy may be considered | |
Unresectable T3-4 or N+ | Concurrent chemo-RT. If unable to tolerate chemo, definitive RT with concomitant boost (CB) and consider concurrent cetuximab | |
2002 Stage | Hypopharynx | |
Early T1-2 not requiring total laryngectomy (T1N0-1, small T2N0, T1N2) | Definitive RT. If < complete response, salvage surgery and neck dissection as indicated. If complete response, neck dissection considered for N2-3 | |
Alternatively, partial laryngopharyngectomy and ipsilateral or bilateral selective neck dissection (N0) or comprehensive neck dissection (N+). Post-op chemo-RT for + margin or nodal ECE. Post-op RT (or chemo-RT if multiple factors) for pN2-3, close margin, PNI, LVSI, cartilage invasion | ||
T2-4N0/+ requiring total laryngectomy | Concurrent chemo-RT as extrapolated from RTOG 91–11. Or, induction chemo ×2c (with a third cycle if PR). If CR at primary site, proceed with definitive RT (≥70 Gy). If primary site has only PR, proceed with concurrent chemo-RT. Nonresponders to induction chemo should undergo surgery → post-op RT or chemo-RT as indicated. If residual neck mass after definitive RT or initial N2-3, post-RT neck dissection considered Or, laryngopharyngectomy and selective (N0) or comprehensive neck dissection (N+ or T4). Post-op chemo-RT for + margin or nodal ECE. Post-op RT (or chemo-RT if multiple factors) for pT3-4, pN2-3, close margin, PNI, LVSI, cartilage invasion | |
Unresectable T3-4 or N+ | Concurrent chemo-RT. If unable to tolerate chemo, definitive RT with CB | |
Studies
RT dose fractionation
-
Yamazaki et al. (2006): 180 patients with T1N0 glottic carcinoma randomized to 2 Gy/fx to 60 Gy (if ≤2/3 TVC involved) or 66 Gy (if >2/3 TVC involved) vs. 2.25 Gy/fx to 56.25–63 Gy. The 2.25 Gy/fx arm improved 5-year LC (77Æ92%), but not CSS (97 vs. 100%) or toxicity.
-
RTOG 95–12 (Trotti et al. 2006, abstract): Randomized 250 patients with T2 glottic cancer to 70 Gy in 35 fx vs. 79.2 Gy at 1.2-Gy b.i.d. b.i.d. arm had nonsignificant trend for improved 5-year LC (70Æ79%, p > 0.11), DFS (37Æ51%, p > 0.07), and OS (62Æ73%, p > 0.19), but trial was underpowered.
-
Le et al. (1997) reviewed 398 patients with T1–2 glottic cancer treated with RT alone. On multivariate analysis, overall treatment time ≤43 days, fraction size ≥2.25 Gy, and total dose ≥65 Gy improved LC for T2 lesions. Anterior commissure involvement decreased T1 LC, and impaired cord mobility and subglottic extension decreased T2 LC.
-
Garden et al. (2003) reviewed 230 patients treated with RT alone for T2 glottic cancer. Treatment with ≤2 Gy/fraction had decreased 5-year LC (68%) compared to >2 Gy/fraction (82%) or b.i.d. RT (79%).
-
RTOG 90–03 (Fu et al. 2000; update ASTRO 2005): 268 patients with locally-advanced cancer of the oral cavity, oropharynx, supraglottic larynx, or hypopharynx randomized to 2/70 Gy (standard) vs. 1.2 b.i.d./81.6 Gy (HFX) vs. split-course 1.6 b.i.d./67.2 Gy (with 2 week break) vs. CB-RT to 72 Gy (1.8 Gy/fraction with a 1.5-Gy boost on the last 12 treatment days). On update, 5-year LRF and DFS improved w/ HFX and CB vs. standard fx and split-course. LRF: 60% standard, 58% split-course, 52% CB, 51% HFX. DFS: 21% standard, 27% split-course, 29% CB, 31% HFX. No difference in DM (27–29%), CSS (40–46%). Trend for improved OS with HFX (37 vs. 29–34%).
Chemo-RT for larynx preservation
-
Larynx preservation rates:
-
RT alone: ∼60–70%.
-
Induction chemo Æ RT: ∼65–75%.
-
Concurrent chemo-RT: ∼80–85%.
-
-
VA Larynx Trial (Department of Veterans Affairs Laryngeal Cancer Study Group 1991): 332 patients with III/IV larynx (T1N1 excluded), randomized to surgery and post-op RT (50–74 Gy) vs. induction cisplatin/5-FU × 2c (with a third cycle if PR/CR) Æ RT (66–76 Gy). No routine neck dissection for N+ patients. Chemo allowed 64% larynx preservation at 2 years. There was no difference in 2-year OS (68%). Chemo-RT decreased distant recurrences, but had higher LF (12 vs. 2%). Organ preservation improved quality of life. Salvage laryngectomy was required for 56% of T4 patients.
-
EORTC 24891 (Lefebvre et al. 1996; update ASCO 2004): 202 patients with operable pyriform sinus tumors randomized to surgery Æ post-op RT (50–70 Gy) vs. induction cisplatin/5-FU × 2c (with a third cycle if PR/CR) Æ RT (70 Gy). Nonresponders to chemo underwent surgery Æ RT. Fifty-one to fifty-four percent of patients had a CR after chemo. There was no difference in LRF, and chemo decreased DM (36Æ25%). The 3/5-year functional intact larynx rates were 42/35% with chemo. On update, no difference in 5- or 10-year OS and PFS.
-
RTOG 91–11 (Forastiere et al. 2003; update ASCO 2006): 547 patients with stage III/IV larynx (T2–3 or low-volume T4 without gross cartilage destruction or >1 cm base of tongue invasion, or LN+) randomized to one of three arms: RT alone, chemo Æ RT, or concurrent chemo-RT. RT was 2/70 Gy in all arms. Induction chemo was cisplatin/5-FU × 2c Æ reassessment. If progression or <PR, treated with laryngectomy and post-op RT. If PR/CR Æ third cycle chemo Æ RT. Concurrent chemo was cisplatin × 3c. All patients with cN2 had neck dissection within 8 weeks after RT. On update, concurrent chemo-RT improved 5-year larynx preservation (84%) vs. induction chemo (71%) and RT alone (66%), and LRC (69%) vs. induction chemo (55%) and RT alone (51%). Chemo reduced the rate of DM (13% concurrent, 14% induction vs. 22% RT alone) and improved DFS (39% with chemo vs. 27% with RT alone). No difference in OS (55% concurrent, 59% induction, 54% RT alone).
-
GORTEC 2000–01 (Pointreau et al. 2009): 220 patients with locally-advanced larynx or hypopharynx cancer that required total laryngectomy randomized to 3c of TPF (docetaxel, cisplatin, 5-FU) vs. PF (cisplatin, 5-FU) chemo. If CR, PR, and larynx mobility, patients received RT with or without additional chemo; if no response, patients had surgery and post-op RT with or without additional chemo. TPF improved overall response (80 vs. 59%) and 3-year larynx preservation rate (70 vs. 58%), but had more neutropenia.
-
TAX 324 (Posner et al. 2007): Randomized 501 patients with unresectable stage III/IV head and neck SCC (33% were larynx or hypopharynx) to induction TPF chemo (docetaxel, cisplatin, 5-FU) vs. PF (cisplatin, 5-FU) every 3 weeks for 3 cycles. Patients then had concurrent weekly carboplatin and RT to 70 Gy. TPF improved 3-year OS (48Æ62%) and LRC (62Æ70%), but not DM. TPF increased neutropenia (54Æ84%). Twenty-one percent of patients who got TPF induction were not able to receive subsequent concurrent chemo-RT.
-
EORTC 24954 (Lefebvre et al. 2009): 450 patients with resectable T3–T4 larynx or T2–T4 hypopharynx, N0–N2 randomized to sequential arm (2c cisplatin/5-FU Æ if >50% tumor reduction, 2 more cycles cisplatin/5-FU Æ 70 Gy) vs. alternating arm (4 c cisplatin/5-FU in weeks 1, 4, 7, and 10 alternating with 20 Gy RT during 2-week interval to 60 Gy total). No difference in larynx preservation, PFS, OS, or acute and late toxicity.
-
Cetuximab (Bonner et al. 2006): 424 patients with locoregionally advanced resectable or unresectable stage III–IV SCC of oropharynx, larynx, or hypopharynx randomized to RT or RT + cetuximab given 1 week before RT and weekly during RT. RT options included 2/70 Gy, 1.2 b.i.d./72–76.8 Gy, or CB 72 Gy. Cetuximab increased 3-year LRC (34Æ47%) and OS (45Æ55%). With the exception of acneiform rash and infusion reactions with cetuximab, toxicity was similar.
-
See Oropharynx chapter 7 for list of other key trials of chemo-RT, most of which included patients with larynx or hypopharynx cancer.
Post-op RT and post-op chemo-RT
-
RTOG 95–01 (Cooper et al. 2004): 459 patients with operable cancer of the oral cavity, oropharynx, larynx, or hypopharynx who had ≥2 involved lymph nodes, nodal extracapsular extension, or a + margin randomized to post-op RT (2/60–66 Gy) vs. post-op chemo-RT (2/60–66 Gy and cisplatin ×3 c as in EORTC 22931). Chemo-RT improved 2-year DFS (43Æ54%), LRC (72Æ82%), and had a trend for improved OS (57Æ63%), but increased grade 3–4 toxicity (34Æ77%).
-
EORTC 22931 (Bernier et al. 2004): 334 patients with operable stage III/IV oral cavity, oropharynx, larynx, and hypopharnx cancer randomized to post-op RT (2/66 Gy) vs. post-op chemo-RT (2/66 Gy and cisplatin 100 mg/m2 on days 1, 22, 43). All patients received 54 Gy to the low-risk neck. Eligible stages included pT3–4N0/+, T1–2N2–3, and T1–2N0–1with ECE, +margin, or PNI. Chemo-RT improved 3/5-year DFS (41/36Æ59/47%), 3/5-year OS (49/40Æ65/53%), and 5-year LRC (69Æ82%), but increased grade 3–4 toxicity (21Æ41%).
-
Combined RTOG/EORTC analysis (Bernier 2005): Chemo-RT improved OS, DFS, and LRC for ECE and/or + margins, but provided only trend for improvements (p > 0.06) for stage III–IV, PNI, LVSI, and/or enlarged LN in levels IV–V for OPX or oral cavity tumors based on EORTC data. Patients with ≥2 LN without ECE as their only factor did not benefit from chemo (p > 0.73).
-
Ang et al. (2001): 213 patients with locally-advanced oral cavity, oropharynx, larynx, and hypopharynx cancers treated with surgery randomized by risk factors to post-op RT. Risk factors included >1 node group, ≥2 nodes, nodes >3 cm, microscopic +margins, PNI, oral cavity site, and nodal extracapsular extension. Low-risk: no risk factors Æ no RT. Intermediate risk: 1 risk factor (but not ECE) Æ 1.8/57.6 Gy. High-risk: ECE or ≥2 risk factors Æ 1.8/63 Gy in 7 weeks or in 5 weeks with a CB. The 5-year LRC/OS for low-risk was 90/83%, for intermediate risk 94/66%, and for high-risk 68/42%. Overall treatment time <11 weeks increased LRC, and CB had a trend for improved OS.
Meta-analyses
-
Altered fractionation (Bourhis 2006): Meta-analysis of 15 trials with 6,515 patients, 74% with stage III–IV disease, mostly of oropharynx and larynx, treated with conventional RT (1.8–2/65–70 Gy), hyperfractionated RT (higher dose, same time), accelerated RT (same dose, shorter time), or accelerated RT with reduced total dose. Altered fractionation improved 5-year OS by 3.4%, with greatest benefit for hyperfractionated RT (8% benefit) vs. accelerated RT (1.7–2% benefit). Five-year LRC benefit 6.4% overall, mainly for local as opposed to regional failure. Benefit highest for youngest patients (<50–60 years). No effect of altered fractionation on DM.
-
MACH-NC meta-analysis (Pignon et al. 2009): 93 phase III trials and 17,346 patients. OS benefit (4.5%) at 5 years when chemotherapy was added to RT, with greater benefit for concurrent chemo-RT vs. induction chemo followed by RT (6.5% OS benefit with concurrent chemo-RT). Similar results in trials with post-op RT, conventional, and altered fractionation. No difference between mono or polychemotherapy regimens, but increased benefit with platinum-based compounds. Decreasing benefit with increasing age, with no benefit observed if ≥71 years.
Radiation Techniques
Simulation and field design
-
Simulate the patient supine with the head hyperextended. Wire neck scars and the tracheostoma (if present). Shoulders may be pulled down with straps. Immobilize with a thermoplastic head and shoulder mask. Bolus may be needed for anterior commissure tumors and over the tracheostoma (if present).
-
A 3D conformal or IMRT plan should be used for any but simple opposed-lateral fields in order to spare normal tissues.
-
Computed dosimetry should be used in all cases. Wedges and/or compensating filters may be required.
-
Use fluoroscopy if available to evaluate superior motion of larynx with swallowing to ensure appropriate location of superior border.
-
Glottic larynx traditional field design.
-
For T1N0, use a 5 × 5-cm field with the superior border at the top of the thyroid cartilage, the inferior border at the bottom of the cricoid, a 1-cm skin flash anteriorly, and a 2-cm margin posteriorly (or the anterior edge of the vertebral body) (Fig. 9.1).
-
For glottic T2N0, the field size is increased to 6 × 6 cm with the inferior border one tracheal ring below the cricoid.
-
For T3–4N0, extend the superior border to 2 cm above the angle of the mandible, the posterior border behind the spinous processes, and the inferior border to include 1.5–2 cm margin on the subglottic extent of the tumor. Match the lateral fields to the low-neck AP field. Treat the lateral fields to 42–45 Gy with a small cord block, then move the posterior border off-cord and use an electron boost to treat the elective posterior neck to 50 Gy. Boost the primary with a 1.5-cm margin to 70 Gy with chemo or to 72 Gy with a CB if chemo not used.
Fig. 9.1 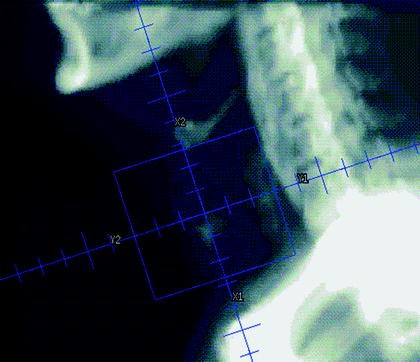
Lateral DRR of a field used to treat a T1 glottic carcinoma
-
-
Supraglottic larynx
-
For T1N0 treat the primary and levels II–III.
-
For T2–3, also treat low-neck because of increased risk of microscopic nodal disease.
-
For advanced cases, treat as described above for glottic.
-
-
Hypopharynx
-
Treat primary and levels II–V and retropharyngeal nodes in all cases.
-
With traditional field design, the superior border is the skull base and mastoid. The inferior border is 1 cm below the inferior extent of disease (or 1 cm below cricoid) on the laterals and matched to the AP low-neck field. With posterior pharyngeal wall tumors, the anterior border does not need to flash the skin. A clothespin may be used to spare the skin anteriorly.
-
-
Post-op
-
With traditional fields, use 3-field technique with stoma in low-neck AP field. Lateral fields cover neopharynx, adenopathy, and 1.5–2 cm margin on preoperative extent of disease.
-
With conventional three-field techniques, the spinal cord is shielded on the lateral fields at the matchline if no gross disease is present. If gross disease is present at the matchline, angling the lateral fields to match the divergence of the AP field may help. A small midline block on the AP field may be necessary.
-
Indications to boost tracheal stoma to 60–66 Gy: emergent tracheostomy, subglottic extension, tumor invasion to soft tissues of neck, extranodal extension in level VI, close/+ margin, scar crosses stoma.
-
-
For low-lying high-risk areas in which matchline would go through the area, extended-field IMRT may be used.
-
Alternatively, may consider caudal tilt technique in which the lateral field gantry is moved 10° anterior and the couch is kicked 10° away from the beam and the SCV field is included in these lateral fields. At 42-Gy, posterior border is brought off-cord and this long strip is supplemented with electrons.
-
-
IMRT
-
IMRT is not recommended for T1–2N0 glottic cancers, but may be considered for more advanced lesions.
-
GTV: clinical and/or radiographic gross disease.
-
CTV1: 0.5–2 cm margin on primary and/or nodal GTV (depending on the presence or absence of anatomic boundaries to microscopic spread).
-
CTV2: elective neck.
-
Individualized planning target volumes are used for the GTV, CTV1, and CTV2.
-

Dose prescriptions
-
T1–2N0 glottic larynx
-
>2 Gy/fx preferred. If 2 Gy/fx is used, total dose >66 Gy.
-
UCSF uses 2.25 Gy/fx.
-
Tis: 56.25–58.5 Gy.
-
T1N0: 63 Gy.
-
T2N0: 65.25 Gy.
-
-
-
T3–4 and LN+ patients
-
Concurrent chemo-RT.
-
Total dose typically 70 Gy in daily fx with cisplatin 100 mg/m2 q3 weeks ×3c.
-
Altered fractionation and multiagent chemo have been evaluated with no consensus on the optimal approach.
-
-
With definitive RT, use altered fractionation. Options:
-
Six fx/week during weeks 2–6: 70 Gy at 2 Gy/fx to primary and gross adenopathy.
-
CB: 72 Gy in 6 weeks (1.8 Gy/fx large field; 1.5 Gy boost as second daily fx during last 12 treatment days).
-
Hyperfractionation: 81.6 Gy in 7 weeks at 1.2 Gy b.i.d.
-
-
-
Post-op RT
-
60–66 Gy at 2 Gy/fx to high-risk areas and the postoperative bed.
-
Post-op chemo-RT indicated for nodal ECE and/or +margin(s) and considered for other risk features, including pT3–4, pN2–3, PNI, LVSI. Concurrent single agent cisplatin 100 mg/m2 q3 weeks recommended.
-
-
Elective neck
-
Uninvolved nodal stations: ≥50–56 Gy at 1.6–2 Gy/fx.
-
-
IMRT
-
IMRT has been shown to reduce long-term toxicity in oropharyngeal, paranasal sinus, and nasopharyngeal cancers by reducing dose to salivary glands, temporal lobes, auditory structures, and the optic apparatus. The use of IMRT for laryngeal and hypopharyngeal cancers is evolving and may be used at the discretion of the treating physician.
-
Simultaneous integrated boost (“dose-painting”) technique used at UCSF.
-
33 fx: GTV = 70 Gy at 2.12-Gy/fx, CTV1 = 59.4 Gy at 1.8-Gy/fx, CTV2 = 54 Gy at 1.64-Gy/fx.
-
-
Alternative techniques.
-
Simultaneous integrated boost in 35 fx.
-
(a)
GTV = 70 Gy at 2-Gy/fx, CTV1 = 63 Gy at 1.8-Gy/fx, CTV2 = 56 Gy at 1.6-Gy/fx.
-
(a)
-
Sequential technique.
-
(a)
Initial lower-dose phase (weeks 1–5) followed by high-dose boost volume phase (weeks 6 and 7) using two to three separate dose plans.
-
(a)
-
CB schedule.
-
(a)
Delivers dose to subclinical targets once daily for 6 weeks, and a separate boost plan as second daily treatment during last 12 treatment days.
-
(a)
-
-
Typically, seven nonopposing beam angles are used.
-
Extended whole field neck technique is typically preferred for larynx and hypopharynx as the glottic larynx is considered a target or when gross disease extends inferiorly and close to the glottic larynx. With this technique, lateral fields are typically not used because they would require treating through the shoulder, so these are replaced with anterior oblique fields.
-
A split field technique with matched conventional low anterior neck field is sometimes used for nasopharynx and oropharynx lesions to reduce the dose to the glottic larynx. In this situation, the matchline is typically just above the arytenoids. A gradient match technique may be used as well.
-
Dose limitations
-
Spinal cord maximum dose ≤45–50 Gy. Brainstem maximum dose ≤54 Gy. Keep 50% of the volume of each parotid ≤20 Gy (if possible) and mean dose <26 Gy. Mandible maximum dose ≤70 Gy. Brachial plexus dose <60 Gy.
-
Tracheostomas are limited to ≤50 Gy unless (1) significant subglottic extension, (2) emergent tracheostomy, (3) extranodal extension in neck level VI, or (4) close/+ margin, in which case it is boosted to 60–66 Gy.
-
For other head and neck primary sites, the goal mean dose to the larynx is <35–45 Gy and 2/3 should be kept below 50 Gy.
-
70 Gy carries 5% risk of laryngeal cartilage necrosis.
COMPLICATIONS
-
Complications of RT include mucositis, dermatitis, xerostomia, dysgeusia, soft-tissue fibrosis, hypothyroidism, and rarely radionecrosis, pharyngocutaneous fistula, or carotid rupture.
-
Perioperative complications of surgery include bleeding, airway obstruction, infection, and wound complications. Post-op complications include webs, stenosis, chondritis, fistulas, and aspiration.
-
Patients need ≥2,000 calories/day to avoid malnutrition. Supplements (e.g., Boost or Ensure) and/or feeding tubes may be used.
-
Amifostine may decrease xerostomia and mucositis, but it may be associated with significant side effects (e.g., hypotension, N/V).
FOLLOW-UP
-
H&P every 1–3 month for year 1, every 2–4 month for year 2, every 4–6 month for years 3–5, and every 6–12 months thereafter. Posttreatment baseline imaging recommended, and thereafter, as clinically indicated. CXR annually. TSH every 6–12 month if neck irradiated. Speech, swallow, dental, and hearing evaluations and rehabilitation as indicated. Smoking cessation counseling.
-
If recurrence is suspected but biopsy is negative, follow closely (at least monthly) until it resolves.
References
References
Ang KK, Trotti A, Brown BW, et al. Randomized trial addressing risk features and time factors of surgery plus radiotherapy in advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys 2001;51:571-578.
Bernier J, Cooper JS, Pajak TF, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck. 2005;27(10):843-50.
Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004;350:1945-1952.
Bonner JA, Harari PM, Giralt J, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med 2006; 354: 567-578.
Bourhis J, Overgaard J, Audry H, et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: a meta-analysis. Lancet. Sep 2 2006;368(9538):843-854.
Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004;350:1937-1944.
Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349:2091-2098.
Fu KK, Pajak TF, Trotti A, et al. A Radiation Therapy Oncology Group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat Oncol Biol Phys 2000;48:7-16.
Garden AS. The Larynx and Hypopharynx. In: Cox JD, Ang KK, editors. Radiation oncology: rationale, technique, results. 8th ed. St. Louis: Mosby; 2003. pp. 255-281.
Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. The Department of Veterans Affairs Laryngeal Cancer Study Group. N Engl J Med 1991;324:1685-1690.
Le QT, Fu KK, Kroll S, et al. Influence of fraction size, total dose, and overall time on local control of T1-T2 glottic carcinoma. Int J Radiat Oncol Biol Phys 1997;39:115-126.
Lefebvre JL, Rolland F, Tesselaar M et al. Phase 3 randomized trial on larynx preservation comparing sequential vs alternating chemotherapy and radiotherapy. J Natl Cancer Inst. 2009;101(3):142-52.
Lefebvre JL, Chevalier D, Luboinski B, et al. Larynx preservation in pyriform sinus cancer: preliminary results of a European Organization for Research and Treatment of Cancer phase III trial. EORTC Head and Neck Cancer Cooperative Group. J Natl Cancer Inst 1996;88:890-899.
Pignon JP, Maître AL, Maillard E, et al. Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): An update on 93 randomised trials and 17,346 patients. Radiother Oncol. 2009 May 14. [Epub ahead of print].
Pointreau Y, Garaud P, Chapet S, et al. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J Natl Cancer Inst 2009;101(7):498-506.
Posner MR, Hershock DM, Blajman CR, et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer. N Engl J Med 2007;357:1705-1715.
Trotti A, Pajak T, Emami B, et al. A randomized trial of hyperfractionation versus standard fractionation in T2 squamous cell carcinoma of the vocal cord. Int J Radiat Oncol Biol Phys 2006;66(3):S15.
Yamazaki H, Nishiyama K, Tanaka E, et al. Radiotherapy for early glottic carcinoma (T1N0M0): results of prospective randomized study of radiation fraction size and overall treatment time. Int J Radiat Oncol Biol Phys 2006;64(1):77-82
Further Reading
Adelstein DJ, Li Y, Adams GL, et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J Clin Oncol 2003;21:92-98.
Brizel DM, Albers ME, Fisher SR, et al. Hyperfractionated irradiation with or without concurrent chemotherapy for locally advanced head and neck cancer. N Engl J Med 1998;338:1798-1804.
Forastiere A, Maor M, Weber R, et al. Long-term Results of Intergroup RTOG 91-11: A Phase III Trial to Preserve the Larynx -Induction Cisplatin/5-FU and Radiation Therapy versus Concurrent Cisplatin and Radiation Therapy versus Radiation Therapy, ASCO National Proceedings, 2006.
Garden AS, Forster K, Wong PF, et al. Results of radiotherapy for T2N0 glottic carcinoma: does the “2” stand for twice-daily treatment? Int J Radiat Oncol Biol Phys 2003;55:322-328.
Greene FL, American Joint Committee on Cancer., American Cancer Society. AJCC cancer staging manual. 6th ed. New York: Springer; 2002.
Lee N, Phillips TL. Cancer of the Larynx. In: Leibel SA, Phillips TL, editors. Textbook of radiation oncology. 2nd ed. Philadelphia: Saunders; 2004. pp. 679-698.
Lefebvre JL, Ang KK. Larynx preservation consensus panel. Larynx preservation clinical trial design: key issues and recommendations-a consensus panel summary. Int J Radiat Oncol Biol Phys. 2009;73(5):1293-1303.
Lefebvre JL, Chevalier D, Luboinski B et al. Is laryngeal preservation (LP) with induction chemotherapy (ICT) safe in the treatment of hypopharyngeal SCC? Final results of the phase III EORTC 24891 trial. Journal of Clinical Oncology, 2004 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 22, No 14S (July 15 Supplement), 2004: 5531
Mendenhall WM, Hinerman RW, Amdur RJ, et al. Larynx. In: Perez CA, Brady LW, Halperin EC, et al., editors. Principles and practice of radiation oncology. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2004. pp. 1094-1116.
National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Head and Neck Cancers. Available at: http://www.nccn.org/professionals/physician_gls/PDF/head-and-neck.pdf. Accessed on May 19, 2009.
Shah HK, Khuntia D, Hoffman HT, Harari PM. Hypopharynx. In: Halperin EC, Perez CA, Brady LW, et al., editors. Principles and practice of radiation oncology. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2008. pp. 958-974.
Zelefsky MJ. Cancer of the Hypopharynx. In: Leibel SA, Phillips TL, editors. Textbook of radiation oncology. 2nd ed. Philadelphia: Saunders; 2004. pp. 657-678.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2010 Springer-Verlag New York
About this chapter
Cite this chapter
Pejavar, S., Hansen, E.K., Yom, S.S., Schechter, N.R. (2010). Larynx and Hypopharynx Cancer. In: Hansen, E., Roach, M. (eds) Handbook of Evidence-Based Radiation Oncology. Springer, New York, NY. https://doi.org/10.1007/978-0-387-92988-0_9
Download citation
DOI: https://doi.org/10.1007/978-0-387-92988-0_9
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-0-387-92987-3
Online ISBN: 978-0-387-92988-0
eBook Packages: MedicineMedicine (R0)