
Abstract
This chapter will describe the sensory innervation of the head and neck with special emphasis on anatomy relevant to regional anesthesia. The trigeminal (fifth cranial) nerve provides the majority of sensory innervation of the head, with exclusive coverage of the face. Fibers from the cervical plexus and the greater and lesser occipital nerves provide sensory innervation to the neck and back of the head. The information in this chapter will be useful for performing blocks described in Chaps. 15, 16, 17, and 18.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Trigeminal nerve
- Ophthalmic nerve
- Maxillary nerve
- Mandibular nerve
- Cervical plexus
- Greater occipital nerve
- Lesser occipital nerve
- Nerve of Arnold
1 Clinical Anatomy of Trigeminal Nerve
-
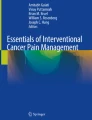
The trigeminal nerve (cranial nerve V), the largest of the cranial nerves, is fundamentally the sensory nerve of the head and supplies sensory innervation to the entire face all the way from the lambdoidal suture on the vertex of the skull to the bottom of the chin. Of its three major divisions, the ophthalmic and maxillary nerves are purely sensory, while the mandibular nerve is a mixed sensory and motor nerve, the motor fibers being distributed primarily to the muscles of mastication. In addition, the trigeminal nerve acts as a conduit for postganglionic parasympathetic fibers from the ciliary, pterygopalatine, mandibular, and otic ganglia in the head. The preganglionic fibers destined for these ganglia arise from the oculomotor nerve (for the ciliary ganglion), facial nerve (for the pterygopalatine and submandibular ganglia), and glossopharyngeal nerve (for the otic ganglion).
-
The sensory and motor roots of the trigeminal nerve arise from the ventral aspect of the base of the pons. Sensory branches are sent to the large semilunar (trigeminal, semilunar, or Gasserian) ganglion, which lies in a shallow depression, recess, or cleft in the meningeal layer of dura (trigeminal or Meckel’s cave; trigeminal fossa) in the middle cranial fossa on the dorsal surface of the petrous temporal bone near its tip or apex. The ganglion’s anterior aspect gives rise to three main divisions: the ophthalmic (V1), maxillary (V2), and mandibular (V3) nerves (Fig. 9.1).
Fig. 9.1 
Major branches of the trigeminal nerve: ophthalmic, maxillary, and mandibular nerves. The roots of the trigeminal nerve arise from the base of the pons and form the Gasserian ganglion
-
A smaller motor root lies underneath the main trigeminal ganglion and supplies motor fibers to the mandibular nerve. These motor fibers supply mostly the muscles of mastication, namely, the masseter, temporalis, medial and lateral pterygoids, as well as the anterior belly of the digastric, mylohyoid, tensor tympani, and tensor veli palatini muscles.
-
The three major divisions of the trigeminal nerve exit the cranium through three distinct foramina – the ophthalmic nerve enters the orbit through the superior orbital fissure, where it divides into its three main branches, the frontal, lacrimal and nasociliary nerves. The maxillary nerve passes through the foramen rotundum to cross over the top of the pterygopalatine fossa and then enters the floor of the orbit through the inferior orbital fissure. After exiting the skull through the foramen rotundum, the maxillary nerve courses anteriorly over the pterygopalatine fossa and enters the floor of the orbit through the infraorbital fissure as the infraorbital nerve; the infraorbital nerve courses in the infraorbital canal, and descending branches include the greater palatine, lesser palatine, and nasopalatine and superior alveolar nerves. The mandibular nerve courses into the infratemporal fossa through the foramen ovale and divides into its two major branches, the lingual nerve and inferior alveolar nerve. The terminal branches of these three divisions, destined for the face, namely, the supraorbital, infraorbital, and mental nerves, exit the skull through the supraorbital, infraorbital, and mental foramina, respectively, and usually lie vertically in-line with each other in the plane of the pupil (neonate, Fig. 9.2a; adolescent, Fig. 9.2b). The greater palatine, lesser palatine, and nasopalatine nerves exit the palate through corresponding foramina of the posterior aspect of the secondary palate and anterior aspect of the primary palate. Although the terminal branches are the nerves that we focus on for many common regional anesthesia blocks, it is important to remember that each of the trigeminal divisions send branches internally to supply the oral and nasal mucosa as well as the mucosa of the paranasal sinuses external branches to supply the lateral aspect of the face.
Fig. 9.2 
Neonate (a) and adolescent (b) skull models depicting three distinct foramina, through which branches of the trigeminal nerve exit the cranium. The ophthalmic, maxillary, and mandibular nerves exit through the supraorbital foramen (SO), infraorbital foramen (IO), and mental foramen (M), respectively


1.1 Ophthalmic Nerve (V1 Division of the Trigeminal Nerve, Pure Sensory)
-
The uppermost ophthalmic branch of the trigeminal nerve is a pure sensory nerve and passes through the superior orbital fissure (sphenoidal fissure) into the orbit.
-
The nerve divides into three main branches – lacrimal, frontal, and nasociliary – just prior to entering the orbit through the superior orbital fissure.
-
The lacrimal nerve is the smallest of the three divisions. It enters the orbit through the superior orbital fissure and communicates with the zygomaticotemporal branch of the maxillary nerve. It courses through the lateral aspect of the orbit over the lateral rectus muscle. The lacrimal nerve then enters the lacrimal gland and innervates it with parasympathetic secretomotor fibers (from the zygomaticotemporal nerve) and the adjoining conjunctiva with sensory fibers. The nerve eventually pierces the orbital septum to innervate the skin of the lateral aspect of the upper eyelid, joining with filaments from the facial nerve.
-
The division’s largest branch, the frontal nerve, courses anteriorly through the orbit along the upper surface of the levator palpebrae superioris muscle and bifurcates into its terminal sensory branches, the larger supraorbital nerve laterally and the smaller supratrochlear nerve medially.
-
The supraorbital nerve courses anteriorly between the levator palpebrae superioris and the periosteum of the orbital roof, continues anteromedially towards the trochlea, exits the orbit through the supraorbital foramen (or notch in some cases), and finally curves superiorly into the forehead before branching into its medial and lateral branches. Anesthesia of the supraorbital nerve blocks the conjunctiva and skin of the upper eyelid as well as the ipsilateral upper forehead as far back as the lambdoidal suture (Figs. 9.3 and 9.4). It also supplies sensory fibers to the mucous membrane of the frontal air sinuses.
Fig. 9.3 
Cutaneous innervation by the trigeminal nerve and cervical plexus
Fig. 9.4 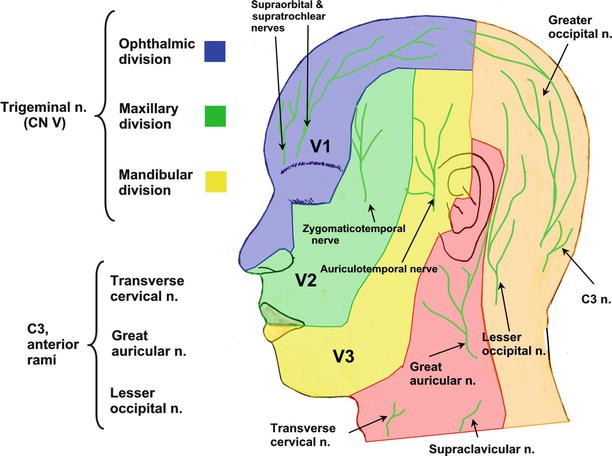
Cutaneous innervation by the trigeminal nerve, cervical plexus, and dorsal nerve roots
-
The supratrochlear nerve traverses the orbit along the same plane as the supraorbital nerve but just medial to it, passes over the trochlea, and enters the front of the face via the frontal notch (or just medial to the supraorbital foramen or notch). It then courses superiorly into the forehead. As it passes through the orbit, the nerve sends a branch to join the infratrochlear branch of the nasociliary nerve. This nerve supplies sensation to the medial part of the upper eyelid, the conjunctiva, and the lower-middle forehead (Fig. 9.4).
-
The nasociliary nerve is the intermediate branch (in terms of size) of the frontal nerve and passes obliquely through the orbit to reach its medial aspect. Its anterior and posterior ethmoidal branches pass through the ethmoidal foramina to enter the cranium. The nerve then travels on the upper surface of the cribriform plate of the ethmoid bone underneath the dura mater and descends through a slitlike opening in the crista galli to enter the nasal cavity. The nasociliary nerve supplies two internal nasal branches that innervate the lateral wall of the nasal cavity and the mucous membrane of the front part of the nasal septum.
-
The ethmoidal branches also supply the mucosa lining the ethmoid air cells. The posterior branch leaves the orbit through the posterior ethmoidal foramen and innervates the sphenoidal sinus. The nasociliary nerve terminates in the infratrochlear and anterior ethmoidal branches; the former supplies the conjunctiva and skin of the medial aspect of the upper eyelid, while the latter supplies the anterior and middle ethmoid cells and then sends two internal branches that innervate the mucous membranes of the front part of the nasal septum and lateral nasal wall. The anterior ethmoidal branch eventually exits the face as the external nasal nerve, which innervates the skin of the nasal ala and apex of the nose.


1.2 Maxillary Nerve (V2 Division of the Trigeminal Nerve, Pure Sensory)
-
The maxillary nerve, like the ophthalmic, also contains purely sensory fibers. It exits the skull through the foramen rotundum, courses beneath the skull base anteriorly, and crosses over the upper part of the pterygopalatine (sphenopalatine) fossa (medial to the lateral pterygoid plate on each side) before entering the orbit through the inferior orbital fissure as the infraorbital nerve (Fig. 9.5).
Fig. 9.5 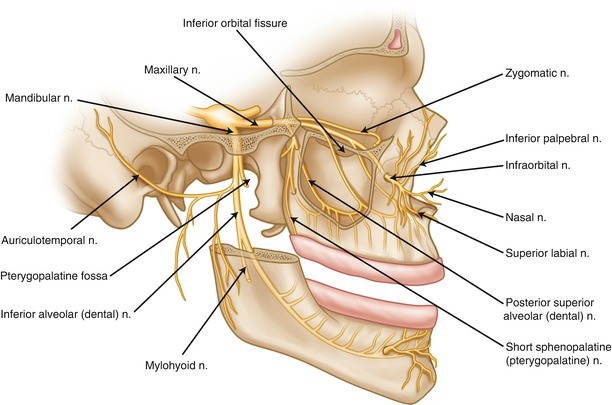
Anatomy of the maxillary and mandibular nerves
-
Suspended from the nerve as it courses over the pterygopalatine fossa is the parasympathetic pterygopalatine, or more commonly called sphenopalatine ganglion, which lies within the fossa. Several branches of the maxillary nerve appear to arise from the pterygopalatine ganglion; however, the nerve fibers within them simply pass through the sphenopalatine ganglion without synapsing. Although they seem to be branches of the ganglion, they are in reality branches of the maxillary nerve just coursing through the ganglion and very intimately associated with it.
-
During its course through the infraorbital groove and/or canal in the floor of the orbit, the maxillary nerve gives off two superior alveolar (dental) branches (the middle and anterior superior alveolar nerves) that supply the maxillary teeth and gingivae before terminating as the infraorbital nerve, which surfaces onto the face through the infraorbital foramen (Fig. 9.5).
-
The middle and anterior superior alveolar (dental) nerves arise from the main trunk of the nerve as it passes through the infraorbital groove and/or canal, while the posterior superior alveolar nerve is given off just before it enters the floor of the orbit. The nerve pierces the infratemporal surface of the maxilla to run under the mucous membrane of the maxillary sinus, which it supplies. It then breaks up into small branches to form the posterior part of the superior dental plexus to supply the maxillary molars. Branches given off from within the pterygopalatine fossa include the zygomatic nerve to the orbit (with its zygomaticotemporal and zygomaticofacial branches), the short sphenopalatine (pterygopalatine) nerves, and the posterior superior alveolar (dental) nerve (Fig. 9.5).
-
The zygomaticofacial nerve passes along the infero-lateral aspect of the orbit and exits through a foramen in the zygoma to supply the skin on the cheek. The zygomaticofacial nerve merges with nerve fibers from the palpebral branches of the maxillary nerve and zygomatic branches from the facial nerve to form a plexus. The zygomaticotemporal nerve sends a branch to join the lacrimal nerve, providing parasympathetic, secretomotor innervation to the lacrimal gland. The posterior superior alveolar nerve also arises high in the pterygopalatine fossa before the maxillary nerve enters the infraorbital groove. The nerve then pierces the infratemporal surface of the maxilla to course under the mucous membrane of the maxillary sinus which it supplies. The posterior, anterior, and middle superior alveolar (dental) nerves form the superior dental plexus, which innervates the maxillary teeth and gingivae. Together with the infraorbital nerve, these superior alveolar nerves also supply sensory innervation to the mucosa lining the maxillary sinus.
-
The palatine nerves (Fig. 9.6), the greater (anterior) and lesser (middle and posterior), are the terminal sensory endings of the maxillary nerve and emerge as branches from the pterygopalatine ganglion. The sensory fibers within them pass through the ganglion without synapsing. They are distributed to the roof of the mouth, the soft palate, the palatine tonsil, and the mucous membrane lining the nasal cavity. The branches descend through the pterygopalatine (greater palatine) canal and emerge on the hard palate; the anterior branch emerges through the greater palatine foramen (Fig. 9.6), while the middle/posterior branches emerge via a minor/lesser palatine foramen (an opening behind the greater palatine foramen). The sensory supply of the greater branch includes the gums and the mucosa and glands of the hard palate; the sensory supply of the lesser branches includes the uvula, the tonsils, and the soft palate.
Fig. 9.6 
Left side: the greater and lesser palatine nerves emerge on the hard palate from the greater and lesser palatine foramen, respectively. The nasopalatine nerve emerges from the incisive foramen. Right side: sensory innervation of the hard palate
-
Nasal branches (also arising from the ganglion) enter the nasal cavity through the sphenopalatine foramen to be distributed in lateral and medial groups to the posterior aspects of the superior and middle nasal conchae laterally and the posterior part of the roof of the nasal septum medially. The largest of these nerves is the nasopalatine (long sphenopalatine) nerve which courses anteroinferiorly on the nasal septum and then descends through the incisive foramen in the anterior aspect of the hard palate to be distributed to the roof of the mouth (Fig. 9.6).
-
The pharyngeal nerve arises from the posterior aspect of the pterygopalatine ganglion and courses through the palatovaginal canal to supply the mucosa of the nasopharynx just posterior to the opening of the Eustachian (auditory, pharyngotympanic) tube.
-
The terminal infraorbital nerve passes through the inferior orbital fissure into the floor of the orbit, where it courses through the infraorbital groove and/or canal (just below the eye and lateral to the nose), and reaches the facial surface of the maxilla. It then divides into the inferior palpebral nerves (lower eyelid), external and internal nasal nerves (wings or ala of the nose), and medial and lateral branches of the superior labial nerve (upper lip).
-
The infraorbital nerve innervates the lower eyelid and upper lip, including the philtrum, the lateral portion of the nasal cavity and the skin of the cheek. Blockade of the infraorbital nerve produces anesthesia of the middle third of the ipsilateral face (Fig. 9.5).


1.3 Mandibular Nerve (V3 Division of the Trigeminal Nerve, Sensory and Motor to Muscles of Mastication)
-
The mandibular nerve is the third and largest branch of the trigeminal and the only mixed nerve (i.e., with both a sensory and a motor component). It exits the skull posterior to the maxillary nerve (Fig. 9.5) through the foramen ovale, enters the infratemporal fossa, and forms a short, thick trunk, which divides quickly into a small, mainly motor, anterior trunk and a large, mainly sensory, posterior trunk.
-
The main sensory posterior (mandibular) trunk receives a few filaments from the motor root, and its branches are the auriculotemporal, lingual, and inferior alveolar (dental) nerves.
-
The anterior trunk of the mandibular nerve gives rise to the buccal nerve (sensory) and the masseteric, deep temporal, and lateral pterygoid nerves (motor).
-
The main branch (posterior trunk) continues as the inferior alveolar (dental) nerve medial to the ramus of the mandible. After giving off the nerve to the mylohyoid, the inferior alveolar nerve enters the mandibular canal through the mandibular foramen, which is guarded by a tongue-shaped process of bone called the lingula (used as a landmark for locating the nerve during an inferior alveolar nerve block) (Fig. 9.5). Within the mandibular canal the nerve courses inferiorly and anteriorly to innervate the mandibular teeth and gingivae. The nerve then curves anteriorly to follow the body and anterior aspect of the mandible and exits through the mental foramen, located on the mental process of the mandible, giving off the incisive nerve and its terminal branch – the mental nerve.
-
Other terminal nerves of the posterior trunk include the lingual nerve (lying under the lingual mucosa and supplying the mucosa of the floor of the mouth, mandibular gingivae, and general sensation to the anterior two-thirds of tongue) and the auriculotemporal nerve (dividing into superficial temporal branches behind the temporomandibular joint to supply the joint, the external acoustic meatus and auricle of the ear, and the scalp over the temple). The auriculotemporal nerve usually has two roots encircling the middle meningeal artery within the infratemporal fossa.
-
The mental nerve, with its three branches (one ascending to reach the chin and two descending to innervate the skin and mucous membrane of the lower lip), is the primary target of anesthesia.
-
The mandibular nerve also supplies the skin of the temporal region, lower jaw, and chin (Figs. 9.4 and 9.5); the mandibular gingival and labial mucosae; and the meninges of the middle cranial fossa.
2 Clinical Anatomy of the Cervical Plexus
-
The cervical plexus is a mixed spinal nerve plexus in the neck formed from the anterior (ventral) rami of the first four cervical nerves.
-
Sensory and motor fibers supplying the neck and posterior scalp arise from these four cervical (C1–C4) spinal nerves (Fig. 9.7). The cervical plexus is unique in that it divides early into cutaneous branches (penetrating the cervical fascia to supply the skin and subcutaneous tissues of the neck) and muscular branches (deeper branches which innervate the neck muscles, the diaphragm and joints of the cervical spine), which can be blocked separately. The branches of the plexus provide sensory innervation to the skin and subcutaneous tissues of the anterior and lateral aspects of the neck; part of the posterior scalp; the skin inside, above, and posterior to the external ear; and the posterior aspect and lower third of the auricle or pinna of the ear (Fig. 9.4). The cervical plexus lies deep to the sternocleidomastoid muscle (Fig. 9.8) and internal jugular vein, but is anterior to the scalenus medius and levator scapulae muscles.
Fig. 9.7 
Schematic of the cervical plexus, which arises from the anterior primary rami of C1–C4
Fig. 9.8 
Cutaneous innervation by the superficial cervical plexus
-
Each ramus (except the first) divides into ascending and descending parts that unite in communicating loops; the first or C2 and C3 loop supplies superficial sensory branches to the head and neck; the second or C3 and C4 loop gives rise to cutaneous nerves supplying the shoulder region and upper thorax as well as muscular (motor) branches which go deep to supply the muscles. C3, C4, and C5 anterior rami form the phrenic nerve which supplies the diaphragm (its sole motor supply), as well as the fibrous pericardium, mediastinal pleura and diaphragmatic pleura and peritoneum with sensory fibers.
-
Motor branches innervating the strap muscles of the neck (sternohyoid, sternothyroid, and omohyoid) emerge from the ansa cervicalis, a neural loop formed from the joining of the descendens hypoglossi (C1) and descendens cervicalis (C2 and C3) which form the ansa cervicalis usually embedded within the anterior aspect of the carotid sheath deep to the sternocleidomastoid.
-
Classic cervical plexus anesthesia can be achieved by injecting along the tubercles of the transverse processes of the cervical vertebrae, producing both motor and sensory blockade. The transverse processes of the cervical vertebrae form peculiar elongated troughs for the emergence of the cervical spinal nerve roots (Fig. 9.9). These troughs lie immediately lateral to an aperture for the cephalad passage of the vertebral artery, the foramen transversarium. At the lateral end of the transverse process, the trough is guarded by an anterior and a posterior tubercle, the anterior of which can often easily be palpated.
Fig. 9.9 
Nerve roots of the cervical plexus emerging from the troughs formed by the transverse processes, posterior and lateral to the vertebral artery
-
These tubercles also serve as the attachment sites for the anterior and middle scalene muscles, which form a compartment for the cervical plexus as well as the brachial plexus immediately below. The compartment at this level is less developed than the one formed around the brachial plexus.
-
The deep muscular branches curl anteriorly around the lateral border of the scalenus anterior and proceed caudally and medially. Many branches serve the deep anterior neck muscles; other branches include the superior root of the ansa cervicalis, the trapezius branch of the plexus, and the phrenic nerve. These deep muscular branches also supply the sternocleidomastoid muscle as they pass behind it.
-
The sensory fibers emerge from behind the scalenus anterior muscle but are separate from the motor branches and continue laterally to emerge superficially under the posterior border (clavicular head) of the sternocleidomastoid muscle at about its midpoint (Erb’s point). The branches, including the lesser occipital nerve, great auricular nerve, transverse cervical nerve, and supraclavicular nerves (medial, intermediate and lateral [posterior] branches), innervate the skin on the anterior and posterior aspects of the neck and shoulder (Fig. 9.8).
-
After arising from the second and third cervical nerve roots, the great auricular nerve ascends up to the angle of the mandible and gives off anterior and posterior branches to supply the skin over the parotid gland and the mastoid process (Fig. 9.8).



3 Clinical Anatomy of Occipital Nerves
The posterior scalp over the occipital region is innervated by sensory fibers of the greater and lesser occipital nerves.
3.1 Lesser Occipital Nerve (C2)
-
This nerve arises from the second (sometimes also the third) anterior cervical ramus and is a superficial (cutaneous) nerve. It traverses cephalad from the posterior edge of the sternocleidomastoid muscle towards the top of the head, where it pierces the deep fascia and ascends the scalp behind the auricle, dividing into several branches (Fig. 9.10).
Fig. 9.10 
Greater and lesser occipital nerve distributions. Sites of needle insertion are marked with X

3.2 Greater Occipital Nerve (C2)
-
The greater occipital nerve arises from the posterior ramus of the second cervical spinal nerve as its medial branch (the cervical plexus arises from the anterior rami) and travels in a cranial direction, medial to the occipital artery (Fig. 9.10), to reach the skin at a location within the aponeurosis of the trapezius muscle just inferior to the superior nuchal line. At this point, it provides branches medially to supply the head and laterally to supply the skin of the scalp in the area behind the auricle (post-auricular area). It supplies motor fibers to the semispinalis capitis muscle. The lateral branch supplies the splenius, longissimus, and semispinalis capitis muscles.
4 Clinical Anatomy of the Nerve of Arnold
-
The Nerve of Arnold is the sensory auricular branch of the vagus nerve. It arises from the jugular (superior) ganglion of the vagus nerve. Soon after its origin, it is joined by a filament from the petrous (inferior) ganglion of the glossopharyngeal nerve, after which it passes behind the internal jugular vein and enters the mastoid canaliculus on the lateral wall of the jugular fossa. Passing through the substance of the temporal bone, it crosses the facial canal about 4 mm (in adult) above the stylomastoid foramen, where it gives off an ascending branch which joins the facial nerve. The nerve then passes through the tympanomastoid fissure between the mastoid process and the temporal bone, becomes superficial, and divides into two branches. One branch joins the posterior auricular nerve, while the other travels to the skin of the posterior auricular area and to the posterior wall and floor of the external acoustic meatus which it supplies with sensory innervation (Fig. 9.11). The nerve also provides sensory innervation to the inferior portion of the outer aspect of the tympanic membrane.
Fig. 9.11 
Sensory distribution of the Nerve of Arnold, indicated by green-shaded area

Suggested Reading
Chapter 28: Neck. In: Standring S, editor. Gray’s anatomy. 40th ed. London: Churchill Livingstone; 2008. p. 455–62.
Chapter 29: Face and scalp. In: Standring S, editor. Gray’s anatomy. 40th ed. London: Churchill Livingstone; 2008. p. 492–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this chapter
Cite this chapter
Merritt, G., Walji, A.H., Tsui, B.C.H. (2016). Clinical Anatomy of the Head and Neck. In: Tsui, B., Suresh, S. (eds) Pediatric Atlas of Ultrasound- and Nerve Stimulation-Guided Regional Anesthesia. Springer, New York, NY. https://doi.org/10.1007/978-0-387-79964-3_9
Download citation
DOI: https://doi.org/10.1007/978-0-387-79964-3_9
Publisher Name: Springer, New York, NY
Print ISBN: 978-0-387-79963-6
Online ISBN: 978-0-387-79964-3
eBook Packages: MedicineMedicine (R0)