
Abstract
The central epidemiologic features of cancer of the endometrium are the following: a much increased risk associated with obesity, evident both in premenopausal and postmenopausal women; a decreased risk with increasing parity; a decreased risk with increasing duration of use of combination-type oral contraceptives (COCs); an increased risk with menopausal estrogen therapy (ET) use; and a marked reduction in this risk when a progestin is added to ET (estrogen–progestin therapy, EPT) and continuous-combined EPT may be associated with a decreased risk, especially in heavier women. These observations are readily explained by a simple “unopposed estrogen hypothesis”; that is, estrogen “unopposed” by a progestin increases risk. The basis for this hypothesis is that estrogen unopposed by a progestin increases cell division in the endometrium. Analysis shows that reducing the standard dose of ET by as much as a half will have no effect on the ET-associated risk of endometrial cancer. This hypothesis also provides an explanation of why 1 year of COC use has a smaller preventive effect than a birth. It also suggests that the recently introduced COCs with an increase in the number of days of active pill intake from 21 to 24 days per 28-day COC cycle will significantly increase the protective effect of COC use. Use of the progestin-containing intrauterine system (IUS) with its continuous release of progestin reduces the risk of endometrial cancer to a marked extent; a year of such use may provide as much protection as a birth. Some of this progestin-containing IUS effect may, however, not be due to the progestin as non-hormonal IU devices (IUDs) have also been shown to decrease endometrial cancer risk although to a lesser extent. It is now clear that the protective effect of parity is markedly affected by the age at which the last birth occurs: for the same number of total births, there is a 45 % greater effect of a last birth after age 40 than a last birth before age 25. It remains to be seen if this age effect is also seen with the protection afforded by hormonal IUSs or with COCs where the active pills are given for 12 weeks out of every 13.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The risk of endometrial cancer increases markedly with increasing body mass index (BMI; kg/m2) and use of menopausal estrogen therapy (ET), while increasing parity and use of combination-type oral contraceptives (COCs) decrease risk significantly. The effects of these factors can be explained by a simple “unopposed estrogen hypothesis” for endometrial cancer [1, 2]; that is, endometrial cancer risk is increased by exposure of the endometrium to estrogen “unopposed” by progesterone or a synthetic progestin, and the increased risk is essentially caused by the increased mitotic activity of the endometrium induced by such exposure. Increased mitotic activity as a general risk factor is supported by a considerable amount of evidence; essentially, for a given tissue, the mitotic rate plays a central role in determining the rates at which the underlying carcinogenic processes, such as mutation, proliferation, and cell death, will occur in some stem cell compartment [3, 4].
The Age Incidence of Endometrial Cancer
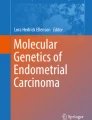
The incidence of the common non-hormone-dependent adult cancers (e.g., stomach, colon) rises continuously and increasingly rapidly with age. On a log–log scale the age-incidence curve of such cancers is linear. The incidence of endometrial cancer also increases with age, but there is a distinct slowing of the rate of increase after menopause. This is clearly seen in Fig. 1, which shows the age-specific incidence rates for endometrial cancer in the Birmingham Region of the UK from 1968 to 1972 [5]. Note: This “historical” data is used in order to avoid distortion due to high hysterectomy rates, high obesity rates, and widespread use of COCs and menopausal hormone therapy in the USA, all of which profoundly affect the incidence of endometrial cancer. It should be noted that the incidence of endometrial cancer does not decrease at menopause; it is just that its rate of increase is sharply curtailed.


Age-specific incidence rates for endometrial cancer in the Birmingham region of the UK, 1968–1972
Figure 1 indicates that the hormonal pattern of premenopausal women [cyclic production of relatively large amounts of estradiol (E2) and progesterone (P4)] causes a much greater rate of increase in risk of endometrial cancer than the hormonal pattern of postmenopausal women (constant low E2 and effectively no P4). The premenopausal level of E2 “unopposed” by progesterone although present for only 50–60 % of the cycle has a greater effect than the constant low postmenopausal E2: we would expect that some of the greater increase in the premenopausal period is caused by the repopulation of the functionalis of the endometrium at the start of each cycle [6, 7].
The increase in the incidence of endometrial cancer is very rapid at premenopausal ages: from age 35 to 40, the incidence increases ~250 % while age increases only 14 %, and years since menarche only increases from ~22 to ~27 years, a 23 % increase. This large increase in incidence is because incidence increases as the 6th power of years since menarche (this is shown approximately in Fig. 1). It is this power relationship that explains the large preventive effects of relatively short periods of COC use and the large increases in risk associated with relatively short periods of menopausal ET use.
Estrogen Dose and Endometrial Cell Mitotic Rate
E2 is the predominant intracellular estrogen in the endometrium and estrogens stimulate mitosis in endometrial cells [8]. Progestins dramatically reduce mitotic activity by reducing the concentration of estrogen receptors, by increasing the metabolism of E2 to the less active estrone [9], and by stimulating differentiation of endometrial cells to a secretory state.
Figure 2 shows the plasma concentrations of E2 and P4 and the mitotic rate of the glandular endometrial cells during the menstrual cycle [10,11,12]. The mitotic rate reaches a near maximal level early on in the cycle around day 5. The rate stays roughly constant for ~14 days, until around day 19, after which it drops to a very low level when P4 increases. The maximal mitotic rate is induced by the relatively low early follicular plasma E2 concentration of ~50 pg/ml; later increases in E2 levels do not appear to induce any further increase in mitotic rate. Thus, there appears to be an upper limit, no greater than ~50 pg/ml, to the effective plasma concentration of E2.


Plasma concentrations of estradiol and progesterone and endometrial mitotic rate by day of cycle
The existence of a low ceiling of E2 effect has important implications. In particular, this limit implies that, in premenopausal women, changes in E2 will have little effect. Increases in E2 concentration above normal will not increase endometrial cell division, while decreases in E2 may, at most, only decrease mitotic activity for the few days of the cycle during which E2 is normally close to the basal ~50 pg/ml level. In postmenopausal women, E2 plasma levels are strongly correlated with increasing BMI—the average levels increase from ~7.5 pg/ml at a BMI of 20 kg/m2 to ~13.2 pg/ml at a BMI of 30 kg/m2 [13]. The E2 plasma levels are well below the early follicular level of ~50 pg/ml even in women with a high BMI, and increases in E2 may, therefore, increase the endometrial mitotic rate until the upper limit for E2 effect is reached. We can refine this estimate of the upper limit by considering the effects of menopausal ET (see below).
Bioavailable E2
Plasma E2 is bound with high affinity to sex hormone-binding globulin (SHBG) and SHBG-bound E2 is not bioavailable [14]. SHBG levels decrease significantly with increasing BMI, so that, for example, SHBG levels decrease ~43 % with a BMI change from 20 to 30 kg/m2. The proportion of E2 that is bioavailable increases from ~49 % at a BMI of 20 kg/m2 to ~63 % at a BMI of 30 kg/m2; the average bioavailable E2 plasma levels increase from ~3.7 pg/ml at a BMI of 20 kg/m2 to ~8.3 pg/ml at a BMI of 30 kg/m2. (The above figures were calculated using the mass action approach of Södergard et al. [15] with the estimated association constants as given by Dunn et al. [16], and with the E2 and SHBG values given by the Endogenous Hormones and Breast Cancer Collaborative Group [13].)
Body Mass Index
Increasing BMI is strongly associated with a greatly increasing risk of endometrial cancer, the risk approximately doubling between a BMI of 23 kg/m2 and a BMI of 30 kg/m2 [17]. This is evident both in premenopausal [18] and postmenopausal women [19]. At premenopausal ages, increasing BMI, especially obesity, is associated with an increased frequency of anovulatory cycles [20], in which in the absence of P4, the endometrium is stimulated throughout the cycle. During the postmenopausal period, increasing BMI is associated with higher levels of E2 from conversion of androgens to estrogens, as well as lower levels of SHBG, so that the estrogen is more bioactive [1, 21].
With increasing BMI, the protective effect of an earlier menopause will decrease until a situation is reached where there will be no effect at all as can be deduced from the results of several studies [22].
Menopausal Estrogen Therapy (ET)
The dose of menopausal ET most commonly used in the USA, that is, conjugated estrogens (CE) at 0.625 mg/day, results in endometrial cell proliferation approximately equal to that found during the follicular phase of the menstrual cycle [8]. Thus, it is to be expected that ET will substantially increase a woman’s risk of developing endometrial cancer, and that this increase will be strongly dependent on the duration of use. In our study, an increased risk of ~16.8 % per year of use was found [22] and similar risks have been reported in other studies [23,24,25].
The increased risk from ET use is strongly dependent on BMI. In our study [22] the increased risk per year of use of ~16.8 % was an average of 19.3 % for women with a BMI of <30 kg/m2 and of 7.7 % for women with a BMI of ≥30 kg/m2. Similar results were reported by Brinton and coworkers [26] with a relative risk of 3.8 for women with a BMI of <28 kg/m2 and 1.05 for women with a BMI of ≥28 kg/m2. The Million Women Study [27] found that ET use was associated with no increase in risk in women with a BMI of ≥30 kg/m2. We conservatively estimate that there is no increased risk from ET use in women with a BMI ≥32 kg/m2. Plasma E2 is ~14.8 pg/ml in a 32 kg/m2 woman [13], and it can be concluded that the ceiling of effective non-SHBG-bound plasma E2 is ~9.7 pg/ml (calculated as described above).
All effective doses of ET are likely to result in plasma estrogen levels above this ceiling level. This can be seen most easily by considering the plasma estrogen levels of a woman on the 50 μg E2 transdermal patch, which achieves roughly the same effects as a CE dose of 0.625 mg/day. A 50 μg E2 patch increases plasma E2 levels by ~30 pg/ml [28,29,30] and has little effect on SHBG [31, 32], so that non-SHBG-bound E2 will increase from ~3.7 pg/ml to ~18.4 pg/ml in a 20 kg/m2 woman. Thus, the steady-state plasma non-SHBG-bound E2 level of all women on a 50 μg E2 patch is well above the ceiling level of ~9.7 pg/ml. Even at only half the dose, i.e., a 25 μg E2 patch, the non-SHBG-bound E2 will be ~11.0 pg/ml in a 20 kg/m2 woman, still above the ceiling. Thus, different doses of ET should have similar effects, as has been observed [25].
Menopausal Estrogen–Progestin Therapy
To reduce the increased endometrial cancer risk from menopausal ET, progestins were added to ET [estrogen–progestin therapy (EPT)] for between 10 and 13 days per month in a sequential fashion (sequential EPT).
Although there was some individual variation in response the increased endometrial cell proliferation associated with CE at 0.625 mg/day was generally reduced to the levels seen in the secretory phase of the cycle by the addition of a progestin equivalent to oral medroxyprogesterone acetate (MPA) at 5 mg/day [8, 33,34,35,36,37]. This and other findings [38,39,40] persuaded most prescribers that 10–13 days of progestin was sufficient to abolish any increased endometrial cancer risk, and this became standard practice [40].
Key and Pike [2] argued that if endometrial cell proliferation in the basalis layer was the key to increased risk from ET, there would still be an increased risk from sequential EPT even with 13 days of progestin use, since there would still be unopposed estrogen for around 15 days per treatment cycle. Moreover, Fig. 1 shows that endometrial cancer incidence is increasing rapidly in the premenopausal period, so that the notion that mimicking the progestin phase of the menstrual cycle would provide adequate protection was always suspect. Epidemiologic studies have consistently reported increased risks with sequential ET use and a meta-analysis shows a relative risk per year of use of 1.05 (95 % CI 1.02–1.08), clearly an increased risk although much smaller than was seen with ET.
Sequential EPT causes regular bleeding in many women and is associated with other negative side effects; as a result, continuous-combined EPT (ccEPT) regimens were prescribed in which the estrogen and progestin are always taken together. If the dose of progestin used in ccEPT is sufficient to block endometrial epithelial cell division, then one would predict that there should be no increased risk of endometrial cancer from use of ccEPT, and that there would be a decreased risk in heavier women as it would be expected that the progestin component would block endogenous estrogen in addition to blocking the action of the estrogen in the EPT. The Women’s Health Initiative randomized trial of ccEPT found a decreased risk of endometrial cancer with a relative risk of 0.81 (95 % CI 0.48–1.36; based on 27 and 31 cases of endometrial cancer) during 5.6 years of use [41]. Similar results were observed in the much smaller HERS II randomized trial [42], and in a number of epidemiological studies [27, 43,44,45]; and the only two studies reporting effects by BMI found much larger protective effects in heavier women [27, 44]. A number of these studies were done in Europe where higher doses of nor-testosterone-derived progestins were used [27, 36, 43, 45]. A number of other studies with MPA at 2.5 mg/day did not show a decreased risk with ccEPT [22, 46,47,48]: this would be in agreement with the results of studies that showed that endometrial epithelial cell proliferation is slightly increased with ccEPT with MPA at 2.5 mg/day [36, 49, 50]. It is clear that there is little risk from ccEPT, but whether there is a decreased risk with the low-dose 2.5 mg MPA ccEPT is unclear.
Parity
Endometrial cancer risk decreases significantly with increasing parity. A comprehensive meta-analysis found a relative risk per birth of 0.86, i.e., a 14 % reduction in risk per birth. Two and three births are therefore estimated to reduce risk by 26 % (relative risk of 0.862) and 36 % (relative risk of 0.863), respectively. A meta-analysis of epidemiological studies contributing data to the Epidemiology of Endometrial Cancer Consortium found that the relative risk (for a given number of births) was reduced by a factor of 0.88 for each 5 years later that the last birth took place. Compared to a woman who has her last birth under age 25, a woman who has the same number of births but has her last birth after age 35 has a 33 % lower risk of endometrial cancer and if she has her last birth after age 40 a 45 % lower risk. Women with only a single birth tend to have the birth late and this appears to be the reason that some earlier analyses had found the first birth to be more protective than subsequent births. A number of authors have suggested that these results support the hypothesis that the reduction in risk of endometrial cancer is related to a mechanical shed of malignant or premalignant cells at each delivery [51].
Hormonal Contraception
Combined Oral Contraceptives
The use of COCs is associated with a marked long-term reduction in endometrial cancer risk. The recently published comprehensive meta-analysis of epidemiological studies of COC use and endometrial cancer found that the reduction in risk increased with increasing duration of use: every 5 years of use was associated with a relative risk of 0.76 (i.e., a 24 % reduction in risk) [52]. Use of COCs for 10 years is associated with a 42 % reduction in risk (relative risk of 0.762). The reduction was still evident 30 years after use of COCs had stopped and there was no evidence of any change in the protective effect with changes in the doses and formulations of COCs over time. The reduction in risk will be somewhat higher at younger ages and lower at much older ages. Whether the extent of protection is greater with later age of COC use has not been investigated.
COCs are a mixture of an estrogen (ethinyl-estradiol) and a progestin. Their composition is such that they are progestin dominant for the endometrium, so that endometrial proliferation is much reduced during a COC cycle compared to a normal menstrual cycle. The observed reduction in risk with COC use is what we would predict from a mathematical model of incidence if the total endometrial proliferation over a 28-day cycle on a COC is reduced by a third compared to a normal cycle [53]. The common COCs have been packaged with 21 active and 7 placebo pills (21/7). Very recently, they have been packaged with 24 active and 4 placebo pills (24/4) or 84 active and 7 placebo pills (84/7). These COCs will be associated with less proliferation than the 21/7 OCs and should thus be associated with a greater protective effect against endometrial cancer.
Levonorgestrel Intrauterine System (LNG-IUS)
The use of the intrauterine system of delivery of the progestin, levonorgestrel, as a progestin-only contraceptive results in atrophy of the glandular epithelium [54]. The LNG-IUS used was designed for 5 years of use, and their use would thus be predicted to significantly reduce the risk of endometrial cancer. In the single epidemiological study of the effects of the LNG-IUS on endometrial cancer risk a 50 % reduction in risk was found with the purchase of a single LNG-IUS and a 75 % reduction in risk was found with the purchase of two or more LNG-IUSs. This study was done using the National Reimbursement Registry linked to the Finnish Cancer Registry and the LNG-IUS had been prescribed for treatment of menorrhagia. Comparison was made of the endometrial cancer rate in the LNG-IUS users to the rate in the general population. The study did not adjust for parity, BMI or COC use, or for the fact that the women were being treated with the LNG-IUS for menorrhagia. They also did not adjust the general population rate for the proportion of women in the general population who had been hysterectomized, but this would have made their figure for reduction in risk even greater. The study should be considered as providing strong suggestive evidence of a protective effect. As we noted above, the finding is what we would expect from the effect of the LNG-IUS on endometrial glandular proliferation, and from the substantial evidence that the use of the LNG-IUS in women with endometrial hyperplasia results in disease regression in the majority of cases [55] and use of LNG-IUS has been found to eradicate some early-stage endometrial cancers [56, 57]. Further studies are clearly needed.
Depot Medroxyprogesterone Acetate
Depot medroxyprogesterone acetate (DMPA) administered every 3 months at a 150 mg dose produces profound progestogenic effects on the endometrium; this is as expected, since the dose of progestin is sufficient to suppress ovulation throughout the 3 months, and the serum level of MPA soon after injection is some 25 times higher than is needed to suppress ovulation [58]. The single case-control study of DMPA and endometrial cancer was conducted in Thailand by the WHO in the late 1980s: the study found a 79 % lower risk (relative risk of 0.21; 95 % CI 0.06–0.79) of endometrial cancer for ever use of DMPA based on 3 cases and 84 controls [59]. No additional studies have been reported. Our understanding of the etiology of endometrial cancer strongly suggests that DMPA use will be associated with a lower risk of endometrial cancer with the effect being greater the longer the duration of use.
Non-hormonal Intrauterine Devices
The earliest epidemiological studies of the possible effects of non-hormonal intrauterine devices (IUDs) on endometrial cancer risk were made in the early 1990s. A comprehensive meta-analyses of the results of the published studies was reported by Beining et al. [60] and more recently Felix et al. [61] conducted a detailed analysis of the individual-level data on cases and controls included in the studies contributing to the Epidemiology of Endometrial Cancer Consortium (E2C2). Almost all individual studies found a reduction in risk with use of an IUD. The overall estimate of the reduction in risk found by Beining et al. was 46 % (95 % CI: 38–53 %) while the reduction in risk found by Felix et al. was 11 % (95 % CI: 34–21 % increase) for a copper-containing IUD and 31 % (95 % CI: 42–18 %) for an inert IUD. A majority of the studies included in the meta-analysis of Beining et al. were not members of E2C2 and these non-E2C2 studies contributed significantly to the greater protection they found for IUD use. For most studies Beining et al. did not have information on the type of IUD, and almost all of the studies did not adequately adjust for other endometrial cancer risk factors. Looking at the results as a whole it appears that more recent use is associated with a greater protective effect but a protective effect is present for at least 10 years after stopping IUD use. It is not clear that there is a duration of use effect.
Although Felix et al. found only a small protective effect of the copper IUD, the single study investigating the effect of the copper IUD on endometrial glandular proliferation found an 80 % reduction in Ki67 comparing baseline to 6 months after IUD insertion (all comparisons made in the mid-follicular phase of the cycle) [62], so that we would have predicted a significantly reduced risk of endometrial cancer. In Table 2 in Felix et al. the crude relative risk for the copper IUD is 0.26; this becomes 0.89 after adjustment. This is in sharp contrast to the results for an inert IUD where the crude relative risk of 0.71 is hardly changed at all, becoming 0.69, after adjustment. It is not clear why there is such a difference in the effect of adjustment.
The protective effect of IUD use may be quite large and further analyses and possibly further studies are needed.
Smoking
Cigarette smoking has been consistently found to be associated with an approximately 25 % lower risk of endometrial cancer in postmenopausal women [63,64,65]. Risk was lower in current than in past smokers and some studies found a greater reduction in risk with increasing numbers of cigarettes smoked per day. There was no reduction in risk among premenopausal women. Smokers are known to have an earlier age at menopause and their average BMI is lower than that of nonsmokers, but adjustment for these factors did not explain the protective effect in postmenopausal women. Multiple studies have found no effect of smoking on serum estrogen levels in postmenopausal women but did find consistent elevations of androstenedione [66,67,68,69]. Although a number of investigators suggested that the elevated levels of androstenedione could be causally related to the protective effect of smoking, epidemiological studies of androgen levels as they relate to endometrial cancer risk have found no evidence for such an effect [70]. At present no viable hypothesis has been proposed that would explain the protective effect of smoking. Since the effect is quite large this area might benefit from direct study of the biological effect of smoking on endometrial cells.
Chemoprevention
The use of COCs is a most effective approach to chemoprevention of endometrial cancer. The protection is very long-lasting and should be further increased with the newer formulations of COCs with a higher ratio of active to placebo pills. DMPA, the progestin-containing IUS-LNG, and IUDs also provide protection against endometrial cancer, probably greater protection than is observed with COCs used for the same length of time.
The substantial reduction in risk of endometrial cancer seen with a late age at last birth suggests that endometrial sloughing may have a substantial protective effect. Further detailed studies of the endometrium—at or soon after delivery, at the end of the sloughing period while taking COCs with different ratios of active to placebo pills, and after varying periods of using DMPA, LNG-IUS, and IUDs—should lead to a deeper understanding of the basis of the protective effect of births and how we might hope to capitalize on the late age of births’ protective effect.
Conclusions
-
Proliferation of the endometrium is dependent on estrogen unopposed by a progestin.
-
Maximum proliferation is achieved at a relatively low level of bioavailable estradiol.
-
Basal estrogen levels in the postmenopausal age group are dependent on body mass index (BMI).
-
Bioavailable estradiol levels are also dependent on BMI.
-
The above facts explain many epidemiologic observations concerning the risk of developing endometrial cancer in relation to age, obesity, and type of exogenous hormonal use.
-
COCs, other hormonal contraceptives, and IUDs provide substantial long-lasting protective effects against endometrial cancer and newer formulations of COCs will in all likelihood provide even greater protection than has been seen with “traditional” COCs.
References
Siiteri PK. Steroid hormones and endometrial cancer. Cancer Res. 1978;38:4360–6.
Key TJ, Pike MC. The dose-effect relationship between ‘unopposed’ oestrogens and endometrial mitotic rate: its central role in explaining and predicting endometrial cancer risk. Br J Cancer. 1988;57:205–12.
Cairns J. Somatic stem cells and the kinetics of mutagenesis and carcinogenesis. Proc Natl Acad Sci U S A. 2002;99:10567–70.
Preston-Martin S, Pike MC, Ross RK, Jones PA, Henderson BE. Increased cell division as a cause of human cancer. Cancer Res. 1990;50:7415–21.
Waterhouse J, Muir C, Correa P, Powell J. Cancer incidence in five continents. IARC Sci Publ. 1976;15:1–583.
Ferenczy A. Studies on the cytodynamics of human endometrial regeneration. I. Scanning electron microscopy. Am J Obstet Gynecol. 1976;124:64–74.
Salamonsen LA. Tissue injury and repair in the female human reproductive tract. Reproduction. 2003;125:301–11.
Whitehead MI, Townsend PT, Pryse-Davies J, Ryder TA, King RJ. Effects of estrogens and progestins on the biochemistry and morphology of the postmenopausal endometrium. N Engl J Med. 1981;305:1599–605.
Tseng L, Gurpide E. Induction of human endometrial estradiol dehydrogenase by progestins. Endocrinology. 1975;97:825–33.
Ferenczy A, Bertrand G, Gelfand MM. Proliferation kinetics of human endometrium during the normal menstrual cycle. Am J Obstet Gynecol. 1979;133:859–67.
Goebelsmann UM, Mishell DR. The menstrual cycle. In: Mishell DR, Davajian V, editors. Reproductive endocrinology, infertility and contraception. Philadelphia: F.A. Davis Company; 1979. p. 67–89.
Thorneycroft IH, Mishell Jr DR, Stone SC, Kharma KM, Nakamura RM. The relation of serum 17-hydroxyprogesterone and estradiol-17-beta levels during the human menstrual cycle. Am J Obstet Gynecol. 1971;111:947–51.
Endogenous Hormones and Breast Cancer Collaborative Group. Body mass index, serum sex hormones, and breast cancer risk in postmenopausal women. J Natl Cancer Inst. 2003;95:1218–26.
Pardridge WM. Serum bioavailability of sex steroid hormones. Clin Endocrinol Metab. 1986;15:259–78.
Sodergard R, Backstrom T, Shanbhag V, Carstensen H. Calculation of free and bound fractions of testosterone and estradiol-17 beta to human plasma proteins at body temperature. J Steroid Biochem. 1982;16:801–10.
Dunn JF, Nisula BC, Rodbard D. Transport of steroid hormones: binding of 21 endogenous steroids to both testosterone-binding globulin and corticosteroid-binding globulin in human plasma. J Clin Endocrinol Metab. 1981;53:58–68.
Friedenreich C, Cust A, Lahmann PH, Steindorf K, Boutron-Ruault MC, Clavel-Chapelon F, et al. Anthropometric factors and risk of endometrial cancer: the European prospective investigation into cancer and nutrition. Cancer Causes Control. 2007;18:399–413.
Henderson BE, Casagrande JT, Pike MC, Mack T, Rosario I, Duke A. The epidemiology of endometrial cancer in young women. Br J Cancer. 1983;47:749–56.
Weiderpass E, Persson I, Adami HO, Magnusson C, Lindgren A, Baron JA. Body size in different periods of life, diabetes mellitus, hypertension, and risk of postmenopausal endometrial cancer (Sweden). Cancer Causes Control. 2000;11:185–92.
Hartz AJ, Barboriak PN, Wong A, Katayama KP, Rimm AA. The association of obesity with infertility and related menstrual abnormalities in women. Int J Obes. 1979;3:57–73.
Siiteri PK. Extraglandular oestrogen formation and serum binding of oestradiol: relationship to cancer. J Endocrinol. 1981;89:119–29.
Pike MC, Peters RK, Cozen W, Probst-Hensch NM, Felix JC, Wan PC, et al. Estrogen-progestin replacement therapy and endometrial cancer. J Natl Cancer Inst. 1997;89:1110–6.
Beresford SAA, Weiss NS, Voigt LF, McKnight B. Risk of endometrial cancer in relation to use of oestrogen combined with cyclic progestagen therapy in postmenopausal women. Lancet. 1997;349:458–61.
Persson I, Weiderpass E, Bergkvist L, Bergstrom R, Schairer C. Risks of breast and endometrial cancer after estrogen and estrogen-progestin replacement. Cancer Causes Control. 1999;10:253–60.
Cushing KL, Weiss NS, Voigt LF, McKnight B, Beresford SA. Risk of endometrial cancer in relation to use of low-dose, unopposed estrogens. Obstet Gynecol. 1998;91:35–9.
Brinton LA, Hoover RN. Estrogen replacement therapy and endometrial cancer risk: unresolved issues. Obstet Gynecol. 1993;81:265–71.
Beral V, Bull D, Reeves G, Collaborators MWS. Endometrial cancer and hormone-replacement therapy in the Million Women Study. Lancet. 2005;365:1543–51.
Powers MS, Schenkel L, Darley PE, Good WR, Balestra JC, Place VA. Pharmacokinetics and pharmacodynamics of transdermal dosage forms of 17B-estradiol: comparison with conventional oral estrogens used for hormone replacement. Am J Obstet Gynecol. 1985;152:1099–106.
Schiff I, Sela HK, Cramer D, Tulchinskiy D, Ryan KJ. Endometrial hyperplasia in women on cyclic or continuous estrogen regimens. Fertil Steril. 1982;37:79–82.
Selby PL, Peacock M. Dose dependent response of symptoms, pituitary, and bone to transdermal oestrogen in postmenopausal women. BMJ. 1986;293:1337–9.
Nachtigall LE, Raju U, Banerjee S, Wan L, Levitz M. Serum estradiol-binding profiles in postmenopausal women undergoing three common estrogen replacement therapies: associations with sex hormone-binding globulin, estradiol, and estrone levels. Menopause. 2000;7:243–50.
Ropponen A, Aittomaki K, Vihma V, Tikkanen MJ, Ylikorkala O. Effects of oral and transdermal estradiol administration on levels of sex hormone-binding globulin in postmenopausal women with and without a history of intrahepatic cholestasis of pregnancy. J Clin Endocrinol Metab. 2005;90:3431–4.
Whitehead MI, Townsend PT, Pryse-Davies J, Ryder T, Lane G, Siddle N, et al. Actions of progestins on the morphology and biochemistry of the endometrium of postmenopausal women receiving low-dose estrogen therapy. Am J Obstet Gynecol. 1982;142:791–5.
King RJB, Townsend PT, Siddle N, Whitehead MI, Taylor RW. Regulation of estrogen and progesterone receptor levels in epithelium and stroma from pre- and postmenopausal endometrial. J Steroid Biochem. 1982;16:21–9.
Lane G, Siddle NC, Ryder TA, Pryse-Davies J, King RJB, Whitehead MI. Dose dependent effects of oral progesterone on the oestrogenised postmenopausal endometrium. BMJ. 1983;287:1241–5.
King RJB, Whitehead MI. Assessment of the potency of orally administered progestins in women. Fertil Steril. 1986;46:1062–6.
Lane G, Siddle NC, Ryder TA, Pryse-Davies J, King RJB, Whitehead MI. Is provera the ideal progestogen for addition to postmenopausal estrogen therapy? Fertil Steril. 1986;45:345–52.
Flowers CE, Wilborn WH, Hyde BM. Mechanisms of uterine bleeding in postmenopausal patients receiving estrogen alone or with a progestin. Obstet Gynecol. 1983;61:135–43.
Paterson MEL, Wade-Evans T, Sturdee DW, Thom MH, Studd JWW. Endometrial disease after treatment with oestrogens and progestogens in the climacteric. BMJ. 1980;22:822–4.
King RJB, Whitehead MI. Progestin action in relation to the prevention of endometrial abnormalities. In: Raynaud JP, Ojasoo T, Martini L, editors. Medical Management of Endometriosis. Raven Press: New York, 1984;67–77.
Anderson GL, Judd HL, Kaunitz AM, Barad DH, Beresford SA, Pettinger M, et al. Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: the Women’s Health Initiative randomized trial. JAMA. 2003;290:1739–48.
Hulley S, Furberg C, Barrett-Connor E, Cauley J, Grady D, Haskell W, et al. Noncardiovascular disease outcomes during 6.8 years of hormone therapy: Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA. 2002;288:58–66.
Weiderpass E, Baron JA, Adami HO, Magnusson C, Lindgren A, Bergstrom R, et al. Low-potency oestrogen and risk of endometrial cancer: a case-control study. Lancet. 1999;353:1824–8.
Doherty JA, Cushing-Haugen KL, Saltzman BS, Voigt LF, Hill DA, Beresford SA, et al. Long-term use of postmenopausal estrogen and progestin hormone therapies and the risk of endometrial cancer. Am J Obstet Gynecol. 2007;197:139.e1–7.
Allen NE, Tsilidis KK, Key TJ, Dossus L, Kaaks R, Lund E, et al. Menopausal hormone therapy and risk of endometrial carcinoma among postmenopausal women in the European Prospective Investigation Into Cancer and Nutrition. Am J Epidemiol. 2010;172:1394–403.
Newcomb PA, Trentham-Dietz A. Patterns of postmenopausal progestin use with estrogen in relation to endometrial cancer (United States). Cancer Causes Control. 2003;14:195–201.
Razavi P, Pike MC, Horn-Ross PL, Templeman C, Bernstein L, Ursin G. Long-term postmenopausal hormone therapy and endometrial cancer. Cancer Epidemiol Biomarkers Prev. 2010;19:475–83.
Jain MG, Rohan TE, Howe GR. Hormone replacement therapy and endometrial cancer in Ontario, Canada. J Clin Epidemiol. 2000;53:385–91.
Langer RD, Landgren BM, Rymer J, Helmond FA, Investigators O. Effects of tibolone and continuous combined conjugated equine estrogen/medroxyprogesterone acetate on the endometrium and vaginal bleeding: results of the OPAL study. Am J Obstet Gynecol. 2006;195:1320–7.
Dahmoun M, Odmark IS, Risberg B, Karlsson MG, Pavlenko T, Backstrom T. Apoptosis, proliferation, and sex steroid receptors in postmenopausal endometrium before and during HRT. Maturitas. 2004;49:114–23.
Albrektsen G, Heuch I, Tretli S, Kvale G. Is the risk of cancer of the corpus uteri reduced by a recent pregnancy? A prospective study of 765,756 Norwegian women. Int J Cancer. 1995;61:485–90.
Collaborative Group on Epidemiological Studies on Endometrial Cancer. Endometrial cancer and oral contraceptives: an individual participant meta-analysis of 27 276 women with endometrial cancer from 36 epidemiological studies. Lancet Oncol. 2015;16:1061–70.
Pike MC. Age-related factors in cancers of the breast, ovary, and endometrium. J Chronic Dis. 1987;40 Suppl 2:59S–69.
Guttinger A, Critchley HO. Endometrial effects of intrauterine levonorgestrel. Contraception. 2007;75(6 Suppl):S93–8.
Whiteman MK, Zapata LB, Tepper NK, Marchbanks PA, Curtis KM. Use of contraceptive methods among women with endometrial hyperplasia: a systematic review. Contraception. 2010;82:56–63.
Montz FJ, Bristow RE, Bovicelli A, Tomacruz R, Kurman RJ. Intrauterine progesterone treatment of early endometrial cancer. Am J Obstet Gynecol. 2002;186:651–7.
Orbo A, Rise CE, Mutter GL. Regression of latent endometrial precancers by progestin infiltrated intrauterine device. Cancer Res. 2006;66:5613–7.
Fotherby K, Koetsawang S, Mathrubutham M. Pharmacokinetic study of different doses of depo provera. Contraception. 1980;22:527–36.
WHO Collaborative Study of Neoplasia and Steroid Contraceptives. Depot-medroxyprogesterone acetate (DMPA) and risk of endometrial cancer. Int J Cancer. 1991;49:186–90.
Beining RM, Dennis LK, Smith EM, Dokras A. Meta-analysis of intrauterine device use and risk of endometrial cancer. Ann Epidemiol. 2008;18:492–9.
Felix AS, Gaudet MM, La Vecchia C, Nagle CM, Shu XO, Weiderpass E, et al. Intrauterine devices and endometrial cancer risk: a pooled analysis of the Epidemiology of Endometrial Cancer Consortium. Int J Cancer. 2015;136:E410–22.
Guleria K, Agarwal N, Mishra K, Gulati R, Mehendiratta A. Evaluation of endometrial steroid receptors and cell mitotic activity in women using copper intrauterine device: can Cu-T prevent endometrial cancer? J Obstet Gynaecol Res. 2004;30:181–7.
Zhou B, Yang L, Sun Q, Cong R, Gu H, Tang N, et al. Cigarette smoking and the risk of endometrial cancer: a meta-analysis. Am J Med. 2008;121:501–8. e3.
Al-Zoughool M, Dossus L, Kaaks R, Clavel-Chapelon F, Tjonneland A, Olsen A, et al. Risk of endometrial cancer in relationship to cigarette smoking: results from the EPIC study. Int J Cancer. 2007;121:2741–7.
Felix AS, Yang HP, Gierach GL, Park Y, Brinton LA. Cigarette smoking and endometrial carcinoma risk: the role of effect modification and tumor heterogeneity. Cancer Causes Control. 2014;25:479–89.
Friedman AJ, Ravnikar VA, Barbieri RL. Serum steroid hormone profiles in postmenopausal smokers and nonsmokers. Fertil Steril. 1987;47:398–401.
Khaw K-T, Tazuke S, Barrett-Connor E. Cigarette smoking and levels of adrenal androgens in postmenopausal women. N Engl J Med. 1988;318:1705–9.
Cauley JA, Gutai JP, Kuller LH, LeDonne D, Powell JG. The epidemiology of serum sex hormones in postmenopausal women. Am J Epidemiol. 1989;129:1120–31.
Schlemmer A, Jensen J, Riis BJ, Christiansen C. Smoking induces increased androgen levels in early post-menopausal women. Maturitas. 1990;12:99–104.
Allen NE, Key TJ, Dossus L, Rinaldi S, Cust A, Lukanova A, et al. Endogenous sex hormones and endometrial cancer risk in women in the European Prospective Investigation into Cancer and Nutrition (EPIC). Endocr Relat Cancer. 2008;15:485–97.
Acknowledgement
Research reported in this publication was partially supported by NCI under award number P30CA008748 (PI: Thompson) to Memorial Sloan Kettering Cancer Center.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Pike, M.C., Chung, K., Olson, S., Pearce, C.L., Wu, A.H. (2016). The Essential Epidemiology of Cancer of the Endometrium: An Update. In: Muggia, F., Santin, A.D., Oliva, E. (eds) Uterine Cancer. Current Clinical Oncology. Springer, Cham. https://doi.org/10.1007/7631_2016_11
Download citation
DOI: https://doi.org/10.1007/7631_2016_11
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-47267-6
Online ISBN: 978-3-319-47269-0
eBook Packages: MedicineMedicine (R0)