
Abstract
Systemic sclerosis is a connective tissue disease characterized by tissue fibrosis leading to interstitial lung disease. Transforming growth factor-β (TGF-β) has been of interest as a potential diagnostic marker and also as a drug target in systemic sclerosis. The aim of this study was to assess the serum content of TGF-β1 in patients with systemic sclerosis and to assess its potential role in tissue fibrosis. The study included 30 patients, 5 men and 25 women, of the mean age of 46.9 ± 12.8 years, diagnosed with systemic sclerosis. The control group consisted of 19 women of the mean age of 28.4 ± 7.8 years, diagnosed with primary Raynaud’s disease. TGF-β1 serum levels were measured, chest imaging examinations were performed, and fibrotic tissue changes were assessed using the modified Rodnan Skin Score. We found that the mean serum TGF-β1 content in patients with systemic sclerosis was 598.7 ± 242.6 pg/mL, whereas it was 568.4 ± 322.2 pg/mL in the control group (p = 0.378). We also failed to substantiate any significant relationship between TGF-β1 serum levels and the severity of pulmonary and skin fibrosis in systemic sclerosis. In conclusion, systemic sclerosis does not seem a disease that would be accompanied by a specific enhancement of serum TGF-β1. Thus, this cytokine is rather unlikely to play an essential role in the development and course of the disease, nor can it be considered diagnostic or prognostic marker.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Systemic sclerosis is a connective tissue disease characterized by tissue fibrosis leading to multiple organ impairment. The disease most often affects the skin, subcutaneous tissue, and internal organs, especially the lungs, kidneys, gastrointestinal tract, and heart. The pathogenesis of the disease remains unclear, but disorders of the immune system leading to the production of autoantibodies against topoisomerase I (anti-Scl-70), against centromeres, and other factors are of significant importance. The occurrence of morphological changes and vascular dysfunction also play a role in the perpetuation of the disease. As a result of these processes, fibroblasts are activated, and excessive amounts of collagen are produced. Collagen accumulates and progressive fibrosis occurs, destructing tissue. One of the cytokines involved in systemic sclerosis is the transforming growth factor-β (TGF-β) and its isoform TGF-β1 that is related to the activity of connective tissue cells (Lafyatis 2014; Collier 2002; Klippel and Dieppe 1998). TGF-β has its receptors in virtually all eukaryotic human cells. It is believed that in systemic sclerosis, TGF-β stimulates fibroblasts to produce extracellular matrix components and inhibits enzymes that degrade them. An often reported organ complication of systemic sclerosis is fibrosis of lung tissue, known as interstitial lung disease, which may result in the development of secondary pulmonary hypertension (Piorunek et al. 2013). One piece of evidence of the TGF-β role in the pathogenesis of systemic sclerosis is the fact that in animal models of diseases with fibrosis, administration of antibodies against TGF-β prevents excessive production of connective tissue and consequent destruction of organs (Leask 2006; Verrecchia et al. 2006; Border and Noble 1994; Border and Ruoslahti 1992). Recently, TGF-β has been of interest as a diagnostic and prognostic marker and also as a drug target in systemic sclerosis and some other diseases (Wermuth and Jimenez 2018; Du et al. 2017; Jakubowska et al. 2015; Piotrowski et al. 2015). Therefore, the present study seeks to define the content of serum TGF-β in patients with systemic sclerosis and to assess its potential value in the early diagnosis of systemic sclerosis-related tissue fibrosis.
2 Methods
The study consisted of 30 patients (F/M; 25/5) of the mean age of 46.9 ± 12.8 years, with the diagnosis of systemic sclerosis based on the criteria of the American Rheumatism Association (Collier 2002). Duration of systemic sclerosis ranged from 1 to 20 years (mean 8.1 ± 5.3 years). The control group consisted of 19 women, aged from 20 to 48 (mean 28.4 ± 7.8) years whose diagnosis was the primary Raynaud disease.
The presence of interstitial lung disease was established by chest X-rays in the posterior-anterior projection and by high-resolution computed tomography. Pulmonary hypertension was diagnosed on the basis of clinical signs such as progressive dyspnea, fatigue, and chest pain resulting in limitation of patients’ exercise tolerance and on the estimated pulmonary artery pressure exceeding 35 mmHg in Doppler echocardiography (Collier 2002). The following score of organ changes was used in this study:
-
0 – no evidence of interstitial lung disease and pulmonary hypertension
-
1 – interstitial changes involving basal lung fields
-
2 – interstitial changes involving middle and upper lung fields
-
3 – interstitial changes involving middle and upper lung fields and pulmonary hypertension.
To evaluate the skin involvement in patients with systemic sclerosis, a modified Rodnan Skin Score (mRSS) was used. The hardening of skin areas was assessed on a 4-point scale: 0, normal; 1, slight hardening; 2, moderate hardening; and 3, significant skin hardening. This assessment involves both the degree of skin hardening and the extent of skin involvement. The total mRSS score ranges from 0 to 51 points (Denton and Black 2004; Akesson et al. 2003; Clements 2000).
The TGF-β1 content was evaluated with a commercial Quantikine human TGF-β1 kit (R&D Systems, Minneapolis, MN), based on the ELISA method. The test enables the quantitative assessment of activated TGF-β1. The minimum detectable concentration of TGF-β1 was in a range of 1.7–15.4 pg/mL. However, the manufacturer of the test kit does not specify the range of a normal serum level of the cytokine since it is not defined. Thus, TGF-β1 level found in this study was compared with that reported in previous studies performed in patients suffering from systemic sclerosis and in healthy persons.
Data were presented as means ±SD. Differences between the two groups were evaluated with a two-tailed t-test. A p-value <0.05 defined statistically significant differences. The evaluation was conducted using a commercial STATISTICA package (StatSoft; Tulsa, OK).
3 Results
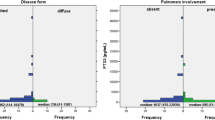
The mean serum TGF-β1 content in patients with systemic sclerosis was 598.7 ± 242.6 pg/mL, whereas in the control group, consisting of patients with primary Raynaud’s disease, it was 568.4 ± 322.2 pg/mL (p = 0.38) (Fig. 1). The maximum levels of 1250.0 pg/mL and 1310.0 pg/mL and minimum levels of 200.0 pg/mL and 270.0 pg/mL, respectively, were not significantly different either.

Serum TGF-β1 content is systemic sclerosis and control patients. Data are means ±SD
Skin hardening was observed in all of the systemic sclerosis patients, with the mean mRSS score of 9.7 ± 9.2 and the min-max range of 1–34 points. A lung involvement with characteristic interstitial fibrotic changes was noticed in 19 (63.4%) out of the 30 systemic sclerosis patients. This involvement was confined to basal lung segments in 12 (40.0%) and to the middle and upper lung fields in 5 (16.7%) patients. In 2 (6.7%), patients, the features of interstitial lung disease were accompanied by pulmonary hypertension.
A relation between the severity of skin involvement, evaluated by mRSS scale, and the serum TGF-β1 content in systemic sclerosis patients turned out insignificant (p = 0.476; r = 0.14). Likewise, TGF-β1 content failed to relate to the appearance of lung involvement in the patients (r = 0.32).
4 Discussion
The findings of this study failed to confirm the existence of any relationship between the serum TGF-β1 content and the appearance and severity of pulmonary and skin fibrosis in patients with systemic sclerosis. We confronted these findings with the previous literature data on the subject of TGF-β1 in systemic sclerosis. Scala et al. (2004) did not observe a significant difference in the content of total TGF-β1 between patients with a limited as well as generalized form of systemic sclerosis and control subjects, with the mean TGF-β1 of 3499 ± 2357 pg/mL, 3552 ± 2357 pg/mL, and 3542 ± 4410 pg/mL, respectively. Snowden et al. (1994) detected TGF-β1 in the plasma of 6 out of the 39 patients with systemic sclerosis, employing a test having the minimum detectable level of 100 pg/mL, i.e., being more than sixfold less sensitive for TGF-β1 detection than the test used in the current study. This level of detection was not reached in serum samples from any of the 60 healthy subjects and 9 patients with Raynaud’s disease, implying a tendency for a higher TGF-β1 content in some patients with systemic sclerosis. In contradistinction, Dziadzio et al. (2005) reported a reduced content of the active form of TGF-β1 in patients with scleroderma, in particular in the generalized disease, compared to the control subjects, with the median TGF-β of 520 pg/mL and 1,230 pg/mL, respectively. These authors, however, failed to notice any significant reduction in the total content of TGF-β1 in scleroderma. The opposite results were reported by Dantas et al. (2016) who show an increase in active TGF-β1 and its association with clinical manifestations of scleroderma. Therefore, the issue of the content and role of TGF-β1 in the course of systemic sclerosis is highly contentious, and the data are discrepant. The issue is further compounded by as yet undetermined normal level of serum TGF-β1 in the general population. In addition, discrepancy in TGF-β1 values may stem from the assessment of active versus total TGF-β1 or using different not standardized commercial kits. In the current study, the active form of TGF-β1 showed a tendency for elevation in systemic sclerosis patients, which seems somehow in line with the findings of Dziadzio et al. (2005). Scala et al. (2004), on the other side, who showed no changes in serum TGF-β1 in various types of scleroderma, investigated the total TGF-β1 content. The accuracy of TGF-β1 measurement may be highly affected by the fact that only a part of this protein, having a mass of 25 kDa, is in the active form that has a very short half-life in bodily fluids. Wakefield et al. (1990) reported the half-life of active TGF-β1 as short as 2–3 min, compared with more than a 100 min for the latent TGF-β1 form. The existence of this dual form of TGF-β1 introduces a nuisance in the understanding of TGF-β1 bioactivity, which can hardly be resolved at the current state of knowledge. In addition, in the pathogenesis of systemic sclerosis, not so much the serum content as the ratio of active to latent TGF-β1 form could be a key factor. Other theories raise the possibility of overexpression of type I fibroblast receptors (Leask 2006; Border and Noble 1994) or disruption of the intracellular transduction cascade of TGF-β1 by a defective Smad protein as the mechanisms by which TGF-β affects tissue fibrosis (Verrecchia et al. 2006).
Of note, the control group of the current study consisted of patients with primary Raynaud’s disease, which may enhance the predilection for or be a presage of systemic sclerosis (Cutolo et al. 2017). Nonetheless, we found no appreciable difference in the serum content of active TGF-β1 between patients with systemic sclerosis and Raynaud’s disease, which strengthens the impression that this form of TGF-β1 may not be at play in shaping detrimental molecular and cellular changes underlying fibrosis in systemic sclerosis. To this end, our findings are in line with those of Snowden et al. (1994) who investigated the serum content of TGF-β1 in nine patients with Raynaud’s disease, who were part of the control group, and found the undetectable level of it. In addition, we also failed to demonstrate any association between the serum content of TGF-β1 and fibrotic changes in the skin or the lungs, which is generally in line with data from previous studies (Dziadzio et al. 2005; Snowden et al. 1994). In conclusion, we believe that despite a biological plausibility of the stimulating role of TGF-β1 in the development of skin and other tissues’ fibrotic changes in the course of systemic sclerosis, we found in this study no supportive evidence for such an action. A lack of changes in serum TGF-β1 also makes it unlikely that this cytokine could be considered a diagnostic marker or a marker of severity of skin or lungs involvement in systemic sclerosis. A multifarious and complex bioactivity of TGF-β1 remains contentious and is open to continuing exploration in other study designs.
References
Akesson A, Fiori G, Krieg T, van den Hoogen FHJ, Seibold JR (2003) Assessment of skin, joint, tendon and muscle involvement. Clin Exp Rheumatol 21:S5–S8
Border WA, Noble NA (1994) Transforming growth factor beta in tissue fibrosis. N Engl J Med 331:1286–1292
Border WA, Ruoslahti E (1992) Transforming growth factor-beta in disease: the dark side of tissue repair. J Clin Invest 90:1–7
Clements PJ (2000) Systemic sclerosis (scleroderma) and related disorders: clinical aspects. Baillieres Best Pract Res Clin Rheumatol 14:1–16
Collier D (2002) Systemic sclerosis. In: West S (ed) Rheumatology secrets, 2nd edn. Hanley & Belfus, Philadelphia
Cutolo M, Smith V, Furst DE, Khanna D, Herrick AL (2017) Points to consider-Raynaud’s phenomenon in systemic sclerosis. Rheumatology (Oxford) 56(Suppl 5):v45–v48
Dantas AT, Gonçalves SM, de Almeida AR, Gonçalves RS, Sampaio MC, Vilar KM, Pereira MC, Rêgo MJ, Pitta ID, Marques CD, Duarte AL, Pitta MG (2016) Reassessing the role of the active TGF-β1 as a biomarker in systemic sclerosis: association of serum levels with clinical manifestations. Dis Markers 2016:6064830
Denton CP, Black CM (2004) Scleroderma – clinical and pathological advances. Best Pract Res Clin Rheumatol 18:271–290
Du J, Yu Y, Zhan J, Zhang H (2017) Targeted therapies against growth factor signaling in breast cancer. Adv Exp Med Biol 1026:125–146
Dziadzio M, Smith RE, Abraham DJ, Black CM, Denton CP (2005) Circulating levels of active transforming growth factor beta1 are reduced in diffuse cutaneous systemic sclerosis and correlate inversely with the modified Rodnan skin score. Rheumatology (Oxford) 44:1518–1524
Jakubowska K, Naumnik W, Niklińska W, Chyczewska E (2015) Clinical significance of HMGB-1 and TGF-β level in serum and BALF of advanced non-small cell lung cancer. Adv Exp Med Biol 852:49–58
Klippel JH, Dieppe PA (1998) Rheumatology, 2nd edn. Mosby, London
Lafyatis R (2014) Transforming growth factor β – at the centre of systemic sclerosis. Nat Rev Rheumatol 10:706–719
Leask A (2006) Scar wars: is TGFbeta the phantom menace in scleroderma? Arthritis Res Ther 8:213–219
Piorunek T, Kuznar-Kaminska B, Cofta S, Batura-Gabryel H, Poplawski D, Majewski D, Puszczewicz M, Wysocka E (2013) Lung impairment in scleroderma. Adv Exp Med Biol 755:149–154
Piotrowski WJ, Kiszałkiewicz J, Pastuszak-Lewandoska D, Antczak A, Górski P, Migdalska-Sęk M, Górski W, Czarnecka K, Nawrot E, Domańska D, Brzeziańska-Lasota E (2015) TGF-β and Smads mRNA expression in pulmonary sarcoidosis. Adv Exp Med Biol 852:59–69
Scala E, Pallotta S, Frezzolini A, Abeni D, Barbieri C, Sampogna F, De Pità O, Puddu P, Paganelli R, Russo G (2004) Cytokine and chemokine levels in systemic sclerosis: relationship with cutaneous and internal organ involvement. Clin Exp Immunol 138:540–546
Snowden N, Coupes B, Herrick A, Illingworth K, Jayson MI, Brenchley PE (1994) Plasma TGF beta in systemic sclerosis: a cross-sectional study. Ann Rheum Dis 53:763–767
Verrecchia F, Mauviel A, Farge D (2006) Transforming growth factor-beta signaling through the Smad proteins: role in systemic sclerosis. Autoimmun Rev 5:563–569
Wakefield LM, Winokur TS, Hollands RS, Christopherson K, Levinson AD, Sporn MB (1990) Recombinant latent transforming growth factor beta 1 has a longer plasma half-life in rats than active transforming growth factor beta 1, and a different tissue distribution. J Clin Invest 86:1976–1984
Wermuth PJ, Jimenez SA (2018) Abrogation of transforming growth factor-β-induced tissue fibrosis in TBRIcaCol1a2Cre transgenic mice by the second generation tyrosine kinase inhibitor SKI-606 (Bosutinib). PLoS One 13:e0196559
Conflicts of Interest
The authors declare no conflicts of interest in relation to this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Bioethics Committee of the Karol Marcinkowski University of Medical Sciences in Poznań, Poland.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Majewski, D. et al. (2019). Systemic Sclerosis and Serum Content of Transforming Growth Factor. In: Pokorski, M. (eds) Medical Science and Research. Advances in Experimental Medicine and Biology(), vol 1153. Springer, Cham. https://doi.org/10.1007/5584_2019_341
Download citation
DOI: https://doi.org/10.1007/5584_2019_341
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-19058-3
Online ISBN: 978-3-030-19059-0
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)