
Abstract
Epidemiological studies show that long-term exposure to air pollution may increase the relative risk of obstructive lung diseases such as COPD or asthma. The risk of increased obstruction is higher among residents living in close proximity to high traffic routes where there are high concentrations of PM10. The present study consists of two parts: the measurement of the concentration of air pollutants and of pulmonary function in selected groups of people. The study was conducted in Warsaw, Poland, in seven localizations with typical urban canyon characteristics and roads with high traffic. The control group consisted of people living in other regions of Poland with a significantly lower (p < 0.05) concentration of air pollutants. The study was performed in the years 2008–2012. The incidence of obstructive lung disease was determined according to the GOLD guidelines. The study subjects were all non-smokers. The relative risk of disease took into account different exposure times to air pollutants. The findings indicate that an increase in PM10 concentration by each 10 μg/m3 caused an increase in the relative risk of lung obstruction by a factor of 1.27, 1.24, and 1.19 for the residence period in the vicinity to heavy traffic city roads for 20, 30, and 40 years, respectively as compared with the residence of rural unpolluted areas. A decrease in the number of people with lung obstruction with the length of residence actually indicates that people exposed to high concentrations of PM10 become affected by lung obstruction at a lower age. The study shows a positive relative risk of lung obstruction due to an exposure to high PM10 emission.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The air pollution contributes to 8 million deaths annually, which constitutes 15 % of deaths of all causes over the world. Exposure to ambient air pollution causes an increase in morbidity and mortality of a variety of diseases, including respiratory diseases such as asthma or COPD, cardiovascular diseases (Arena et al. 2006; Wong et al. 2002; Pope et al. 2004). According to Global Burden of Disease Study (Murray et al. 2012), chronic obstructive pulmonary disease (COPD), is the third most common cause of death worldwide, and comes in nine place in a rating based on the disability life adjusted years (DALY) indicator. Asthma is not as serious as COPD, taking into account the number of deaths and lost DALY years, and is not listed in the first 30 disorders in the GBDS ranking (Lozano et al. 2012; Murray et al. 2012). COPD and asthma are characterized by a decrease in airway flow, which is usually assessed by respiratory function tests. The severity and progression of COPD is determined by forced expiratory flow in 1 s (FEV1), expressed as a percentage of predicted value (Vestbo et al. 2013).
COPD reduces a person’s quality of life and imposes a substantial economic burden on society due to decreased productivity, absenteeism, and health care costs. It is estimated that the 2008 indirect costs of COPD and asthma-related premature mortality were as high as 18 billion USD in the US (National Heart, Lung, and Blood Institute 2012). In the EU, as much as 6 % of the healthcare budget is dedicated to treatment of respiratory disorders, out of which 56 %, i.e., 36.8 billion EUR are COPD-related costs (Rabe et al. 2007).
Although the most significant risk factor of COPD and asthma is tobacco smoking, the disease affects non-smokers as well (Kohansal et al. 2009). It is estimated that non-smokers constitute 25–45 % of all COPD cases (Salvi and Barnes 2009). Therefore, it is important that the epidemiological studies on the influence on human health of air suspended particles took into account a non-smoking population as well.
The short-term studies on the influence on the human health of the air PM10 concentration have clearly shown an increase in hospital admissions related to asthma or COPD, including increased mortality caused by these diseases (Peacock et al. 2011; Schwartz 1996). The long-term studies, albeit less often conducted, also show an increased incidence and intensification of COPD symptoms in persons exposed to increased PM10 concentration (Gan et al. 2013; Andersen et al. 2011). One of the methods for the relative risk assessment of the incidence of lung obstruction in a population is to study a correlation between increased concentration of pollutants and decreased respiratory indices. For instance, a study on air pollution and lung diseases in adults (SAPALDIA) showed a fall in FEV1 of 1.6 %, and FVC of 3.4 % when PM10 increased by 10 μg/m3 in relation to the concentration of this particular pollutant in the area inhabited by a control group (Ackermann-Liebrich et al. 1997). Likewise, a study on air pollution on lung function, inflammation and aging (SALIA) showed a fall in FEV1 of 4.7 %, in FVC of 3.4 %, and in FEV1/FVC of 1.1 % during the same increase in air pollutants (Schikowski et al. 2005). Prospective cohort studies show that a decrease, on average, in spirometric indices is less significant in persons living in less polluted areas compared with those exposed to high concentrations of sulfates, nitrogen oxides, and hydrocarbons (Tashkin et al. 1994).
The objective of the present study was to examine the relative risk of lung obstruction in people older than 40 years living close to urban roads with intense traffic. To this end, we compared pulmonary function in a group of persons exposed long-term to statistically greater concentrations of air pollutants, such as CO, NO2, or PM10 (p < 0.05), with that in a control group consisting of persons living in rural areas.
2 Methods
The study was approved by an institutional Research Review Board. It consists of two parts: the measurements of air traffic-related pollutant concentration and of pulmonary function. The measurements were done in the city of Warsaw, Poland, in seven predefined locations in 2008–2012. The road sections, selected for the study were typical urban canyons characterized by severe traffic intensity and congestion. A limited dispersion of air pollution, compared with other road fragments, resulted in a similar level of air pollution in the total section investigated. Nevertheless, there is a building storey-dependent difference in the concentration of air pollutants due to a vertical gas and particulate dispersion in urban canyons.
The air pollution measurements were taken in series, choosing months in which the dominant contributing factor was heavy road traffic (June and October) and which are not considered as a holiday or heating season. An AirpointerTM mobile monitoring station for the measurement of air pollution concentration was used (MLU, Wiener Neudorf, Austria). The measurements were conducted for 24 h, 7 days a week. The measuring equipment was localized about 1 m from the edge of the street. The device registered the following concentrations: carbon monoxide, nitrous oxides, volatile organic compounds, and the PM10 suspended particle. The concentration of PM10 was measured using a nephelometric method, which is based on the measurement of light dispersion in relation to the concentration of solid particles with a diameter of >10 μm. The urban sections selected were characterized by high traffic congestion; from 30,000 to 70,000 vehicles per day. In addition to seven sections in Warsaw, measurements also were done in two control points localized in the cleanest, from the standpoint of air pollution, areas of Eastern Poland. The control points were at least 250 m away from roads, and the traffic congestion was of one order of magnitude lower than that in Warsaw.
Respiratory function was studied from April to June and from September to October. The choice of the study period excluded the winter heating periods that cause a passing increase in air pollution, which could affect the functional results. The other reason was to avoid a holiday season, during which the sample would not be representative. Pulmonary function was assessed with an EasyOne spirometer (ndd Medizintechnik AG, Zürich, Switzerland). This device is compatible with the international standards of the European Respiratory Society (ERS). The following parameters were measured: functional vital capacity (FVC), forced expired volume in 1 s (FEV1), FEV1/FVC, peak expired flow (PEF), and forced expiratory flow at 50 % (FEF50). The measurement was followed by a questionnaire that provided information on age, place, and duration of residence, tobacco smoking habits, and respiratory symptoms. The period of residence at a location was stratified into 20, 30, and 40 years to assess the variability in the occurrence of lung obstruction caused by prolonged environmental exposure to pollutants.
Smoking persons and those aged below 40 were excluded from further study procedures. The effect on the incidence of lung obstruction of increased PM10 alone could be estimated. The exclusion of younger than 40 years persons was due to the above mentioned prolonged exposure paradigm used. The GOLD guidelines (2011) for the interpretation of pulmonary function were used to determine the incidence of obstructive disease. Lung obstruction was diagnosed when the FEV1/FVC ratio was less than 0.7. Post-bronchodilator tests or reversibility of bronchoconstriction were not assessed. Therefore, no distinction between asthma and COPD could be done and the results pertain to general lung obstruction.
The results of measurements of PM10 concentrations were used to determine average exposure of people to particulate matter, both in urban conditions and the control area. The study was not conducted throughout the entire year; thus, the average annual PM10 concentration could not be calculated. Nevertheless, substantial differences in the concentration of pollutants between testing sites was observed. Taking that into account, a general exposure level of PM10 for certain groups of habitants could be determined, although an accurate estimation of a difference between the study results and the actual mean annual concentration was not possible. Despite this limitation, it is important to underscore that the measurement of air pollution in close proximity to roads seems more accurate than the actual data provided by the National Environmental Monitoring, which has monitoring stations in distant locations from the sites chosen for this study. Furthermore, the accuracy of the present data was verified by the determination of confidence intervals for exposure-response functions.
Taking into account the GOLD guidelines (2011) and the three defined periods of residence, it was possible to determine the relative risk (RR) of the incidence of lung obstruction in the groups studied. As a result, three patterns of exposure-response functions were obtained. The first step in RR calculation was to determine the incidence number within each group, and to estimate the probability of the occurrence of lung obstruction. By relating these results to the control group, it was possible to define particular RR for each of the seven measurement sites. Because different groups were exposed to different PM10 concentrations, the results were normalized for inter-group comparisons by matching the RR of lung obstruction with the concentration increase of PM10 by 10 μg/m3. The final step was to determine the confidence intervals and mean concentration results.
3 Results
Daily fluctuations in PM10 concentration were observed in the city road traffic sections studied, particularly present when PM10 increased during rush hours. Nevertheless, the mean concentrations of PM10 in all seven stations was an order of magnitude greater than its level at the two control points; highly distinct differences (p < 0.05) (Table 1). Pearson’s linear correlation between PM10 concentration and traffic congestion was calculated. The correlation coefficients were significant (p < 0.05), varying from 0.53 to 0.72, showing that traffic congestion had a strong impact on the increase in PM10.
A total of 4,985 persons (3,997 living in urban areas and 988 control subjects from non-urban areas) were subjected to respiratory function tests followed by questionnaires. A number of persons had to be discarded from final analysis due to insufficient technical quality of test results (short forced expiration, improper placement of the mouthpiece, and improper position of the tongue during the test), unambiguous interpretation of results, or lack of proper cooperation of the persons studied. Tobacco smokers were excluded as well, to avoid a possible bias in determining the influence of air pollution on respiratory function. Additionally, persons aged below 40 were also excluded from further analysis, since the incidence of lung obstruction in this age category is low. After the exclusions, there remained 2,378 persons living in urban areas in the vicinity to busy traffic roads and 762 control persons from outside such areas, whose results qualified for further analysis. These study persons were stratified into three groups depending on the period of residence at either location: 20, 30, and 40 years. The respective groups encompassed 1,031, 797, and 550 persons from polluted areas and 296, 249, finally 208 persons from control areas. Detailed results in regard to each of the seven city road traffic sections and two control points (C) are presented in Table 2.
A number of residents at a given location were decreasing with the extension of the period of living at a given location, which may have affected the accuracy of the estimation of the relative risk of lung obstruction. Also, the control group was, on average, junior to persons living in the areas of heavy exposure to pollution. In general, the incidence of lung obstruction decreased as the period of residence increased, with the exception of the control group. However, as the population number decreased with longer living at a location as above mentioned, the probability of lung obstruction actually increased in both studied and control groups. The study also suggests that in the control groups, not exposed to high concentrations of air pollution, the risk of lung obstruction is less related to the residence period, but the influence of person’s age assumes a bearing. It means that the probability of lung obstruction in these groups depends on the correlation between the person’s increasing age and the length of residence to a greater degree than in the other groups studied.
Finally, we determined the relative risk (RR) of lung obstruction in response to increased PM10 concentration. The probability of the occurrence of lung obstruction in each group was determined and related to the control group by the following formula:
Where:
-
RR i is the relative risk of lung obstruction in i group at i concentration of PM 10 ;
-
p i is the probability of lung obstruction in i group at i concentration of PM 10 ;
-
p 0 is the probability of lung obstruction in the control group.
Since each group studied was exposed to a different PM10 concentration, the results were recalculated to normalize the relative risk of lung obstruction to an increase in PM10 by 10 μg/m3. The risk of lung obstruction for each residence period is presented in Table 3 and the statistical elaboration of these data is displayed in Fig. 1.

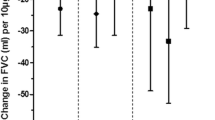
Median and spread of the relative risk of lung obstruction in response to an increase in PM10 by 10 μg/m3
The results of the relative risk of lung obstruction in response to an increase in PM10 by each 10 μg/m3 demonstrate a wide spread of values around the median, where the maximum risk is 1.45 and the minimum is 1.00, and rather an opposite to the expected trend for reduced risk as the residence period increases. There is a small difference in the number of people with lung obstruction in the control groups. However, when the number of people decreases, the probability of lung obstruction increases. In case of the urban groups, the number of people with lung obstruction decreases, as the length of residence increases. That means that people exposed to high concentrations of PM10 become affected by lung obstruction at a much lower age than those living in the areas of low PM10 concentration. That spurious decrease in the incidence of lung obstruction in urban citizens, along with little changes in the control groups, caused an overall decrease in the relative risk. Nonetheless, the results demonstrate a positive relative risk of lung obstruction due to an exposure to PM10. The substantial spread of the relative risk underscores that different diagnostic recommendations might affect the final results.
4 Discussion
A long-term exposure to air pollution caused by high concentrations of PM10 in close proximity to roads characterized by high traffic volume and traffic congestion may increase the risk of COPD. It also has a negative effect on lung function (Schikowski et al. 2005). The present study demonstrates that there is a relationship between a long-term concentration of air pollutants, with the PM10 level taken as a surrogate, and the incidence of lung obstruction, which is demonstrated by the calculated values of the relative risk factor.
In the presented study, as opposed to other studies, the relative risk was related to lung obstruction, instead of mortality. That seems of importance in view of the ambiguity of results from studies analyzing the interconnection between risk and mortality from respiratory and other diseases related to particles suspended in the air (Pope et al. 2004). The problem may lie in the complex and not fully understood pathophysiological pathways connecting the exposure to suspended particles to mortality from cardiopulmonary disorders. The present study also is based on actual data tallied in a big bustling city with a high emission of PM10 and contrasting rural areas, rather than on purely statistical data.
Generally, the relative risk varies depending on the characteristics of groups studied, the type of contamination, and the time of exposure. There is, however, one common feature of different analyses of the matter. The results always confirm, although to a different degree, that air pollution, especially one caused by suspended particles, have a significant impact on the increase of lung obstruction and related mortality. A case in point is the Schikowski et al. (2005) study, which is similar in assumptions to the present article, but describes a specific type of lung obstructive disease – COPD. That study shows that a decrease in respiratory capacity and an increase in COPD incidence are caused by exposure to PM10 and other pollutants characteristic of road traffic. A decrease in FEV1 by 5.1 % (95 % CI 2.5–7.7) has been related to an increase in the mean PM10 (interquartile range) by 7 μg/m3 within 5 years. A corresponding decrease in FVC was 3.7 % (95 % CI 1.8–5.5) and the odds ratio for COPD was 1.33 (95 % CI 1.03–1.72). In a different study, concerning the short-term exposure to pollution stemming from suspended particles, it has been demonstrated that an increase in the 24-h concentration of PM2.5 by 10 μg/m3 increases the relative risk of daily mortality from heart disease by 0.4 to 1.0 % (Brook et al. 2010). That study revealed that it is worthwhile to look at the absolute risk, which may be a more effective way of presenting the information about health hazards, particularly that statistically calculated relative risk is not evenly spread within the population. The relative risk is, however, greater for persons who live in areas of higher concentrations of PM2.5 for long time than for those affected in the short-term; 1.76 and 1.06, respectively, for a change of 10 μg/m3 (Dockery 2006; Brook et al. 2010). Short-term increases in PM2.5 should not be neglected, because they might lead to tens of thousands of deaths in the US alone. Nonetheless, studies on the adverse health effects of daily exposure to increased concentrations of suspended particles do not seem to provide sufficient information on the reduction in life expectancy, the influence of air pollution on long-term mortality, or the role of pollutants in the occurrence and progression of chronic diseases (McMichael et al. 1998).
5 Conclusions
The present study confirms the impact of increased PM10 concentration by each 10 μg/m3 on the risk of lung obstruction. The study covered a population sample older than 40 years, in which the risk of obstructive lung diseases is higher than that of asthma. We took into account only non-smoking persons, unaffected by this key factor of lung obstruction. The calculated relative risk of lung obstruction amounted to 1.27, 1.24, and 1.19 for persons living in urban areas exposed to an average increase in PM10 emission of 10 μg/m3 for 20, 30, and 40 years, respectively. A tendency for a decrease in the risk of obstruction was revealed, opposing the expectancy, which seems spurious as it indicates that in fact lung obstruction develops faster in the groups living shorter in the polluted air. That spurious decrease in the incidence of lung obstruction in urban citizens, along with little changes in the control groups, caused an overall decrease in the relative risk. The study shows a positive relative risk of lung obstruction due to an exposure to high PM10 emission.
References
Ackermann-Liebrich U, Leuenberger P, Schwartz J, Schindler C, Monn C, Bolognini G, Bongard JP, Brändli O, Domenighetti G, Elsasser S, Grize L, Karrer W, Keller R, Keller-Wossidlo H, Künzli N, Martin BW, Medici TC, Perruchoud AP, Schöni MH, Tschopp JM, Villiger B, Wüthrich B, Zellweger JP, Zemp E (1997) Lung function and long term exposure to air pollutants in Switzerland. Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) Team. Am J Respir Crit Care Med 155:122–129
Andersen Z, Hvidberg M, Jensen S, Ketzel M, Loft S, Sørensen M, Tjønneland A, Overvad K, Raaschou-Nielsen O (2011) Chronic obstructive pulmonary disease and long-term exposure to traffic-related air pollution. Am J Respir Crit Care Med 183:455–461
Arena VC, Mazumdar S, Zborowski JV, Talbott EO, He S, Chuang YH, Schwerha JJ (2006) A retrospective investigation of PM10 in ambient air and cardiopulmonary hospital admissions in Allegheny County, Pennsylvania: 1995–2000. J Occup Environ Med 48:38–47
Brook RD, Rajagopalan S, Pope CA III, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong Y, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC Jr, Whitsel L, Kaufman JD (2010) Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation 121:2331–2378
Dockery DW (2006) Health effects of particulate air pollution. Ann Epidemiol 19:257–742
Gan W, FitzGerald M, Carlsten C, Sadatsafavi M, Brauer M (2013) Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am J Respir Crit Care Med 187:721–727
GOLD – Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. (Revised 2011). Available from: https://www.goldcopd.org. Accessed on 21 Nov 2014
Kohansal R, Martinez-Camblor P, Agusti A, Buist AS, Mannino DM, Soriano JB (2009) The natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohort. Am J Respir Crit Care Med 180:3–10
Lozano R, Naghavi M, Foreman K, Kim S, Shibuya K, Aboyans V, Abraham J et al (2012) Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2095–2128
McMichael AJ, Anderson HR, Brunekreef B, Cohen AJ (1998) Inappropriate use of daily mortality analyses to estimate longer-term mortality effects of air pollution. Int J Epidemiol 27:450–453
Murray CJ, Vos T, Lozano R, Naqhavi M, Flaxman AD, Michaud C, Ezzati M et al (2012) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2197–2223
National Heart, Lung, and Blood Institute (2012) Morbidity and mortality: chart book on cardiovascular, lung and blood diseases. National Institutes of Health, Bethesda. https://www.nhlbi.nih.gov/files/docs/research/2012_ChartBook_508.pdf. Accessed on 21 Nov 2014
Peacock JL, Anderson HR, Bremner SA, Marston L, Seemungal TA, Strachan DP, Wedzicha JA (2011) Outdoor air pollution and respiratory health in patients with COPD. Thorax 66:591–596
Pope CA 3rd, Burnett RT, Thurston GD et al (2004) Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation 109:71–77
Rabe KF, Hurd S, Anzueto A et al (2007) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 176:532–555
Salvi SS, Barnes PJ (2009) Chronic obstructive pulmonary disease in nonsmokers. Lancet 374:733–743
Schikowski T, Sugiri D, Ranft U, Gehring U, Heinrich J, Wichmann HE, Krämer U (2005) Long-term air pollution exposure and living close to busy roads are associated with COPD in women. Respir Res 6:152
Schwartz J (1996) Air pollution and hospital admissions for respiratory disease. Epidemiology 7:20–28
Tashkin DP, Detels R, Simmons M, Liu H, Coulson AH, Sayre J, Rokaw S (1994) The UCLA population studies of chronic obstructive respiratory disease: XI. 6. Impact of air pollution and smoking on annual change in forced expiratory volume in one second. Am J Respir Crit Care Med 149:1209–1217
Vestbo J, Hurd SS, Agustí AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, Stockley RA, Sin DD, Rodriguez-Roisin R (2013) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 187:347–365
Wong TW, Tam WS, Yu TS, Wong AH (2002) Associations between daily mortalities from respiratory and cardiovascular diseases and air pollution in Hong Kong, China. Occup Environ Med 59:30–35
Acknowledgements
The study was financed as a research project from the Polish budget funds for science for the years 2008–2012.
Conflicts of Interest
The authors declare no conflicts of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Adamkiewicz, Ł., Gayer, A., Mucha, D., Badyda, A.J., Dąbrowiecki, P., Grabski, P. (2014). Relative Risk of Lung Obstruction in Relation to PM10 Concentration as assessed by Pulmonary Function Tests. In: Pokorski, M. (eds) Environmental Biomedicine. Advances in Experimental Medicine and Biology(), vol 849. Springer, Cham. https://doi.org/10.1007/5584_2014_103
Download citation
DOI: https://doi.org/10.1007/5584_2014_103
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-14689-8
Online ISBN: 978-3-319-14690-4
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)