
Abstract
Lower limb injuries are extremely common in sports, particularly contact sports. The injuries can be divided into acute and chronic causes. It is important for the radiologist to be aware of all the possible causes of both acute and chronic symptoms within the lower leg and also any subsequent complications so that the correct imaging modalities can be selected and the possible range of pathologies considered. This chapter discusses the biomechanics of lower limb injury as well as the most common acute and chronic causes seen in sports and also any potential complications and their characteristic imaging findings. The most appropriate imaging modalities for each of the conditions are also described.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
The lower limb is subject to marked biomechanical stresses during the majority of athletic activity (Dvorak and Junge 2000). This region is the most frequently injured area in a number of sports with audits in professional football demonstrating 87% of all injuries occurring here, in particular the thigh (23%), ankle (14%), knee (18%), leg (11%) and groin (14%). Among acute lower extremity injuries, ankle sprain occurred in 7% and thigh strain in 17% (Ekstrand et al. 2011).
This chapter discusses the biomechanics of lower limb injuries and also the role of imaging in their management, highlighting specific acute and chronic osseous, muscle and tendon injuries commonly encountered in athletes. Injuries relating to the pelvis, knee, ankle and foot will not be discussed in detail as these areas are covered in their specific chapters.
2 Acute Osseous Injury
Biomechanically the cortex provides the majority of a bone’s strength for force absorption (Nordin and Frankel 2001a). The trabecular bone and marrow contribute relatively little to the overall strength but do determine the bone’s cross-sectional area influencing the distribution of applied forces, important for resisting chronic stress and explaining the subsequent distribution of injuries particularly seen in the tibia.
Acute trauma in the context of sporting injuries frequently results in soft-tissue injury; however, in contact sports acute fractures may also occur on tackling or player collision (Hawkins et al. 2001; Fuller et al. 2004; Chomiak et al. 2000). In the context of sports injuries, acute fractures of the femur and hip are rare but injuries of the tibia, fibula, ankle and foot are more frequent.
In contrast to chronic osseous injuries where concomitant injuries and local muscle imbalance are important for injury development, in acute injury the forces applied are usually sudden and excessive leading to acute structural failure (fracture) not dependent on concomitant injuries (Nordin and Frankel 2001a). The rate of force application is also important, as forces applied at a high rate induce increased bone stiffness resulting in shattering if the bone strength limit is exceeded. As bone fails, the energy producing the fracture is dissipated into the soft tissues resulting in significant associated injury due to the high energies involved (Nordin and Frankel 2001a).
The forces applied to the tibia and fibula can be direct, torsional or bending which influence the subsequent fracture configuration. The majority of fractures of the tibia and fibula usually have an oblique orientation in the mid to distal shaft resulting from the lateral or medial oblique forces produced from a direct blow during a fall, from tackling or from falling players (Figs. 1, 2, 3, and 4) (Giza et al. 2003; Fuller et al. 2004). This particular fracture pattern involving a direct blow and low velocity is sometimes termed ‘footballer’s fracture’ (Boden et al. 1999; Chang et al. 2007).

(a, b) Footballer with acute severe leg pain after a tackle. (a) Anteroposterior (AP) and (b) lateral radiographs, both showing a comminuted oblique displaced fracture through the diaphysis of the tibia and an oblique fracture of the distal fibula. The player went on to have plate fixation of the fractures

(a) AP radiograph of a tibial fracture and a proximal fibular fracture in a professional footballer treated with intramedullary nail. There is persistent non-union across the fracture site. (b) The intramedullary nail had to be removed and a circular frame was applied due to non-union secondary to infection. Antibiotic beads were implanted providing a method for antibiotic delivery

(a–c) Professional footballer with severe lower leg pain after stamping; radiographs showed some cortical irregularity. (a) Coronal T1-weighted and (b) T2-weighted fat-suppressed MR images show depression of the distal medial tibial cortex (arrows) with associated bone marrow oedema. (c) Corresponding axial T1-weighted MR image shows the main cortex (arrows) with periosteal haematoma and elevation (arrowheads). Note the defect in the elevated periosteum with haematoma (*)

(a–c) Footballer with lateral leg pain following a tackle. (a) Plain-film radiograph—lateral view of the right fibula fracture. (b) Coronal T1-weighted MR image showing a cortical defect in the mid-shaft of the fibula (arrow). (c) Axial T2-weighted fat-suppressed MR image showing muscle contusion and a fibular fracture with associated bone marrow oedema
2.1 Imaging Strategy and Management
For fractures of the tibia and fibula radiographs are usually sufficient to confirm the diagnosis and fracture configuration (Figs. 1 and 2). CT and MR imaging can be used to confirm fractures when radiographs are negative and an undisplaced fracture rather than just soft-tissue contusion is suspected (Figs. 3 and 4) (Jarraya et al. 2013).
CT is the method of choice in detecting osteopenia, one of the earliest imaging findings in fatigue cortical bone injury (Gaeta et al. 2005). Moreover, CT utilising dual energy via the virtual non-calcium-subtraction technique can be used for the detection of bone marrow oedema after trauma, especially in cases when MR imaging is contraindicated (Nicolaou et al. 2012).
MR imaging demonstrates soft-tissue oedema in the area of impact but also allows evaluation of the cortical and trabecular bone for oedema and low-signal fracture lines. Cortical abnormalities include buckling or increased thickness with high T2-weighted signal due to periosteal haematoma (Fig. 3).
Treatment for tibia and fibula fractures is often conservative with casting, but if the injury is of high velocity resulting in bone comminution and soft-tissue disruption, internal fixation and soft-tissue reconstruction will be required. In these cases, CT examination can be useful to define the exact fracture configuration and extent for surgical treatment. Despite the soft-tissue damage subsequent reconstruction (primary or grafting) does not require MR or ultrasound imaging unless there are specific vascular complications.
The recovery time for these injuries will depend on the fracture position and severity of associated injuries. While the majority of patients sustaining a lower limb fracture will return to their sport, fracture of the tibia and fibula can be career ending for athletes involved in contact sports (Chomiak et al. 2000). One series on 357 soccer players presenting with fractures reported that 83% of players made a full return to sport taking a mean of 15 ± 17 weeks with fractures of the distal tibial diaphysis having the highest rate of morbidity and non-return to soccer (Robertson and Wood 2017). Non-union is the most significant complication and if appearances are indeterminate on radiographs ultrasound or CT can be used to give a more accurate assessment of callus formation. If non-union is confirmed internal fixation and bone grafting may be required, which is not without complication (Fig. 2).
3 Chronic Exertional Leg Pain
The commonest causes of chronic exertional athletic lower extremity pain include medial tibial stress syndrome, stress fractures, chronic exertional compartment syndrome and popliteal artery and nerve entrapment (Gaeta et al. 2008). Several series have found slightly different incidences for each type of injury but together these processes most frequently occurr in athletes (Kaufman et al. 2000; Edwards Jr. et al. 2005; Bonasia et al. 2015).
3.1 Chronic Osseous Stress Response and Injury
Overuse injuries occur when the ability of cortical bone to remodel and compensate is exceeded by chronic excessive forces not individually reaching acute overload (Nordin and Frankel 2001a; Anderson et al. 1997). Causes of increased stress normally relate to a sustained increase in training and more commonly present in athletes who are female, have suffered prior osseous injury and have concomitant lower limb injuries (e.g., muscle strain) and especially in the lower leg, if there is ankle pronation (Anderson et al. 1997; Batt et al. 1998; Fredericson et al. 1995; Gaeta et al. 2008). Causes of increased stress include low bone mineral density, hormone imbalance, low-fat diet, high-mileage running, leg length discrepancy, high longitudinal arch of the foot and excessive forefoot varus (Bonasia et al. 2015).
Studies of military recruits have shown that stress injuries and fractures most commonly affect the calcaneus and metatarsals (Jarraya et al. 2013). In the femur stress reactions most frequently occur in the femoral neck and are important to detect early as the consequences for osteonecrosis or complete fracture are serious (Robertson and Wood 2017).
3.1.1 Tibia and Fibula
In the tibia the fracture position can vary according to sporting activity, with runners experiencing middle to distal third, dancers middle third and jumping athletes (e.g., tennis, basketball and volleyball) proximal third injuries (Batt et al. 1998). The mid and distal diaphysis of the tibia is thought to be the most vulnerable region as this is the narrowest cross-sectional area of the bone and has relatively little surrounding musculature to dissipate applied forces. In the tibia, compressive forces concentrate medially and fractures can present here or be part of medial tibial stress syndrome (MTSS, see below) (Gaeta et al. 2008). Fractures that develop on the anterolateral tibia occur as a result of tensile forces and subsequently have a higher risk of non-union, especially if the orientation is longitudinal and not perpendicular to the cortex (Fredericson et al. 1995; Edwards Jr. et al. 2005; Green et al. 1985). Fibular stress fractures are much less frequent and usually occur at the distal shaft, 5–6 cm proximal to the lateral malleolus (Bonasia et al. 2015).
Symptoms are usually of insidious onset, occurring on exertion, and are a differential diagnosis for chronic exercise-induced pain. However, if allowed to progress pain can be present at rest or on weight bearing (Fredericson et al. 1995; Edwards Jr. et al. 2005). In contrast, in chronic exertional compartment syndrome pain subsides after cessation of exercise (Ringler et al. 2013).
Clinical findings include localised tenderness and indirect pain produced by tibial percussion at a distant site (Batt et al. 1998; Yates and White 2004; Bonasia et al. 2015). This latter finding is thought to correlate well with more severe clinical and imaging extent (Fredericson et al. 1995).
3.2 Medial Tibial Stress Syndrome (MTSS)
This is an overuse syndrome in running and jumping athletes which is defined as involving the posteromedial tibial periosteum (Batt et al. 1998; Yates and White 2004). There has been previous controversy concerning the aetiology of this condition with initial theories suggesting a chronic periosteal traction injury from adjacent muscles (Anderson et al. 1997; Batt et al. 1998; Fredericson et al. 1995; Yates and White 2004). However, the osseous changes are usually distal to the main muscle origins and it is now thought to be the beginning of the spectrum of osseous stress reaction of the tibia (Figs. 5 and 6). This condition is interchangeable with posterior ‘shin splints’ and some clinicians define both terms as lower leg exertional pain not due to a compartment syndrome, fracture or muscle hernia (Batt et al. 1998; Edwards Jr. et al. 2005).

(a–c) Long-distance runner with recurrent anterior lower leg pain. (a) Coronal proton-density MR image of the tibia showing a fracture line (arrow) in the anterior tibial cortex and associated marrow oedema-like signal intensity in keeping with a stress fracture. (b) Axial proton-density-weighted MR image of the tibia showing marrow oedema-like signal intensity (arrow) in the anterior cortex of the tibia. (c) Lateral radiograph shows cortical hypertrophy and a ‘black line’ defect on the anterior cortex of the middle third of the tibia. Persistent fracture in this case resulted in the need for IM nail insertion in order to aid healing

(a, b) Professional athlete with persistent anterior lower leg pain. (a) Axial T1-weighted MR image and (b) axial proton-density-weighted fat-suppressed MR image reveal bone marrow and endosteal oedema (arrow) involving the anterior aspect of the mid diaphysis of the tibia, in keeping with a stress reaction, but no fracture is seen here
Compressive stresses are concentrated on the concave aspect of the posteromedial tibial cortex stimulating osteoblastic and osteoclastic activity as the bone remodels (Anderson et al. 1997, Batt et al. 1998, Fredericson et al. 1995, Yates and White 2004). As with other osseous stress reactions, as the repetitive loading continues, trabecular failure may occur, ultimately resulting in cortical fracture (Fig. 7).

Female marathon runner presenting at major games with continuous anterior tibial pain. Lateral radiograph of the tibia shows anterior cortical thickening and multiple stress fractures. The athlete had to withdraw from competition
MTSS is a very common cause of overuse leg injury, with an incidence ranging from 4% to 35% in athletic and military recruits (Bonasia et al. 2015). As in other osseous stress injuries the development of this condition is increased in athletes that are female, have a pronated foot or have injury elsewhere within the lower limb kinetic chain (Batt et al. 1998; Yates and White 2004). It is bilateral in over 70% of cases which is thought to relate to running and jumping (e.g., basketball and tennis) being the most common underlying mechanisms of injury. The area of diaphysis affected can vary depending on sporting activity but the majority of injuries involve the mid and distal diaphyseal region where the cross-sectional area is smallest (Batt et al. 1998; Anderson et al. 1997; Fredericson et al. 1995; Yates and White 2004). Clinical findings include diffuse posteromedial tibial tenderness which is unaffected by ankle or knee movement (Batt et al. 1998; Edwards Jr. et al. 2005; Bonasia et al. 2015).
3.2.1 Imaging and Management of Osseous Stress Reaction
In athletes it is especially important to make an early diagnosis and determine the extent of osseous damage to give prognostic information (Ohta-Fukushima et al. 2002). Radiographs are insensitive and can be negative in up to 85% of cases but are usually performed initially to exclude a complete fracture (Fig. 6) (Anderson et al. 1997; Ohta-Fukushima et al. 2002; Batt et al. 1998; Fredericson et al. 1995; Gaeta et al. 2005; Bonasia et al. 2015). MR imaging has been repeatedly shown to be an accurate, sensitive and specific technique compared to CT and isotope scanning (Anderson et al. 1997; Milgrom et al. 1984; Batt et al. 1998; Fredericson et al. 1995; Gaeta et al. 2005).
T2-weighted (fat-suppressed) MR sequences are most sensitive for detecting periosteal, cortical and bone marrow oedema (Fig. 8) (Anderson et al. 1997; Batt et al. 1998; Gaeta et al. 2005). Isotope bone scans show increased activity but lack spatial resolution (Fig. 9) and can be negative if osteoblastic activity is markedly reduced (Milgrom et al. 1984).

Running athlete with clinical diagnosis of anterior shin splints. Axial T2-weighted fat-suppressed MR image shows marked anterolateral periosteal oedema of the tibia with no associated intracortical or bone marrow change

(a–c) Running athlete with tibial pain. (a) Lateral radiograph shows diffuse anterior cortical thickening (arrowheads) with an ill-defined lucency in the superficial cortex (arrow). (b) Isotope bone scan image shows increased uptake (arrow) in the region. (c) Corresponding axial CT shows diffuse resorption through the anterior cortex but also a linear fracture (arrows)
The MR classification and the management of osseous stress reaction are summarised in Table 1. Further discussion is beyond the scope of this chapter (see Lefere et al. 2021 and Karantanas 2021, respectively).
3.3 Chronic Exertional Compartment Syndrome (CECS)
Compartment syndrome is defined as increased interstitial pressure within an anatomically confined compartment that interferes with neurovascular function. Normal pressures within a muscle compartment are between 0 and 4 mmHg and can peak above 60 mmHg on exercise but quickly dissipate on cessation. However, if this pressure is sustained above 15 mmHg blood flow is compromised and muscle ischaemia can occur (Zabetakis 1986). The pathophysiology of increased tissue pressures is not yet fully understood (Guermazi et al. 2017).
Chronic exertional compartment syndrome commonly affects the anterior and lateral calf lower leg muscular compartments (Peterson and Renstrom 1986; Zabetakis 1986; Martens et al. 1984; Gaeta et al. 2008). It is thought to occur because of abnormally increased pressure within muscle compartments enclosed by relatively noncompliant fasciae. Potentially any athlete can be affected but it is particularly common in distance runners, cyclists and cross-country skiers. The athlete usually presents with crescendo pain and paraesthesia after exercise which eases on ceasing activity and unlike popliteal artery syndrome is not posture dependant (Martens et al. 1984; Nicholas and Hershman 1986). There may also be muscle swelling and it is important to rule out an underlying muscle hernia which usually exists in 40–60% of patients (Bonasia et al. 2015). The diagnosis can sometimes be made with history alone but intracompartmental pressure monitoring, MRI and near-infrared spectroscopy are useful to establish a diagnosis (Bonasia et al. 2015). Recent work has demonstrated that the sensitivity of MRI in the diagnosis of chronic exertional compartment syndrome was comparable to measuring compartment pressure with a slit or weak catheter (Gaeta et al. 2008).
3.3.1 Imaging
The role of near-infrared spectroscopy and MRI is yet to be established in the diagnosis of chronic exertional compartment syndrome (Bonasia et al. 2015) and it is not routinely used in clinical practice at present.
On ultrasound the muscle can appear echogenic with relative sparing of periseptal areas which are still receiving sufficient blood flow from the adjacent fascia (Van Holsbeeck and Introcasco 2001). Studies evaluating muscle cross-sectional area on ultrasound both before and after exercise describe two different patterns in symptomatic patients. In one group the muscle compartment cannot expand with a relatively rigid fascia compared to normal subjects (where muscle volume can increase by 10–15%). In the other symptomatic group, although the muscle compartment does expand during exercise, there is a slow reduction in volume post-exercise compared to normal subjects (Van Holsbeeck and Introcasco 2001).
Post-exercise MR imaging can show oedema in the clinically affected muscles confirming the diagnosis (Fig. 10). However, this technique despite being sensitive post-exercise is not completely specific with oedema being found in asymptomatic athletes and normal muscle appearances occurring in athletes with objective clinical features (Fig. 11) (Tucker 2010).

(a, b) Running athlete with chronic exertional right-leg pain. Axial T2-weighted fat-suppressed MR image post-exercise shows persisting soleus oedema (arrowheads) (a), on right right side, and (b) normal appearances on the left asymptomatic side. The athlete underwent fasciotomy

Running athlete with chronic exertional right-leg pain, clinically related to soleus. Axial T2-weighted fat-suppressed MR image post-exercise shows soleus oedema (arrows). Note asymptomatic peroneus muscle oedema (arrowheads)
The initial treatment of chronic exertional compartment syndrome includes training modifications and assessment for orthotics; however, if symptoms persist fasciotomy of the muscle compartment is performed. Morbidity can potentially result if there is subsequent muscle herniation or scarring (Van Holsbeeck and Introcasco 2001).
3.4 Vascular and Nerve Compression
3.4.1 Vascular
Popliteal artery entrapment is an uncommon cause of chronic exertional calf pain which can occur during exercise or on particular postural changes (Atilla et al. 1998; Elias et al. 2003). The condition is usually precipitated in young male athletes by a change in muscle bulk due to adolescent growth or increased training (Atilla et al. 1998; Collins et al. 1989; Edwards Jr. et al. 2005). This most commonly occurs in sports which involve high-intensity repetitive plantar and dorsiflexion such as soccer, basketball and running. Repeated knee flexion resulting in microtrauma and intimal fibrosis of the artery resulting in this condition have been described in a skier (Toorop et al. 2004).
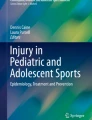
Symptoms occur due to muscle ischaemia from compression of the popliteal artery (and occasionally vein) at the level of the medial head of gastrocnemius (MHG). The MHG can be normal with compression resulting from muscle hypertrophy; however, more frequently there is also a congenital anomalous origin or fibrous slip. Causes of the condition can be classified into six types (Fig. 12): medial deviation of popliteal artery and normal MHG (type 1), aberrant origin of MHG from intercondylar notch compressing the artery (type 2), slip of MHG compressing the popliteal artery (type 3), popliteal artery passing deep to popliteus muscle or fibrous band in the popliteal fossa (type 4), any entrapment also resulting in the involvement of the popliteal vein (type 5) and compression of a normal artery by a normal but hypertrophied MHG (type 6) (Collins et al. 1989; Rich et al. 1979; Labmayr et al. 2019).

Line drawing of PAES
The diagnosis is clinical with complete loss or a decrease in ankle pulses between dorsiflexion and plantarflexion associated with calf and foot pain. The underlying abnormality can be bilateral in up to 67% but does not always result in bilateral symptoms (Collins et al. 1989; Chernoff et al. 1995; Hai et al. 2008).
3.4.2 Imaging and Management
The diagnosis, extent and severity of compression can be confirmed by imaging using a combination of ultrasound, MR imaging (angiography) or conventional arteriography. Ultrasound is typically the first technique used and can depict change in vessel calibre and distal flow showing systolic peaks and dampening during dynamic manoeuvres (Fig. 13a, b). The artery may be medially deviated by muscle, but this is present in less than 25% of cases. MR imaging is nearly always then performed as it allows complete non-invasive investigation of muscular anatomy while time-of-flight angiography can depict vessel compression in different foot positions (Fig. 13c) (Atilla et al. 1998). Subsequent complications such as adventitial disease or post-stenotic aneurysms can also be demonstrated by MR imaging although this is rare in true athletic-induced pain. If MR imaging features are equivocal angiography may be required to more accurately define the degree of compression (Fig. 13d, e) (Atilla et al. 1998; Edwards Jr. et al. 2005).

(a–e) Male track hurdler with recent onset of intermittent calf pain. (a) Doppler ultrasound evaluation of the right popliteal artery shows normal systolic and diastolic waveform. (b) Corresponding evaluation with plantarflexion shows dampening of the systolic and diastolic variation consistent with arterial compression. (c) Time-of-flight MR angiography image shows complete vessel occlusion on plantarflexion (arrow). (d) Subtraction angiography image shows normal vessel calibre in neutral position and (e) subsequent complete occlusion on plantarflexion. At surgery an anomalous slip of the medial head of the gastrocnemius was identified (grade 3 abnormality)
3.4.3 Nerve Compression
Treatment in athletes usually requires surgical release of the MHG and anomalous slips:
In the lower limb this most commonly involves the common or superficial peroneal nerves. This is usually thought to be due to fascial thickening or scarring (see later) or less commonly because of an adjacent bony abnormality, ganglion cyst or an intraneural ganglion (Nicholas and Hershman 1986; Yablon et al. 2016). Superficial peroneal injury can occur secondary to trauma and is seen in dancers, football players and runners. The peroneal nerve has a superficial course and lacks epineural supporting tissue with traction injuries, contusion and penetrating trauma being the three mechanisms involved in the spectrum of pathological conditions. Traction injuries of the peroneal nerve can occur following ankle inversion, high-grade varus sprains of the knee, proximal fibular fractures, dislocation of the knee and posterolateral corner injury. Oblique locking screws in intramedullary tibial nailing may also result in peroneal nerve palsy.
Direct impact in contact sports and football may result in peroneal nerve contusion. The nerve will appear hyperintense on T2-weighted imaging, hypointense on T1-weighted imaging and thickened. Oedema in the adjacent lateral compartment muscles and in the proximal fibula should alert the reporting radiologist to a potential peroneal nerve lesion. Other miscellaneous lesions resulting in peroneal nerve injuries include anterior or lateral compartment syndrome after minor trauma and a Morel-Lavallée lesion (Van Den Bergh et al. 2013).
A ganglion of the proximal tibiofibular joint can result in direct compression of the common peroneal nerve (Fig. 14a, b) or actually extend into and along the nerve sheath (Fig. 14c) (Ilahi et al. 2003; Miskovsky et al. 2004; Spinner et al. 2000).

(a–c) Two runners with lateral calf pain on exertion. (a) Axial T2-weighted fat-suppressed MR image shows a ganglion (arrows) extending into the peroneus muscles adjacent to the fibula (F). Note low-signal fibrous tissue (*) within the ganglion. (b) Coronal T1-weighted fat-suppressed post-IV gadolinium MR image shows low-signal fluid (*) and the enhancing ganglion wall (arrows) tracking to the tibiofibular joint (T = tibia, F = fibula). (c) Coronal T2-weighted fat-suppressed MR image in a different runner shows a high signal and enlarged common peroneal nerve (*). At surgery this was found to be a neural cyst originating from the tibiofibular joint
Traditionally the diagnosis of peripheral neuropathy has been based on history, clinical findings and electromyography. Imaging also plays an important role and magnetic resonance neurography is gaining an increasing role in the diagnosis of peripheral nerve disorders (Chhabra et al. 2012).
4 Acute Lower Limb Muscle Injury
Muscle and tendon injury most commonly occurs at zones of anatomical or functional transition as these sites generate the greatest concentrations of intrinsic forces (Garrett Jr. et al. 1987; Nordin and Frankel 2001b). These are the commonest injuries in all sporting activities because the lower limb is essential for athletic movement.
4.1 Biomechanical Basis of Acute Lower Limb Muscle Injury
Lower limb muscles experience a wide range of physiological movement and must be able to maintain significant stamina while undergoing repetitive explosive activity. Studies have shown that acute muscle injury, especially of the lower limb, accounts for more than 37% of all athletic injuries. The hamstring muscle complex is the most commonly affected (Guermazi et al. 2017). The rectus femoris and gastrocnemius muscles are also frequently affected. These muscles are more susceptible because they contain a high proportion of fast-twitch type 2 fibres and span multiple joints (Guermazi et al. 2017).
4.2 Imaging of Acute Lower Limb Muscle Injury
In experienced hands and with modern equipment MR imaging and ultrasound are both accurate techniques for the evaluation of lower limb muscle injury (Robinson 2004; Van Holsbeeck and Introcasco 2001; Connell et al. 2004; Cross et al. 2004; Steinbach et al. 1998; Flores et al. 2018). However, the large muscle bulk often present in athletes means that the depth of resolution and field of view offered by ultrasound can be limiting especially in the pelvis and proximal thigh. Acute muscle injuries can be classified as direct or indirect, with direct injuries resulting in lacerations and contusions and indirect injuries in muscle tears. The latter account for the majority of significant muscle injuries in high-level athletes (Purohit and King 2015). In mild contusion, US shows focal isoechoic muscle swelling and the lesion usually resolves quickly. With more severe contusions, the haematoma may vary in appearance depending on the time between injury and examination. Initially within the first 20 h haematomas may appear both hyperechoic and hypoechoic. Within the following days, haematomas tend to appear hypoechoic or anechoic and will subsequently resolve, possibly resulting in scar tissue (Draghi et al. 2013).
4.2.1 Hamstring Injuries
This muscle group is particularly susceptible to strain with injury occurring during running and sprinting as the muscles eccentrically contract decelerating knee extension (Mink 1992; Shellock et al. 1991; Nicholas and Hershman 1986; Garrett Jr. 1988; Slavotinek et al. 2000; De Smet and Best 2000; Garrett Jr. et al. 1984; Speer et al. 1993; Taylor et al. 1993; Rubin 2012). Contusions to the hamstrings are rare (Rubin 2012). The three muscles (semimembranosus, semitendinosus and biceps femoris) cross two joints (hip and knee) and have the largest proportion of type 2 fast-twitch fibres in the body. A number of clinical and imaging studies have confirmed that the long head of biceps femoris is the most commonly injured muscle accounting for over 80% of all injuries (alone or in combination) with partial tears more common than complete tears (De Smet and Best 2000; Slavotinek et al. 2000; Speer et al. 1993; Rubin 2012). In comparison to the other muscles within the group it has two heads proximally (long and short), which mechanically reduces the elasticity of the muscle making it more susceptible to acute injury (Fig. 15). The proximal or distal myotendinous area can be injured with almost equal incidence and strains can appear intramuscular as histologically the tendons extend throughout a large proportion of the main muscle (Fig. 16) (Garrett Jr. et al. 1984). Acute injuries are more frequent in older players and those with previous identical hamstring injuries. Hamstring injuries increase during the competitive season (Hagglund et al. 2013).

Professional footballer with acute-onset thigh pain. Axial T2-weighted fat-suppressed MR image shows minor area of oedema (arrow) within the long head of biceps femoris (grade 1 injury)

(a–c) Professional footballer with recurrent hamstring injuries. (a) Axial T2-weighted fat-suppressed MR image from 2002 shows an acute grade 2 injury involving the long head of biceps femoris (small arrowheads). (b) Corresponding longitudinal ultrasound image 1 week later shows a hypoechoic haematoma (H) with an area (arrowheads) occupying 10–20% of the muscle diameter (grade 2 injury). (c) Axial T2-weighted fat-suppressed MR image from new injury in 2005 shows marked oedema involving the myotendinous junction of the short and long heads (arrowheads) of biceps femoris
Semimembranosus and semitendinosus are rarely affected on their own although isolated semitendinosus tears can occur particularly in running and jumping athletes (De Smet and Best 2000). This is thought to be secondary to sudden forced hip flexion with knee extension which is required to hurdle or perform the long jump.
Several studies have evaluated specific imaging factors for hamstring injury and subsequent time to recovery. There are numerous imaging systems for grading of acute muscle injury with the most widely used being the ‘modified Peetrons’ and BAMIC (British Athletics Muscle Injury Classification) methods (Pollock et al. 2014). Studies have shown that these techniques are reasonably reproducible; however their isolated use for predicting return to play is less so. Higher grade (severe) injuries do correlate with a significantly longer return to sport but the lower grades in these classifications are less discriminatory.
The British Athletics Muscle Injury Classification grades hamstring injuries from 0 to 4 based on MRI indicators of injury extent (cross-sectional area and length of injury) and classifies location according to their anatomical site: myofascial (a), musculotendinous (b) or intratendinous (c).
Grade 0 injuries encompass injuries that are MRI negative reflecting a focal neuromuscular injury or muscle injury consistent with DOMS. Grade 1–3 injuries are small, moderate or extensive tears of muscle tissue, respectively (Figs. 16, 17, and 18). Grade 4 injuries are complete tears to either muscle or tendon.

(a, b) Professional footballer with acute-onset thigh pain. (a) Axial proton-density-weighted fat-suppressed MR image and (b) corresponding coronal proton-density-weighted fat-suppressed MR image demonstrate a hamstring tear (arrow) represented by a region of high signal intensity adjacent to the myotendinous junction of the long head of biceps femoris with interstitial feathery high signal. The tendon demonstrates features of laxity indicative of tendon involvement (BAMIC grade 2c injury). Moderate perifascial fluid is also present

(a) Axial proton-density-weighted fat-suppressed MR image showing a grade 2 biceps femoris tear (arrow) with oedematous change around the sciatic nerve. (b) Transverse ultrasound image of the conjoint tendon demonstrating a heterogeneous mass with mixed hypo- and hyperechogenicity compatible with a haematoma around the conjoint tendon. The site of tear was treated with platelet-rich plasma (PRP) injection (black arrow shows needle) as the patient was symptomatic, avoiding the sciatic nerve (arrow)
Hamstring injuries that are intratendinous are more prone to re-injury and result in a delay in time to return to full training. This study also demonstrated an increased time to return to full training in the more extensive grade of tendon injury, i.e., grade 3 injury (Pollock et al. 2016).
4.2.2 Quadriceps
Rectus femoris is the most commonly injured muscle within the quadriceps group and the second or third most injured after hamstring strains (Speer et al. 1993; Peterson and Renstrom 1986; Garrett Jr. 1988; Garrett Jr. 1990; Noonan and Garrett Jr. 1999; Taylor et al. 1993; Kassarjian et al. 2014). The rectus femoris differs from the other group muscles in that it spans two joints, the hip and the knee joint, and originates from two heads (indirect and direct).
The rectus femoris outer unipennate muscle originates from the anterior aponeurosis which forms the direct tendon and attaches to the anterior inferior iliac spine. The inner bipennate muscle originates from the central aponeurosis which forms the indirect tendon and is inserted into the superior acetabular ridge and posterolateral aspect of hip joint capsule. This envelopment results in a muscle-within-a-muscle configuration.
Due to its complex anatomy and muscle-within-a-muscle structure, injuries to the rectus femoris muscle may not always be classified according to the traditional three-point muscle injury grading system.
The most common site of rectus femoris injury in football involves injury of the distal myotendinous junction when the muscle belly strips from the undersurface of the distal tendon (Fig. 19).

Professional footballer with distal thigh pain 1 week after acute injury. Axial T2 weighted fat suppressed MR image of the mid thigh shows a region of injury centred around the myotendinous junction with feathery oedema surrounding the central tendon. There is a region of haematoma formation (arrow) also seen which is low in signal in this subacute injury
The indirect component of rectus femoris has a long intramuscular myotendinous junction and is susceptible to a more unique longitudinally oriented injury. This results in not only myotendinous injury, but also in separation and dissociation of the inner bipennate component from the outer unipennate muscle (a type of intramuscular degloving injury), and may lead to retraction of the inner muscle belly. This degloving injury differs from the typical myotendinous injury of the indirect portion of the rectus femoris and occurs in the periphery of the fibres of inner bipennate muscle (Figs. 20 and 21) (Kassarjian et al. 2014).

(a, b) Professional footballer with severe proximal thigh pain. (a) Axial T2-weighted fat-suppressed MR image showing an acute tear of the myotendinous junction of the indirect head of the rectus femoris (arrow) and a heterogeneous area of intramuscular oedema. (b) Coronal proton-density-weighted fat-suppressed MR image shows a full-thickness tear of the indirect head of rectus femoris tendon with complete disruption of the musculotendinous junction (arrow)

(a–d) Professional footballer with severe acute proximal thigh pain. (a) Axial T1- and (b) T2-weighted fat-suppressed MR images show a swollen and oedematous proximal right rectus femoris (*), extensive perifascial fluid (arrows) and intact low-signal tendon (arrowhead). (c) Axial T2-weighted fat-suppressed MR image above the level of the previous images shows more extensive muscle oedema and fluid (arrows) extending towards vastus lateralis (VL) and overlying sartorius (S). A small remnant of muscle is seen intact (arrowheads). (d) Longitudinal extended field-of-view ultrasound image confirms grade 2 injury (arrowheads) just distal to the origin from the anterior inferior iliac spine (AIIS). The muscle deep to the area and adjacent to the femur (Fe) appears intact (arrows)
4.2.3 Calf
The gastrocnemius-soleus muscles eccentrically contract to modulate dorsiflexion at the ankle during normal gait and heel strike. However, in sprinting the foot initially strikes the ground with the distal first and second rays and not the heel resulting in more forceful ankle dorsiflexion (Lees and Nolan 1998; Novacheck 1998; Sammarco and Hockenbury 2001). This muscle complex also concentrically contracts on push-off for sprinting, jumping and cutting-in.
Aponeurosis distraction is a specific type of injury which occurs at the margin of two synergistic muscles. The muscles most frequently involved are the medial head of gastrocnemius and soleus or, less commonly, semimembranosus and semitendinosus (Bianchi et al. 1998). When this involves the medial head of gastrocnemius it is known as ‘tennis leg’ (Bianchi et al. 1998; Mink 1992; Harwin and Richardson 2017). This injury typically occurs during forced dorsiflexion with the knee in extension causing powerful eccentric loading of the gastrocnemius and soleus muscles. Although in the past there has been debate over whether plantaris is primarily involved (Helms et al. 1995), larger reviews of this condition have subsequently shown little or no involvement of plantaris with the medial head of gastrocnemius being the primary site of injury with fluid between the soleus and gastrocnemius muscles (Fig. 23) (Bianchi et al. 1998; Delgado et al. 2002; Speer et al. 1993; Harwin and Richardson 2017). The aponeurosis between the two muscles is a potentially weak area as soleus consists mainly of T1 fibres and is relatively inelastic compared to the gastrocnemius which also spans two joints and consists of T2 fibres (Bianchi et al. 1998; Mink 1992). The Achilles tendon is usually not injured.
Ultrasound or MR imaging can demonstrate muscle fibre disruption adjacent to the aponeurosis and the presence of perifascial fluid and haematoma (most commonly a grade 2 injury) (Fig. 22) (Bianchi et al. 1998; Delgado et al. 2002). These injuries respond well to conservative treatment although scarring can occur in the region of the aponeurosis (Fig. 23) (Bianchi et al. 1998).

(a, b) Rugby league player with acute onset calf pain. (a) Axial T2-weighted fat-suppressed and (b) sagittal T2 weighted fat suppressed MR imaging of the calf showing acute injury to the soleus myotendinous junction with muscle fibre disruption seen around the central tendon. A small tendon defect (white arrow) is seen in this grade 2c soleus injury. Haematoma formation is seen deep to the medial soleus muscle belly (black arrow)

Professional ballet dancer with previous calf pain and persisting swelling but relatively little symptoms. Transverse extended field-of-view ultrasound image shows a normal-appearing lateral head of gastrocnemius (LHG) but hyperechoic nodular thickening (arrowheads) between the medial head of gastrocnemius (MHG) and soleus (So). This is consistent with scar tissue and adjacent fascia appears of more normal thickness (arrows)
Soleus muscle injuries have been previously considered rare, potentially due to the widespread use of sonographic assessment; however, they are now felt to be more frequent than previously thought as a result of increased use of MR imaging.
Ultrasound is not sensitive enough in assessing soleus traumatic tears compared with MR imaging (Fig. 24). Injuries at the myofascial junction are more readily identified than those at the musculotendinous units. Factors which contribute to difficult visualisation and underappreciation of soleus injuries include the deep location of the soleus muscle and the fact that soleus is often extensively vascularised. Moreover, soleus injuries may be underappreciated in the context of a more superficial (and therefore easily detectable) gastrocnemius strain (Balius et al. 2014). Therefore, subtle soleus injuries may be missed sonographically. MR imaging has become the modality of choice for detection of soleus strains. Soleus injuries on MRI may be classified as musculotendinous or myofascial.

(a–c) Professional rugby league player with acute calf pain. (a) Longitudinal ultrasound image shows subtle soleus injury with hypoechoic change abutting the posterior cortex of the tibia (arrow). (b) Axial T1-weighted MR image and c axial T2-weighted fat-suppressed MR image showing grade 2 injury of the soleus muscle with low-grade muscle fibre disruption
4.3 Delayed-Onset Muscle Soreness
Delayed-onset muscle soreness (DOMS) develops when specific muscle groups undergo unaccustomed vigorous exercise (Flores et al. 2018). This usually occurs in recreational athletes who sporadically participate in sport; however, this can also occur in professional athletes when training is intensified after injury. The aetiology of DOMS is thought to be due to increased compartment pressure and water content affecting type 2 fast-twitch fibres with resultant disruption of the Z bands of sarcomeres within the muscle (Flores et al. 2018).
Clinically diffuse lower limb muscle pain develops 12–24 h after activity and is exacerbated by eccentric contraction (Noonan and Garrett Jr. 1999; Newham et al. 1983; Zabetakis 1986). This helps to clinically differentiate DOMS from a muscle tear or strain, which usually causes immediate focal pain and is exacerbated by concentric contraction. Additionally DOMS usually resolves within 7 days without any specific treatment (Peterson and Renstrom 1986; Mink 1992).
Imaging is rarely necessary in the majority of cases (Fornage 2000) but can be useful in excluding other causes of severe pain if the clinical history is not clear. MR imaging can show oedema in multiple muscles, but this is not a specific or sensitive finding with the abnormality persisting up to 82 days after clinical resolution (Marcantonio and Cho 2000; Steinbach et al. 1998). At the early phase of injury perifascial fluid may be demonstrated. The involved muscle belly may also demonstrate diffuse muscle oedema without the feathery pattern typical of strain or perifascial fluid (Guermazi et al. 2017). Ultrasound is usually normal, but its main role is for excluding a significant muscle strain or tear, which allows appropriate rehabilitation to continue.
4.4 Muscle Contusion
Muscle contusion occurs secondary to direct nonpenetrating trauma causing muscle fibre disruption and haematoma. This usually results from muscle being compressed against bone but can also occur when superficial muscle is compressed against a contracted underlying muscle (Jarvinen et al. 2005). Muscle contusion is commonly seen in contact sports (‘dead leg’) with rectus femoris and vastus intermedius being the most affected muscles (Flores et al. 2018). It is a clinical diagnosis obtained from patient history, but on examination, compared to a severe muscle tear, muscle function is relatively normal given the degree of pain (Zarins and Ciullo 1983; Jarvinen et al. 2005; Armstrong 1984; Stauber 1988; Jackson and Feagin 1973).
4.4.1 Imaging
In a similar manner to muscle strain MR imaging or ultrasound can be used to evaluate the muscle and underlying periosteum although MR imaging is preferable if an associated bone injury is suspected. The difficulty for either imaging modality is defining if there is muscle distraction especially if the clinical history is unclear.
On ultrasound an acute contusion (0–48 h) appears ill defined with irregular margins and marked echogenic swelling of the fascicles and entire muscle (Fig. 25) (Aspelin et al. 1992). MR imaging also demonstrates oedema and mixed intrinsic signal as the blood products develop. In comparison to muscle strain, contusion is characterised by the haematoma crossing aponeurotic boundaries representing the demarcation of the impact (Robinson 2004; Van Holsbeeck and Introcasco 2001).

Rugby player with lower leg pain following a direct impact injury. Transverse ultrasound image of the lateral aspect of the lower leg with diffuse hyperechoic change present within the peroneal muscle compartment and also in the overlying subcutaneous tissues in keeping with a muscle contusion
In severe clinical cases, dynamic ultrasound imaging may be helpful to confirm that a complete tear is not present and to document the extent of muscle damage and any retraction. At 48–72 h ultrasound appearances become better defined with the haematoma appearing hypoechoic and a clearer echogenic margin which expands centrally as the muscle repairs (Van Holsbeeck and Introcasco 2001; Robinson 2004). MR imaging also demonstrates these changes although the degree of adjacent muscle and soft-tissue oedema can persist for some time.
In the following weeks the contusion can be monitored for regeneration of muscle, scar tissue or more rarely myositis ossificans (Zarins and Ciullo 1983; Garrett Jr. 1988). However, in sporting injuries, the majority of contusions heal with normal muscle regeneration and chronic complications are relatively rare (Peterson and Renstrom 1986; Jarvinen et al. 2005).
5 Complications of Lower Limb Muscle Injury
5.1 Fibrous Scarring
Scar tissue can restrict muscle function resulting in reduced contractile strength increasing the risk of re-injury at the junction of the muscle and scar (Fig. 26) (Speer et al. 1993; Jarvinen et al. 2005; Taylor et al. 1993). Scar tissue, especially after hamstring tears, can also involve adjacent nervous tissue and cause referred symptoms which produce significant pain on sprinting or sudden movement (Fig. 27).

(a, b) Professional footballer with previous hamstring injury complaining of recurrent pain. (a) Axial T1- and (b) T2-weighted fat-suppressed MR images show normal left semitendinosus (ST). There is reduced muscle bulk on the right, thickened (scarred) low-signal tendon (arrow) and oedema (arrowheads) within the remaining muscle indicating a retear

(a, b) Professional footballer with previous hamstring injury. (a) Axial proton-density-weighted fat-suppressed MR image showing conjoint tendon injury with oedema and (b) axial proton-density-weighted fat-suppressed MR image obtained 6 weeks after the initial injury showing a further acute injury at the same site where there is thickening of the tendon (white arrow) at the site of previous healing
MR imaging usually defines scar tissue as a low-signal soft-tissue thickening either paralleling the tendon (Fig. 26) or with a more amorphous appearance at the muscle periphery (Fig. 27). Ultrasound detects fibrotic scarring as an echogenic focus, but dynamic stressing can assess the relative inelasticity of this tissue and any adherence to adjacent structures which is why this technique is most useful for initial evaluation in athletes (Fig. 28).

Professional football player with previous hamstring tear and leg pain on sprinting. Transverse ultrasound image shows peripheral echogenic scar tissue (arrows) of semitendinosus adherent to the sciatic nerve (S) with some loss of the normal muscle echotexture (*) due to previous injury
5.2 Myositis Ossificans
Myositis ossificans is a rare complication of muscle injury and usually develops after injuries associated with a large haematoma or contusion.
Clinically the development of myositis ossificans should be suspected when the degree of pain and soft-tissue swelling persists and is out of proportion to the original injury (Peterson and Renstrom 1986; Lacout et al. 2012). The commonest muscle group involved by this condition is the quadriceps, as this area is most commonly affected by muscle contusion.
Prior to the development of calcification or ossification ultrasound appearances are similar to an organising haematoma (see contusion before). However, an advantage of ultrasound is that it can depict the zone phenomenon with calcification being peripheral and centripetal (Lacout et al. 2012) and demonstrate the relatively well-defined peripheral margins and borders with adjacent soft tissues (Bodley et al. 1993; Peck and Metreweli 1988). MR imaging performed at this stage can show an extremely heterogeneous appearance with surrounding oedema that can sometimes be misinterpreted as an aggressive or even malignant process (Fig. 29) (De Smet et al. 1992; Shirkhoda et al. 1995). Ultrasound can also demonstrate peripheral calcification and ossification, as early as 2–3 weeks, before it is clearly evident on plain-film or MR imaging (Bodley et al. 1993; Peck and Metreweli 1988; Lacout et al. 2012).

(a–c) Painful rapidly growing mass in a professional footballer following previous direct blow to the distal hamstring region. (a) Axial T1-weighted MR image showing a hyperintense mass abutting the posterior femoral cortex. (b) Lateral radiograph of the thigh shows an ossified lesion with a noncalcified central area arising from the posterior cortex of the femur. (c) Axial CT image showing a mass typical of myositis ossificans in the posterior thigh muscles, with peripheral ossification
5.3 Muscle Atrophy/Hypertrophy/Hernia
On MR imaging muscle atrophy shows decreased muscle bulk and increased T1-weighted signal due to fat deposition between the muscle fibres. These features are not uncommonly seen in muscles which retear (Fig. 30). On ultrasound the muscle echotexture is increased due to fat deposition with additional loss of fascial plane definition.

(a, b) Triathlete with previous high grade right sided proximal rectus femoris injury. (a) T2 weighted fat suppressed axial MR imaging shows here is thickening of the rectus femoris tendon at the site of previous injury (arrow). (b) T2 weighted axial imaging - there is adjacent fat atrophy change within the muscle around the myotendinous junction and relative loss of muscle bulk
A muscle hernia, also known as myofascial herniation, is defined as an abnormal protrusion of muscular tissue through a fascial defect, initially described by Richet in 1853 (Naffaa et al. 2017). This commonly occurs in the anterior and lateral muscle groups of the lower leg (especially tibialis anterior) (Fig. 31) but is also recognised within peroneus longus, peroneus brevis, extensor digitorum longus, gastrocnemius and flexor digitorum longus (Bianchi et al. 1995). It is thought that the fascia overlying tibialis anterior has an area of potential weakness due to penetrating branches of the peroneal nerve and vessels (Khaladkar et al. 2016).

(a) Transverse and (b) longitudinal ultrasound images of the anterolateral aspect of the leg showing an acute muscle hernia in a professional footballer after blunt trauma of the anterolateral aspect of the leg. Protrusion of the extensor digitorum longus muscle through a defect in the overlying fascia is shown (arrow)
The hernia usually presents as a mass which may only appear after exercise or on standing (Bianchi et al. 1995). The hernia may be painful on exertion and the clinical differential diagnosis includes an incompetent perforating vein or chronic exertional compartment syndrome.
Ultrasound can accurately identify the normal thick echogenic muscle fascia with any defect seen as a hypoechoic gap (Fig. 31) (Bianchi et al. 1995). Dynamic manoeuvres (using a gel stand-off) can be performed to reproduce the muscle hernia if it is currently reduced. On acute herniation the muscle may appear hyperechoic due to compression of the fascial planes within it. However, if chronic it may appear hypoechoic and ill defined due to a degree of oedema (Bianchi et al. 1995). MR imaging can demonstrate a hernia if present at rest but may be relatively ineffective in demonstrating small or exertional lesions (Bianchi et al. 1995; Steinbach et al. 1998).
5.4 Morel-Lavallée Lesion and Periosteal Haematoma
5.4.1 Morel-Lavallée Lesion
Athletes can develop Morel-Lavallée lesion through contact injuries most commonly in football and rugby when tackling involves the lower limb. The injury is usually a direct force which causes a shearing injury between the subcutaneous fat and underlying deep fascia and muscles. The areas most commonly affected are the lateral hip where the overlying subcutaneous fat may shear from the tensor fascia lata and the anteromedial or anterolateral knee where the fat shears from the underlying vastus retinaculum and extensor mechanism (Robinson et al. 2008). During the acute phase, ultrasound shows haematoma and oedema between fascia and fat. The underlying muscles often appear normal. Individual fat lobules can be visualised as separated by blood products and fluid and over time a pseudocapsule may form (Mclean and Popovic 2017). The resulting mass has been named a Morel-Lavallée lesion. Appearances are variable but are generally hypoechoic with hyper- and hypoechoic fat lobules separated by septa and hypoechoic fluid, surrounded by the hyperechoic pseudocapsule. MRI shows fluid and fat oedema at the fascial interface with subcutaneous haemorrhage in the acute phase (Fig. 32). Sedimentation of blood components can also result in a fluid-fluid levels. Slow growth can occur over time due to reaccumulation of fluid and the appearance, along with the associated pain, can be misdiagnosed as soft-tissue tumour, particularly if the trauma has been omitted from the history. Chronic lesions may develop a fibrous pseudocapsule and calcify with reaccumulation of fluid causing growth. MRI may be useful to further evaluate uncertain cases, as is follow-up interval scanning.

(a, b) Pain and swelling of the lateral knee in a professional footballer caused by a chronic haematoma after a sheering injury. (a) Axial proton-density-weighted fat-suppressed MR image and (b) coronal proton-density fat-suppressed MR image showing a Morel-Lavallée lesion located over the lateral aspect of the knee with areas of heterogeneous hyperintensity and septa formation secondary to shearing of the subcutaneous tissues away from underlying fascia
5.5 Periosteal Haematoma
Periosteal haematoma may be seen after a direct-impact injury and represents a collection of blood underneath the periosteum. The imaging findings are initially of smooth periosteal reaction which matures over time, often with associated new bone formation. Imaging may be helpful in order to differentiate between myositis ossificans and periosteal haematoma (Fig. 33).

(a–c) Pain in the quadriceps compartment 2 months following direct-impact injury. (a) Plain-film and (b, c) ultrasound images showing periosteal haematoma within the mid-shaft of the femur. There is smooth, well-established periosteal reaction. The adjacent musculature images normally
6 Conclusion
Imaging injuries in high-level athletes is a complex but rewarding process as the diagnosis can markedly influence treatment and performance. There are a number of imaging techniques available for evaluating lower limb osseous and soft-tissue injuries, and choice can be limited by local availability and radiologist preference. The radiologists’ role in assessing injury is to grade the severity and extent of injury so appropriate treatment can be implemented.
In acute osseous injuries, radiographs are usually sufficient to confirm or exclude immediate severe injury. In acute and overuse injuries of the leg and calf, several imaging modalities play a role in depicting findings, with US and MR imaging being the most frequently utilised.
Each of the modalities has both strengths and weaknesses and the utility of each will depend upon the particular clinical scenario and the question which needs to be answered. Ultimately more than one imaging modality may be needed in conjunction with clinical examination in order to best assess overuse injuries of the leg and calf.
Things to Remember
-
1.
The lower limb is essential for all athletic movements and is the most commonly injured area for all sporting activities.
-
2.
Radiographs are the first-line imaging investigation for evaluating acute osseous injury but MR imaging is a sensitive technique for acute complications and overuse injuries.
-
3.
MR imaging and ultrasound are both accurate techniques for assessing acute and chronic soft-tissue injuries as well as subsequent complications.
-
(a)
Ultrasound provides a rapid and dynamic assessment.
-
(b)
MR imaging is sensitive for very-low-grade injuries and also maintains its field of view in athletes with large muscle bulk or diffuse symptoms.
-
(a)
7 Boxes
Box 1: Acute Osseous Injury
-
Radiographs—sufficient in majority of cases.
-
CT—to define complex fracture patterns prior to treatment.
-
MRI—for suspected radiographically occult injuries.
Box 2: Chronic Osseous Stress
-
MRI most useful for defining the severity of cortical and bone marrow changes.
-
Radiographs—usually negative but performed initially.
-
CT—can be helpful in ruling out a cortical fracture.
-
Isotope bone scanning—sensitive but lacks spatial resolution compared to MRI.
Box 3: Acute Lower Limb Muscle Injury
-
Ultrasound—accurate, fast and dynamic. Particularly useful in differentiating large grade 2 from grade 3 injuries. Can be negative in very-low-grade injury.
-
MRI—accurate and useful in athletes with large muscle bulk or diffuse symptoms.
Box 4: Complications of Muscle Injury
-
Ultrasound—particularly useful in diagnosing early myositis ossificans, muscle hernias and adherence of scar tissue.
-
MRI—particularly useful in defining subtle atrophic changes.
References
Anderson MW, Ugalde V, Batt M, Gacayan J (1997) Shin splints: MR appearance in a preliminary study. Radiology 204:177–180
Armstrong RB (1984) Mechanisms of exercise-induced delayed onset muscular soreness: a brief review. Med Sci Sports Exerc 16:529–538
Aspelin P, Ekberg O, Thorsson O, Wilhelmsson M, Westlin N (1992) Ultrasound examination of soft tissue injury of the lower limb in athletes. Am J Sports Med 20:601–603
Atilla S, Ilgit ET, Akpek S, Yucel C, Tali ET, Isik S (1998) MR imaging and MR angiography in popliteal artery entrapment syndrome. Eur Radiol 8:1025–1029
Balius R, Rodas G, Pedret C, Capdevila L, Alomar X, Bong DA (2014) Soleus muscle injury: sensitivity of ultrasound patterns. Skelet Radiol 43:805–812
Batt ME, Ugalde V, Anderson MW, Shelton DK (1998) A prospective controlled study of diagnostic imaging for acute shin splints. Med Sci Sports Exerc 30:1564–1571
Bianchi S, Abdelwahab IF, Mazzola CG, Ricci G, Damiani S (1995) Sonographic examination of muscle herniation. J Ultrasound Med 14:357–360
Bianchi S, Martinoli C, Abdelwahab IF, Derchi LE, Damiani S (1998) Sonographic evaluation of tears of the gastrocnemius medial head (“tennis leg”). J Ultrasound Med 17:157–162
Boden BP, Lohnes JH, Nunley JA, Garrett WE Jr (1999) Tibia and fibula fractures in soccer players. Knee Surg Sports Traumatol Arthrosc 7:262–266
Bodley R, Jamous A, Short D (1993) Ultrasound in the early diagnosis of heterotopic ossification in patients with spinal injuries. Paraplegia 31:500–506
Bonasia DE, Rosso F, Cottino U, Rossi R (2015) Exercise-induced leg pain. Asia Pac J Sports Med Arthrosc Rehabil Technol 2:73–84
Chang WR, Kapasi Z, Daisley S, Leach WJ (2007) Tibial shaft fractures in football players. J Orthop Surg Res 2:11
Chernoff DM, Walker AT, Khorasani R, Polak JF, Jolesz FA (1995) Asymptomatic functional popliteal artery entrapment: demonstration at MR imaging. Radiology 195:176–180
Chhabra A, Faridian-Aragh N, Chalian M, Soldatos T, Thawait SK, Williams EH, Andreisek G (2012) High-resolution 3-T MR neurography of peroneal neuropathy. Skelet Radiol 41:257–271
Chomiak J, Junge A, Peterson L, Dvorak J (2000) Severe injuries in football players. Influencing factors. Am J Sports Med 28:S58–S68
Collins PS, Mcdonald PT, Lim RC (1989) Popliteal artery entrapment: an evolving syndrome. J Vasc Surg 10:484–489; discussion 489–90.
Connell DA, Schneider-Kolsky ME, Hoving JL, Malara F, Buchbinder R, Koulouris G, Burke F, Bass C (2004) Longitudinal study comparing sonographic and MRI assessments of acute and healing hamstring injuries. AJR Am J Roentgenol 183:975–984
Cross TM, Gibbs N, Houang MT, Cameron M (2004) Acute quadriceps muscle strains: magnetic resonance imaging features and prognosis. Am J Sports Med 32:710–719
De Smet AA, Best TM (2000) MR imaging of the distribution and location of acute hamstring injuries in athletes. AJR Am J Roentgenol 174:393–399
De Smet AA, Norris MA, Fisher DR (1992) Magnetic resonance imaging of myositis ossificans: analysis of seven cases. Skelet Radiol 21:503–507
Delgado GJ, Chung CB, Lektrakul N, Azocar P, Botte MJ, Coria D, Bosch E, Resnick D (2002) Tennis leg: clinical US study of 141 patients and anatomic investigation of four cadavers with MR imaging and US. Radiology 224:112–119
Draghi F, Zacchino M, Canepari M, Nucci P, Alessandrino F (2013) Muscle injuries: ultrasound evaluation in the acute phase. J Ultrasound 16:209–214
Dvorak J, Junge A (2000) Football injuries and physical symptoms. A review of the literature. Am J Sports Med 28:S3–S9
Edwards PH Jr, Wright ML, Hartman JF (2005) A practical approach for the differential diagnosis of chronic leg pain in the athlete. Am J Sports Med 33:1241–1249
Ekstrand J, Hagglund M, Walden M (2011) Injury incidence and injury patterns in professional football: the Uefa injury study. Br J Sports Med 45:553–558
Elias DA, White LM, Rubenstein JD, Christakis M, Merchant N (2003) Clinical evaluation and MR imaging features of popliteal artery entrapment and cystic adventitial disease. AJR Am J Roentgenol 180:627–632
Flores DV, Mejia Gomez C, Estrada-Castrillon M, Smitaman E, Pathria MN (2018) MR imaging of muscle trauma: anatomy, biomechanics, pathophysiology, and imaging appearance. Radiographics 38:124–148
Fornage BD (2000) The case for ultrasound of muscles and tendons. Semin Musculoskelet Radiol 4:375–391
Fredericson M, Bergman AG, Hoffman KL, Dillingham MS (1995) Tibial stress reaction in runners. Correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med 23:472–481
Fuller CW, Smith GL, Junge A, Dvorak J (2004) The influence of tackle parameters on the propensity for injury in international football. Am J Sports Med 32:43S–53S
Gaeta M, Minutoli F, Scribano E, Ascenti G, Vinci S, Bruschetta D, Magaudda L, Blandino A (2005) CT and MR imaging findings in athletes with early tibial stress injuries: comparison with bone scintigraphy findings and emphasis on cortical abnormalities. Radiology 235:553–561
Gaeta M, Minutoli F, Mazziotti S, Visalli C, Vinci S, Gaeta F, Blandino A (2008) Diagnostic imaging in athletes with chronic lower leg pain. AJR Am J Roentgenol 191:1412–1419
Garrett WE Jr (1988) Injuries to the muscle-tendon unit. Instr Course Lect 37:275–282
Garrett WE Jr (1990) Muscle strain injuries: clinical and basic aspects. Med Sci Sports Exerc 22:436–443
Garrett WE Jr, Califf JC, Bassett FH 3rd (1984) Histochemical correlates of hamstring injuries. Am J Sports Med 12:98–103
Garrett WE Jr, Safran MR, Seaber AV, Glisson RR, Ribbeck BM (1987) Biomechanical comparison of stimulated and nonstimulated skeletal muscle pulled to failure. Am J Sports Med 15:448–454
Giza E, Fuller C, Junge A, Dvorak J (2003) Mechanisms of foot and ankle injuries in soccer. Am J Sports Med 31:550–554
Green NE, Rogers RA, Lipscomb AB (1985) Nonunions of stress fractures of the tibia. Am J Sports Med 13:171–176
Guermazi A, Roemer FW, Robinson P, Tol JL, Regatte RR, Crema MD (2017) Imaging of muscle injuries in sports medicine: sports imaging series. Radiology 285:1063
Hagglund M, Walden M, Ekstrand J (2013) Risk factors for lower extremity muscle injury in professional soccer: the UEFA injury study. Am J Sports Med 41:327–335
Hai Z, Guangrui S, Yuan Z, Zhuodong X, Cheng L, Jingmin L, Yun S (2008) CT angiography and MRI in patients with popliteal artery entrapment syndrome. AJR Am J Roentgenol 191:1760–1766
Harwin JR, Richardson ML (2017) “Tennis leg”: gastrocnemius injury is a far more common cause than plantaris rupture. Radiol Case Rep 12:120–123
Hawkins RD, Hulse MA, Wilkinson C, Hodson A, Gibson M (2001) The association football medical research programme: an audit of injuries in professional football. Br J Sports Med 35:43–47
Helms CA, Fritz RC, Garvin GJ (1995) Plantaris muscle injury: evaluation with MR imaging. Radiology 195:201–203
Ilahi OA, Younas SA, Labbe MR, Edson SB (2003) Prevalence of ganglion cysts originating from the proximal tibiofibular joint: a magnetic resonance imaging study. Arthroscopy 19:150–153
Jackson DW, Feagin JA (1973) Quadriceps contusions in young athletes. Relation of severity of injury to treatment and prognosis. J Bone Joint Surg Am 55:95–105
Jarraya M, Hayashi D, Roemer FW, Crema MD, Diaz L, Conlin J, Marra MD, Jomaah N, Guermazi A (2013) Radiographically occult and subtle fractures: a pictorial review. Radiol Res Pract 2013:370169
Jarvinen TA, Jarvinen TL, Kaariainen M, Kalimo H, Jarvinen M (2005) Muscle injuries: biology and treatment. Am J Sports Med 33:745–764
Karantanas AH (2021) Natural history and monitoring of fractures and microfractures. Med Radiol https://doi.org/10.1007/174_2020_271
Kassarjian A, Rodrigo RM, Santisteban JM (2014) Intramuscular degloving injuries to the rectus femoris: findings at MRI. AJR Am J Roentgenol 202:W475–W480
Kaufman KR, Brodine S, Shaffer R (2000) Military training-related injuries: surveillance, research, and prevention. Am J Prev Med 18:54–63
Khaladkar SM, Kondapavuluri SK, Kamal A, Kalra R, Kamal V (2016) Detection of myofascial herniation on dynamic sonography and magnetic resonance imaging. Case Rep Radiol 2016:4245189
Labmayr V, Aliabadi A, Tiesenhausen K, Brodmann M, Schmid F, Moore D (2019) Popliteal artery entrapment syndrome (PAES) in a 17-year-old adolescent. Case Rep Vasc Med 2019:8540631
Lacout A, Jarraya M, Marcy PY, Thariat J, Carlier RY (2012) Myositis ossificans imaging: keys to successful diagnosis. Indian J Radiol Imaging 22:35–39
Lees A, Nolan L (1998) The biomechanics of soccer: a review. J Sports Sci 16:211–234
Lefere M, Demeyere A, Vanhoenacker F (2021) Overuse bone trauma and stress fractures. Med Radiol https://doi.org/10.1007/174_2020_240
Marcantonio DR, Cho GJ (2000) Focus on muscle in orthopedic MRI. Semin Musculoskelet Radiol 4:421–434
Martens MA, Backaert M, Vermaut G, Mulier JC (1984) Chronic leg pain in athletes due to a recurrent compartment syndrome. Am J Sports Med 12:148–151
Mclean K, Popovic S (2017) Morel-Lavallee lesion: AIRP best cases in radiologic-pathologic correlation. Radiographics 37:190–196
Milgrom C, Chisin R, Giladi M, Stein M, Kashtan H, Margulies J, Atlan H (1984) Negative bone scans in impending tibial stress fractures. A report of three cases. Am J Sports Med 12:488–491
Mink JH (1992) Muscle injuries. In: Deutsch A, Mink JH, Kerr R (eds) MRI of the foot and ankle, 1st edn. Raven Press, New York
Miskovsky S, Kaeding C, Weis L (2004) Proximal tibiofibular joint ganglion cysts: excision, recurrence, and joint arthrodesis. Am J Sports Med 32:1022–1028
Naffaa L, Moukaddam H, Samim M, Lemieux A, Smitaman E (2017) Semimembranosus muscle herniation: a rare case with emphasis on muscle biomechanics. Skelet Radiol 46:373–378
Newham DJ, Mills KR, Quigley BM, Edwards RH (1983) Pain and fatigue after concentric and eccentric muscle contractions. Clin Sci (Lond) 64:55–62
Nicholas J, Hershman E (1986) The lower extremity and spine in sports medicine. Mosby, St Louis
Nicolaou S, Liang T, Murphy DT, Korzan JR, Ouellette H, Munk P (2012) Dual-energy CT: a promising new technique for assessment of the musculoskeletal system. AJR Am J Roentgenol 199:S78–S86
Noonan TJ, Garrett WE Jr (1999) Muscle strain injury: diagnosis and treatment. J Am Acad Orthop Surg 7:262–269
Nordin M, Frankel VH (2001a) Biomechanics of bone. In: Nordin M, Frankel VH (eds) Basic biomechanics of the musculoskeletal system, 3rd edn. Lippincott Williams and Wilkins, Philadelphia
Nordin M, Frankel VH (2001b) Biomechanics of skeletal muscle. In: Nordin M, Frankel VH (eds) Basic biomechanics of the musculoskeletal system, 3rd edn. Lippincott Williams and Wilkins, Philadelphia
Novacheck TF (1998) The biomechanics of running. Gait Posture 7:77–95
Ohta-Fukushima M, Mutoh Y, Takasugi S, Iwata H, Ishii S (2002) Characteristics of stress fractures in young athletes under 20 years. J Sports Med Phys Fitness 42:198–206
Peck RJ, Metreweli C (1988) Early myositis ossificans: a new echographic sign. Clin Radiol 39:586–588
Peterson L, Renstrom P (1986) Sports injuries. Year Book Medical, Chicago
Pollock N, James SL, Lee JC, Chakraverty R (2014) British athletics muscle injury classification: a new grading system. Br J Sports Med 48:1347–1351
Pollock N, Patel A, Chakraverty J, Suokas A, James SL, Chakraverty R (2016) Time to return to full training is delayed and recurrence rate is higher in intratendinous (‘c’) acute hamstring injury in elite track and field athletes: clinical application of the British Athletics Muscle Injury Classification. Br J Sports Med 50:305–310
Purohit NB, King LJ (2015) Ultrasound of lower limb sports injuries. Ultrasound 23:149–157
Rich NM, Collins GJ Jr, Mcdonald PT, Kozloff L, Clagett GP, Collins JT (1979) Popliteal vascular entrapment. Its increasing interest. Arch Surg 114:1377–1384
Ringler MD, Litwiller DV, Felmlee JP, Shahid KR, Finnoff JT, Carter RE, Amrami KK (2013) Mri accurately detects chronic exertional compartment syndrome: a validation study. Skelet Radiol 42:385–392
Robertson GA, Wood AM (2017) Femoral neck stress fractures in sport: a current concepts review. Sports Med Int Open 1:E58–E68
Robinson P (2004) Ultrasound of muscle injury. In: Mcnally E (ed) Practical musculoskeletal ultrasound. Churchill Livingston, London
Robinson P, Farrant JM, Bourke G, Merchant W, Mckie S, Horgan KJ (2008) Ultrasound and MRI findings in appendicular and truncal fat necrosis. Skelet Radiol 37:217–224
Rubin DA (2012) Imaging diagnosis and prognostication of hamstring injuries. AJR Am J Roentgenol 199:525–533
Sammarco GJ, Hockenbury RT (2001) Biomechanics of the foot and ankle. In: Nordin M, Frankel VH (eds) Basic biomechanics of the musculoskeletal system, 3rd edn. Lipponcott Williams and Wilkins, Philadelphia
Shellock FG, Fukunaga T, Mink JH, Edgerton VR (1991) Exertional muscle injury: evaluation of concentric versus eccentric actions with serial MR imaging. Radiology 179:659–664
Shirkhoda A, Armin AR, Bis KG, Makris J, Irwin RB, Shetty AN (1995) MR imaging of myositis ossificans: variable patterns at different stages. J Magn Reson Imaging 5:287–292
Slavotinek JP, Stilger VG, Fon GT (2000) Hamstring injuries in footballers: the prevalence and prognostic value of MRI findings. Radiology 217:191
Speer KP, Lohnes J, Garrett WE Jr (1993) Radiographic imaging of muscle strain injury. Am J Sports Med 21:89–95; discussion 96.
Spinner RJ, Atkinson JL, Harper CM Jr, Wenger DE (2000) Recurrent intraneural ganglion cyst of the tibial nerve. Case report. J Neurosurg 92:334–337
Stauber W (1988) Eccentric action of muscles: physiology, injury, and adaption. In: Stauber W (ed) Exercise and sports sciences reviews. Franklin Institute, Philadelphia
Steinbach L, Fleckenstein J, Mink J (1998) MR imaging of muscle injuries. Semin Musculoskelet Radiol 1:128–141
Taylor DC, Dalton JD Jr, Seaber AV, Garrett WE Jr (1993) Experimental muscle strain injury. Early functional and structural deficits and the increased risk for reinjury. Am J Sports Med 21:190–194
Toorop R, Poniewierski J, Gielen J, Maes M, Van Schil P, D’archambeau O (2004) Popliteal artery entrapment syndrome. Jbr-Btr 87:154–155
Tucker AK (2010) Chronic exertional compartment syndrome of the leg. Curr Rev Musculoskelet Med 3:32–37
Van Den Bergh FR, Vanhoenacker FM, De Smet E, Huysse W, Verstraete KL (2013) Peroneal nerve: normal anatomy and pathologic findings on routine MRI of the knee. Insights Imaging 4:287–299
Van Holsbeeck M, Introcasco J (2001) Musculoskeletal ultrasound. St Louis, Miss, Mosby
Yablon CM, Hammer MR, Morag Y, Brandon CJ, Fessell DP, Jacobson JA (2016) US of the peripheral nerves of the lower extremity: a landmark approach. Radiographics 36:464–478
Yates B, White S (2004) The incidence and risk factors in the development of medial tibial stress syndrome among naval recruits. Am J Sports Med 32:772–780
Zabetakis P (1986) Muscle soreness and rhabdomyolysis. In: Nicholas J, Hershman E (eds) The lower extremity and spine in sports medicine. Mosby, St Louis
Zarins B, Ciullo JV (1983) Acute muscle and tendon injuries in athletes. Clin Sports Med 2:167–182
Acknowledgments
The author would like to thank Drs. P. Bearcroft, A.J. Grainger and P.J. O’Connor for contributing images to this chapter.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Attard, V., Rowbotham, E., Robinson, P. (2021). Acute and Overuse Lesions of the Leg and Calf. In: Vanhoenacker, F.M., Maas, M., Gielen, J.L. (eds) Imaging of Orthopedic Sports Injuries. Medical Radiology(). Springer, Cham. https://doi.org/10.1007/174_2020_268
Download citation
DOI: https://doi.org/10.1007/174_2020_268
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-75361-0
Online ISBN: 978-3-030-75362-7
eBook Packages: MedicineMedicine (R0)