
Abstract
Neck nodal metastases are common in head and neck cancer and influence prognosis profoundly. This chapter focuses on the commonest cancer type, squamous cell carcinoma, although other malignancies are also outlined. CT, MRI and US are the mainstay imaging modalities for routine nodal evaluation and are reliant on anatomic criteria, which are described in this chapter. 18F-FDG PET/CT provides functional information by virtue of tumour hypermetabolism although its role in staging is not established. Neck nodal distribution and nodal staging using the current levels-based and TNM systems respectively are described. Besides N stage, other nodal features demonstrable on imaging, including extracapsular spread and precise location, can influence therapy and prognosis. Anatomic imaging is particularly challenging in the post-treatment neck, especially for assessment of residual nodal cancer following chemoradiation. In this regard, 18F-FDG PET/CT may have some advantages; currently there is great interest in the development of other functional techniques such as diffusion-weighted MRI.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Head and neck cancers commonly metastasize to cervical nodes. The frequency of nodal metastases from head and neck squamous cell carcinoma (HNSCC) is approximately 50% although this is variable, being dependent on factors such as the primary tumour site and stage. Nodal metastases cause morbidity and mortality by invading vital structures in the neck and by increasing the risk of more distant tumour spread. Nodal status is a very important prognostic indicator in HNSCC as metastatic cervical nodes reduce patient survival by 30–50% (Layland et al. 2005; Tankere et al. 2000) and multiple nodes, extranodal spread and lower cervical metastases are additional adverse prognostic factors. The treatment options of surgery and/or (chemo) radiotherapy are influenced by nodal status. Given the importance of nodal disease on patient outcomes, prompt detection of nodal metastases at initial presentation and after treatment is essential to prevent their rapid progression to more advanced and unsalvageable disease. Clinical palpation, although a valuable skill, is inaccurate for nodal detection and characterisation (Merritt et al. 1997; Johnson 1990) and therefore imaging has an essential role at every step of the patient pathway from initial diagnosis through to post therapeutic surveillance.
This chapter will review the normal nodal distribution and lymphatic drainage pathways in the head and neck region and the imaging features that are employed for distinguishing metastatic nodes from benign nodes using both anatomical and functional imaging criteria. Nodal staging and imaging strategies with respect to clinical and subclinical nodal disease, as well as prediction of therapeutic response and post therapeutic evaluation, are outlined. Emphasis throughout this chapter is on HNSCC although other head and neck carcinomas as well as lymphoma will be discussed briefly.
2 Nodal Group Classification and Pathways of Lymphatic Drainage
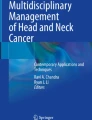
Early classifications of cervical nodal distribution were purely anatomical in that individual nodes or nodal groups were named according to the structures they were in close proximity to, such as submandibular nodes, jugulodigastric nodes, etc. While this classification remains useful today for describing specific nodes, over the years a levels-based system has emerged with the objectives of being simple, reproducible and relevant in the era of selective surgical and radiotherapy treatments as well as cross-sectional imaging. In this system, the majority of cervical nodes are assigned to one of six levels (I–VI) whose boundaries are readily identifiable on imaging. A further seventh level (VII) is sometimes used also which refers to nodes in the superior mediastinum (Som et al. 1999). Several neck nodal groups are located outside these levels and are still referred to anatomically such as the retropharyngeal, facial, parotid and periparotid, occipital and peri auricular nodal groups. A more detailed account of the levels-based system can be found in “Clinical and Endoscopic Examination of the Head and Neck” and by reference to the article by Som et al. (1999), but a brief summary is shown in Fig. 1 and illustrated by axial MRI images (Figs. 2a–f and 3a, b).

Schematic illustration of the imaging-based level system of nodal distribution in the right side of the neck. Solid lines indicate boundaries of levels and dotted lines indicate level subdivisions. Facial, parotid, post auricular, occipital, retropharyngeal and superficial external jugular nodes (latter two groups are not shown) reside outside these levels and referred to by anatomical names. Level VII nodes are in the superior mediastinum (not shown). (d anterior belly of the digastric muscle, ca carotid artery (common and internal), cr cricoid cartilage, hy hyoid bone, ijv internal jugular vein, smg submandibular gland, scm sternocleidomastoid muscle)

Distribution of cervical nodes using the imaging-based level system on axial T1 W post contrast MRI. (CCA common carotid artery, ICA internal carotid artery, IJV internal jugular vein, scm; sternocleidomastoid muscle) a Level IA (submental); nodes below the mylohyoid muscle, between the anterior bellies of the digastric muscles and hyoid bone. b Level IB (submandibular); nodes lateral to the anterior belly of digastric muscle and anterior to the posterior margin of the submandibular gland (the latter is denoted by a dashed line). Level II (upper internal jugular); nodes around the upper internal jugular vein. The lower limit is the inferior margin of the body of the hyoid bone. IIA nodes are anterior, medial or lateral, or posterior but inseparable from the vein. c Level IIA and Level IIB (upper internal jugular); nodes posterior to the upper internal jugular vein are IIA if inseparable from the vein and IIB if separable from the vein. d Level III (Mid jugular); nodes around the mid-internal jugular vein between the inferior margin of the body of the hyoid bone and inferior margin of the cricoid cartilage, lateral to the common carotid artery and anterior to the posterior margin of the sternocleidomastoid muscle. Level VA (upper posterior triangle); nodes posterior to posterior margin of the sternocleidomastoid muscle, anterior to the trapezius muscle and above the lower border of the cricoid cartilage (dashed line denotes the boundary between level III and VA). e Level IV (lower internal jugular); nodes around the lower internal jugular vein between the level of the cricoid cartilage and clavicle, lateral to the common carotid artery, and anterior to a line extending from the posterior margin of the sternocleidomastoid muscle to the posterolateral margin of the scalenus anterior muscle (denoted by a dashed line).Level VB (lower posterior triangle) nodes lie posterior to this line, anterior to the trapezius muscle and inferior to the cricoid cartilage. f Level VI (central compartment or visceral); nodes medial to the carotid arteries and extending between the hyoid bone and the manubrium. These include nodes along the thyroid gland, prelaryngeal and paratracheal nodes

Additional nodes not covered by the level-based system (Facial, post auricular and occipital nodes as well as level VII (superior mediastinal) nodes are not shown) (ICA internal carotid artery, IJV internal jugular vein). a Retropharyngeal nodes, medial to the internal carotid artery and posterolateral to the pharynx. b Parotid and periparotid nodes
Lymphatic drainage in the head and neck tends to be site-specific and follow predictable pathways down the neck. The first draining node or nodal basin for a given site is termed the first echelon or sentinel node(s) and subsequent nodal basins are termed the second and third echelons, etc. The typical lymphatic drainage for different primary cancer sites in the head and neck is listed in Table 1. Awareness of this lymphatic drainage has relevance for nodal staging, treatment planning and to search for occult primary cancers. Midline structures such as the tongue, or sites with a particularly enriched lymphatic network, such as the pyriform sinus, frequently drain bilaterally. Furthermore, lymphatic drainage can vary between individuals and can be disrupted by previous infections, neck surgery and radiotherapy.
3 Imaging Modalities
This section will provide a brief overview of the main modalities used for neck node evaluation, as well as of some of the newer functional imaging techniques which are presently in the domain of clinical research. Computed tomography (CT), magnetic resonance imaging (MRI), ultrasound (US) and (18)F-fluorodeoxyglucose positron emission tomography (FDG-PET) are the four main imaging modalities in routine clinical use for assessment of cervical nodal metastases. There is considerable variation in the reported accuracies of these modalities, which is unsurprising given the heterogeneity of study designs in terms of patient selection, imaging protocols, radiological diagnostic criteria and histopathological evaluation (Castelijns and van den Brekel 2002; van den Brekel et al. 1996). However, the choice of imaging technique is influenced also by other factors, which include the optimum modality for evaluating the primary site, available resources and radiological expertise. The limitations of conventional imaging for lymph node assessment have provided the impetus for research into new functional imaging techniques. These include techniques such as sentinel node lymphoscintigraphy and techniques that can be added to MRI such as diffusion-weighted imaging (DWI), proton magnetic resonance spectroscopy (MRS), dynamic contrast-enhanced MRI (DCE-MRI) and ultrasmall superparamagnetic iron oxide (USPIO) MRI, or added to CT such as dynamic contrast-enhanced CT. Some of these new techniques will be briefly mentioned at the end of this section.
3.1 CT and MRI
CT or MRI is the most widely used modality which reflects the fact that these modalities have acceptable and comparable accuracies for nodal malignancy, and because these can simultaneously assess the primary tumour and the neck nodes. A detailed account of the relative merits of CT and MRI is beyond the scope of this chapter although in general, MRI is excellent for soft tissue characterisation and does not involve ionising radiation, whereas CT is quicker to perform hence less susceptible to motion artifacts which make it especially suitable for dyspnoeic or claustrophobic patients. In practice whatever modality is used to stage the primary tumour is used also to stage the neck. Both modalities require intravenous contrast medium administration for optimum nodal characterisation.
3.2 US and US-Guided Fine-Needle Aspiration Cytology
US is the most practically useful imaging modality for cervical lymph nodes, although it is unsuitable in some deeply seated nodal groups such as those in the retropharyngeal space. US is quick, inexpensive, well tolerated, does not require intravenous contrast media and can display specific imaging features of discriminatory value more readily than CT or MRI, such as the nodal hilum and vascularity. A further major benefit of US is that it can be used to guide fine-needle aspiration for cytology (US-FNAC), which with sufficient experience can be performed successfully in nodes as small as 4 mm in diameter. The superiority of US-FNAC compared to US alone has been shown in several studies (Atula et al. 1997; Stuckensen et al. 2000; de Bondt et al. 2007). For example, one study documented 93% accuracy for US-FNAC compared to US alone (75%), CT (78%) and MRI (82%) (van den Brekel et al. 1993). Errors on US-FNAC are usually caused by sampling errors or cytological misinterpretation leading to false negative results. Because of its high accuracy, US-FNAC is well suited for investigating equivocal nodal findings in head and neck cancer patients, especially with the aim of distinguishing between patients with a N0 and a N+ neck, as this distinction has a major impact on clinical management. It is also performed in patients presenting with unexplained neck lymphadenopathy or suspected thyroid cancer where US is the initial imaging technique for assessing the primary site.
3.3 FDG-PET Imaging
Most head and neck cancers, including primary tumours as well as metastatic nodes, have increased glycolytic activity that can be detected using (18)F-fluorodeoxyglucose-PET (FDG-PET) imaging. Studies indicate that FDG-PET is superior to anatomic imaging techniques for the detection of nodal metastases in HNSCC (Schoder and Yeung 2004; Adams et al. 1998; Ng et al. 2006). However, FDG-PET is limited by its poorer spatial resolution and lack of anatomic detail. Combined PET/CT overcomes these limitations by permitting direct co-registration of functional and anatomic data, which translates into a higher accuracy for tissue characterisation than either PET or CT alone (Syed et al. 2005; Schwartz et al. 2005). In a recent study comparing imaging modalities for preoperative staging in HNSCC, FDG-PET/CT detected nodal metastases with 93% accuracy on a level-by-level basis, compared to 86% for patients evaluated by either CT or MRI (Roh et al. 2007). However, false negative and positive results occur using FDG-PET/CT thus, at present, there is no general consensus that using FDG-PET/CT for routine staging significantly improves clinical management (Ng et al. 2006; Hyde et al. 2003; Brouwer et al. 2004; Krabbe et al. 2008)
3.4 Diffusion-Weighted Imaging
DWI is the most developed of all the new functional MRI techniques. It evaluates free water motion (diffusion), which is quantified using apparent diffusion coefficients (ADCs) calculated from rate of signal loss on DWI images acquired with increasing diffusion encoding gradients (b-factors). DWI is non-invasive, relatively quick and can be performed with a large field of view to feasibly image most nodal groups in the neck. Nodal metastases show restricted diffusion and hence lower ADC values compared to normal nodes (Abdel Razek et al. 2006; de Bondt et al. 2009a; Holzapfel et al. 2009; Vandecaveye et al. 2009). However, to date there are few studies comparing DWI with conventional imaging, although one such study has shown that, for nodes between 4 and 9 mm, DWI achieved appreciably higher sensitivity than conventional turbo spin-echo MRI (76% vs. 7%) while specificity was only slightly lower (94% vs. 99.5%) (Vandecaveye et al. 2009).
3.5 Magnetic Resonance Spectroscopy
Proton (1H) MRS measures tissue metabolites, which may then be used for tissue characterisation. Most research to date has focused on two metabolites, choline (Cho) and creatine (Cr), that can be detected in many tissues as spectral peaks at 3.22 and 3.03 ppm. Preliminary studies in HNSCC document higher Cho/Cr ratios in both primary tumour and metastatic nodes compared to normal muscle (Mukherji et al. 1997; Bisdas et al. 2007; King et al. 2004a), and in metastatic nodes compared to reactive nodes (Bisdas et al. 2007). Furthermore, MRS has been shown to be of utility for differentiating cervical lymphadenopathies (King et al. 2005). Nevertheless, at present, MRS has important technical limitations that hamper a role in nodal staging. These include constraints on the minimum voxel size (~1 cm3), contamination by surrounding tissues, and prolonged acquisition times which make MRS both susceptible to motion artifacts and unfeasible for assessing the entire neck.
3.6 Dynamic Contrast-Enhanced (DCE) MRI
DCE-MRI uses low molecular weight paramagnetic contrast agents such as gadolinium to assess the microvasculature and extravascular extracellular space of nodal cancers. In the head and neck region rapid serial imaging is performed using T1 W gradient recalled echo sequences as the intravenous contrast passes through the node, and the resultant data are analysed using time-intensity plots or pharmacokinetic models. Early work suggests that there may be a difference in the contrast enhancement of metastatic and normal nodes, with the former showing a delayed and lower peak enhancement, and slower washout phase (Fischbein et al. 2003).
3.7 Lymphoscintigraphy for Sentinel Node Localisation
Lymphoscintigraphy can be used for sentinel node localisation. It is already an established technique in malignant melanoma and breast cancer and currently is under investigation in HNSCC. Sentinel node imaging typically entails injecting Tc-99 m radiolabelled colloid into tissues around the primary tumour and mapping the subsequent lymphatic drainage including first echelon nodes using preoperative planar scintigraphy or single photon emission computed tomography (SPECT) as well as intraoperative hand held gamma detectors. The localised sentinel node is subsequently excised and examined for cancer, which is used to predict whether there is likely cancer in downstream nodes. In recent years, there has been significant interest in the role of sentinel node biopsy (SNB) for staging the clinical N0 neck in HNSCC. Accumulating evidence from pilot studies of SNB in oral/oropharyngeal HNSCC suggest this technique can achieve over 90% sensitivity and specificity for predicting overall neck nodal status. On the basis of these results, the risk of occult metastases after a negative SNB may be under 5%, hence SNB in these patients could eliminate the need for prophylactic neck dissections (Alvarez Amezaga et al. 2007; Alkureishi et al. 2010). The indications for SNB have still to be established. In this regard it may be unsuitable for floor of mouth tumours due their close proximity to the lymphatic basin which hinders sentinel nodal detection (Alkureishi et al. 2010). As a modification of the sentinel node technique, pilot studies have evaluated using US-guided FNAC instead of excision biopsy for radiolocalised sentinel nodes in N0 HNSCC (Nieuwenhuis et al. 2000, 2002; Hoft et al. 2002). However, the results thus far have been discouraging as this approach achieves poor sensitivities for predicting a positive nodal status and offers no practical diagnostic gains compared to conventional US-FNAC (Nieuwenhuis et al. 2000; van den Brekel et al. 1991).
4 Imaging Criteria for Malignant Nodes
The main imaging modalities used for initial nodal evaluation, namely CT, MRI and US, utilise anatomic criteria to differentiate malignant from benign nodes, although some centres supplement this with functional data from FDG-PET. Imaging features more suggestive of normal or reactive nodes include small size, oval shape, presence of central hilum, hilar vascularity, homogeneous cortex (Figs. 4, 5, 6) and minimal FDG uptake. By comparison, imaging features suggestive of metastatic nodes include nodal enlargement, rounded shape, absent hilum, peripheral or other non hilar vascularity, heterogeneous parenchyma which includes necrosis or cystic change, border irregularity suggestive of extracapsular tumour spread (ECS) (Figs. 4, 5, 6) and avid FDG uptake. Each criterion is discussed in more detail below.

a Grey scale US of a normal lymph node (long arrow) showing the peripheral cortex (long arrow) central echogenic hilum (short arrow) with hilar vascularity. b Grey scale US (top) with corresponding grey scale and power Doppler US (below) of a metastatic node from SCC. The node shows enlargement, long:short axis ratio <2, absent hilum, absent hilar vascularity and a peripheral disorganised vascular pattern

a Axial CT post contrast showing normal jugulodigastric lymph nodes bilaterally (long arrows). The hilum, when seen, appears as a focal depression of the parenchyma (short arrows). A nodal vessel is seen emerging from the nodal hilum on the right (arrowhead). b Axial CT pre and post contrast (left and right) in a patient with HNSCC showing enlarged rounded right level IIA metastatic nodes. The more anterior node (short arrow) appears solid, whereas the posterior node (long arrow) is necrotic

a Axial T1 W MRI showing normal bilateral submandibular lymph nodes (arrows) with identifiable hila (arrowheads). b Axial T1 W post contrast MRI (left) and T2 W fat saturated MRI (right) showing metastatic left level IIA nodes (arrows) from nasopharyngeal carcinoma. The posterior node (short arrow) appears solid, whereas the anterior node (long arrow) is necrotic and has an ill-defined border suggestive of early extracapsular spread
4.1 Size
Normal cervical lymph nodes range in size from a few millimeters to just over 2.5 cm in longitudinal diameter (Figs. 4, 5, 6). Nodal size declines with age and varies according to location. Nodes in the upper internal jugular chain, notably the jugulodigastric region, are usually the largest due to mild hyperplasia as a result of chronic exposure to repeated infections in the oral cavity and pharynx, while nodes towards the skull base and thoracic inlet tend to be smaller.
Nodal enlargement is an important feature of malignant infiltration although no threshold of nodal size is both highly sensitive and highly specific, which reflects the fact that moderately enlarged nodes in the neck are frequently reactive while small tumour deposits may not alter nodal dimensions. Over the years, numerous studies have investigated optimal size cut-offs for nodal metastases in HNSCC. One of the most influential is a CT-based study by van den Brekel et al. that documented short axis diameter thresholds of 11 mm for level II and 10 mm elsewhere as the most accurate overall, achieving 82% sensitivity and specificity. In addition, these thresholds could be lowered to 8–10 mm for groups of 3 or more nodes draining a primary tumour (van den Brekel et al. 1990). These criteria are still widely used today, albeit with minor modifications such as a lower threshold of 5 mm short axis diameter for retropharyngeal nodes (King et al. 2000).
Nevertheless, it should be highlighted that optimum size criteria are arbitrary and may be altered depending on whether a higher sensitivity or higher specificity is desired. One early study documented that lowering the short axis diameter cut-off from 15 to 5 mm increased the sensitivity of CT from 56 to 98% but lowered the specificity from 84 to 13% (Curtin et al. 1998). In addition, the patient population may influence optimum thresholds. Van den Brekel et al. performed another study of size criteria in HNSCC, this time using US, and found that thresholds achieving the highest global accuracy were 9 mm for level II and 8 mm for other levels (74% sensitivity and 78% specificity), whereas for a subgroup of patients without palpable nodes, optimal thresholds were lower, namely 7 mm for level II and 6 mm for other levels (80% sensitivity and 59% specificity) (van den Brekel et al. 1998a).
4.2 Shape
Normal or reactive nodes tend to be oval or reniform in shape and have a ratio of the longitudinal to transverse axis diameter (L/T) >2, while nodal metastases are more rounded resulting in a lower L/T ratio (Figs. 4, 5, 6). In clinical practice, a L/T ratio <2 is widely adopted as a criterion of malignancy. In one large study, nodal shape achieved 95% accuracy although it should be noted that the majority of these nodes were >1 cm (Steinkamp et al. 1995). Furthermore, normal nodes in the submandibular and parotid regions tend to be more rounded. The presence of eccentric cortical widening has been described in malignant nodes including in the neck (Vassallo et al. 1992), although this feature may also occasionally be found in normal or reactive nodes, especially those in the submandibular region.
4.3 Hilum
Lymph nodes contain a hilum composed of arteries, veins, lymphatics and sometimes fat (Figs. 4, 5, 6). This is visualised optimally by US due to the presence of numerous reflective interfaces within the lymphatic sinuses. Using grey scale US, the hilum appears as an echogenic linear structure traversing into the centre of the node, and is detected in ~66% and >90% of normal nodes <5 and >5 mm, respectively (Ying et al. 2001). Conventional CT and MRI are generally less capable of depicting hila, although with careful attention a hilum is often identifiable, especially when there is fatty metaplasia. Loss of the nodal hilum can occur in malignant nodes due to direct invasion or compression by tumour. The reported sensitivity of this feature on conventional US varies widely between 44 and 95% (Vassallo et al. 1992; Ahuja et al. 2001a; Ahuja and Ying 2002; Ying et al. 1998). False negative results using this criterion are not surprising given that the majority of microscopic tumour deposits are located within the subcapsular sinuses, as afferent lymphatic channels enter the nodes peripherally (van den Brekel et al. 1996).
4.4 Vascular Pattern
The vascular architecture within lymph nodes can be assessed using power Doppler US, which in normal nodes typically extends into the hilum and branches outwards into the parenchyma (Figs. 4, 7). This hilar vascular pattern is more florid in reactive nodes. In contrast, metastatic nodes tend to display disorganised vascular patterns including peripheral cortical or subcortical vascularity, and focal areas of displaced or absent vascularity, with or without preservation of the hilar pattern (Ariji et al. 1998; Na et al. 1997a; Wu et al. 1998). Published studies using vascularity to differentiate metastatic from reactive nodes have reported sensitivities of 83–89% and specificities of 87–98% (Ariji et al. 1998; Wu et al. 1998). While vascular patterns are important, they are not always demonstrable in normal nodes, especially in those under 5 mm (Ying et al. 2001). Furthermore, abnormal vascular patterns are non-specific as they may occur in non-malignant lymphadenopathies (Ahuja et al. 2001b). Quantitative indices of vascular resistance including the resistive index (RI) and pulsatility index (PI) can be measured in intranodal vessels using spectral Doppler US. Several studies have shown that metastatic nodes have higher RI and PI than benign nodes (Na et al. 1997a; Wu et al. 1998; Ahuja et al. 2001b; Steinkamp et al. 1994; Dragoni et al. 1999). Measuring these indices is highly operator dependent and so currently there is no consensus on the optimal cut-offs for malignancy.

Grey scale US with power Doppler showing a prominent reactive submandibular lymph node with florid hilar vascularity (arrows)
4.5 Parenchymal Heterogeneity and Necrosis
Normal parenchyma in the nodal cortex appears relatively uniform on conventional imaging whereas parenchymal heterogeneity is usually pathological (Figs. 4, 5, 6). Moreover, in the context of known HNSCC, nodal heterogeneity is specific for metastasis. These heterogeneous areas may be composed of variable amounts of solid tumour, deposits of keratin and necrotic tumour, which may or may not be cystic. Intranodal necrosis in HNSCC correlates with nodal size as it reflects tumour growth beyond its blood supply, and is identified in 56–63% of metastatic nodes >1.5 cm compared to 10–33% of nodes <1 cm (Friedman et al. 1993; Don et al. 1995). CT, MRI and US can all depict necrosis >3 mm in size; the accuracies of MRI and CT for detecting necrosis are similar (91–92%) and higher than that of US (84%) (King et al. 2004b). The lower accuracy of US may be explained partly by the fact that necrosis sometimes can appear isoechoic to normal nodal parenchyma. Metastatic nodes can be almost entirely cystic and thus may cause initial diagnostic confusion with benign cystic lesions, namely branchial cleft cysts, especially if solitary and located along the mid to upper jugular chain. Nevertheless, the precise location, appearance and different clinical presentations of head and neck cancers and benign cysts can usually discriminate these conditions. Metastatic nodal calcification is rare at presentation in HNSCC (Eisenkraft and Som 1999; Gormly and Glastonbury 2004) and the presence of calcification should raise the suspicion of nodal metastases from thyroid cancer. Nodal calcification may also be found in benign pathologies, especially granulomatous diseases, as well as other untreated and treated malignancies such as adenocarcinoma and lymphoma (Eisenkraft and Som 1999).
4.6 Border Irregularity
In the absence of infection or previous treatment, loss of the normally smooth nodal border is highly suspicious for ECS (Figs. 6 , 8, 9 ). The risk of ECS increases with nodal size, being present in approximately 50 and 75% of nodal metastases with a diameter of 2–3 cm and >3 cm, respectively (Snow et al. 1982; Collins 1987). In addition, ECS is reported to occur in 23% of metastatic nodes <1 cm, which accounts for 30% of all nodal ECS (Don et al. 1995; Collins 1987). ECS has major prognostic significance, which is discussed in a later section. The reported sensitivity and specificity of CT for ECS is 62–81% and 60–90% (Carvalho et al. 1991; Steinkamp et al. 1999; Xu et al. 1998; Souter et al. 2009) and of MRI is 74 and 72% (Steinkamp et al. 2002). Several early studies reported that MRI was inferior to CT for detecting ECS, although more recent studies indicate comparable accuracies (King et al. 2004c). Moreover, another MRI study documented that the presence of border irregularity on T2 W fat suppressed sequences achieved up to 87% sensitivity and 94% specificity for metastases, and encouragingly the accuracy remained high for nodes <10 mm in short axis diameter (up to 78% sensitivity and 97% specificity) (de Bondt et al. 2009b). Nevertheless, imaging detection of ECS is subjective and dependent on radiologists experience as it may be subtle or mistaken for perinodal inflammatory changes (Souter et al. 2009; Steinkamp et al. 2002; de Bondt et al. 2009b). It is noteworthy that metastatic nodes may appear paradoxically to have sharper, well-demarcated margins than benign nodes on grey scale US because of their reduced echogenicity, as this increases their conspicuity against the echogenic surrounding tissue (Shozushima et al. 1990).

Axial T1 W post contrast MRI in a patient with HNSCC showing metastatic left mid-upper internal jugular lymphadenopathy with gross extracapsular spread (small arrows). The enhancing nodal borders are ill defined and extend into the surrounding deep cervical fascia as well as invade the left sternocleidomastoid muscle and paravertebral muscles, both of which show abnormal enhancement. Tumour also contacts the left internal carotid artery and internal jugular vein. (ICA; internal carotid artery, IJV; internal jugular vein, scm; sternocleidomastoid muscle)

Axial CT post contrast showing a heterogeneous right level II nodal mass with gross extracapsular spread. There is complete encasement of the right internal carotid artery (ICA), which is narrowed, as well as frank invasion of muscles and overlying skin (short arrows)
4.7 FDG-PET Uptake
On FDG-PET, tissue FDG uptake can be assessed semi-quantitatively using standardised uptake values (SUVs). In normal nodes there is typically no or minimally increased SUV relative to background activity in the surrounding cervical tissue. By comparison, metastatic nodes typically show elevated SUVs, and the higher the SUV, the more likely a node is malignant. Despite these generalisations, at present there is no consensus in the literature regarding an appropriate SUV cut-off for malignancy, which partly reflects the overlap between uptake in benign and malignant nodes. False negative FDG-PET results are usually due to intrinsic low metabolic activity in small tumour deposits, and for this reason the utility of FDG-PET in patients with no palpable nodal disease is debated (Ng et al. 2006; Brouwer et al. 2004; Krabbe et al. 2008). Identification of metastatic nodes may be hampered also by low FDG uptake in markedly necrotic nodes, and when a node lies in close proximity to the primary tumour, as nodal uptake may be obscured by intense uptake at the primary site (King et al. 2008). False positive FDG-PET results can occur due to hypermetabolism in reactive nodes as well as other benign lymphadenopathies, recent biopsy and infection.
4.8 Functional MRI
On DWI, metastatic nodes show restricted diffusion and a low ADC (Fig. 10). Regions of necrosis, which are common in HSNCC, should be excluded from the ADC measurement as these reduce the discriminatory performance of DWI by increasing the ADC. In a recent study comparing SCC with benign nodes, DWI achieved 84% sensitivity and 94% specificity for metastases in nodes measuring >4 mm in short axis diameter (Vandecaveye et al. 2009). However, at present the optimum thresholds for discrimination of metastatic from benign nodes have still to be confirmed. On MRS, metastatic nodes have high Cho/Cr ratios (Fig. 11) but again optimum discriminatory thresholds have not been established.

Axial DWI-MRI diffusion image at b1000 (left) with corresponding ADC map (right) in a patient with HNSCC. Metastatic right level II nodes (short arrows) and a left level II nodal mass (long arrow) have a mean ADC of 0.94 and 1.04 × 10−3 mm2/s respectively. These values are comparatively low, signifying restricted diffusion, which is compatible with malignant infiltration

Proton MRS of a metastatic periparotid node from HNSCC. a) Axial T1W post contrast MRI showing MRS voxel placement (red box). b) The corresponding MRS spectrum shows an elevated Cho peak and a high Cho/Cr ratio of 5.64, which is suggestive of malignancy. Lipid peaks are also demonstrated
5 Micrometastases
It should be noted that cancerous deposits may be microscopic, for instance comprising small clusters of cells, hence it is not feasible nor realistic to expect any of the current imaging modalities to detect these. Radiologically, the term micrometastases generally refers to tumour deposits <3 mm, which are not detected reliably by present day imaging techniques. These have been found in 25% of neck dissection specimens from patients with no clinicoradiological evidence of nodal disease (clinical N0) (van den Brekel et al. 1996). While micrometastases usually occur alongside larger deposits, in 10–25% of clinical N0 but pathologically positive neck dissection specimens, they are the sole manifestation of nodal malignancy (van den Brekel et al. 1992, 1996). Their exact clinical significance is unclear some of these could progress to clinically apparent disease if left untreated.
6 Nodal Staging
Nodal staging of metastases from HNSCC is incorporated into the TNM system, which currently uses the 7th editions of the AJCC and UICC guidelines (Sobin et al. 2009; Edge et al. 2010). Staging evaluates nodal number (single or multiple), site (unilateral, contralateral or bilateral) and greatest dimension (using 3 and 6 cm thresholds). Of note, while diagnosis of a metastatic node entails measurement of the minimum axial diameter, staging entails measurement of the maximum diameter. In general, a single ipsilateral node ≤3 cm indicates N1 disease, any node >6 cm indicates N3; any other combination indicates N2 disease. N2 is further subdivided into N2a (single node >3 cm), N2b (multiple ipsilateral nodes) and N2c (bilateral or contralateral nodes). Nodal staging in HNSCC, nasopharyngeal carcinoma and thyroid cancer are summarised in Table 2. In HNSCC, the presence of metastatic nodes denotes a moderate or advanced overall stage III or IV.
7 Impact of Nodal Imaging on Patient Management
7.1 Detection of Metastatic Nodes
To understand the impact of imaging for identifying or excluding metastatic nodes, it is worth outlining the treatment strategies for the neck with (N+) and without (N0) clinicoradiological evidence of nodal metastases.
N+ neck: In patients with any evidence of metastatic neck nodal disease, definitive surgical treatment usually entails a radical or modified radical neck dissection on the involved side(s). Both of these operations remove all lymph nodes within levels I–V operated(s), while these differ only in terms of whether extra-lymphatic structures (spinal accessory nerve, sternocleidomastoid muscle, internal jugular vein) are also removed (Robbins et al. 2002). In recent years several workers have advocated the use of a selective neck dissection (SND), which preserves at least one of the neck levels I–V to treat early node positive disease (localised, small volume nodes that lack ECS) (Andersen et al. 2002; Schmitz et al. 2009; Traynor et al. 1996) while minimising surgical morbidity. Radiotherapy fields usually encompass both sides of the neck although current radiotherapy regimes, which include intensity modulated radiotherapy (IMRT), deliver higher doses to positive nodes and lower doses to normal appearing nodal groups, especially those that lie close to important structures such as the parotid glands, oesphagus and spinal cord.
N0 neck: Depending on the primary site, up to 40% of necks in HNSCC with no palpable or radiological nodal metastases harbour occult nodal metastases (van den Brekel et al. 1996). Clinical management of these patients varies between a “watchful waiting” policy and elective treatment using radiotherapy or neck dissection. One surgical approach in the N0 neck is to perform a prophylactic unilateral SND on the same side as the primary tumour in order to diagnose and remove potential sites of occult metastases, and occasionally bilateral SNDs when the tumour is located in the midline. However, the optimal management of this subgroup is controversial in terms of how to balance the increased risk of unsalvageable recurrences that would occur under a “watchful waiting” policy in the minority of patients who have disease against the morbidity of prophylactic neck treatments in the majority of patients who do not have disease. To address this dilemma, many clinicians choose to surgically treat the neck electively if the risk of occult nodal metastases in the individual exceeds 20% (Weiss et al. 1994; Pfister et al. 2000; Pillsbury and Clark 1997). Patients with early T stage tumours in the glottis, parotid gland and paranasal sinuses have a low risk of nodal metastasis (<10%), hence the neck is usually managed by watchful waiting. Conversely, patients with tumours that have an advanced T-stage, are deeply invading (e.g. >4 mm in oral tongue cancers), have a high grade or are at high-risk sites (including the oropharynx, hypopharynx and supraglottis) usually undergo prophylactic neck treatment by surgery or radiotherapy (Shear et al. 1976; Martinez-Gimeno et al. 1995).
Based on the treatment stratifications described above, nodal imaging has the most impact on patient management in the following situations:
-
1.
Distinguishing between patients with an N0 and an N+ neck. In this situation, finding even one single metastatic node in an otherwise normal neck could change management from a conservative “watchful waiting” policy to surgery/radiotherapy, or change the surgical approach from a limited to a more extensive neck dissection. Conversely, proving that a single indeterminate node is reactive rather than metastatic could have the opposite effect on management.
-
2.
Identification of metastatic nodes outside the usual surgical and radiotherapy treatment fields including the contralateral neck, retropharyngeal, parotid, suboccipital, buccal, facial and level VI nodes; nodes adjacent to sites which may be preferentially spared during radiotherapy, such as the salivary glands. In these situations, the radiotherapy or surgical fields may need to be extended or the modality of treatment changed from one to the other.
To this end, US-FNAC is an invaluable ancillary investigation for any accessible lymph nodes with equivocal malignant features on imaging that will alter treatment (Dirix et al. 2006; Bussels et al. 2006).
7.2 Extracapsular Tumour Spread
Extracapsular tumour invasion of adjacent structures should be carefully documented as this may affect nodal resectability (Table 2) (Figs. 6, 8, 9). Tumour invasion of the internal or common carotid artery usually precludes neck dissection as the initial treatment due to the high risk of severe surgical morbidity combined with the risks of generally poor prognosis of these patients due to advanced disease (Freeman 2005). Unfortunately, imaging has a limited accuracy for detecting carotid invasion although, as a general rule, tumour directly contacting the vessel under 180° and over 270° of the vessel circumference indicates that vascular invasion is probably absent and present, respectively (Steinkamp et al. 1999; Yousem et al. 1995; Yoo et al. 2000). In addition, some workers have documented that tumour fixation to the artery may be detected by palpation during US (Gritzmann et al. 1990; Mann et al. 1994).
Invasion of the prevertebral muscle or fascia tends to indicate unresectable disease to be within muscle. The presence of an intact fat plane between the tumour and the prevertebral fascia on imaging usually indicates that the fascia has not been breached, but the loss of this fat plane does not necessarily indicate that invasion is present.
Fortunately, tumoural invasion of the external carotid artery or its branches does not preclude surgery because these vessels can be sacrificed due to the rich collateral arterial supply in the head and neck region from the contralateral side. Similarly, the sternocleidomastoid muscle, internal jugular vein and skin can all be sacrificed if there is suspected involvement of these structures on imaging.
7.3 Identification of Patients at High Risk for Distant Metastases
Several nodal features at diagnosis are associated with a higher risk of developing distant metastases, including size >6 cm, >3 nodes involved, ECS and nodes in the lower neck/supraclavicular fossa (Alvi and Johnson 1997; de Bree et al. 2000; Leemans et al. 1993). These criteria may be used to decide whether further imaging, such as FDG-PET, is required to search for distant metastases centres recommend further imaging studies such as whole body PET-CT (Brouwer et al. 2006; Senft A et al. 2008).
8 Treatment Assessment
8.1 Prediction of Treatment Response to (Chemo)radiotherapy
There is currently great interest in identifying imaging markers with prognostic significance for (chemo)radiotherapy response which can be obtained either before treatment or early in a course of treatment, as these may facilitate better therapeutic stratification including dose escalations or cessation of (chemo)radiotherapy in favour of early conversion to surgery. Besides those markers already incorporated into the TNM staging (maximum nodal size, multiplicity and laterality), ECS is probably the most important as it indicates biologically aggressive disease as evidenced by increased risk of locoregional failure, distant metastases and reduced survival by as much as 50% (Myers et al. 2001; Larsen et al. 2009). At present most of the research regarding ECS is based on histology rather than imaging data. In the current edition of the TNM staging (Edge et al. 2010), ECS does not alter N stage per se although has been added as a descriptor (E+ or E– for clinical/radiologic evidence).
The prognostic significance of intranodal necrosis detected on imaging is unclear. A few studies using CT have documented that appreciable pre-treatment nodal necrosis is an independent risk factor for regional failure to (chemo)radiotherapy (Grabenbauer et al. 1998; Munck et al. 1991; Wang et al. 1996), which may be explained by the fact that tumour radiosensitivity is impaired by tissue hypoxia. Nevertheless, in clinical practice it is common for markedly necrotic nodes to demonstrate a complete response to (chemo)radiotherapy.
Several markers from functional imaging techniques obtained before treatment or early in the course of treatment show promise for prognostication. Early results suggest that local control is more likely to occur in nodes with higher vascularity as shown by a higher K trans on DCE-MRI (Kim et al. 2010). Nodes with a lower pre-treatment ADC and a higher early treatment rise in ADC on DWI (Fig. 12) (Kim et al. 2009; Vandecaveye et al. 2010) are also more likely to show tumour control. Using FDG-PET, primary tumours with a lower SUV are more likely to show an overall response in the neck (Schwartz et al. 2003; Wong et al. 2002). Furthermore, high pretreatment FDG uptake in nodal metastasis in HNSCC may be a risk factor for distant recurrence (Kubicek et al. 2010).

Axial DWI-MRI ADC map (left) and T1 W post contrast MRI in a patient with a left tonsillar SCC and metastatic IIA node pretreatment (upper row) and 2 weeks intra treatment with concomitant chemoradiotherapy (lower row). The ADC of the node increased from 1.1 × 10−3 mm2/s pretreatment to 1.5 × 10−3 mm2/s at 2 weeks intra treatment. This indicates increased diffusion, which favours a treatment response. There has been no locoregional recurrence as of 3 years post treatment
8.2 Post Treatment Assessment
The majority of nodal metastases in HNSCC respond completely to (chemo)radiotherapy; in a minority of patients residual tumour persists, which may progress to surgically unsalvageable disease. Historically, regional control rates for early nodal disease treated surgically or by radiotherapy were broadly equivalent, whereas for advanced nodal disease, control rates from radiotherapy alone were poor and suboptimal compared to radiotherapy followed by a planned neck dissection. For this reason, it was common practice to perform a neck dissection in this cohort, irrespective of whether or not there was evidence of a complete clinic-radiological response to radiotherapy. While this aggressive strategy reduced the risk of regional failures, this produced unnecessary surgical morbidity as up to two thirds of planned neck dissections were pathologically negative (Ojiri et al. 2002). Fortunately, with the development of more efficacious chemoradiotherapeutic regimens, there has been a shift towards a more conservative approach in terms of only performing neck dissection after (chemo)radiotherapy if there is clinical evidence of residual disease. This shift in practice places an even greater burden on imaging modalities to distinguish patients with post treatment regional failure who will require early salvage surgery, from patients with regional control, who can be placed under close imaging surveillance instead.
MRI and CT both have a high negative predictive value (94–97%) for residual nodal disease if the nodal metastases have essentially disappeared (Ojiri et al. 2002; Liauw et al. 2006; Yeung et al. 2008; Lin et al. 2007); under these circumstances patients may be spared surgery and undergo imaging surveillance instead. However, sterilised nodal metastases frequently regress incompletely, to leave behind a variable amount of scar tissue (Fig. 13). CT-based studies have documented residual nodes ≤1.5 cm with no focal abnormality (Liauw et al. 2006), or nodes with >90% reduction in size (Labadie et al. 2000) to be associated with tumour control. Larger residual masses or those containing a focal abnormality are non-specific as these may represent residual cancer or a benign mass of inflammatory tissue and fibrotic scarring. The documented positive predictive value of a post treatment mass is low, ranging between 36 and 59% (Ojiri et al. 2002; Liauw et al. 2006; Inohara et al. 2009). Ojiri et al. documented that 57% of hemi necks with nodes >15 mm were pathologically negative on neck dissection (Ojiri et al. 2002), and Yao et al. documented that post treatment nodes >50 mm could be disease-free (Yao et al. 2004). Difficulties in post treatment nodal assessment are partly due to the fact that anatomic abnormalities associated with malignancy can resolve very slowly after successful treatment, especially in nodes that were predominantly necrotic or had extracapsular invasion into adjacent muscles before treatment. The performance of US is similar to CT and MRI in that the disappearance of nodes usually indicates response (Furukawa and Furukawa 2010; Yusa et al. 2000), whereas residual masses are non-specific. It has been shown that sonographic features associated with malignancy, namely abnormal vascularity, altered echogenicity, absent hilum and border irregularity can persist in the benign post treatment mass (Yusa et al. 2000). Furthermore, while US guided biopsy can be performed in these cases, this is prone to sampling errors due to the fact that residual cancer may be small and dispersed within larger areas of inflammation and scarring.

Axial T1 W post contrast MRI showing right nodal metastases pretreatment (left) and 6 months post chemoradiotherapy (right). An enlarged right level II node (arrow) has reduced significantly in size following treatment although there is a small amount of residual soft tissue remaining. This was believed to represent a post treatment scar and there has been no regional recurrence as of 3 years post treatment
FDG-PET is now well established in the post treatment assessment of HNSCC (Fig. 14) and has become a part of routine imaging follow-up in some centres. The false positive and negative results from FDG-PET can be reduced by delaying the scan until at least several months after treatment. From the accumulating evidence which includes several review papers (Wong 2008; Isles et al. 2008; de Bree et al. 2009), the consensus appears to be that (1) FDG-PET/CT is more accurate than CT or MRI, (2) subjective assessment is often superior to SUV measurements, (3) FDG-PET/CT performed at least 10–12 weeks after treatment has a high negative predictive value (96%) although the positive predictive value is low (49%) (Isles et al. 2008).

Axial FDG-PET/CT at the oropharyngeal level in a patient with a right tonsillar SCC (short arrow) and a 1.8 cm metastatic right level II node (long arrow) before treatment (top row) and after completion of chemoradiation (bottom row). Pretreatment, both tumour sites show avid FDG uptake; tonsil SUVmax = 6.1, Level II node SUVmax = 4.3. Post treatment, neither site shows appreciable increased FDG uptake. The patient has had no recurrence as of 2 years post treatment. Mild physiological FDG uptake is present in lymphoid tissue in the tongue base (arrowheads)
Functional MRI and CT techniques can be easily incorporated into post treatment assessment and of these DWI appears to be the most promising. Successful treatment leads to cell death and a progressive rise in ADC so that benign post treatment residual masses have significantly higher ADCs than residual cancers, even as early as 3–6 weeks post treatment (de Bree et al. 2009; Vandecaveye et al. 2011). It is difficult to establish a universal ADC threshold for residual cancer due to differences in DWI protocols between institutions although several studies suggest a potential discriminatory cut-off ~1.3 × 10−3 mm2/s (Vandecaveye et al. 2010; Abdel Razek et al. 2007; King et al. 2010) or a less than 20% rise in ADC values when compared to the pre-treatment DWI (Vandecaveye et al. 2011). One precaution when evaluating DWI is to exclude areas of frank necrosis from the ADC measurement as these may undergo early fibrotic organisation, which lowers the ADC and thus can simulate residual cancer. Using proton MRS, the persistence of a Cho peak after treatment may be a marker for residual cancer (King et al. 2010). Finally, preliminary studies suggest that residual cancers have greater vascularity than benign post treatment masses on DCE-MRI (Hoskin et al. 1999), although an optimum DCE parameter and threshold has not been established.
8.3 Post Treatment Surveillance
Even after employing anatomical imaging, functional imaging and imaging-guided biopsy, it may not be possible to distinguish between a nodal mass caused by residual cancer and one caused by benign post treatment inflammation and scarring. Currently, there is a shift towards less surgical intervention, even in those patients with residual nodal masses post chemo(radiation). Furthermore, some relapses occur at the tumour margin or from occult metastases, and these tumour recurrences may not manifest until much later in the post treatment period. Consequently, there is no substitute for close clinical and imaging surveillance.
The first post treatment baseline MRI or CT examination following chemo(radiotherapy) or surgery is usually performed between 4 and 8 weeks after treatment (Liauw et al. 2006; Lell et al. 2000; Som et al. 1993), although in those patients with a low risk of residual disease this may be postponed to 4–6 months. Patients at a greater risk of locoregional relapse, including those with advanced disease treated by chemoradiotherapy, should undergo regular follow-up imaging. Most regional relapses/recurrences occur within the first 3 years of treatment, with the majority being diagnosed in the first 2 years. Imaging follow-up is therefore usually performed every 4–6 months for 2–3 years (Lell et al. 2000; Som et al. 1993), being more frequent in the earlier post treatment period. MRI or CT is the main technique for surveillance although some centres now include FDG-PET, either routinely as a post treatment baseline or more selectively for patients with a suspicious residual node on conventional imaging. US-FNAC also has a role in post treatment surveillance and has been specifically investigated for the early detection of occult nodal metastases in patients with an N0 neck (van den Brekel et al. 1999) who have undergone surgery at the primary site without an elective neck dissection. A watchful waiting strategy involving regular US follow-up, including every 8–10 weeks in the first year, has been shown to detect nodal recurrences early, thereby increasing the chances of performing salvage surgery (van den Brekel et al. 1999).
9 Brief Overview of Non-HNSCC Lymphadenopathies
9.1 Lymphoma
Cervical disease in Hodgkin’s (HL) and non-Hodgkin’s lymphomas (NHL) is described in “Neck Lymphoma”. Neck HL nearly always presents as nodal involvement. In general about 50% of NHL in the head and neck shows neck node involvement (Chisin and Weber 1994; King et al. 2004d; Hanna et al. 1997), the incidence being greater in diffuse large cell lymphomas than Natural Killer/T cell lymphomas. The size criteria for the diagnosis of lymphomatous nodes are not well established in comparison to those for carcinoma. In general cut-offs between 1 and 1.5 cm are used although multiple smaller nodes are also considered suspicious (Cheson et al. 1999). Lymphomatous nodes show a spectrum of morphological imaging appearances. At one end of the spectrum, lymphomatous nodes have similar features to nodal metastases from HNSCC, including a round shape, loss of the hilum and in NHL necrosis, matting and extra capsular spread sometimes may be present (King et al. 2004d; Saito et al. 2001; Wang et al. 1999). At the other end of the spectrum, lymphomatous nodes have similar features to normal or reactive nodes, namely an oval shape, preserved hilum and hilar vascularity which may be florid. The hilum is frequently identified, even in markedly enlarged rounded nodes, although it may be compressed and eccentrically displaced (Fig. 15). Calcification prior to therapy is rare and described mainly in mediastinal rather than cervical nodes (Apter et al. 2002). DWI is especially promising for lymphoma detection as involved nodes have much lower ADC than SCC (Abdel Razek et al. 2006; Sumi et al. 2003; King et al. 2007) as well as normal nodes (Kwee et al. 2010). FDG-PET also shows promise in detecting disease in normal sized lymph nodes, which could influence radiotherapy planning. Both HL and NHL are FDG avid, and aggressive lymphomas tend to have higher SUV values than indolent lymphomas (Hicks et al. 2005). FDG-PET or FDG-PET/CT has been shown to be comparable or superior to morphological imaging techniques as well as gallium67 scintigraphy for detecting nodal lymphoma. In centres where PET/CT is available, it is increasingly becoming the main imaging investigation for staging and therapeutic monitoring (Collins 2006).

Axial T1 W post contrast MRI showing a typical appearance of nodal lymphoma. There is gross lymphadenopathy with multiple enlarged rounded nodes, most of which appear solid although a right level II node demonstrates necrosis (arrow). Hila can be preserved even in grossly enlarged lymphomatous nodes (arrowheads)
9.2 Other Head and Neck Carcinomas
-
(1)
Thyroid carcinoma: Thyroid cancer commonly spreads to cervical lymph nodes (see “Thyroid and Parathyroid Neoplasms”). Papillary carcinoma is the most common thyroid cancer and it has the highest incidence of nodal metastases (30–90%), followed by medullary carcinoma (50%), anaplastic carcinoma (40%) and follicular carcinoma (10%). Medullary carcinoma has a greater propensity to spread bilaterally and to the mediastinum (Machens et al. 2002). See Table 1 for routes of nodal spread and Table 2 for nodal staging.
Ultrasound is the method of choice for imaging nodal metastases from thyroid cancer in the neck. In addition to the general features of metastatic nodes described for HNSCC, nodal metastases from papillary carcinoma may show micro- and macrocalcifications, increased echogenicity compared to muscle, and cystic change (Fig. 16) (Ahuja et al. 1995; Rosario et al. 2005). Calcifications may also be detected by CT, and cystic change may be seen by both CT and MRI; in the latter modality the cystic area may have a characteristic high T1 W signal intensity (Som et al. 1994; King 2008). The presence of unexplained nodes with calcification on CT or high T1-W signal cystic regions on MRI should prompt the search for a primary thyroid papillary carcinoma. Metastatic nodes in the central compartment tend to be small and more difficult to detect or characterise than those in the lateral compartment. Nonetheless, special effort should be made to try to evaluate these, especially those in the lower paratracheal/paraoesphageal regions, as failure to resect these may be responsible for so-called thyroid bed tumour recurrences. Nodal metastases from papillary carcinoma are frequently smaller than 5 mm, for which FNAC may be technically difficult to perform. Fortunately, detection of these small nodes is less of a concern for surgical planning because they can be treated successfully by radioactive iodine post operatively (Wang et al. 1999; Lell et al. 2000). Iodine scintigraphy is used following surgery to identify residual nodal metastases in the neck and nodal metastases in the mediastinum, but it will miss iodine negative nodes (this tendency is greater in the less well differentiated cancers). These iodine negative nodes may sometimes be detectable using (Hyde et al. 2003) F-FDG-PET/CT.
Fig. 16 
Grey scale US showing nodal metastases from thyroid papillary carcinoma. The nodes are hyperechoic, with one showing an anechoic cystic component (arrows)
-
(2)
Salivary gland carcinoma: The majority of nodal metastases from salivary malignancies arise from primaries in the submandibular gland (42%), followed by parotid gland (25%) and oral cavity (9%) (Terhaard et al. 2004; Lloyd et al. 2010). Similar halves overall survival, independent of T stage. The frequency of nodal metastases is related to the underlying histology, grade and T stage; in this respect many of the subtypes have a high risk whereas adenoid cystic carcinoma uncommonly involves lymph nodes (Ferlito et al. 2001). Routes of spread are shown in Table 1. Conventional imaging criteria for nodal metastases in salivary cancer are similar to those used for HNSCC. In general, salivary cancers are relatively radioresistant, hence documented nodal metastases are treated by neck dissection (Stennert et al. 2003). The incidence of occult nodal metastasis in salivary cancer ranges widely, between 12 and 48% (Stennert et al. 2003; Armstrong et al. 1992; Regis De Brito Santos et al. 2001; Rodriguez-Cuevas et al. 1995), and not surprisingly the optimal management of clinical N0 disease is debated (Stennert et al. 2003; Regis De Brito Santos et al. 2001; Frankenthaler et al. 1993; Medina 1998; Korkmaz et al. 2002). In practice, parotid and submandibular nodes are usually resected along with the primary tumour specimen, and these may undergo intraoperative frozen section histological analysis to determine whether to proceed to a comprehensive neck dissection.
-
(3)
Nasopharyngeal carcinoma: Nasopharyngeal carcinoma commonly spreads to regional nodes and cervical lymphadenopathy may be the presenting feature (see also “Neoplasms of the Nasopharynx”). Nodal staging differs from that of HNSCC (Table 2) but the imaging criteria for nodal metastases are similar to those used for HNSCC. Lateral retropharyngeal nodes are common in this disease and are best identified by MRI (Fig. 3a). Routes of nodal spread are shown in Table 1. The presence of metastatic nodes in the lower neck or supraclavicular fossa increases the risk of distant metastases. With respect to post RT surveillance, it is common for benign nodes that have been spared from the radiation field (submental, paratracheal and suprasternal nodes) to become chronically enlarged due to altered lymphatic drainage.
-
(4)
Skin cancer: Skin cancer of the head and neck involves the superficial nodal groups more commonly than in HNSCC (Table 1). The appearance of metastatic nodes from squamous cell carcinoma of the skin are similar to those of other HNSCC whereas nodal metastases from malignant melanoma tend to show less necrosis and extracapsular spread (van den Brekel et al. 1998b), and may have a high signal intensity on T1 W MR imaging due the paramagnetic effects of melanin. For malignant melanoma, the risk of developing nodal metastases is related to lesion thickness, with melanomas <1 mm thickness having a rate of nodal metastases of <5% while >4 mm thickness increases the risk to about 35% (McMasters and Swetter 2003).

9.3 Non-malignant Lymphadenopathy
Conventional imaging criteria using size, morphology or FDG uptake to identify metastatic lymphadenopathy are based on studies that predominantly compare metastatic nodes with normal and reactive lymph nodes. However, these same imaging criteria are much less accurate for differentiating metastatic nodes from other nodal pathologies. As a consequence, biopsy is almost invariably required for diagnosis. A detailed account of benign cervical lymphadenopathies is beyond the scope of this chapter although tuberculous lymphadenitis merits special attention as it is one of commonest causes of persistent cervical lymphadenopathy in the developing world as well as in parts of the developed world. Tuberculous nodes may be discrete, matted or form confluent masses (King et al. 1999) and may show calcification. Other imaging findings include nodal enlargement, necrosis, abscess formation, peri-adenitis and increased FDG uptake; all of these overlap with nodal metastases on imaging (Moon et al. 1997). Tuberculous nodes can also fistulate to the skin, which is highly suggestive of this diagnosis. Several non-infectious cervical lymphadenopathies may overlap with malignancy on imaging including Castleman’s disease (Fig. 17), sarcoidosis, Rosai-Dorfman disease and Kikuchi-Fujimoto disease (Koyama et al. 2004; La Barge et al. 2008; Fulcher 1993; Na et al. 1997b).

Axial CT post contrast showing an enlarged homogeneous left level II lymph node. This was diagnosed as Castleman's disease
10 Conclusion
Imaging of cervical nodal metastases has an important role in nodal detection, treatment planning and post treatment assessment. Imaging often requires a multimodality approach for the best results. A summary of the main points to be remembered when assessing nodal metastases are listed in Table 3.
References
Abdel Razek AA, Soliman NY, Elkhamary S, Alsharaway MK, Tawfik A (2006) Role of diffusion-weighted MR imaging in cervical lymphadenopathy. Eur Radiol 16:1468–1477
Abdel Razek AA, Kandeel AY, Soliman N et al (2007) Role of diffusion-weighted echo-planar MR imaging in differentiation of residual or recurrent head and neck tumors and posttreatment changes. Am J Neuroradiol 28:1146–1152
Adams S, Baum RP, Stuckensen T, Bitter K, Hor G (1998) Prospective comparison of 18F-FDG PET with conventional imaging modalities (CT, MRI, US) in lymph node staging of head and neck cancer. Eur J Nucl Med 25:1255–1260
Ahuja A, Ying M (2002) An overview of neck node sonography. Invest Radiol 37:333–342
Ahuja AT, Chow L, Chick W, King W, Metreweli C (1995) Metastatic cervical nodes in papillary carcinoma of the thyroid: ultrasound and histological correlation. Clin Radiol 50:229–231
Ahuja A, Ying M, King A, Yuen HY (2001a) Lymph node hilus: gray scale and power Doppler sonography of cervical nodes. J Ultrasound Med 20:987–992, quiz 94
Ahuja AT, Ying M, Ho SS, Metreweli C (2001b) Distribution of intranodal vessels in differentiating benign from metastatic neck nodes. Clin Radiol 56:197–201
Ahuja A, Ying M, Yuen YH, Metrewelli C (2001c) Power Doppler sonography to differentiate tuberculous cervical lymphadenopathy from nasopharyngeal carcinoma. AJNR 22:735–740
Alkureishi LW, Ross GL, Shoaib T et al (2010) Sentinel node biopsy in head and neck squamous cell cancer: 5-year follow-up of a European multicenter trial. Ann Surg Oncol 17:2459–2464
Alvarez Amezaga J, Barbier Herrero L, Pijoan del Barrio JI et al (2007) Diagnostic efficacy of sentinel node biopsy in oral squamous cell carcinoma. Cohort study and meta-analysis. Med Oral Patol Oral Cir Bucal 12E:235–243
Alvi A, Johnson JT (1997) Development of distant metastasis after treatment of advanced-stage head and neck cancer. Head Neck 19:500–505
Andersen PE, Warren F, Spiro J et al (2002) Results of selective neck dissection in management of the node-positive neck. Arch Otolaryngol Head Neck Surg 128:1180–1184
Apter S, Avigdor A, Gayer G, Portnoy O, Zissin R, Hertz M (2002) Calcification in lymphoma occurring before therapy: CT features and clinical correlation. Am J Roentgenol 178:935–938
Ariji Y, Kimura Y, Hayashi N et al (1998) Power Doppler sonography of cervical lymph nodes in patients with head and neck cancer. Am J Neuroradiol 19:303–307
Armstrong JG, Harrison LB, Thaler HT et al (1992) The indications for elective treatment of the neck in cancer of the major salivary glands. Cancer 69:615–619
Atula TS, Varpula MJ, Kurki TJ, Klemi PJ, Grenman R (1997) Assessment of cervical lymph node status in head and neck cancer patients: palpation, computed tomography and low field magnetic resonance imaging compared with ultrasound-guided fine-needle aspiration cytology. Eur J Radiol 25:152–161
Bisdas S, Baghi M, Huebner F et al (2007) In vivo proton MR spectroscopy of primary tumours, nodal and recurrent disease of the extracranial head and neck. Eur Radiol 17:251–257
Brouwer J, de Bree R, Comans EF, Castelijns JA, Hoekstra OS, Leemans CR (2004) Positron emission tomography using [18F]fluorodeoxyglucose (FDG-PET) in the clinically negative neck: is it likely to be superior? Eur Arch Otorhinolaryngol 261:479–483
Brouwer J, Senft A, de Bree R et al (2006) Screening for distant metastases in patients with head and neck cancer: is there a role for (18)FDG-PET? Oral Oncol 42:275–280
Bussels B, Hermans R, Reijnders A, Dirix P, Nuyts S, Van den Bogaert W (2006) Retropharyngeal nodes in squamous cell carcinoma of oropharynx: incidence, localization, and implications for target volume. Int J Radiat Oncol Biol Phys 65:733–738
Carvalho P, Baldwin D, Carter R, Parsons C (1991) Accuracy of CT in detecting squamous carcinoma metastases in cervical lymph nodes. Clin Radiol 44:79–81
Castelijns JA, van den Brekel MW (2002) Imaging of lymphadenopathy in the neck. Eur Radiol 12:727–738
Cheson BD, Horning SJ, Coiffier B et al (1999) Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J Clin Oncol 17:1244
Chisin R, Weber AL (1994) Imaging of lymphoma manifestations in the extracranial head and neck region. Leuk Lymphoma 12:177–189
Collins SL (1987) Controversies in the management of cancer of the neck. In: Thawley SE, Panje WR (eds) Comprehensive management of head and neck tumours. Saunders, Philadelphia, pp 1386–1443
Collins CD (2006) PET in lymphoma. Cancer Imaging 6S:63–70
Curtin HD, Ishwaran H, Mancuso AA, Dalley RW, Caudry DJ, McNeil BJ (1998) Comparison of CT and MR imaging in staging of neck metastases. Radiology 207:123–130
de Bondt RB, Nelemans PJ, Hofman PA et al (2007) Detection of lymph node metastases in head and neck cancer: a meta-analysis comparing US, USgFNAC, CT and MR imaging. Eur J Radiol 64:266–272
de Bondt RB, Hoeberigs MC, Nelemans PJ et al (2009a) Diagnostic accuracy and additional value of diffusion-weighted imaging for discrimination of malignant cervical lymph nodes in head and neck squamous cell carcinoma. Neuroradiology 51:183–192
de Bondt RB, Nelemans PJ, Bakers F et al (2009b) Morphological MRI criteria improve the detection of lymph node metastases in head and neck squamous cell carcinoma: multivariate logistic regression analysis of MRI features of cervical lymph nodes. Eur Radiol 19:626–633
de Bree R, Deurloo EE, Snow GB, Leemans CR (2000) Screening for distant metastases in patients with head and neck cancer. Laryngoscope 110:397–401
de Bree R, van der Putten L, Brouwer J, Castelijns JA, Hoekstra OS, Leemans CR (2009) Detection of locoregional recurrent head and neck cancer after (chemo)radiotherapy using modern imaging. Oral Oncol 45:386–393
Dirix P, Nuyts S, Bussels B, Hermans R, Van den Bogaert W (2006) Prognostic influence of retropharyngeal lymph node metastasis in squamous cell carcinoma of the oropharynx. Int J Radiat Oncol Biol Phys 65:739–744
Don DM, Anzai Y, Lufkin RB, Fu YS, Calcaterra TC (1995) Evaluation of cervical lymph node metastases in squamous cell carcinoma of the head and neck. Laryngoscope 105:669–674
Dragoni F, Cartoni C, Pescarmona E et al (1999) The role of high resolution pulsed and color Doppler ultrasound in the differential diagnosis of benign and malignant lymphadenopathy: results of multivariate analysis. Cancer 85:2485–2490
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A 3rd (2010) American joint committee on cancer, cancer staging manual, 7th edn. Springer, New York
Eisenkraft BL, Som PM (1999) The spectrum of benign and malignant etiologies of cervical node calcification. Am J Roentgenol 172:1433–1437
Ferlito A, Shaha AR, Rinaldo A, Mondin V (2001) Management of clinically negative cervical lymph nodes in patients with malignant neoplasms of the parotid gland. J Otorhinolaryngol Relat Spec 63:123–126
Fischbein NJ, Noworolski SM, Henry RG, Kaplan MJ, Dillon WP, Nelson SJ (2003) Assessment of metastatic cervical adenopathy using dynamic contrast-enhanced MR imaging. Am J Neuroradiol 24:301–311
Frankenthaler RA, Byers RM, Luna MA, Callender DL, Wolf P, Goepfert H (1993) Predicting occult lymph node metastasis in parotid cancer. Arch Otolaryngol Head Neck Surg 119:517–520
Freeman SB (2005) Advanced cervical metastasis involving the carotid artery. Curr Opin Otolaryngol Head Neck Surg 13:107–111
Friedman M, Roberts N, Kirshenbaum GL, Colombo J (1993) Nodal size of metastatic squamous cell carcinoma of the neck. Laryngoscope 103:854–856
Fulcher AS (1993) Cervical lymphadenopathy due to Kikuchi disease: US and CT appearance. J Comput Assist Tomogr 17:131–133
Furukawa MK, Furukawa M (2010) Diagnosis of lymph node metastases of head and neck cancer and evaluation of effects of chemoradiotherapy using ultrasonography. Int J Clin Oncol 15:23–32
Gormly K, Glastonbury CM (2004) Calcified nodal metastasis from squamous cell carcinoma of the head and neck. Australas Radiol 48:240–242
Grabenbauer GG, Steininger H, Meyer M et al (1998) Nodal CT density and total tumor volume as prognostic factors after radiation therapy of stage III/IV head and neck cancer. Radiother Oncol 47:175–183
Gritzmann N, Grasl MC, Helmer M, Steiner E (1990) Invasion of the carotid artery and jugular vein by lymph node metastases: detection with sonography. Am J Roentgenol 154:411–414
Hanna E, Wanamaker J, Adelstein D, Tubbs R, Lavertu P (1997) Extranodal lymphomas of the head and neck. A 20-year experience. Arch Otolaryngol Head Neck Surg 123:1318–1323
Hicks RJ, Mac Manus MP, Seymour JF (2005) Initial staging of lymphoma with positron emission tomography and computed tomography. Semin Nucl Med 35:165–175
Hoft S, Muhle C, Brenner W, Sprenger E, Maune S (2002) Fine-needle aspiration cytology of the sentinel lymph node in head and neck cancer. J Nucl Med 43:1585–1590
Holzapfel K, Duetsch S, Fauser C, Eiber M, Rummeny EJ, Gaa J (2009) Value of diffusion-weighted MR imaging in the differentiation between benign and malignant cervical lymph nodes. Eur J Radiol 72:381–387
Hoskin PJ, Saunders MI, Goodchild K, Powell ME, Taylor NJ, Baddeley H (1999) Dynamic contrast enhanced magnetic resonance scanning as a predictor of response to accelerated radiotherapy for advanced head and neck cancer. Br J Radiol 72:1093–1098
Hyde NC, Prvulovich E, Newman L, Waddington WA, Visvikis D, Ell P (2003) A new approach to pre-treatment assessment of the N0 neck in oral squamous cell carcinoma: the role of sentinel node biopsy and positron emission tomography. Oral Oncol 39:350–360
Inohara H, Enomoto K, Tomiyama Y et al (2009) The role of CT and (18)F-FDG PET in managing the neck in node-positive head and neck cancer after chemoradiotherapy. Acta Otolaryngol 129:893–899
Isles MG, McConkey C, Mehanna HM (2008) A systematic review and meta-analysis of the role of positron emission tomography in the follow up of head and neck squamous cell carcinoma following radiotherapy or chemoradiotherapy. Clin Otolaryngol 33:210–222
Johnson JT (1990) A surgeon looks at cervical lymph nodes. Radiology 175:607–610
Kim S, Loevner L, Quon H et al (2009) Diffusion-weighted magnetic resonance imaging for predicting and detecting early response to chemoradiation therapy of squamous cell carcinomas of the head and neck. Clin Cancer Res 15:986–994
Kim S, Loevner LA, Quon H et al (2010) Prediction of response to chemoradiation therapy in squamous cell carcinomas of the head and neck using dynamic contrast-enhanced MR imaging. Am J Neuroradiol 31:262–268
King AD (2008) Imaging for staging and management of thyroid cancer. Cancer Imaging 8:57–69
King AD, Ahuja AT, Metreweli C (1999) MRI of tuberculous cervical lymphadenopathy. J Comput Assist Tomogr 23:244–247
King AD, Ahuja AT, Leung SF et al (2000) Neck node metastases from nasopharyngeal carcinoma: MR imaging of patterns of disease. Head Neck 22:275–281
King AD, Yeung DK, Ahuja AT, Leung SF, Tse GM, van Hasselt AC (2004a) In vivo proton MR spectroscopy of primary and nodal nasopharyngeal carcinoma. Am J Neuroradiol 25:484–490
King AD, Tse GM, Ahuja AT et al (2004b) Necrosis in metastatic neck nodes: diagnostic accuracy of CT, MR imaging, and US. Radiology 230:720–726
King AD, Tse GM, Yuen EH et al (2004c) Comparison of CT and MR imaging for the detection of extranodal neoplastic spread in metastatic neck nodes. Eur J Radiol 52:264–270
King AD, Lei KI, Ahuja AT (2004d) MRI of neck nodes in non-Hodgkin’s lymphoma of the head and neck. Br J Radiol 77:111–115
King AD, Yeung DK, Ahuja AT et al (2005) Human cervical lymphadenopathy: evaluation with in vivo 1H-MRS at 1.5 T. Clin Radiol 60:592–598
King AD, Ahuja AT, Yeung DK et al (2007) Malignant cervical lymphadenopathy: diagnostic accuracy of diffusion-weighted MR imaging. Radiology 245:806–813
King AD, Ma BB, Yau YY et al (2008) The impact of 18F-FDG PET/CT on assessment of nasopharyngeal carcinoma at diagnosis. Br J Radiol 81:291–298
King AD, Yeung DK, Yu KH et al (2010) Pretreatment and early intratreatment prediction of clinicopathologic response of head and neck cancer to chemoradiotherapy using 1H-MRS. J Magn Reson Imaging 32:199–203
Korkmaz H, Yoo GH, Du W et al (2002) Predictors of nodal metastasis in salivary gland cancer. J Surg Oncol 80:186–189
Koyama T, Ueda H, Togashi K, Umeoka S, Kataoka M, Nagai S (2004) Radiologic manifestations of sarcoidosis in various organs. Radiographics 24:87–104
Krabbe CA, Dijkstra PU, Pruim J et al (2008) FDG PET in oral and oropharyngeal cancer. Value for confirmation of N0 neck and detection of occult metastases. Oral Oncol 44:31–36
Kubicek GJ, Champ C, Fogh S et al (2010) FDG-PET staging and importance of lymph node SUV in head and neck cancer. Head Neck Oncol 2:19
Kwee TC, Ludwig I, Uiterwaal CS et al (2010) ADC measurements in the evaluation of lymph nodes in patients with non-Hodgkin lymphoma: feasibility study. MAGMA 24:1–8
La Barge DV 3rd, Salzman KL, Harnsberger HR et al (2008) Sinus histiocytosis with massive lymphadenopathy (Rosai-Dorfman disease): imaging manifestations in the head and neck. Am J Roentgenol 191W:299–306
Labadie RF, Yarbrough WG, Weissler MC, Pillsbury HC, Mukherji SK (2000) Nodal volume reduction after concurrent chemo- and radiotherapy: correlation between initial CT and histopathologic findings. Am J Neuroradiol 21:310–314
Larsen SR, Johansen J, Sorensen JA, Krogdahl A (2009) The prognostic significance of histological features in oral squamous cell carcinoma. J Oral Pathol Med 38:657–662
Layland MK, Sessions DG, Lenox J (2005) The influence of lymph node metastasis in the treatment of squamous cell carcinoma of the oral cavity, oropharynx, larynx, and hypopharynx: N0 versus N+. Laryngoscope 115:629–639
Leemans CR, Tiwari R, Nauta JJ, van der Waal I, Snow GB (1993) Regional lymph node involvement and its significance in the development of distant metastases in head and neck carcinoma. Cancer 71:452–456
Lell M, Baum U, Greess H et al (2000) Head and neck tumors: imaging recurrent tumor and post-therapeutic changes with CT and MRI. Eur J Radiol 33:239–247
Liauw SL, Mancuso AA, Amdur RJ et al (2006) Postradiotherapy neck dissection for lymph node-positive head and neck cancer: the use of computed tomography to manage the neck. J Clin Oncol 24:1421–1427
Lin D, Glastonbury CM, Rafaelian O, Eisele DW, Wang SJ (2007) Management of advanced nodal disease following chemoradiation for head and neck squamous cell carcinoma: role of magnetic resonance imaging. J Otolaryngol 36:350–356
Lloyd S, Yu JB, Ross DA, Wilson LD, Decker RH (2010) A prognostic index for predicting lymph node metastasis in minor salivary gland cancer. Int J Radiat Oncol Biol Phys 76:169–175
Machens A, Hinze R, Thomusch O, Dralle H (2002) Pattern of nodal metastasis for primary and reoperative thyroid cancer. World J Surg 26:22–28
Mann WJ, Beck A, Schreiber J, Maurer J, Amedee RG, Gluckmann JL (1994) Ultrasonography for evaluation of the carotid artery in head and neck cancer. Laryngoscope 104:885–888
Martinez-Gimeno C, Rodriguez EM, Vila CN, Varela CL (1995) Squamous cell carcinoma of the oral cavity: a clinicopathologic scoring system for evaluating risk of cervical lymph node metastasis. Laryngoscope 105:728–733
McMasters KM, Swetter SM (2003) Current management of melanoma: benefits of surgical staging and adjuvant therapy. J Surg Oncol 82:209–216
Medina JE (1998) Neck dissection in the treatment of cancer of major salivary glands. Otolaryngol Clin North Am 31:815–822
Merritt RM, Williams MF, James TH, Porubsky ES (1997) Detection of cervical metastasis: a meta-analysis comparing computed tomography with physical examination. Arch Otolaryngol Head Neck Surg 123:149–152
Moon WK, Han MH, Chang KH et al (1997) CT and MR imaging of head and neck tuberculosis. Radiographics 17:391–402
Mukherji SK, Schiro S, Castillo M, Kwock L, Muller KE, Blackstock W (1997) Proton MR spectroscopy of squamous cell carcinoma of the extracranial head and neck: in vitro and in vivo studies. Am J Neuroradiol 18:1057–1072
Munck JN, Cvitkovic E, Piekarski JD et al (1991) Computed tomographic density of metastatic lymph nodes as a treatment-related prognostic factor in advanced head and neck cancer. J Natl Cancer Inst 83:569–575
Myers JN, Greenberg JS, Mo V, Roberts D (2001) Extracapsular spread A significant predictor of treatment failure in patients with squamous cell carcinoma of the tongue. Cancer 92:3030–3036
Na DG, Lim HK, Byun HS, Kim HD, Ko YH, Baek JH (1997a) Differential diagnosis of cervical lymphadenopathy: usefulness of color Doppler sonography. Am J Roentgenol 168:1311–1316
Na DG, Chung TS, Byun HS, Kim HD, Ko YH, Yoon JH (1997b) Kikuchi disease: CT and MR findings. Am J Neuroradiol 18:1729–1732
Ng SH, Yen TC, Chang JT et al (2006) Prospective study of [18F]fluorodeoxyglucose positron emission tomography and computed tomography and magnetic resonance imaging in oral cavity squamous cell carcinoma with palpably negative neck. J Clin Oncol 24:4371–4376
Nieuwenhuis EJ, Colnot DR, Pijpers HJ et al (2000) Lymphoscintigraphy and ultrasound-guided fine needle aspiration cytology of sentinel lymph nodes in head and neck cancer patients. Recent Results Cancer Res 157:206–217
Nieuwenhuis EJ, Castelijns JA, Pijpers R et al (2002) Wait-and-see policy for the N0 neck in early-stage oral and oropharyngeal squamous cell carcinoma using ultrasonography-guided cytology: is there a role for identification of the sentinel node? Head Neck 24:282–289
Ojiri H, Mendenhall WM, Stringer SP, Johnson PL, Mancuso AA (2002) Post-RT CT results as a predictive model for the necessity of planned post-RT neck dissection in patients with cervical metastatic disease from squamous cell carcinoma. Int J Radiat Oncol Biol Phys 52:420–428
Pfister DG, Ang K, Brockstein B et al (2000) NCCN practice guidelines for head and neck cancers. Oncology (Williston Park) 14:163–194
Pillsbury HC 3rd, Clark M (1997) A rationale for therapy of the N0 neck. Laryngoscope 107:1294–1315
Regis De Brito Santos I, Kowalski LP, Cavalcante De Araujo V, Flavia Logullo A, Magrin J (2001) Multivariate analysis of risk factors for neck metastases in surgically treated parotid carcinomas. Arch Otolaryngol Head Neck Surg 127:56–60
Robbins KT, Clayman G, Levine PA et al (2002) Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Arch Otolaryngol Head Neck Surg 128:751–758
Rodriguez-Cuevas S, Labastida S, Baena L, Gallegos F (1995) Risk of nodal metastases from malignant salivary gland tumors related to tumor size and grade of malignancy. Eur Arch Otorhinolaryngol 252:139–142
Roh JL, Yeo NK, Kim JS et al (2007) Utility of 2-[18F] fluoro-2-deoxy-d-glucose positron emission tomography and positron emission tomography/computed tomography imaging in the preoperative staging of head and neck squamous cell carcinoma. Oral Oncol 43:887–893
Rosario PW, de Faria S, Bicalho L et al (2005) Ultrasonographic differentiation between metastatic and benign lymph nodes in patients with papillary thyroid carcinoma. J Ultrasound Med 24:1385–1389
Saito A, Takashima S, Takayama F, Kawakami S, Momose M, Matsushita T (2001) Spontaneous extensive necrosis in non-Hodgkin lymphoma: prevalence and clinical significance. J Comput Assist Tomogr 25:482–486
Schmitz S, Machiels JP, Weynand B, Gregoire V, Hamoir M (2009) Results of selective neck dissection in the primary management of head and neck squamous cell carcinoma. Eur Arch Otorhinolaryngol 266:437–443
Schoder H, Yeung HW (2004) Positron emission imaging of head and neck cancer, including thyroid carcinoma. Semin Nucl Med 34:180–197
Schwartz DL, Rajendran J, Yueh B et al (2003) Staging of head and neck squamous cell cancer with extended-field FDG-PET. Arch Otolaryngol Head Neck Surg 129:1173–1178
Schwartz DL, Ford E, Rajendran J et al (2005) FDG-PET/CT imaging for preradiotherapy staging of head-and-neck squamous cell carcinoma. Int J Radiat Oncol Biol Phys 61:129–136
Senft A, de Bree R, Hoekstra OS (2008) Screening for distant metastases in head and neck cancer patients by chest CT or whole body FDG-PET: a prospective multicenter trial. Radiother Oncol 87:221–229
Shear M, Hawkins DM, Farr HW (1976) The prediction of lymph node metastases from oral squamous carcinoma. Cancer 37:1901–1907
Shozushima M, Suzuki M, Nakasima T, Yanagisawa Y, Sakamaki K, Takeda Y (1990) Ultrasound diagnosis of lymph node metastasis in head and neck cancer. Dentomaxillofac Radiol 19:165–170
Snow GB, Annyas AA, van Slooten EA, Bartelink H, Hart AA (1982) Prognostic factors of neck node metastasis. Clin Otolaryngol Allied Sci 7:185–192
Sobin L, Gospodarowicz M, Wittekind C (2009) International union against cancer. TNM classification of malignant tumours, 7th edn. Wiley-Blackwell, New York
Som PM, Urken ML, Biller H, Lidov M (1993) Imaging the postoperative neck. Radiology 187:593–603
Som PM, Brandwein M, Lidov M, Lawson W, Biller HF (1994) The varied presentations of papillary thyroid carcinoma cervical nodal disease: CT and MR findings. Am J Neuroradiol 15:1123–1128
Som PM, Curtin HD, Mancuso AA (1999) An imaging-based classification for the cervical nodes designed as an adjunct to recent clinically based nodal classifications. Arch Otolaryngol Head Neck Surg 125:388–396
Souter MA, Allison RS, Clarkson JH, Cowan IA, Coates MH, Wells JE (2009) Sensitivity and specificity of computed tomography for detection of extranodal spread from metastatic head and neck squamous cell carcinoma. J Laryngol Otol 123:778–782
Steinkamp HJ, Maurer J, Cornehl M, Knobber D, Hettwer H, Felix R (1994) Recurrent cervical lymphadenopathy: differential diagnosis with color-duplex sonography. Eur Arch Otorhinolaryngol 251:404–409
Steinkamp HJ, Cornehl M, Hosten N, Pegios W, Vogl T, Felix R (1995) Cervical lymphadenopathy: ratio of long- to short-axis diameter as a predictor of malignancy. Br J Radiol 68:266–270
Steinkamp HJ, van der Hoeck E, Bock JC, Felix R (1999) The extracapsular spread of cervical lymph node metastases: the diagnostic value of computed tomography. Rofo 170:457–462
Steinkamp HJ, Beck A, Werk M, Felix R (2002) Extracapsular spread of cervical lymph node metastases: diagnostic value of magnetic resonance imaging. Rofo 174:50–55
Stennert E, Kisner D, Jungehuelsing M et al (2003) High incidence of lymph node metastasis in major salivary gland cancer. Arch Otolaryngol Head Neck Surg 129:720–723
Stuckensen T, Kovacs AF, Adams S, Baum RP (2000) Staging of the neck in patients with oral cavity squamous cell carcinomas: a prospective comparison of PET, ultrasound, CT and MRI. J Craniomaxillofac Surg 28:319–324
Sumi M, Sakihama N, Sumi T et al (2003) Discrimination of metastatic cervical lymph nodes with diffusion-weighted MR imaging in patients with head and neck cancer. Am J Neuroradiol 24:1627–1634
Syed R, Bomanji JB, Nagabhushan N et al (2005) Impact of combined (18)F-FDG PET/CT in head and neck tumours. Br J Cancer 92:1046–1050
Tankere F, Camproux A, Barry B, Guedon C, Depondt J, Gehanno P (2000) Prognostic value of lymph node involvement in oral cancers: a study of 137 cases. Laryngoscope 110:2061–2065
Terhaard CH, Lubsen H, Van der Tweel I, et al (2004) Salivary gland carcinoma: independent prognostic factors for locoregional control, distant metastases, and overall survival: results of the Dutch head and neck oncology cooperative group. Head Neck 26:681–692 (discussion 92–93)
Traynor SJ, Cohen JI, Gray J, Andersen PE, Everts EC (1996) Selective neck dissection and the management of the node-positive neck. Am J Surg 172:654–657
van den Brekel MW, Stel HV, Castelijns JA et al (1990) Cervical lymph node metastasis: assessment of radiologic criteria. Radiology 177:379–384
van den Brekel MW, Stel HV, Castelijns JA, Croll GJ, Snow GB (1991) Lymph node staging in patients with clinically negative neck examinations by ultrasound and ultrasound-guided aspiration cytology. Am J Surg 162:362–366
van den Brekel MW, Stel HV, van der Valk P, van der Waal I, Meyer CJ, Snow GB (1992) Micrometastases from squamous cell carcinoma in neck dissection specimens. Eur Arch Otorhinolaryngol 249:349–353
van den Brekel MW, Castelijns JA, Stel HV, Golding RP, Meyer CJ, Snow GB (1993) Modern imaging techniques and ultrasound-guided aspiration cytology for the assessment of neck node metastases: a prospective comparative study. Eur Arch Otorhinolaryngol 250:11–17
van den Brekel MW, van der Waal I, Meijer CJ, Freeman JL, Castelijns JA, Snow GB (1996) The incidence of micrometastases in neck dissection specimens obtained from elective neck dissections. Laryngoscope 106:987–991
van den Brekel MW, Castelijns JA, Snow GB (1998a) The size of lymph nodes in the neck on sonograms as a radiologic criterion for metastasis: how reliable is it? Am J Neuroradiol 19:695–700
van den Brekel MW, Pameijer FA, Koops W, Hilgers FJ, Kroon BB, Balm AJ (1998b) Computed tomography for the detection of neck node metastases in melanoma patients. Eur J Surg Oncol 24:51–54
van den Brekel MW, Castelijns JA, Reitsma LC, Leemans CR, van der Waal I, Snow GB (1999) Outcome of observing the N0 neck using ultrasonographic-guided cytology for follow-up. Arch Otolaryngol Head Neck Surg 125:153–156
Vandecaveye V, De Keyzer F, Vander Poorten V et al (2009) Head and neck squamous cell carcinoma: value of diffusion-weighted MR imaging for nodal staging. Radiology 251:134–146
Vandecaveye V, Dirix P, De Keyzer F et al (2010) Predictive value of diffusion-weighted magnetic resonance imaging during chemoradiotherapy for head and neck squamous cell carcinoma. Eur Radiol 20:1703–1714
Vandecaveye V, Dirix P, De Keyzer F et al (2011) Diffusion weighted magnetic resonance imaging early after (chemo) radiotherapy to monitor treatment response in head and neck squamous cell carcinoma. Int J Radiat Oncol Biol Phys [Epub ahead of print]
Vassallo P, Wernecke K, Roos N, Peters PE (1992) Differentiation of benign from malignant superficial lymphadenopathy: the role of high-resolution US. Radiology 183:215–220
Wang HM, Ng SH, Wang CH, Liaw CC, Tsai MH, Lai GM (1996) Correlation between computed tomographic density of lymph node metastases and response to cisplatin-based chemotherapy in patients with head and neck squamous cell carcinoma in an area in which betel quid chewing is prevalent. Cancer 78:1972–1979
Wang P, Yu Q, Shi H (1999) CT findings of non-Hodgkin lymphoma in the head and neck. Zhonghua Kou Qiang Yi Xue Za Zhi 34:208–210
Weiss MH, Harrison LB, Isaacs RS (1994) Use of decision analysis in planning a management strategy for the stage N0 neck. Arch Otolaryngol Head Neck Surg 120:699–702
Wong RJ (2008) Current status of FDG-PET for head and neck cancer. J Surg Oncol 97:649–652
Wong RJ, Lin DT, Schoder H et al (2002) Diagnostic and prognostic value of [(18)F]fluorodeoxyglucose positron emission tomography for recurrent head and neck squamous cell carcinoma. J Clin Oncol 20:4199–4208
Wu CH, Chang YL, Hsu WC, Ko JY, Sheen TS, Hsieh FJ (1998) Usefulness of Doppler spectral analysis and power Doppler sonography in the differentiation of cervical lymphadenopathies. Am J Roentgenol 171:503–509
Xu W, Liu D, Lu Z (1998) CT scanning of the cervical lymph node metastases: compared with histologic sections. Lin Chuang Er Bi Yan Hou Ke Za Zhi 12:99–102
Yao M, Graham MM, Smith RB et al (2004) Value of FDG PET in assessment of treatment response and surveillance in head-and-neck cancer patients after intensity modulated radiation treatment: a preliminary report. Int J Radiat Oncol Biol Phys 60:1410–1418
Yeung AR, Liauw SL, Amdur RJ et al (2008) Lymph node-positive head and neck cancer treated with definitive radiotherapy: can treatment response determine the extent of neck dissection? Cancer 112:1076–1082
Ying M, Ahuja A, Metreweli C (1998) Diagnostic accuracy of sonographic criteria for evaluation of cervical lymphadenopathy. J Ultrasound Med 17:437–445
Ying M, Ahuja A, Brook F, Metreweli C (2001) Vascularity and grey-scale sonographic features of normal cervical lymph nodes: variations with nodal size. Clin Radiol 56:416–419
Yoo GH, Hocwald E, Korkmaz H et al (2000) Assessment of carotid artery invasion in patients with head and neck cancer. Laryngoscope 110:386–390
Yousem DM, Hatabu H, Hurst RW et al (1995) Carotid artery invasion by head and neck masses: prediction with MR imaging. Radiology 195:715–720
Yusa H, Yoshida H, Iwasa S et al (2000) Ultrasonographic assessment for response to radiochemotherapy of metastatic cervical lymph nodes in head and neck cancer: usefulness of grey-scale and color doppler sonography. Ultrasound Med Biol 26:1081–1087
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Bhatia, K.S.S., King, A.D. (2011). Neck Nodal Disease. In: Hermans, R. (eds) Head and Neck Cancer Imaging. Medical Radiology(). Springer, Berlin, Heidelberg. https://doi.org/10.1007/174_2011_382
Download citation
DOI: https://doi.org/10.1007/174_2011_382
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-17868-9
Online ISBN: 978-3-642-17869-6
eBook Packages: MedicineMedicine (R0)