
Abstract
The masticator space is a deep facial space containing the mandibular ramus and the muscles of mastication. The third branch of the trigeminal nerve is also part of the masticator space. Malignancies arising of the masticator space are mostly of mesenchymal origin, such as osteosarcomas, rhabdomysarcomas or angiosarcomas, but also Non-Hodgkin lymphomas are encountered. Beside these primary malignancies, secondary malignancies may involve the masticator space. Malignancies from the surrounding tissues can invade the masticator space, and occasionally a metastasis may occur in this space. The malignant masticator space lesions and their imaging characteristics are described in this chapter, as well as the differential diagnosis with benign entities.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
The masticator space is a deep facial space surrounded by the superficial layer of the deep cervical fascia. The content of the masticator space consists of muscles of the mastication which are the temporalis muscle, the masseter muscle, the lateral and medial pterygoid muscles (Chong and Fan 1996; Aspestrand and Boysen 1992).
These muscles attach to the ascending part of the mandibula, the mandibular ramus. Furthermore, it contains the third branch of the trigeminal nerve (V3), the mandibular nerve. The third branch of the trigeminal nerve leaves the skull base through the oval foramen, passes between the lateral and medial pterygoid muscles, and then enters the mandible through the mandibular foramen. The V3 nerve provides the motor innervation of the masticator muscles, and carries sensory information from the mandibular teeth, gums, and lower lip and chin region.
Primary malignancies arising from/within the masticator space are mostly of mesenchymal origin (Galli et al. 2010; Mendenhall et al. 2010; Palacios and Valvassori 2000). Secondary malignancies involving the masticator space arise from the surrounding structures—such as the oral cavity, pharynx or the parotid gland—or correspond to metastasis from other regions of the body (Nishikawa et al. 2010; Loehn et al. 2009; Glaser et al. 1997).
The spectrum of primary malignant lesions includes osseous lesions such as mandibular osteosarcoma, which is the most common primary malignancy in this space (Fig. 1). Other osseous tumors are e.g. chondrosarcomas or plasmocytoma. Malignant tumors arising within the muscles and fascias are rhabdomyosarcomas or fibrosarcomas, and those arising from the nerve may be neurosarcomas (Gosau et al. 2008; Toranzo-Fernandez et al. 2000; Chemello et al. 1988). Other primary malignancies seen in this space are hemangiosarcomas and Non-Hodgkin’s lymphoma (Daniels et al. 1996).

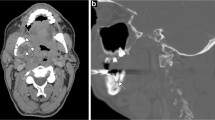
Malignant intrinsic lesion of the left masticator space in a 55-year-old female with trismus and pain of the left V3 territory with biopsy-proven osteosarcoma. a Contrast-enhanced axial CT image shows a soft tissue mass causing osteolysis of the left mandibular ramus with soft tissue infiltration (arrow). b Axial CT image in bone-window-level-setting shows an irregular unsharply demarcated osteolytic region with periostal reaction of the left mandibular ramus (arrow)
The clinical symptoms of malignant lesions of the masticator space are swelling, numbness, pain and trismus. The nerval symptoms of pain and numbness are also caused by involvement of V3, which may serve as a route for perineural tumor spread into the skull base (Hyare et al. 2010). Trismus is a reactive mouth opening impairment and caused by infiltration of the masticator muscles by a malignant tumor or an inflammatory process like an abscess.
2 Imaging Techniques
The different imaging techniques of multidetector-CT (MDCT), and magnetic resonance imaging (MRI), as well as PET-CT and their ability to depict tumoral lesions are described earlier in this book (see "Imaging Techniques").
MDCT of the masticator space is performed in the axial plane beginning cranially from the suprasellar region down to the base of the neck. Symmetrical imaging of the head and neck region is important as some pathologies may be very subtle and the comparison of one side with the other allows to detect and delineate the lesion.
The investigation is performed with intravenous administration of iodinated contrast material. The images are obtained in a soft-tissue- and bone-window-level setting. Coronal and sagittal images may be reconstructed from the axial sections. The section thickness of the different imaging planes should be 3 mm or less, without interval.
MRI is performed with a dedicated head and neck coil. The predominant plane is the axial plane, but also coronal and sagittal planes are obtained. The standard sequences are STIR or T2-weighted fat-suppressed sequences followed by T1-weighted sequences before and after the intravenous application of contrast material. In addition, also T1-weighted contrast enhanced sequences with fatsuppression may be performed. The injection of contrast material is mandatory as it enables to better delineate the tumor extent, including possible perineural spread. The section thickness should not be thicker than 3–4 mm and the matrix should be high, if possible 512 × 512 depending on the scanner technology.
PET is nowadays performed in combination with MDCT (PET-CT, see "Imaging Techniques").
3 General Imaging Findings
The most important goal of imaging is to correctly depict the anatomic extent of the lesion and to determine whether the lesion originates primarily from the structures of the masticator space or invades the masticator space from outside (Chong and Fan 1996). The depiction of the epicentre of the mass as well as the displacement of structures—such as the fatty tissues—may be helpful to exactly localize and characterize the type of lesion.
Malignant tumors arising from the mandible may show a characteristic pattern of bone destruction and periosteal reaction, as has been described for the peripheral skeleton and can also be applied at the mandible.
The radiological appearances of bone destruction has been summarized in a classification system by Lodwick. This system is very useful to describe the aggressiveness of a bone tumor. Lodwick described three types (grading) of destruction (Lodwick et al. 1980):
-
1.
Geographic destruction.
-
2.
Moth-eaten like destruction.
-
3.
Permeative destruction.
These types of destruction correspond to the biological activity and aggressiveness of the lesion. Geographic destruction mostly occurs in benign lesion, while moth-eaten like destruction and permeative destruction are usually seen in very aggressive tumors (Fig. 2). Sometimes moth-eaten like destructions or a mixture of moth-eaten like destruction and permeative destruction may be seen in inflammatory processes; the differential diagnosis may then be difficult based on imaging alone, and the correct diagnosis can often only be obtained by biopsy.

a Forms of osteolysis (A1) geographic no margin (A2) geographic sclerotic margin (A3) geographic unsharp margin (A4) motheaten (A5) permeative b Forms of cortical reactions (B1) bulging of corticalis (B2) thinning of corticalis (B3) thinning and lamellating (B4) sunburst (B5) Codman triangle
Furthermore, Lodwick described several types of periosteal reactions indicating the grade of aggressiveness. Bulging and thinning of the cortex without periosteal reaction reflects more benign types, while thinning or disruption of the cortex, with a periosteal reaction such as a so-called sunburst or Codmans’ triangle indicates malignancy.
In addition to the destruction of the bone, primarily osseous tumors often display a soft tissue component. In some tumors, this soft tissue component may show a calcified matrix. In some tumors such as the chondrosarcoma, characteristic popcorn-like calcifications may be seen.
Malignant tumors arising from the soft tissues of the masticator space may invade the mandible and cause bony destruction, which mostly appears irregular and has unsharp margins. Metastasis within the bone may be either osteolytic, or osteoblastic as is seen for example in prostate cancer (Glaser et al. 1997).
When the V3 is involved by the tumor, signs of muscle atrophy may be seen. Initially, denervation atrophy may result in an increased contrast enhancement of the muscles; later, the muscles will show volume decrease and fatty atrophy, which is easily seen on MRI. Also, increased contrast enhancement and potential thickening of the V3 nerve is a sign of perineural tumor invasion (Fig. 3) (Maroldi et al. 2008).

Graph illustrating perineural tumor spread along the V3 through the oval foramen by a tumor growing around the mandibular nerve
These general radiologic findings should be taken into consideration together with the clinical information to establish for most accurate diagnosis.
4 Imaging Findings of Primary Malignancies
The most common primary malignant bone tumor in the masticator space is the osteosarcoma (Figs. 1 and 4) (Kim et al. 2010; dos Santos and Cavalcanti 2002; Zorzan et al. 2001). MDCT in bone-window-level setting excellently depicts the periosteal and cortical changes which are destructive and sometimes accompanied with a so-called “sunburst” periosteal reaction. This is characteristic for a highly malignant bone tumor. MRI depicts the osseous invasion better than CT (Chidzonga and Mahomva 2007). Especially, T1-weighted contrast enhanced sequences with fatsuppression delineate the tumor extent. PET-CT is a valuable tool to show distant metastasis.

Malignant intrinsic lesion of the left masticator space in a 67-year-old female with trismus and dysaesthesia of the left V3 territory with biopsy-proven osteosarcoma. a Axial contrast-enhanced CT image shows a soft tissue mass in the masticator space surrounding the left mandibular ramus (arrow). b Coronal CT image in bone-window-level-setting shows an irregular unsharp osteolysis of the cortical and spongiotic structures of the left mandibular ramus (arrow); final diagnosis was osteosarcoma of the mandible
Very rarely primary bone malignancies such as multiple myeloma or plasmocytoma may also be seen in the mandibule (Fig. 5). In these cases, if no periosteal or cortical reactions are present, MRI depicts the intraosseous-spongiotic extension of the tumor replacing the normal bone marrow. Other tumors, such as the Ewing sarcoma may arise in the mandible and are sometimes depicted as a subtle osteolytic region on panoramic radiographs of the mandible (Fig. 6). The tumor extension is much better seen on MDCT or MR images.

Malignant intrinsic lesion of the right masticator space in a 72-year-old male with numbness and pain of the right V3 territory with biopsy-proven multiple myeloma. a Axial T1-weighted MR image after i.v. contrastmaterial shows a mass (arrow) infiltrating the right mandible and the adjacent parotid gland. b Coronal fat-suppressed T1-weighted MR image after i.v. contrastmaterial shows the mass (arrow) infiltrating the right mandible and the adjacent masticator muscles. Biopsy revealed plasmocytoma of the right mandible

Malignant intrinsic lesion of the left masticator space in a 32-year-old female with dysaesthesia of the left V3 territory with biopsy-proven Ewing sarcoma. a Panoramic radiograph reveals unsharp permeative osteolysis (arrow) of the left mandibular ramus. b Coronal CT image in bone-window-level-setting shows unsharp-diffuse osteolysis of the left mandibular ramus (arrow)
Fibrosarcoma or rhabdomyosarcoma may cause an unsharp, lobulated mandibular destruction, as seen on panoramic radiographs or on an MDCT in a bone–window-level setting (Fig. 7) (Gosau et al. 2008; Chemello et al. 1988). Contrast-enhanced MDCT or MRI will show a mass originating from the soft tissues of the masticator space with bony destruction.

Malignant intrinsic lesion of the right mandible in a 57-year-old male with progressive swelling of the right cheek and dysaesthesia of the right inferior alveolar nerve with biopsy-proven fibromyxosarcoma. a Panoramic radiograph reveals lobulated slightly unsharply marginated osteolysis of the right mandibular ramus (arrow). b Axial CT image in bone-window-level-setting shows an irregular unsharp osteolysis of the right mandibular ramus (arrow). c Axial CT image in soft window shows osteolytic and a soft tissue mass infiltrating around the mandibular ramus
The presence of a mass within the masticator muscles in a child is highly suggestive for a rhabdomyosarcoma (Fig. 8). These tumors may be hyperintense on STIR or T2-weighted fatsuppressed images with a strong contrast enhancement on T1-weighted images. The mass appears sometimes lobulated with subtle irregular-unsharp margins infiltrating the surrounding tissues.

Malignant intrinsic lesion of the left masticator space in a 5-year-old boy presenting with trismus. a Axial T2w fat-suppressed MR image shows a hyperintense mass (arrow) in the left masticator space within the lateral pterygoid muscle. b Axial T1w fat suppressed MR image after contrastmaterial application shows an enhancing mass (arrow) with the epicentre in the left lateral pterygoid muscle. Biopsy revealed an embryonic pleomorphic rhabdomyosarcoma
Because of its excellent soft tissue contrast resolution, MRI may show signs indicating that the tumor originates from vascular structures (Daniels et al. 1996). The “salt-and-pepper-sign” is a characteristic of vascular tumors and is seen e.g. in angiosarcomas (Fig. 9). Apart from this pattern, MRI may also show diffuse infiltration of such a tumor into the surrounding tissues.

Malignant intrinsic lesion of the left masticator space in a 64-year-old male with trismus. a T2-weighted MR image with fatsuppression shows an ill-defined hyperintense mass (arrow) containing hypointense structures, with its epicentre around the left mandibular ramus and infiltration of the adjacent masticator muscles. b Coronal contrast-enhanced MR image T1-weighted shows an ill-defined mass with a “salt-and-pepper-sign” (arrow). This was histologically diagnosed as an angiosarcoma
5 Imaging Findings of Secondary Malignancies
The masticator space can be invaded by malignancies surrounding or lying close to the masticator space. These secondary neoplasms can be of parotid gland origin. When invading the masticator space, these tumors may reach the V3 and grow perineurally, especially adenoid cystic carcinomas are notorious for their tendency to grow along nerves (Figs. 3 and 10) (Maroldi et al. 2008; Laine et al. 1990).

Malignant extrinsic lesion of the right masticator space in a 49-year-old female with numbness and pain of the right V3 territory with recurrent perineural tumor spread by an adenoid cystic carcinoma of the parotid gland. a Axial contrast-enhanced T1-weighted MR image shows a mass (arrow) primarily originating from the right parotid gland infiltrating the right mandible and the masticator muscles. b The coronal image also shows an enhancement in the right mandible and the masticator muscles and also perineural tumor extension along the V3 with meningeal enhancement (arrow). Histology revealed recurrent adenoid cystic carcinoma
Squamous cell carcinomas originating from the retromolar trigone and from the oropharyngal tonsil can also infiltrate the masticator space, sometimes appearing like a tumor primarily arising from the masticator space (Fig. 11).

Malignant extrinsic lesion of the left masticator space in a 48-year-old male with pain in the left V3 territory by invasion of the mandible by a surgically proven squamous cell carcinoma of the left tonsil. a, b Axial and coronal CT image after i.v. contrast-material application shows osteolysis of the mandibular ramus, surrounded by an enhancing soft tissue (arrow)
The masticator space can also be affected by metastasis. Such metastasis may occur in the soft tissues or in the mandible. Bony metastasis can be osteolytic (e.g. from lung or breast cancer) or osteoblastic (e.g. from prostate cancer) (Glaser et al. 1997; Nishikawa et al. 2010). Osteolytic metastasis produce an irregular-unsharp lysis of the bone, while osteoblastic metastasis appear mostly very sclerotic on conventional radiographs or on MDCT in a bone-window-level setting (Figs. 12 and 13).

Malignant secondary lesion of the right mandible in a 55-year-old female with dysaesthesia of the right V3 territory. a, b Axial and coronal CT image in bone-window-level-setting shows an irregular unsharply marginated osteolysic area (arrow) in the right mandibular ramus. Further investigation revealed metastasis from thyroid carcinoma

Malignant secondary lesion of the right mandible in an 83-year-old male with dysaesthesia of the right V3 territory caused by a osteoblastic metastasis of a prostatic carcinoma. a, b Axial and sagittal CT image in bone-window-level-setting shows sclerotic osteoblastic lesion of the right mandibular ramus (arrow)
6 Posttreatment Imaging
Also after treatment, imaging plays an important role in the management of the patient.
The treatment options for malignancies in the masticator space depend on the histology and extent of the lesion; this may be either surgery, chemotherapy or chemoradiotherapy, or a combination of these (Nishikawa et al. 2010). Posttreatment imaging may delineate complications e.g. after surgery or show tumor response or non-response after therapy. Also tumor recurrence may be depicted by imaging before becoming clinically apparent.
Treatment of bone metastasis, or of osteoporosis by bisphosphonates may cause osteonecrosis of the mandible (Fig. 14) (Bisdas et al. 2008; Studer et al. 2004). In these patients, osteolytic and osteosclerotic changes of the bone can be seen sometimes with fragmentation and sequestration, well delineated on MDCT in a bone-window-level setting or on a so-called Dental-CT. Similar imaging findings may be seen in patients with mandibular osteoradionecrosis, but in a different clinical context.

Intrinsic lesion of the right mandible in a 69-year-old female with dysaesthesia of the right V3 territory caused by bisphosphonates related osteonecrosis. Axial CT image in bone-window-level setting shows lamellating periosteal reaction and sclerosis and fragmentation of the right ascending ramus of the mandible (arrow)
7 Benign Conditions Mimicking Malignancy
Some benign conditions may radiologically mimic malignant pathologies.
A Stafne cyst is a focal cortical depression in the lingual cortex of the posterior mandible. On panoramic radiography, it appears as a cystic lesion. The bony “defect” either contains fat or salivary gland tissue (Fig. 15) (Dorman and Pierse 2002). It has a typical radiologic appearance and location and should not be misinterpretated as a potentially suspect lesion.

Intrinsic variant on the lingual side of the left mandible in a 25-year-old male without any clinical symptoms. a Axial contrast-enhanced CT image shows a bony defect containing fatty tissue in the left mandibular angle (arrow). b Axial CT image in bone-window-level-setting shows a regular margin of the bony defect (arrow). This appearance is characteristic of a Staphne cyst
Osteomyelitis is an important differential diagnosis and sometimes has an appearance similar to malignancies primarily arising from the mandible. In some cases osteomyelitis—especially when chronic—may mimic a malignant tumor as it may show periosteal and cortical reactions resembling a sunburst-appearance of an osteosarcoma (Fig. 16) (Schuknecht and Valavanis 2003). The clinical history of the patient combined with laboratory data and imaging findings lead to the correct diagnosis.

Intrinsic lesion of the right mandible in a 75-year-old male with numbness in the territory of the right inferior alveolar nerve territory caused by biopsy-proven chronic osteomyelitis. Axial CT image in bone-window-level-setting shows sunburst-like periostal reaction (arrows) of the right mandibular ramus
Dentogenic cysts, keratocysts or odontogenic tumors, such as ameloblastoma, may extend in the ascending ramus of the mandible (Kaneda et al. 2003). In most of these cases smooth osteolysis with cortical thinning and scalloping can be seen radiologically (Figs. 17 and 18). The combination of clinical information and radiological findings often allows to establish the dentogenic origin of these lesions.

Benign intrinsic lesion of the right mandible in a 26-year-old male with subtle numbness of the right inferior alveolar nerve. a Panoramic radiograph reveals lobulated smooth osteolysic area (arrow) in the right mandibular ramus. b Coronal CT image in bone-window-level-setting shows a smooth-sharply demarcated osteolytic area in the right mandibular ramus (arrow). Further investigation revealed a keratocyst

Benign intrinsic lesion of the left mandible in a 42-year-old male with numbness in the territory of the left inferior alveolar nerve. a Axial contrast-enhanced CT image shows an expansile, largely non-enhancing soft tissue mass (arrow) within the left mandibular ramus. b Coronal CT image in bone-window-level-setting shows smoothly marginated osteolysis with scalloping of the left mandibular ramus (arrow). This was caused by an ameloblastoma
Intra-osseous vascular malformations may cause mandibular osteolysis; the identification of large feeding vessels allows to make the diagnosis. A biopsy should not be performed in such cases to avoid significant bleeding.
8 Summary
Primary and secondary malignancies of the masticator space are rare entities. Many different kinds of malignant neoplasms can be seen in this space.
By determining the point of origin of the neoplasm, and combining imaging findings with clinical data, in most cases the differential diagnosis can be limited to a number of entities.
References
Aspestrand F, Boysen M (1992) CT and MR imaging of primary tumors of the masticator space. Acta Radiol 33(6):518–522
Bisdas S, Chambron Pinho N, Smolarz A, Sader R, Vogl TJ, Mack MG (2008) Bisphosphonate-induced osteonecrosis of the jaws: CT and MRI spectrum of findings in 32 patients. Clin Radiol 63(1):71–77
Chemello PD, Nelson CL, Tomich CE, Sadove AM (1988) Embryonal rhabdomyosarcoma arising in the masseter muscle as a second malignant neoplasm. J Oral Maxillofac Surg 46(10):899–905
Chidzonga MM, Mahomva L (2007) Sarcomas of the oral and maxillofacial region: a review of 88 cases in Zimbabwe. Br J Oral Maxillofac Surg 45(4):317–318
Chong VF, Fan YF (1996) Pictorial review: radiology of the masticator space. Clin Radiol 51(7):457–465
Daniels RL, Haller JR, Harnsberger HR (1996) Hemangiopericytoma of the masticator space. Ann Otol Rhinol Laryngol 105(2):162–165
Dorman M, Pierse D (2002) Ectopic salivary gland tissue in the anterior mandible: a case report. Br Dent J 193(10):571–572
dos Santos DT, Cavalcanti MG (2002) Osteosarcoma of the temporomandibular joint: report of 2 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94(5):641–647
Galli F, Flor N, Villa C, Franceschelli G, Pompili G, Felisati G, Biglioli F, Cornalba GP (2010) The masticator space value of computed tomography and magnetic resonance imaging in localisation and characterisation of lesions. Acta Otorhinolaryngol Ital 30(2):94–99
Glaser C, Lang S, Pruckmayer M, Millesi W, Rasse M, Marosi C, Leitha T (1997) Clinical manifestations and diagnostic approach to metastatic cancer of the mandible. Int J Oral Maxillofac Surg 26(5):365–368
Gosau M, Draenert FG, Winter WA, Mueller-Hoecker J, Driemel O (2008) Fibrosarcoma of the childhood mandible. Head Face Med 16(4):21
Hyare H, Wisco JJ, Alusi G, Cohen M, Nabili V, Abemayor E, Kirsch CF (2010) The anatomy of the nasopharyngeal carcinoma spread through the pharyngobasilar fascia to the trigeminal mandibular nerve on 1.5T MRI. Surg Radiol Anat 32(10):937–944
Kaneda T, Minami M, Kurabayashi T (2003) Benign odontogenic tumors of the mandible and maxilla. Neuroimaging Clin N Am 13(3):495–507
Kim GT, Lee JK, Choi BJ, Kim J, Han SH, Kwon YD (2010) Malignant transformation of monostotic fibrous dysplasia in the mandible. J Craniofac Surg 21(2):601–603
Laine FJ, Braun IF, Jensen ME, Nadel L, Som PM (1990) Perineural tumor extension through the foramen ovale: evaluation with MR imaging. Radiology 174(1):65–71
Lodwick GS, Wilson AJ, Farrel C, Virtama P, Dittrich F (1980) Determination of growth rates of focal lesions of bone from radiographs. Radiology 134(3):577–583
Loehn B, Walvekar RR, Harton A, Nuss D (2009) Mandibular metastasis from a skull base chordoma: report of a case with review of literature. Skull Base 19(5):363–368
Maroldi R, Farina D, Borghesi A, Marconi A, Gatti E (2008) Perineural tumor spread. Neuroimaging Clin N Am 18(2):413–429
Mendenhall WM, Fernandes R, Werning JW, Vaysberg M, Malyapa RS, Mendenhall NP (2010) Head and neck osteosarcoma. Am J Otolaryngol [Epub ahead of print: 18 Nov]
Nishikawa H, Nakashiro K, Sumida T, Sugita A, Hamakawa H (2010) Mandibular osteoblastic metastasis of poorly differentiated carcinoma of the thyroid gland. Int J Oral Maxillofac Surg 39(3):301–304
Palacios E, Valvassori G (2000) Masticator space tumor, malignant schwannoma. Ear Nose Throat J 79(8):550
Schuknecht B, Valavanis A (2003) Osteomyelitis of the mandible. Neuroimaging Clin N Am 13(3):605–618
Studer G, Grätz KW, Glanzmann C (2004) Osteoradionecrosis of the mandible in patients treated with different fractionations. Strahlenther Onkol 180:233–240
Toranzo-Fernandez JM, Noyola-Frias MA, Sanchez-Hermosillo E, Gonzalez-Mendoza E (2000) Rhabdomyosarcoma in children: report of two cases. J Clin Pediatr Dent 25(1):87–90
Zorzan G, Tullio A, Bertolini F, Sesenna E (2001) Osteosarcoma of the mandibular condyle: case report. J Oral Maxillofac Surg 59(5):574–577
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer-Verlag Berlin Heidelberg
About this chapter
Cite this chapter
Czerny, C., Saat, R. (2011). Malignant Lesions of the Masticator Space. In: Hermans, R. (eds) Head and Neck Cancer Imaging. Medical Radiology(). Springer, Berlin, Heidelberg. https://doi.org/10.1007/174_2011_379
Download citation
DOI: https://doi.org/10.1007/174_2011_379
Publisher Name: Springer, Berlin, Heidelberg
Print ISBN: 978-3-642-17868-9
Online ISBN: 978-3-642-17869-6
eBook Packages: MedicineMedicine (R0)