
Abstract
Background and objective
Transbronchial lung biopsy (TBLB) can be obtained using forceps and usually represents the centrilobular regions. Therefore, disorders that are centered around terminal and respiratory bronchioles or distributed along the lymphatic routes can be diagnosed. This study investigated the diagnostic yield of flexible bronchoscopy in patients with ground-glass opacity (GGO) or alveolar filling for histopathological diagnosis and found out its complications.
Patients and methods
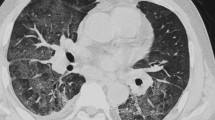
Twenty-six patients with predominant GGO or alveolar opacity in the chest computed tomographic (CT) scan were submitted for TBLB for histopathological confirmation. Patients with respiratory failure, heart failure, coagulopathy, or pathognomonic CT patterns were excluded. All patients were subjected to full history taking, chest CT scan, and TBLB with histopathological examination of the specimens.
Results
The diagnostic yield of TBLB was 73.1%. Histopathological diagnoses included hypersensitivity pneumonitis (23.1%), sarcoidosis (19.2%), adenocarcinoma (11.5%), small cell lung cancer (7.7%), alveolar proteinosis (3.8%), alveolar hemorrhage (3.8%), organizing pneumonia (3.8%), and chronic nonspecific inflammation (26.9%). There was no significant correlation between age, sex, smoking, and histopathological diagnoses. Regarding the predominant CT finding, 15 (57.7%) patients had GGO, whereas 11 (42.3%) patients had alveolar filling with significant (P=0.008) positive correlation between the CT predominant pattern and histopathological diagnoses. There was a positive significant correlation between lymph node enlargement in CT and histopathological diagnosis (P=0.029). Complications from TBLB included the pneumothorax (15.4%) and bleeding (7.7%).
Conclusions
TBLB seems to be a useful and safe procedure. It is of a high diagnostic value. Therefore, it could be considered a routine diagnostic procedure before thoracoscopic or open lung biopsy.
Article PDF
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.References
Austin JH, Müller NL, Friedman PJ, Hansell DM, Naidich DP, Remy-Jardin M, et al. Glossary of terms for CT of the lungs:recommendations of the Nomenclature Committee of the Fleischner Society. Radiology 1996;200:327–331.
Miller WTJr, Shah RM. Isolated diffuse ground-glass opacity in thoracic CT:causes and clinical presentations. Am J Roentgenol 2005;184:613–622.
Engeler CE, Tashjian JH, Trenkner SW, Walsh JW. Ground-glass opacity of the lungparenchyma:a guide to analysis with high-resolution CT. Am J Roentgenol 1993;160:249–251
Collins J, Stern EJ. Ground-glass opacity at CT:the ABCs. Am J Roentgenol 1997;169:355–367.
Remy-Jardin M, Giraud F, Remy J, Copin MC, Gosselin B, Duhamel A. Importance of ground-glass attenuation in chronic diffuse infiltrative lung disease:pathologic-CT correlation. Radiology 1993;189:693–698.
AmericanThoracicSociety;EuropeanRespiratorySociety. AmericanThoracic Society/European Respiratory Society international multidisciplinary consensus classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2002;165:227–304.
Beigelman-Aubry C, Hill C, Guibal A, Savatovsky J, Grenier PA. Multidetector row CTand postprocessing techniques in the assessment of diffuse lung disease. Radiographics 2005;25:1639–1652.
Al-Tubaikh JA. Alveolar lung diseases. Internal medicine. 2010; Springer; 113pp.
Williams T, Brooks T, Ward C. The role of atropine premedication in fiberoptic bronchoscopy using intravenous midazolam sedation. Chest 1998;113:1394–1398.
Harless KW, Scheinhorn DJ, Tannen RC, Zimmerman GA, Allen PA. Administration of oxygen with mouth-held nasal prongs during fiberoptic bronchoscopy. Chest 1978;74:237–238.
Kvale PA. Bronchoscopic lung biopsy. How I do it. J Bronchol 1994;1:321–326.
Izbicki G, Shitrit D, Yarmolovsky A, Bendayan D, Millar G, Fink G, et al. Is routine chest radiography after transbronchial biopsy necessary? A prospective study of 350 cases. Chest 2006;129:1561–1564.
Zavala DC. Pulmonary hemorrhage in fiberoptic transbronchial biopsy. Chest 1976;70:584–588.
Khoo KL, Lee P. Endobronchial epinephrine:confusion is in the air. ATS 2013;187:1137–1138.
Remy-Jardin M, Giraud F, Remy J, Copin MC, Gosselin B, Duhamel A. Importance of ground-glass attenuation in chronic diffuse infiltrative lung disease:pathologic-CT correlation. Radiology 1993;189:693–698.
Joyner LR, Scheinhorn DJ. Transbronchial forceps lung biopsy through the fiberoptic bronchoscope diagnosis of diffuse pulmonary disease. Chest 1975;67:532–535.
Ensminger SA, Prakash UB. Is bronchoscopic lung biopsy helpful in the management of patients with diffuse lung disease? Eur Respir J 2006;28:1081–1084.
Abd El-Kareem D, Akl YM, Nakhla GA, Elhindawi AA, Eltorkey MA. Clinico-pathologic presentation of hypersensitivity pneumonitis in Egyptian patients:a multidisciplinary study. Multidiscip Respir Med 2017; 12:10.
Lynch DA, Rose CS, Way D, King TEJr. Hypersensitivity pneumonitis:sensitivity of high-resolution CT in a population-based study. Am J Roentgenol 1992;159:469–472.
Muller NL, Kullnig P, Miller RR. The CT findings of pulmonary sarcoidosis:analysis of 25 patients. Am J Roentgenol 1989;152:1179–1182.
Trigaux JP, Gevenois PA, Goncette L, Gouat F, Schumaker A, Weynants P. Bronchioloalveolar carcinoma:computed tomography findings. Eur Respir J 1996;9:11–16.
Holbert JM, Costello P, Li W, Hoffman RM, Rogers RM. CT features of pulmonary alveolar proteinosis. Am J Roentgenol 2001;176:1287–1294.
Faria IM, Zanetti G, Barreto MM, Rodrigues RS, Araujo-Neto CA, Pereira eSilva JL, et al. Organizing pneumonia:chest HRCT findings. J Bras Pneumol 2015;41:231–237.
Madkour A, Osman N, Sharkawy S, Gomaa A. Assessment of patients’ satisfaction with flexible bronchoscopy:initial Egyptian experience. Egypt J Broncho 2013;7:71–77.
Hue SH. Complications in transbronchial lung biopsy. Korean J Intern Med 1987;2:209–213.
Milmam N, faurschou P, Munch EP, Grode G. Transbronchial lung biopsy through the fibre optic bronchoscope. Results and complications in 452 examinations. Respir Med 1994;88:749–753.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Rights and permissions
This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Youssef, H.A.A., Khattab, H.M., Shaban, M.M. et al. Diagnostic yield of fiber optic bronchoscopy in alveolar and/or ground glass opacification in chest computed tomographic scan. Egypt J Bronchol 12, 413–418 (2018). https://doi.org/10.4103/ejb.ejb_16_18
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4103/ejb.ejb_16_18