
Abstract
The decision to release a patient receiving medical treatments with unsealed radionuclides should take many factors into account, and is the balance among different requirements. The Italian legislative implementation of the new European Commission Basic Safety Standards (BSS) resulted in the recent Legislative Decree 101/2020, which sets specific dose constraints for the public and for carers and comforters. The aim of the present research is to assess acceptable release criteria (in terms of personal dose-equivalent rate at the moment of hospital discharge) to ensure compliance with the current regulatory framework in Italy. The MicroShield® code was used to derive a more realistic model for the emission of radioactivity by patients treated with radiopharmaceuticals. A geometric source-dependent correction factor, G(r), is introduced in order to take into account the volumetric distribution of the radionuclide into the human body and the attenuation of radiation from body tissues. The proposed approach has the potential to be routinely applied by clinic decision-makers to assess release criteria in the nuclear medicine practice.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Radionuclide therapy (RT) uses unsealed radiopharmaceuticals for the selective delivery of radiation to tumours or pathological areas. Over the last decade, the introduction of new radionuclides, along with improved labelling technology, has resulted in an increased number of applications of RT treatments. At present, many new radiopharmaceuticals are in development or in early phase clinical trials [1,2,3]. These will provide new treatment options for a number of cancers, particularly following unsuccessful treatments with conventional chemotherapeutics or disease relapse.
Depending on the administered activity, RT treatments can be performed with either the patient admitted to hospital or in an outpatient setting. Of note, at present, there is no general agreement on whether it is necessary to hospitalise patients undergoing RT. Along these lines, there has been much debate in recent times about when and under what conditions RT patients can be released. Clinical practice and administration protocols differ from one country to another and the same holds for the practical application of the optimisation principle. This is especially true for decisions regarding the period after which the patient can be allowed to leave hospital following treatment. However, no matter if treated on an outpatient or inpatient basis, safety issues arise for the patient, her/his family, associated carers, staff and the general public when the patient is discharged from the hospital.
It is generally acknowledged that 131I is the unsealed radionuclide that results in the largest dose to medical staff, the public, caregivers, and relatives. However, other radionuclides used in therapy may represent a concern from the radiation protection point of view, among which 177Lu. Administered activity of 131I for patients treated for hyperthyroidism ranges from approximately 100 to 1000 MBq, while for treatment of thyroid cancer, the administered activity ranges from approximately 4000 to 8000 MBq. The major source of radiation to members of the public from administrations of 131I (including sewage treatment workers) will be from external radiation [4]. For medical personnel, relatives, and caregivers too, the major source of radiation is from external exposure, but the potential also exists for them to be exposed to contamination from the patient. For 131I, the patient-release levels in EU Member States are based on residual activities. It is generally accepted that if the residual activity in a patient going home is less than 400 MBq, the dose to family and close friends will almost always be below 1 mSv, provided they carefully comply with the instructions given. In the clinical practice, an administered activity of 600 MBq corresponds to a residual activity of about 400 MBq (considering 66% retention), which corresponds to about 20 \(\upmu \hbox {Sv}/\hbox {h}\) at 1 metre from any point of the body. This figure in some countries is often used as a measure of good practice [5,6,7]
According to the EU Directive 2013/59 (Article 6) [8], EU Member States shall ensure that, where appropriate, dose constraints are established for the purpose of prospective optimisation of protection. In particular, for public exposure, the dose constraint shall be set for the individual dose that members of the public receive from the planned operation of a specified radiation source. The competent authority shall ensure that the constraints are consistent with the dose limit for the sum of doses to the same individual from all authorised practices. For medical exposure, dose constraints shall apply only with regard to the protection of carers and comforters and volunteers participating in medical or biomedical research.
The Italian legislative implementation of the new European Commission Basic Safety Standards (BSS) resulted in the recent Legislative Decree 101/2020 [9]. Prior to its entry into force, any patient treated with unsealed radionuclides needed to be treated on an inpatient basis, with the exclusion of patients administered with less than 600 MBq of 131I. The new Italian legislation reaffirms that any patient administered with an activity of 131I greater than 600 MBq requires to be treated in an inpatient setting. Conversely, for any other RT treatment the decision to release a patient from hospital needs be determined by the nuclear medicine physician on an individual basis, with the support of the local medical physics expert and radiation protection expert. The factors to be taken into account include the following issues related to patients: medical needs of the patient, pattern of contact with other people, age, family/home environment, occupational and public exposures, cost and environmental factors, local social and infrastructural arrangements.
2 Materials and methods
The decision to release a patient who has undergone medical treatment with unsealed radionuclides should take many factors into account, and is the balance among different requirements. Hospitalisation can reduce exposure to the public, but increases exposure to hospital staff and often involves monetary and other costs, thus requiring the application of the principle of optimisation of protection.
Relevant national dose limits must be met for the public, but the ICRP, IAEA and EU propose dose constraints rather than dose limits to be applied to comforters and carers [6]. According to European Directive 2013/59, “carers and comforters” are “individuals knowingly and willingly incurring an exposure to ionising radiation by helping, other than as part of their occupation, in the support and comfort of individuals undergoing or having undergone medical exposure”, and Member States shall ensure that “the exposure of carers and comforters show a sufficient net benefit, taking into account the direct health benefits to a patient, the possible benefits to the carer/comforter and the detriment that the exposure might cause”. The general opinion [10] is that “knowing and willing” individuals can be identified as those living under the same roof as the patient and those who visit the patient in the hospital or at her/his home.
2.1 The regulatory framework
In Italy, Directive 59 was implemented by Decree 101/2020, which entered into force on 27 August 2020. According to the Legislative Decree 101/2020, the residual activity in the patient at the time of discharge shall be such that dose constraints for comforters and carers and members of the public reported in Table 1 are not exceeded (Annex XXV, Legislative Decree 101/2020).
Of note, the effective dose constraint for members of the public is set at 0.3 mSv per treatment. This constraint is particularly restrictive considering that in other European countries it is set at 1 mSv and in the USA at 5 mSv. Moreover, in the European recommendation Radiation Protection n. 97 [5], the constraint for children of the family of the patient is set at 1 mSv, while according to the Italian law they are considered as members of the public.
In any case, a constraint of 0.3 mSv is indicated in some international guides such as in Radiation Protection n. 97 [5] and ICRP [4] and refers to members of the public other than cohabitants of the patient; they are called “third persons”, who are occasional “victims” of the patient-source and could be exposed also to other man-made sources of radiation [5]. On the contrary, as family and close friends may benefit from the presence of the treated patient in the family, and caring for him/her may represent an once-in-a-lifetime circumstance, the dose constraint for them can be higher than the public dose limits [5]. It must be observed that some therapies with radionuclides require a number of treatment cycles, e.g. therapy with 177Lu-DOTATATE, consisting in 4 cycles in 6 to 12-week intervals (with 7.4 GBq administered per cycle). In such a circumstance, the dose constraints need to be met considering the total number of cycles. This is especially true for carers and comforters. In fact, while it is very unlikely that a released patient may repeatedly expose the same individual of the population, carers and comforters are likely to be exposed at each treatment cycle.
Based on the definitions contained in the Italian Decree 101/2020, “carers and comforters” can be considered as the cohabitants of the released patient who are effectively aware of the condition of exposure to which they undergo and therefore in the following they are differentiated from the rest of the population by defining them as “cohabitants”.
When applying these dose constraints, an algorithm is necessary to estimate the activity in patients prior to release and then assess the dose likely to be received by members of the household and members of the public. Accordingly, the IAEA BSS [11] states that: “... a patient shall not be discharged from hospital before the activity of radioactive substances in the body falls below the level specified ... ”.
The Italian Decree 101/2020 pays great attention to the aspects related to the management of the patient undergoing therapy with radiopharmaceuticals.
In the case of 131I treatment, when the administered activity exceeds 600 MBq, it is necessary that the patient is treated in an inpatient setting; before release, a radiometric assessment must be conducted, in collaboration between the radiation protection expert and the medical physics expert, to determine the period of time after which the discharged patient can meet the recommendations referring to the dose constraints.
In all cases of administration for therapeutic purposes of radiopharmaceuticals and/or medical devices containing unsealed radioactive substances other than 131I, the need for an inpatient hospital stay is assessed by the medical specialist on an individual basis, after consulting the medical physics expert and the radiation protection expert, according to the indications provided by publication 94 of the ICRP [4], and is subject to the respect of the recommendations referring to the dose constraints, with particular reference to the protection of pregnant women and paediatric subjects.
2.2 A model for dose assessment
The dose received from the treated patient can be measured and evaluated. In both cases, the methods may be different but always require the introduction of more or less realistic approximations and models. The hypothesis generally considered for both measurements and evaluations is the point source approximation which for a patient is valid at distances of at least 2 m; IAEA, however, suggests considering at least 3 m [6], but actually this distance also depends on the size of the patient considered.
Therefore, as a first approximation, the dose rate due to the patient can be considered as due to a point source, for which the following relation applies:
where D is the dose rate; Q is the activity of the radionuclide at the time of release; \(\varGamma \), is the gamma constant for the given radionuclide [12]; r is the distance between the patient and the exposed subject.
Neglecting the biological decay, that is the body elimination of the radiopharmaceutical after the patient release, the dose to the exposed individual at the time t (corresponding to the duration of exposure) and distance r from the patient is then given by the relationship:
where \(T_{1/2}\) is the physical half-life of the radionuclide. Equation 2, similar to that reported in several US recommendations [13, 14], can be derived from the following integral:
As the dose to an individual likely to receive the highest dose is taken to be the dose to total decay, Eq. 2 becomes:
which represents the total dose to which a person placed for an infinite time (or in any case for a time much longer than the half-life of the administered radionuclide) is exposed at a mean distance r (at least 3 m) from the released patient. The physician has to estimate the occupancy factor, that is the fraction of time that an individual is near the patient [15], introducing a multiplicative factor E in Eq. 4, which becomes:
The US guidelines [14, 16] recommend considering an average distance of 1 m of the exposed individual from the patient and introducing an occupancy factor \(E = 0.25\) for radionuclides with a physical half-life \(T_{1/2}\) greater than 1 day, and E in the range 0.75–1.0 for radionuclides with \(T_{1/2}\) less than or equal to 1 day. This means that in the first case, the person who spends with the patient most of the time is estimated to be no more than 1 m from the patient no more than 25% of the time, and away from the patient for the remaining time. On the other hand, in the case of short-lived radionuclides, the time spent in close proximity to the patient is more relevant and long-term averaging cannot be assumed, as the dose to other persons could be a large fraction of the total dose from the radionuclide. In order to improve the point source approximation, the international standards suggest using \(r^{1.5}\) in the previous equations in place of \(r^{2}\) when \(r<3\) m [6]. In any case, if the patient is breast-feeding an infant or child, additional instructions from the medical staff may be necessary [16].
In the following sections, two case studies will be analysed:
-
Comforters and carers living under the same roof as the patient
-
Individual members of the public
2.2.1 Comforters and carers living under the same roof as the patient
Equation 4 can be applied to comforters and carers living with the patient assuming \(r=2\) m (average distance) and, conservatively, \(E=1\). Furthermore, since \(r<3\) m, \(r^{1.5}\) need to be assumed in Eq. 4 in place of \(r^{2}\) [6].
It is worth noticing that some therapies with radionuclides require repeated treatment cycles (e.g. treatment with 177Lu-DOTATATE, consisting in 4 cycles in 6 to 12-week intervals). In such cases, for each cycle, the dose constraint need to be divided by the overall number of treatment cycles, n. Therefore, imposing \(D(\infty )=(3/n\)) mSv, the activity \(Q_{0}^{cc}\) retained in the patient for each cycle at the time of discharge meets the release criteria when:
where \(\varGamma \) is the gamma constant for the given radionuclide in \(mSv \cdot h^{-1} \cdot MBq^{-1}\) at 1 m and \(T_{1/2}\) is the radionuclide half-life expressed in h.
2.2.2 Members of the public
For individual members of the public, considering shorter contact times, \(E=0.25\) can be safely assumed. Furthermore, as opposite to the previous scenario, repeated treatment cycles have no impact on the dose to the public since it is reasonable to assume that the treated patient is not likely to produce repeated exposure to the same individual of the population (Table 2).
Therefore, considering \(r=2\) m and imposing \(D(\infty )= 0,3 \) mSv, the activity \(Q_{0}^{mp}\) retained in the patient at the time of discharge meets the release criteria when:
2.3 A proposed realistic model using Microshield® code
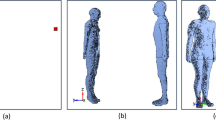
In order to ensure full compliance with the Italian regulatory framework, in the considered scenario, \(Q_{0}^{mp}\) (Eq. 7) could be used to determine the maximum departure activity in patients receiving radionuclide therapy. However, the above considered model is likely to provide far too conservative \(Q_{0}\) values when applied in the clinical practice and more realistic models should be used to prevent unnecessary stay time in hospital. In particular, a number of factors should be taken into account to derive more accurate \(Q_{0}\) values. As an example, the hypothesis of point-like radionuclide source is no longer true when the radiopharmaceutical is injected into the patient as the blood will distribute the radionuclide throughout the body. This process will ultimately end up in the build-up of the radionuclide only in certain tissues. Secondly, the radiation emitted by the radionuclide is to some extent attenuated by the body tissues. The aim of the present research is therefore to implement a more realistic model to account for the mentioned effects (Fig. 1).

Simulation of an extended volumetric source. A water cylinder having a height of 70 cm and a diameter of 30 cm uniformly filled with an activity of \(Q_{0}^\mathrm{Volume}\) was simulated using the Microshield® code. The G(r) factor introduced in Eq. 8 was calculated at a distance \(r=2\) m in the midplane of the cylinder
In the present study, the MicroShield® [17] code was used to derive a more accurate model for the emission of radioactivity by patients treated with radionuclides. MicroShield® is a comprehensive photon/gamma ray shielding and dose assessment software that is widely used for designing shields, estimating source strength from radiation measurements and to assess radiation exposure from a number of custom geometries. For the purpose of radiation protection of the public, in the present study, the representative patient was simulated as a water cylinder having a height of 70 cm and a diameter of 30 cm. The conservative (yet plausible) assumption is made that the radiopharmaceutical is distributed in the trunk of the individual. According to the new model, a geometric correction factor, G(r), needs to be introduced in Eq. 4 in order to take into account the biodistribution of the radionuclide into the human body and the attenuation of radiation from body tissues:
Of note, the G(r) factor depends on the different attenuation of radiation in the body, which is related to the gamma emission energy of the selected radionuclide. The G(r) factor accounts for the geometric extension of the source and reduces to \(G(r) = 1\) for point-like sources (for any r) and for extended volume sources when \(r\rightarrow \infty \).
For comforters and carers, considering \(E=1\), \(r=2\) m (see the dose constraint for comforters and carers in Table 1) with n treatment cycles, Eq. 8 can be solved for \(Q_{0}^\mathrm{Volume}\) to obtain maximum residual activity values in the patient at the time of discharge, according to the volumetric model:
For individuals of the population, considering again \(E=0.25\), \(r=2\) m and \(D(\infty )= 0,3\) mSv, Eq. 8 becomes:
It must be observed that when the treatment cycles are \(n<3\) \(\rightarrow \) \(Q_{0}^{\text {Volume-mp}} < Q_{0}^{\text {Volume-cc}}\). In such a scenario, releasing the patient when the activity retained in the body is calculated using Eq. 10 ensures that dose constrains for comforters and carers are met as well. If \(n>3\) Eq. 9 should be used instead to meet dose constraints even for individuals of the population.
For the sake of simplicity, in the following discussion, we will focus on the more general case \(n<3\) (i.e. \(Q_{0}^{\text {Volume-mp}} < Q_{0}^{\text {Volume-cc}}\)). Therefore, Eq. 10 will be used to ensure compliance with the regulatory dose constraints for both categories. However, the same approach can be applied for \(n>3\), taking Eq. 9 as a reference. A practical application of the case \(n>4\) is provided in Sect. 3.2.
2.4 Impact of the effective half-life, \(T_\mathrm{eff}\)
Physical half-life is defined as the period of time required to reduce the radioactivity level of a source to exactly one half its original value due solely to radioactive decay. Biological half-life is defined as the period of time required to reduce the activity to exactly one half its original value due solely to biological elimination. The effective half-life (\(T_\mathrm{eff}\)) is the actual half-life of a radiopharmaceutical in a given tissue, organ or whole body and is determined by a relationship including both the physical half life (\(T_{1/2}\)) and the biological half-life (\(T_\mathrm{bio}\)):
The biological half-life \(T_\mathrm{bio}\) is rather complex and is affected by many physiological factors among which hepatic and renal function, and level of hydration. Each individual organ in the body has its own \(T_\mathrm{bio}\) and the whole body also has a \(T_\mathrm{bio}\) representing the weighted average of the \(T_\mathrm{bio}\) of all internal organs and the blood pool. As a general rule, radionuclides can be removed from the body through urine and faeces. The excretion fractions of a great number of radionuclides after 24 h and 48 h in urine and faeces expressed as the ratio of excreted activity to the administered activity can be found in [18].
In light of the above, the algorithm proposed by Eq. 10 is conservative. In fact, the solely use of the physical half-life of the radionuclide is likely to produce overestimations of the residual activity in the patient’s body. A more realistic estimate of the residual activity can be obtained by replacing the physical half-life \(T_{1/2}\) in Eq. 10 with the effective half-life, \(T_\mathrm{eff}\):
Equation 12 holds true as long as a monoexponential total body time activity function can be applied, which is the case for many therapeutic radiopharmaceuticals [13].
3 Results
Table 3 shows, for selected radionuclides, the maximum residual activity in the patient at the time of discharge required to meet the dose constraints reported by the Italian regulatory framework according to Eqs. 7 and 10. With reference to Table 3, \(Q_{0}^{mp}\) is the activity calculated through Eq. 7 assuming a pointlike source and no attenuation from the patient. \(Q_{0}^\mathrm{Volume}\) is the activity calculated using Eq. 10, where the geometric factor G was assessed using MicroShield® and assuming a volumetric distribution of the source and radiation attenuation by the patient’s body. As expected, the G(r) factor shows an evident dependency from the radionuclide. For 131I, the volumetric models provides \(Q_{0}^\mathrm{Volume}\) = 318 MBq, which is in good agreement with the consensus value of 400 MBq of residual activity required to release a patient treated with 131I (see Sect. 1).
3.1 Determination of retained activity \(Q_{0}^\mathrm{Volume}\) from Ḣp(10) dose-rate measurements
At a clinical level, the retained activity \(Q_{0}^\mathrm{Volume}\) needs to be translated into dose-rate measurements performed using on-site radiation protection instrumentation, possibly calibrated in terms of personal dose equivalent rate, \(\overset{\cdot }{H}p(10)\). A simple protocol, which requires only a basic radiation detector, is reported in [6] and is recalled here for the sake of completeness. The steps involved are:
-
1.
Determining a fixed distance of at least 3 m at which the dose rate from the patient may be regularly measured. A good approach is to have fixed marks for both the patient and the measurement positions on the wall or the floor of the room.
-
2.
As soon as possible after administration, and certainly before any excretion, measuring the personal dose equivalent rate \(\overset{\cdot }{H}p(10)\) from the patient at this fixed distance. At any future times of interest, measuring the dose rate again at this fixed distance.
-
3.
At a clinical level, the patient release criterion can be determined using the following equation [6]:
$$\begin{aligned} \overset{\cdot }{H}p(10) < \overset{\cdot }{H}p(10)_{0} \frac{Q_{0}^\mathrm{Volume}}{Q_{inj}} \end{aligned}$$(13)where \(Q_{0}^\mathrm{Volume}\) is the retained activity at the time of measurement (Table 3), \(Q_{inj}\) is the administered activity, \(\overset{\cdot }{H}p(10)_{0}\) is the personal dose equivalent rate immediately after administration and \(\overset{\cdot }{H}p(10)\) is the personal dose equivalent rate at the time of measurement.
It is worth noticing that this is only an estimate, as the results may be influenced by redistribution of activity in the patient. However, the estimate is adequate for many purposes.
Table 4 shows the fraction of residual activity in the patient considering only the physical decay of the radionuclide. For each radionuclide, the fraction of residual activity is calculated as the ratio of the injected activity to the activity after 24 h and 48 h.
3.2 Case study: release of patients after treatment with 177Lu-DOTATATE
177Lu-DOTATATE is a radiolabeled somatostatin analog indicated for the treatment of somatostatin receptor-positive gastroenteropancreatic neuroendocrine tumours, including foregut, midgut, and hindgut neuroendocrine tumours in adults. It is administered to patients on an inpatient and outpatient basis, depending on the administered activity and the local regulatory requirements. Patients will typically undergo four therapy cycles each consisting of 7.4 GBq 177Lu-DOTATATE at 6–12-week intervals.
Following administration, these patients present an external radiation hazard due to the gamma emissions of 177Lu. 177Lu has a half-life of 6.647 days, decays by \(\beta \) emission to stable Hafnium (177Hf) with the most abundant \(\beta \) (79.3%) having a maximum energy of 0.497 MeV. The average beta energy is approximately 0.13 MeV. Low gamma energy is also emitted, at 113 keV (6.%) and 208 keV (11%).
The aim of this case study is to assess acceptable release criteria (in terms of residual activity) to ensure compliance with the Italian legislation. As discussed in Sect. 2.3, since \(n=4\) (4 overall treatment cycles), Eq. 9 should be used to assess the residual activity required to meet the dose constraints both for comforters and carers and for the population.
Assuming no biological removal of 177Lu-DOTATATE (i.e. only physical decay, \(T_{1/2}=\) 161 h), \(G(r)=0.5\) (Table 3) and a gamma constant \(\varGamma = 7.61 \times 10^{-6}\) mSv h\(^{-1}\) MBq\(^{-1}\) (Table 3), the proposed volumetric approach (Eq. 9) suggests that the residual activity at the time of discharge would be \(Q_{0}^{\text {Volume-cc}} = 3.4\) GBq. If only the physical decay of 177Lu is considered, the time of patient discharge should be set about 7 days post-administration. However, if biological removal of 177Lu-DOTATATE is considered, it can be shown that some outpatients may be discharged on the same day of admission. The retention of 177Lu within the body as a percentage of total administered activity can be modelled as a biexponential decay process. In particular, 177Lu-DOTATATE is primarily eliminated by kidneys, and the average excretion is about 50% after about 8 hours from administration (i.e retained activity 3.7 GBq), with some patients showing a retention rate in the order of 30% (i.e retained activity 1.1 GBq) after a few hours from the administration [19]. Conversely, it should be noted that some patients show a slow excretion rate, with about 50% of 177Lu-DOTATATE retained in the body after 24 hours from administration. For such patients, treatment on an outpatient basis may not be appropriate. A detailed study on radiation precautions for inpatient and outpatient 177Lu-DOTATATE peptide receptor radionuclide therapy of neuroendocrine tumours can be found in [19].
4 Discussion
The use of unsealed radionuclides for treatment of disease is common practice worldwide. Radionuclide therapies with unsealed sources rely on achieving a selective high concentration of nuclide in the target region, compared with that taken up by the surrounding tissues. Radionuclide treatments can be performed with either the patient admitted to hospital or on an outpatient basis. The criteria to determine which approach is better can vary considerably between countries as they are strongly related to the specific regulatory framework. As a general rule, safety issues for the patient, their family, associated carers, staff and the general public arise with either approach.
The new European Directive 2013/59/Euratom [9] lays down basic safety standards for protection against the risk arising from exposure to ionising radiation. According to the EU Directive 2013/59, carers and comforters are individuals knowingly and willingly incurring an exposure to ionising radiation by helping, other than as part of their occupation, in the support and comfort of individuals undergoing or having undergone medical exposure. Comforters and carers include, for example, members of the patient’s family, or visitors to the patient. Carers and comforters are subjected to medical exposure and, as such, dose constraints need to be applied (EU Directive 2013/59, Article 6, 1c)).
The Italian legislative implementation of the new European Commission Basic Safety Standards (BSS) resulted in the recent Legislative Decree 101/2020 [9] which established specific dose constraints for carers and comforters and the public (reported in Table 1). Furthermore, the recent Italian legislation reaffirms that for any RT treatment (with the exclusion of patients administered with less than 600 MBq of 131I), the decision to release a patient from hospital need be determined by the nuclear medicine physician on an individual basis, with the support of the local medical physics expert and radiation protection expert.
As a general rule, when the patient is hospitalised following RT, the people at risk of exposure include hospital staff, who may or may not be radiation workers or carers. As a consequence, this poses a significant problem. However, it is generally believed that it can be effectively managed with well-trained staff and appropriate facilities. On the other hand, once the patient has been discharged from the hospital, the groups at risk include members of the patient’s family, including children, and carers; they may also include neighbours, visitors to the household, and other people encountered in public places, on public transport or at public events, and finally the general public.
The general approach of international guidelines on this subject is to relate the activity in the patient at the time of discharge to exposure to the public and relatives, releasing her/him when the retained activity drops below specific values determined by selected dosimetric models [6, 10, 16].
The present work allows to evaluate release criteria on the basis of general considerations and assumptions (e.g. radiation attenuation by the patient body, distance from individuals, occupancy factors) aimed at complying with regulatory dose constraints. According to the principle of optimisation of radiation protection, the proposed approach allows a more accurate yet less conservative assessment and therefore the release of the patient with higher residual activity. Where clinical data relating to treatment with a specific radiopharmaceutical are available, it is always necessary to refer to them, modifying accordingly the model described here.
Particular attention must be paid to the choice of release criteria in patients undergoing repeated treatment cycles. In this case, the dose constraints need to be met considering the total number of cycles. A case study on this issue is proposed in Sect. 3.2, where release criteria are evaluated for radionuclide treatment with 177Lu-DOTATATE. Some countries allow for 177Lu-DOTATATE therapy on an outpatient basis. Work by Calais and Turner [20] has shown that outpatient therapy is acceptable within Australia’s regulatory framework where this is routinely carried out, and Olmstead et al. demonstrated the safety and feasibility of an outpatient protocol in Canada [21]. Other countries require inpatient isolation after 177Lu-DOTATATE administration. As a general rule, precautions and restrictions are necessary to limit radiation dose to members of patients’ household and the public. In a recent study, Levart and colleagues estimated the equivalent dose per cycle to close relatives and members of the public for inpatient and outpatient 177Lu-DOTATATE administrations resulting from no restriction on contact with patient [19]. In their study, the authors found that if no contact restrictions are put in place, the cumulative dose per treatment cycle received by family members and the public from patients undergoing 177Lu-DOTATATE are likely to exceed the established constraints for all groups, thereby demonstrating that precautions are necessary when 177Lu-DOTATATE therapy patients leave the hospital. However, these results should be interpreted with caution in the context of the Italian regulatory framework as they were derived against the backdrop of UK legislation (i.e. dose received by patients’ family members less than 5 mSv in 5 years and members of the public less than 1 mSv per year).
5 Conclusion
The decision to hospitalise or release a patient should be determined on an individual basis. In addition to residual activity in the patient, the decision should take many other factors into account including the patients’ wishes, family situation, occupational and public exposures, the presence of children, cost, and environmental factors [22].
The release approach described by Eqs. 9 and 10 has the potential to be used in the clinical practice straight away, provided that reliable assumptions and parameters are used in the model. Most importantly, it is recommended that release of patients should be based on their family situation and the possibility to effectively put in place time and behavioural restrictions suggested by the physician at the moment of release.
Change history
18 November 2021
A Correction to this paper has been published: https://doi.org/10.1140/epjp/s13360-021-02139-8
References
C.D. Kaur, K.K Mishra, A. Sahu, R. Panik, P. Kashyap, S.P. Mishra, A. Kumar, Theranostics: New Era in Nuclear Medicine and Radiopharmaceuticals, Medical Isotopes, Syed Ali Raza Naqvi and Muhammad Babar Imrani, IntechOpen. https://doi.org/10.5772/intechopen.91868. Available from: https://www.intechopen.com/books/medical-isotopes/theranostics-new-era-in-nuclear-medicine-and-radiopharmaceuticals
G. Sgouros, L. Bodei, M. McDevitt, J. Nedrow, Author Correction: Radiopharmaceutical therapy in cancer: clinical advances and challenges. Nat. Rev. Drug Discov. 19(11), 819–819 (2020). https://doi.org/10.1038/s41573-020-0085-5
International Atomic Energy Agency, Trends in Radiopharmaceuticals (ISTR-2019), Proceedings of an International Symposium, Vienna, Austria, 28 October–1 November 2019
ICRP, Release of patients after therapy with unsealed radionuclides. ICRP Publication 94. (ICRP, 2004)
European Commission, Radiation Protection Following Iodine-131 Therapy (Exposures Due to Out-Patients or Discharged In-Patients), Radiation Protection 97 (European Commission, Luxembourg, 1998)
International Atomic Energy Agency, Release of patients after radionuclide therapy, Safety Reports Series No. 63. (IAEA, Vienna 2009)
H. Zhang, L. Jiao, S. Cui, L. Wang, J. Tan, G. Zhang, Y. He, S. Ruan, S. Fan, W. Zhang, The study of external dose rate and retained body activity of patients receiving 131I therapy for differentiated thyroid carcinoma, Int J Environ Res Public Health. 11(10), 10991–11003 (2014)
European Council Directive 2013/59/Euratom on basic safety standards for protection against the dangers arising from exposure to ionising radiation and repealing Directives 89/618/Euratom, 90/641/Euratom, 96/29/Euratom, 97/43/Euratom and 2003/122/Euratom. OJ of the EU. L13; 57: 1–73 (2014)
Legislative Decree 31 July 2020 No. 101 implementing Directive 2013/59/Euratom – “Attuazione della direttiva 2013/59/Euratom, che stabilisce norme fondamentali di sicurezza relative alla protezione contro i pericoli derivanti dall–esposizione alle radiazioni ionizzanti, e che abroga le direttive 89/618/Euratom, 90/641/Euratom, 96/29/Euratom, 97/43/Euratom e 2003/122/Euratom e riordino della normativa di settore in attuazione dell–articolo 20, comma 1, lettera a), della legge 4 ottobre 2019, n. 117– . G.U. n. 201 del 12/08/2020, Supplemento ordinario n. 29/L
M. Singleton, C. Griffiths, G. Morrison, T. Soanes, Dose constraints for comforters and carers, RR155 (HSE, 2003)
International Atomic Energy Agency, International Basic Safety Standards for protection against ionizing radiation and for the safety of radiation sources, Safety Series No. 115 (IAEA, Vienna, 1996)
D.S. Smith, M.G. Stabin, Exposure rate constants and lead shielding values for over 1,100 radionuclides. Health Phys. 102(3), 271–291 (2012). https://doi.org/10.1097/hp.0b013e318235153a
NCRP report n. 155 (Bethesda, 2006)
US Nuclear Regulatory Commission, NUREG-1556, Volume 9. Rev. 3 (2019)
L.R. Coover, E.B. Silberstein, P.J. Kuhn, M.W. Graves, J. Nucl. Med. 41, 11 (2000)
US Nuclear Regulatory Commission, Regulatory Guide 8.39 (1997)
MicroShield code, Grove Software, radiationsoftware.com (2012)
ICRP OIR Data Viewer for Pub. 134, Pub. 137 and Pub. 141 v4010419, 2019 July 30
D. Levart, E. Kalogianni, B. Corcoran et al., Radiation precautions for inpatient and outpatient 177Lu-DOTATATE peptide receptor radionuclide therapy of neuroendocrine tumours. EJNMMI Phys. 6, 7 (2019). https://doi.org/10.1186/s40658-019-0243-1
P.J. Calais, J.H. Turner, Radiation safety of outpatient 177Lu-octreotate radiopeptide therapy of neuroendocrine tumors. Ann. Nucl. Med. 28, 531–9 (2014)
C. Olmstead, K. Cruz, R. Stodilka, P. Zabel, R. Wolfson, Quantifying public radiation exposure related to lutetium-177 octreotate therapy for the development of a safe outpatient treatment protocol. Nucl. Med. Commun. 36, 129–34 (2015)
G.M. Contessa, S.A. De Crescenzo, P. Rossi, The application of the optimization principle in the Italian and European context. Radioprotection 56(3), 199–204 (2021). https://doi.org/10.1051/radiopro/2021019
Author information
Authors and Affiliations
Corresponding author
Additional information
The original online version of this article was revised due to a wrong affiliation for the authors Gian Marco Contessa and Sandro Sandri.
Rights and permissions
About this article

Cite this article
D’Arienzo, M., Contessa, G.M., Sandri, S. et al. Management of patients receiving radionuclide therapy with unsealed radionuclides: a proposed approach to the definition of release criteria in Italy. Eur. Phys. J. Plus 136, 1055 (2021). https://doi.org/10.1140/epjp/s13360-021-01735-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1140/epjp/s13360-021-01735-y