
Abstract
Purpose
To provide 5-year time trends in prevalence and demographic, substance use, and mental health correlates of compulsive exercise among a national sample of college men and women.
Methods
We analyzed 4 academic survey years (2016–2020; N = 8251) of the national (USA) Healthy Minds Study. Compulsive exercise was measured by self-report of any occurrence of “compulsive” exercise in the past 4 weeks. Unadjusted prevalence of compulsive exercise in the past 4 weeks was estimated across the 4 survey years by sex. Multiple logistic regression analyses were conducted among the pooled sample and stratified by sex to estimate the associations between compulsive exercise in the past 4 weeks and demographic, substance use, and mental health correlates.
Results
Among the pooled sample, 11% (95% confidence interval [CI] 9.60–12.42%) of men and 17% (95% CI 15.86–18.24%) of women reported compulsive exercise in the past 4 weeks. Prevalence across the 4 survey years remained stable among men and women. Higher body mass index was associated with greater odds of any compulsive exercise in the past 4 weeks among men, while any sports participation was associated with greater odds of any compulsive exercise in the past 4 weeks among women. Compulsive exercise in the past 4 weeks was associated with greater odds of all mental health symptoms and illicit drug use among men and women, and higher odds of alcohol use among women.
Conclusion
Compulsive exercise is relatively common among college men and women and is associated with substance use behaviors and poor mental health symptoms.
Level of Evidence
V, cross-sectional descriptive study
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Exercise is associated with positive physical health indices [1, 2] and has been shown to be positively associated with improved mental health [3,4,5,6,7]. However, for some, regular exercise can take on compulsive qualities, which portend significant adverse effects. Despite inconsistencies in formal terminology (e.g., “excessive” vs. “compulsive”) and the lack of a formal definition [8, 9], it has been proposed that compulsive exercise encompasses several key patterns, including that the individual feels compelled to perform excessive exercise, the exercise is completed to avoid distress associated with “missing a workout”, the exercise is time consuming, the exercise continues despite injuries, the exercise impairs with social functioning, the exercise routines are intense and vigourous [10], and there is a marked obsessive quality to the exercise [11]. Furthermore, compulsive exercise is commonly used as a compensatory behavior, that is, to burn calories and/or alter the body as part of disordered eating patterns [8]. It is within this context that we frame compulsive exercise in this study.
Overall, research assessing the prevalence of compulsive exercise among non-clinical samples is lacking. This is particularly true among college students. However, research using the Eating Disorder Examination Questionnaire (EDE-Q) [12], a widely used and validated measure of eating disorder psychopathology, has shown that between 31 and 48% of both undergraduate men and women [13,14,15] reported any occurrence of “driven” or “compulsive” exercise for weight loss or body shape change in the past 4 weeks at the time of the study. While it is clear that compulsive exercise occurs at relatively high prevalence among undergraduate students, according to the EDE-Q conceptualization, existing research is limited by the overall small sample sizes (for community-based studies), ranging from 404 to 1158 participants [13,14,15]. This limits the generalizability of such research findings, as well as precludes us from gleaning a comprehensive understanding of how compulsive exercise behavior has changed over time. The compulsive exercise item in the EDE-Q has been shown to display high concurrent validity with the Compulsive Exercise Test, the Commitment to Exercise Scale, and the Exercise Beliefs Questionnaire [16], indicating that it is able to capture the emotional and psychological constructs of compulsive exercise using a single item. This presents a unique strength of the compulsive exercise item in the EDE-Q as it can be easily incorporated into large-scale surveys to capture this problematic behavior among a large, non-clinical sample, as well as assess changes over time.
Among college students, engaging in compulsive exercise is associated with greater risk of a concurrent eating disorder [15], and compulsive exercise is broadly conceptualized as a central component in the development and maintenance of eating disorder psychopathology [8, 9]. Thus, it is not surprising that this behavior is common among individuals who experience eating disorders. For example, depending on the sample population, measure, and chosen cut-offs, prevalence of compulsive exercise ranges from 20 to 81% among individuals with eating disorders [10, 17,18,19]. This underscores the potentially pathological nature of compulsive exercise as it relates to eating disorder psychopathology.
In addition to its relationship with eating disorders, among the general population and individuals with eating disorders, compulsive exercise, as opposed to exercise frequency per se, is associated with several adverse health and social outcomes. For example, compulsive exercise is associated with interference with social and occupational functioning, increased anxiety and depression symptoms, substance use, medical complications (e.g., bradycardia), injury (e.g., stress fractures), and increased suicidality [10, 20,21,22]. These social and health correlates of compulsive exercise may be compounded among adolescent and young adult college students who are already encountering significant challenges and engaging in several life transitions [23]. For example, it is well established that this age group commonly experiences body dissatisfaction [24], eating disorders [25], dieting, and disordered eating [26], is particularly susceptible to poor mental health (e.g., depression, anxiety, suicidal ideation, non-suicidal self-injury) [27], and may engage in regular substance use [28, 29]. Thus, additional research is warranted to better characterize and understand the overlapping nature of compulsive exercise and substance use and mental health symptoms among young people.
Several gaps exist in the knowledge base on compulsive exercise among college students. These include identifying the trends in prevalence over time, identifying the demographic distribution for engaging in compulsive exercise, and identifying the substance use behaviors and mental health symptoms associated with compulsive exercise. Given these gaps, this study has three aims. First, we aim to estimate the prevalence of compulsive exercise among college men and women across four sequential cross-sectional annual cohorts of a large nationwide survey among college students in the United States. Second, we aim to estimate the demographic correlates of compulsive exercise among the pooled sample of college men and women. Lastly, we aim to estimate the associations between compulsive exercise and substance use behaviors and mental health symptoms among the pooled sample of college men and women.
Methods
Cross-sectional data from 4 academic survey years (2016–2017, 2017–2018, 2018–2019, 2019–2020; N = 8251) of the national (USA) Healthy Minds Study (HMS) were analyzed. HMS is an annual survey of several health and social domains among college student participants. Colleges and universities voluntarily elect to participate in HMS. At institutions with ≥ 4000 students, 4000 students were randomly invited to participate in the survey; at institutions with < 4000 students, all students were invited. To be eligible to participate, students must have been at least 18 years old. Students were invited to participate via email and the survey was administered online via Qualtrics. Students were incentivized to participate by using a prize drawing of Amazon gift cards. Students provided informed consent prior to participating. HMS is conducted out of the University of Michigan and Boston University and was approved by the Health Sciences and Behavioral Sciences Institutional Review Board at the University of Michigan and all participating institutions [30].
Measures
Compulsive exercise
Compulsive exercise was measured using the question: “Over the past 4 weeks (28 days), how many times have you exercised in a ‘driven’ or ‘compulsive’ way as a means of controlling your weight, shape or amount of fat, or to burn off calories?” This question is part of the widely used Eating Disorder Examination Questionnaire (EDE-Q) [12]. Responses ranged from 0 to 28 with a mean of 1.08, standard deviation of 3.63, median of 0, and skewness of 4.52. Given the significant positive skewness of this variable, responses were dichotomized to zero (0) times and one (1) or more times. This item has frequently been dichotomized in prior research to determine the prevalence of any occurrence of compulsive exercise [13,14,15, 31,32,33].
Substance use behaviors
Cigarette use was measured using the question: “Over the past 30 days, about how many cigarettes did you smoke per day?” Response options included: “0 cigarettes;” “Less than 1 cigarette;” “1 to 5 cigarettes;” “About one-half pack;” and “1 or more packs.” Responses were dichotomized to zero (0) cigarette use and any cigarette use, as has regularly been done in prior research [34, 35].
Illicit drug use was measured using the question, “Over the past 30 days, have you used any of the following drugs?” Potential response options included: “Marijuana;” “Cocaine (any form, including crack, powder, and freebase);” “Heroin;” “Methamphetamines (also known as speed, crystal meth, or ice);” “Other stimulants (such as Ritalin, Adderall) without a prescription or more than prescribed;” “Opioid pain relievers (such as Vicodin, OxyContin, Percocet, Demerol, Dilaudid, codeine, hydrocodone, methadone, morphine) without a prescription or more than prescribed;” “Ecstasy;” and “Benzodiazepines.” Given the multitude of response options, responses were dichotomized to no illicit drug use and any illicit drug use, as has been done in prior research [36, 37].
Alcohol use was measured using the question: “Over the past 2 weeks, did you drink alcohol?” A dichotomous “yes” or “no” response was available.
Mental health symptoms
Depression was measured using the Patient Health Questionnaire-9 (PHQ-9). This screening tool is based on the nine Diagnostic and Statistical Manual for Mental Disorders (DSM)-IV criteria for a major depressive episode [38, 39]. Responses for each question included: “Not at all;” “Several days;” “More than half the days;” and “Nearly every day”. Scores ranged from 0–27 with higher scores indicating greater depression symptoms. Internal reliability of the PHQ-9 among the sample was good with α = 0.88. This variable was converted into a dichotomous variable with participants who screened negative (scores 0–9) and those who screened positive (10–27) for depression using a previously established clinical cut-point [38, 39]. A cut-off score of ≥ 10 has been shown to maximize sensitivity and specificity among diverse samples [40].
Anxiety was measured using the Generalized Anxiety Disorder 7-Item (GAD-7). This screening tool was developed to reflect all components of the DSM-IV criteria for generalized anxiety disorder [41]. Responses for each question included: “Not at all;” “Several days;” “More than half the days;” and “Nearly every day”. Scores ranged from 0–21 with higher scores indicating greater anxiety symptoms. Internal reliability of the GAD-7 among the sample was excellent with α = 0.91. This variable was converted into a dichotomous variable with participants who screened negative (scores 0–9) and those who screened positive (10–21) for anxiety using a previously established clinical cut-point [41]. A cut-off score of ≥ 10 has been shown to have strong psychometric properties among college men and women [42].
Eating disorder risk was measured using the 5-item SCOFF questionnaire [43]. Responses for each question included: “yes” or “no”. Scores ranged from 0–5 with a positive eating disorder screen indicated by a score of two (2) or more “yes” responses [43, 44]. This cut-off score has been shown to have a sensitivity of 70–100% and specificity of 73–94% for anorexia nervosa, bulimia nervosa, and binge-eating disorder [43,44,45].
Suicidal ideation was measured using the question: “In the past year, did you ever seriously think about attempting suicide?” A dichotomous “yes” or “no” response was available.
Non-suicidal self-injury (NSSI) was measured using the question: “In the past year, have you ever done any of the following intentionally?” Potential responses include: “Cut myself;” “Burned myself;” “Punched or banged myself;” “Scratched myself;” “Pulled my hair;” “Bit myself;” “Interfered with a wound healing;” “Carved words of symbols into my skin;” “Rubbed sharp objects into my skin;” “Punched or banged an object to hurt myself;” and “Other.” Given the multitude of response options, responses were dichotomized to no NSSI and any NSSI, as has been done in prior research [27, 46].
Demographic variables
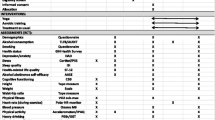
Demographic variables included self-reported age (18–20 years; 21–23 years; 24–26 years; 27 years and older), race/ethnicity (White or Caucasian, non-Hispanic, non-Arab; Black or African American, non-Hispanic; Hispanic/Latino/a; Asian or Asian American; Arab/Middle Eastern or Arab American; American Indian, Alaskan Native, Native Hawaiian or Pacific Islander; Other race/ethnicity; More than one race/ethnicity), sexual orientation (Heterosexual; Gay or lesbian; Bisexual; Queer, questioning, or other), highest parental education (Some college or less; Associate’s or Bachelor’s degree; Graduate degree), and any sports participation (intercollegiate varsity; club; intermural). Body mass index (BMI; kg/m2) was calculated from self-reported height and weight.
Statistical Analysis
Descriptive analyses were conducted to characterize the pooled sample of all 4 survey years. The unadjusted prevalence of any compulsive exercise in the past 4 weeks was estimated across and within the 4 survey years (Pearson chi-square test). Logistic regressions analyses were conducted among the pooled sample of all 4 survey years to estimate the associations between the demographic variables (independent variables: age, BMI, race/ethnicity, sexual orientation, parental education, any sports participation), survey year, and any compulsive exercise in the past 4 weeks (dependent variable). Eight (8) logistic regression analyses were conducted among the pooled sample of all 4 survey years to estimate the associations between any compulsive exercise in the past 4 weeks (independent variable) and substance use behaviors (cigarette use, illicit drug use, alcohol use) and mental health symptoms (depression screen, anxiety screen, eating disorder screen, suicidal ideation, NSSI) as the dependent variables while adjusting for age, BMI, race/ethnicity, sexual orientation, highest parental education, any sports participation, and survey year. Sensitivity analyses were conducted using compulsive exercise as a continuous variable for aims two and three using both logistic regression and Poisson regression analyses. All analyses were stratified by sex given previously documented differences in purpose and presentation of compulsive exercise among men and women [21, 47,48,49,50]. Statistical analyses included preconstructed sample weighting to adjust for nonresponse bias. Sample weights were constructed based on gender, race/ethnicity, academic level, and grade point average. Participants with underrepresented demographic characteristics were assigned greater sample weights [30]. The Benjamini–Hochberg procedure was used to adjust for false discovery given the number of statistical tests [51]. All analyses were conducted in 2021 using Stata 16.1.
Results
Table 1 displays all of the sample demographic characteristics and descriptive statistics. Among the pooled sample of all 4 survey years (N = 8251), 67.61% of participants were women. Among both men and women, the majority of participants were between the ages of 18 and 20 years. Among both men and women, nearly two-thirds of the participants identified as White or Caucasian, non-Hispanic, non-Arab, the majority of men (86.22%) and women (80.92%) identified as heterosexual, and most participants reported the highest level of parental education of Associate’s or Bachelor’s degree or more. More than a quarter (28.23%) of men and 17.86% of women reported some level of sports participation.
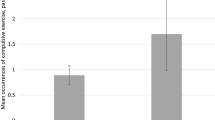
Among the pooled sample of participants, any occurrence of compulsive exercise in the past 4 weeks was more common among women (17.05%, 95% confidence interval [CI] 15.86–18.24%) than men (11.01%, 95% CI 9.60–12.42%); p < 0.001; Table 1). In unadjusted analyses, there were no significant changes in the prevalence of any compulsive exercise in the past 4 weeks over the 4 survey years (men: p = 0.25; women: p = 0.08; Fig. 1).

Prevalence (%) of Any Compulsive Exercise (≥ 1 time) in the Past 4 Weeks by Sex and Healthy Minds Study Survey Year. Note: Preconstructed nonresponse sample weighting was applied to all analyses. Pearson chi-square test: Men: p = 0.25; Women: p = 0.08
Results from logistic regression analyses (Table 2) revealed several significant associations between the demographic correlates and any compulsive exercise in the past 4 weeks. Among men, higher BMI was associated with greater odds of reporting any compulsive exercise in the past 4 weeks. Among women, ages 21–23 years, 24–26 years, and 27 years and older was associated with lower odds of reporting any compulsive exercise in the past 4 weeks. Among women, any sports participation was associated with higher odds of reporting any compulsive exercise in the past 4 weeks. In sensitivity analyses (Supplement Table 1), higher BMI was no longer significantly associated with reporting any compulsive exercise in the past 4 weeks among men. Among women, the effects for age and sports participation remained significant, and in addition, an effect was observed for women identifying as Asian or Asian American to have lower odds of reporting any compulsive exercise in the past 4 weeks.
Results from multiple logistic regression analyses (Table 3) revealed significant associations between any compulsive exercise in the past 4 weeks and substance use behaviors and mental health symptoms. Among men, reporting any compulsive exercise in the past 4 weeks was associated with higher odds of any illicit drug use in the past 30 days, a positive depression screen, a positive anxiety screen, a positive eating disorder screen, self-reported suicidal ideation in the past 12 months, and any self-reported NSSI in the past 12 months, while adjusting for the demographic variables. Reporting any compulsive exercise in the past 4 weeks was not associated with any cigarette use in the past 30 days and alcohol use in the past 2 weeks. In sensitivity analyses (Supplement Table 2 and 3), all variables remained significantly associated with any compulsive exercise in the past 4 weeks with the exception of suicidal ideation in the past 12 months.
Among women, reporting any compulsive exercise in the past 4 weeks was associated with higher odds of any illicit drug use in the past 30 days, alcohol use in the past 2 weeks, a positive depression screen, a positive anxiety screen, a positive eating disorder screen, self-reported suicidal ideation in the past 12 months, and any self-reported NSSI in the past 12 months, while adjusting for the demographic variables. Reporting any compulsive exercise in the past 4 weeks was not associated with any cigarette use in the past 30 days. In sensitivity analyses (Supplement Table 2 and 3), all variables remained significantly associated with any compulsive exercise in the past 4 weeks with the inclusion of any cigarette smoking in the past 30 days.
Discussion
The overarching aim of this study was to provide a contemporary overview of the 5-year trends in prevalence and demographic, substance use, and mental health correlates of compulsive exercise among college men and women. Specifically, our first aim was to estimate the prevalence of compulsive exercise across 4 survey years; our second aim was to estimate the demographic correlates of compulsive exercise; and our third aim was to estimate the associations between compulsive exercise and substance use behaviors and mental health symptoms. Related to our first aim, results showed that prevalence of any occurrence of compulsive exercise in the past 4 weeks remained relatively stable across the survey years for both men and women, and one in ten men and nearly one in five women reported any compulsive exercise in the past 4 weeks from the 2016 to 2020 survey years. These results are slightly lower than prior research using the EDE-Q among college men and women [13,14,15], which may be the result of this study including a larger sample size and both undergraduate and graduate students.
Results related to our second aim showed that, among women, older participants, compared to 18–20-year-olds, had lower odds of reporting any compulsive exercise in the past 4 weeks. It is possible that attempts to alter one’s body via compulsive exercise slightly decrease during the transition through young adulthood (e.g., 18–30 years old) [23]. This is somewhat divergent from research that has shown that body dissatisfaction, a major driver of compulsive exercise [19], continues to be common throughout adolescence into young adulthood among women [24].
Among men, higher BMI was associated with any compulsive exercise in the past 4 weeks. Compulsive exercise is likely used within the context of weight loss attempts [1, 2] or body shape alteration. Exercise regimens may become compulsive, should weight loss efforts be unsuccessful or difficult to maintain, among those with higher BMIs as these individuals seek to achieve an ideal body, or a shape and weight that are unsustainable through healthy means for their bodies. Among men, compulsive exercise may be used to pursue the muscular ideal, which is also associated with higher BMI, and thus may also contribute to explaining the relationship found here with higher weight [48, 52, 53]. Furthermore, higher BMI may reflect the effects of dieting, disordered eating behaviors, and weight loss attempts over time, where repetitive patterns can lead to an increase in BMI [54]. In this way, the relationship may also be explained by body-change efforts having led to increases in BMI over time. However, these competing explanations are difficult to tease out given the cross-sectional nature of the data, indicating the need for future longitudinal research. This may be exemplified by the lack of significant relationship between BMI and compulsive exercise when using compulsive exercise as a continuous variable.
Among women, those who reported any sports participation, that is involvement in intercollegiate varsity, club, or intermural sports, revealed higher odds of any compulsive exercise in the past 4 weeks. This is not surprising as the prevalence of eating disorders is high among athletes [55, 56], with compulsive exercise being a common behavior [21, 57, 58]. This result emphasizes the continued need for prevention, intervention, and research on eating disorder behaviors among athletes.
Regarding our final aim, several significant associations emerged between compulsive exercise and substance use behaviors and mental health symptoms. Among both men and women, reporting any compulsive exercise in the past 4 weeks was associated with higher odds of illicit drug use. The use of illicit drugs (e.g., stimulants) may be a means to increase endurance and performance for compulsive exercise [59], and, in general, illicit drug use is common among individuals who experience eating disorders [37, 60], and engage in disordered eating behaviors [61]. Additionally, both compulsive exercise [10] and illicit drug use [62] may be a means to regulate emotions. Among women, reporting any compulsive exercise in the past 4 weeks was associated with higher odds of any alcohol use in the past two weeks. This may align with Food and Alcohol Disturbance, colloquially known as “drunkorexia”, which describes the use of compensatory behaviors (e.g., compulsive exercise) in preparation for or in response to alcohol use (e.g., to counter the planned ingestion of calories) [63,64,65]. The lack of association between any compulsive exercise in the past 4 weeks and any cigarette use in the past 30 days is not surprising given that cigarette use may reduce the capacity to exercise in a “driven” and “compulsive” manner. However, in sensitivity analyses, any cigarette use in the past 30 days was significantly associated with a greater number of occurrences of compulsive exercise among women. This is a cause of concern as both cigarette use and compulsive exercise may adversely impact the cardiovascular and pulmonary systems of the body [21, 66].
Among both men and women, reporting any compulsive exercise in the past 4 weeks was associated with higher odds of all five mental health symptoms assessed, including a positive depression screen, a positive anxiety screen, a positive eating disorder screen, self-reported suicidal ideation in the past 12 months, and self-reported NSSI in the past 12 months. Both men and women who reported any compulsive exercise in the past 4 weeks had greater odds of exhibiting depression and anxiety symptoms, both of which commonly co-occur with eating disorders [60]. Depression symptoms may also be present if compulsive exercise interferes with social functioning (e.g., reduced socialization, hindered academic achievement, poor job performance) [10]. However, and somewhat contradictory, depression is widely known to be associated with lethargy [67], which would likely impede compulsive exercise. Among men and women, reporting any compulsive exercise in the past 4 weeks was associated with higher odds of self-reported suicidal ideation in the past 12 months. Prior research has shown that over-exercising is associated with suicidal ideation among individuals with eating disorders, and that over-exercising is a contributor to an acquired capability for suicide given an increase in pain insensitivity [22]. Unexpectedly, compulsive exercise was no longer significantly associated with self-reported suicidal ideation in the past 12 months among men in sensitivity analyses that considered compulsive exercise as continuous. This is a curious finding as it may be expected that a greater number of occurrences of compulsive exercise would increase the likelihood of suicidal ideation due to the level of impairment associated with compulsive exercise. However, it may be that the heightened risk for suicidal ideation occurs when any compulsive exercise is present. These divergent findings highlight the need for future research to further explore the relationship between compulsive exercise and suicidal ideation. Among men and women, reporting any compulsive exercise in the past 4 weeks was associated with higher odds of any self-reported NSSI in the past 12 months. It may be that compulsive exercise is a form of NSSI, and both compulsive exercise and NSSI may be mechanisms for emotion regulation [10, 68] or self-punishment [69]. Lastly, it is not surprising that, among both men and women, any compulsive exercise in the past 4 weeks was associated with higher odds of a positive eating disorder screen. Research has consistently shown that individuals with diagnosed eating disorders and disordered eating behaviors use compulsive exercise as a compensatory behavior [10, 17, 19,20,21, 70,71,72]. In addition to constituting a behavior designed to modify appearance, compulsive exercise and other disordered eating behaviors likely serve similar emotion regulation functions [8, 73]. Importantly, individuals with eating disorders who also engage in compulsive exercise may experience medical complications [10, 21], and compulsive exercise is one of the last symptoms to attenuate when treating eating disorders, highlighting the centrality of compulsive exercise with eating disorders [73].
Limitations
Despite the important findings in this study, several limitations are important to note. First, HMS is a cross-sectional survey, which does not allow for causal inference; thus, we do not know whether compulsive exercise temporally predicts any of the substance use and mental health outcomes shown here. However, it is highly plausible that these associations are bidirectional in nature. Future research is needed to further disentangle these temporal relationships. Furthermore, we dichotomized the substance use and mental health measures in this study in accordance with the clinical indicators of these behaviors and mental health disorders, as well as prior research; however, there may be nuances in the severity of substance use behaviors and poor mental health symptoms associated with compulsive exercise. Future research is needed to identify these nuances. Second, HMS is not a cohort study. Thus, we are unable to assess how compulsive exercise changes over time among a single group of college students. However, the strength in this design is the ability to examine time trends in one population. Third, although the current analyses included a number of control variables, other unmeasured confounders may exist. Fourth, given the response rates for each survey year (2016–2017: 23%; 2017–2018: 23%; 2018–2019: 16%; Fall 2019: 16%; Spring 2020: 13%), there is a threat of nonresponse bias. However, to mitigate this, we utilized preconstructed sample weighting. Additionally, a high response rate does not equate to less nonresponse bias [74], and surveys with large sampling frames, including HMS, are likely to obtain dependable results, despite lower response rates [75]. Fifth, the measures are based on self-report, which may increase social desirability bias, and we were limited to a single item measure of compulsive exercise measure. However, the EDE-Q compulsive exercise item has been shown to be highly correlated with the measurement of compulsive exercise via the Compulsive Exercise Test [16]. Further research should consider including multiple measures of compulsive exercise to more broadly assess this problematic behavior among a large sample of participants. Participants were also assumed to understand and discern what “driven” or “compulsive” exercise is, as well as exercise to control “weight, shape or amount of fat, or to burn off calories.” This leaves some room for varying interpretations of this construct, particularly among college men who may not be engaging in compulsive exercise for these specific reasons and are instead exercising to increase muscularity [49, 76]. Strengths of this study include the use of a large and diverse sample of college students in the general population, the use of multiple survey years, and eight substance use and mental health measures. Additionally, we conducted sensitivity analyses that provided additional context and support for results.
Implications
Exercise has been shown to have favorable health effects [1, 2], including the reduction of depression and anxiety symptoms [3,4,5], the prevention of substance use disorder [6], and the overall improvement of mental health [7]. However, the results from this study highlight the potential adverse substance use behaviors and mental health symptoms that may arise should exercise become compulsive. Therefore, while exercise remains a positive and appropriate recommendation for clinical professionals, specifically those on college campuses, to provide to clients, continued monitoring of exercise is warranted. This is particularly relevant as our finding show that even one occurrence of compulsive exercise is associated with substance use behaviors and poor mental health symptoms. Furthermore, clinical professionals should assess quality, frequency, intensity, duration, and motivation of exercise behaviors among college students to appropriately identify compulsive exercise and associated substance use behaviors and mental health symptoms, particularly eating disorders, among college students.
Conclusion
This study showed that prevalence of any compulsive exercise among college students has remained relatively stable across 4 survey years from 2016 to 2020, and 11% of college men and 17% of college women reported engaging in compulsive exercise over the course of the past 4 weeks. Reporting any compulsive exercise over the past 4 weeks was associated with sports participation among women and higher BMI among men, indicating unique demographic characteristics associated with this behavior. Lastly, among both men and women, any compulsive exercise over the past 4 weeks was strongly associated with substance use behaviors and poor mental health symptoms. These results provide contemporary prevalence trends of compulsive exercise among college students and highlight how compulsive exercise may form part of a constellation of unhealthy and risky behaviors including significant substance use behaviors and be associated with poor mental health.
What is already known on this subject?
Compulsive exercise has been shown to be common among small samples of undergraduate college students and is associated with eating disorder psychopathology.
What this study adds?
This study shows the 5-year trends of compulsive exercise among a large, national sample of college students. Over 11% of men and 17% of women report any compulsive exercise in the past 4 weeks. Compulsive exercise is associated with both substance use behaviors and poor mental health symptoms, indicating a need for prevention and intervention programming of this common behavior.
Availability of data and material
The Healthy Minds Study is available to researchers. Please visit http://healthymindsnetwork.org for more information.
References
Obert J, Pearlman M, Obert L, Chapin S (2017) Popular weight loss strategies: a review of four weight loss techniques. Curr Gastroenterol Rep 19:17–20. https://doi.org/10.1007/s11894-017-0603-8
Petridou A, Siopi A, Mougios V (2019) Exercise in the management of obesity. Metabolism 92:163–169. https://doi.org/10.1016/j.metabol.2018.10.009
Cooney G, Dwan K, Mead G (2014) Exercise for depression. JAMA J Am Med Assoc 311:2432–2433. https://doi.org/10.1001/jama.2014.4930
Da Silva MA, Singh-Manoux A, Brunner EJ et al (2012) Bidirectional association between physical activity and symptoms of anxiety and depression: the whitehall II study. Eur J Epidemiol 27:537–546. https://doi.org/10.1007/s10654-012-9692-8
De Moor MHM, Beem AL, Stubbe JH et al (2006) Regular exercise, anxiety, depression and personality: a population-based study. Prev Med (Baltim) 42:273–279. https://doi.org/10.1016/j.ypmed.2005.12.002
Lynch WJ, Robinson AM, Abel J, Smith MA (2017) Exercise as a prevention for substance use disorder: a review of sex differences and neurobiological mechanisms. Curr Addict Reports 4:455–466. https://doi.org/10.1007/s40429-017-0178-3
Chekroud SR, Gueorguieva R, Zheutlin AB et al (2018) Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: a cross-sectional study. Lancet Psychiatry 5:739–746. https://doi.org/10.1016/S2215-0366(18)30227-X
Meyer C, Taranis L (2011) Exercise in the eating disorders: terms and definitions. Eur Eat Disord Rev 19:169–173. https://doi.org/10.1002/erv.1121
Mond J, Gorrell S (2021) “Excessive exercise” in eating disorders research: problems of definition and perspective. Eat Weight Disord Stud Anorexia Bulim Obes. https://doi.org/10.1007/s40519-020-01075-3
Dittmer N, Jacobi C, Voderholzer U (2018) Compulsive exercise in eating disorders : proposal for a definition and a clinical assessment. J Eat Disord 6:1–9
Bratland-Sanda S, Mathisen TF, Sundgot-Borgen J, Rosenvinge JH (2019) Defining compulsive exercise in eating disorders: Acknowledging the exercise paradox and exercise obsessions. J Eat Disord 7:8–10. https://doi.org/10.1186/s40337-019-0238-2
Fairburn CG, Beglin S (2008) Eating Disorder Examination Questionnaire. In: Fairburn CG (ed) Cognitive behavior therapy and eating disorders. Guilford Press, New York, pp 309–313
Lavender JM, De Young KP, Anderson DA (2010) Eating Disorder Examination Questionnaire (EDE-Q): norms for undergraduate men. Eat Behav 11:119–121. https://doi.org/10.1016/j.eatbeh.2009.09.005
Luce KH, Crowther JH, Pole M (2008) Eating Disorder Examination Questionnaire (EDE-Q): norms for undergraduate women. Int J Eat Disord 41:273–276. https://doi.org/10.1002/eat.20504
Schaumberg K, Anderson LM, Reilly E, Anderson DA (2014) Patterns of compensatory behaviors and disordered eating in college students. J Am Coll Heal 62:526–533. https://doi.org/10.1080/07448481.2014.930468
Young S, Touyz S, Meyer C et al (2017) Validity of exercise measures in adults with anorexia nervosa: the EDE, compulsive exercise test and other self-report scales. Int J Eat Disord 50:533–541. https://doi.org/10.1002/eat.22633
Rizk M, Mattar L, Kern L et al (2020) Physical activity in eating disorders: a systematic review. Nutrients 12:1–33. https://doi.org/10.3390/nu12010183
Monell E, Levallius J, Forsén Mantilla E, Birgegård A (2018) Running on empty—a nationwide large-scale examination of compulsive exercise in eating disorders. J Eat Disord 6:1–10. https://doi.org/10.1186/s40337-018-0197-z
Fietz M, Touyz S, Hay P (2014) A risk profile of compulsive exercise in adolescents with an eating disorder: a systematic review. Adv Eat Disord 2:241–263. https://doi.org/10.1080/21662630.2014.894470
Lichtenstein MB, Hinze CJ, Emborg B et al (2017) Compulsive exercise: links, risks and challenges faced. Psychol Res Behav Manag 10:85–95. https://doi.org/10.2147/prbm.s113093
Nagata JM, Carlson JL, Kao JM et al (2017) Characterization and correlates of exercise among adolescents with anorexia nervosa and bulimia nervosa. Int J Eat Disord 50:1394–1403. https://doi.org/10.1016/j.physbeh.2017.03.040
Smith AR, Fink EL, Anestis MD et al (2013) Exercise caution: over-exercise is associated with suicidality among individuals with disordered eating. Psychiatry Res 206:246–255. https://doi.org/10.1016/j.psychres.2012.11.004
Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC (2018) The age of adolescence. Lancet Child Adolesc Heal 2:223–228. https://doi.org/10.1016/S2352-4642(18)30022-1
Bucchianeri MM, Arikian AJ, Hannan PJ et al (2013) Body dissatisfaction from adolescence to young adulthood: findings from a 10-year longitudinal study. Body Image 10:1–7. https://doi.org/10.1016/j.bodyim.2012.09.001
Ward ZJ, Rodriguez P, Wright DR et al (2019) Estimation of eating disorders prevalence by age and associations with mortality in a simulated nationally representative US Cohort. JAMA Netw Open 2:e1912925. https://doi.org/10.1001/jamanetworkopen.2019.12925
Neumark-Sztainer D, Wall M, Larson NI et al (2011) Dieting and disordered eating behaviors from adolescence to young adulthood: Findings from a 10-year longitudinal study. J Am Diet Assoc 111:1004–1011. https://doi.org/10.1016/j.jada.2011.04.012
Eisenberg D, Hunt J, Speer N (2013) Mental health in american colleges and universities: variation across student subgroups and across campuses. J Nerv Ment Dis 201:60–67. https://doi.org/10.1097/NMD.0b013e31827ab077
Arria AM, Caldeira KM, Allen HK et al (2017) Prevalence and incidence of drug use among college students: an 8-year longitudinal analysis. Am J Drug Alcohol Abuse 43:711–718
Schulenberg JE, Johnston LD, O’Malley PM, Bachman JG, Miech RA, Patrick ME (2020) Monitoring the future national survey results on drug use, 1975–2019: Volume II, College students and adults ages 19–60. Ann Arbor: Institute for Social Research, The University of Michigan. Available at http://monitoringthefuture.org/pubs.html#monographs
Eisenberg D, Lipson SK (2020) Healthy Minds Network. https://healthymindsnetwork.org
Lipson SK, Sonneville KR (2017) Eating disorder symptoms among undergraduate and graduate students at 12 U.S. colleges and universities. Eat Behav 24:81–88. https://doi.org/10.1016/j.eatbeh.2016.12.003
Nagata JM, Murray SB, Compte EJ et al (2020) Community norms for the eating disorder examination questionnaire (EDE-Q) among cisgender bisexual plus women and men. Eat Weight Disord Stud Anorexia Bulim Obes. https://doi.org/10.1007/s40519-020-01070-8
Nagata JM, Murray SB, Compte EJ et al (2020) Community norms for the Eating Disorder Examination Questionnaire (EDE-Q) among transgender men and women. Eat Behav 37:101381. https://doi.org/10.1016/j.eatbeh.2020.101381
Gollust SE, Eisenberg D, Golberstein E (2008) Prevalence and correlates of self-injury among university students. J Am Coll Heal 56:491–498
Serras A, Saules KK, Cranford JA, Eisenberg D (2010) Self-injury, substance use, and associated risk factors in a multi-campus probability sample of college students. Psychol Addict Behav 24:119–128. https://doi.org/10.1037/a0017210
Ganson KT, Rodgers RF, Lipson SK et al (2020) Sexual assault victimization and eating disorders among college-enrolled men. J Interpers Violence. https://doi.org/10.1177/0886260520958634
Ganson KT, Murray SB, Nagata JM (2021) Associations between eating disorders and illicit drug use among college students. Int J Eat Disord. https://doi.org/10.1002/eat.23493
Kroenke K, Spitzer RL, Williams JBW (2001) The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 16:606–613
Spitzer RL, Kroenke K, Williams JBW, Group PHQPCS (1999) Validation and utility of a self-report version of PRIME-MD: the PHQ Primary Care Study. JAMA 282:1737–1744. https://doi.org/10.1001/jama.282.18.1737
Levis B, Benedetti A, Thombs BD (2019) Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ. https://doi.org/10.1136/bmj.l1476
Spitzer RL, Kroenke K, Williams JBW, Löwe B (2006) A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 166:1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Byrd-Bredbenner C, Eck K, Quick V (2021) GAD-7, GAD-2, and GAD-mini: psychometric properties and norms of university students in the United States. Gen Hosp Psychiatry 69:61–66. https://doi.org/10.1016/j.genhosppsych.2021.01.002
Morgan JF, Reid F, Lacey JH (1999) The SCOFF questionnaire: assessment of a new screening tool for eating disorders. Br Med J 319:1467–1468. https://doi.org/10.1136/bmj.319.7223.1467
Luck AJ, Morgan JF, Reid F et al (2002) The SCOFF questionnaire and clinical interview for eating disorders in general practice: comparative study. Br Med J 325:755–756. https://doi.org/10.1136/bmj.325.7367.755
Maguen S, Hebenstreit C, Li Y et al (2018) Screen for disordered eating: improving the accuracy of eating disorder screening in primary care. Gen Hosp Psychiatry 50:20–25. https://doi.org/10.1016/j.genhosppsych.2017.09.004
Lipson SK, Kern A, Eisenberg D, Breland-Noble AM (2018) Mental health disparities among college students of color. J Adolesc Heal 63:348–356. https://doi.org/10.1016/j.jadohealth.2018.04.014
Murray SB, Nagata JM, Griffiths S et al (2017) The enigma of male eating disorders: a critical review and synthesis. Clin Psychol Rev 57:1–11. https://doi.org/10.1016/j.cpr.2017.08.001
Mitchison D, Mond J (2015) Epidemiology of eating disorders, eating disordered behaviour, and body image disturbance in males: a narrative review. J Eat Disord 3:1–9. https://doi.org/10.1186/s40337-015-0058-y
Nagata JM, Ganson KT, Griffiths S et al (2020) Prevalence and correlates of muscle-enhancing behaviors among adolescents and young adults in the United States. Int J Adolesc Med Health. https://doi.org/10.1515/ijamh-2020-0001
Murray SB, Brown TA, Lavender JM et al (2020) The evolving nature of weight dissatisfaction and eating behaviors among men: secular trends among college men across four decades. J Abnorm Psychol 129:824–830. https://doi.org/10.1037/abn0000587
Benjamini Y, Hochberg Y (1995) Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc 57:289–300
Goodwin H, Haycraft E, Meyer C (2011) Sociocultural correlates of compulsive exercise: Is the environment important in fostering a compulsivity towards exercise among adolescents? Body Image 8:390–395. https://doi.org/10.1016/j.bodyim.2011.05.006
Tylka TL (2011) Refinement of the tripartite influence model for men: dual body image pathways to body change behaviors. Body Image 8:199–207. https://doi.org/10.1016/j.bodyim.2011.04.008
Neumark-Sztainer D, Wall M, Story M, Standish AR (2012) Dieting and unhealthy weight control behaviors during adolescence: associations with 10-year changes in body mass index. J Adolesc Heal 50:80–86. https://doi.org/10.1016/j.jadohealth.2011.05.010
Bratland-Sanda S, Sundgot-Borgen J (2013) Eating disorders in athletes: overview of prevalence, risk factors and recommendations for prevention and treatment. Eur J Sport Sci 13:499–508. https://doi.org/10.1080/17461391.2012.740504
Joy E, Kussman A, Nattiv A (2016) 2016 update on eating disorders in athletes: a comprehensive narrative review with a focus on clinical assessment and management. Br J Sports Med 50:154–162. https://doi.org/10.1136/bjsports-2015-095735
Gorrell S, Scharmer C, Kinasz K, Anderson D (2020) Compulsive exercise and weight suppression: associations with eating pathology in distance runners. Eat Behav 36:101358. https://doi.org/10.1016/j.eatbeh.2019.101358
Di Lodovico L, Dubertret C, Ameller A (2018) Vulnerability to exercise addiction, socio-demographic, behavioral and psychological characteristics of runners at risk for eating disorders. Compr Psychiatry 81:48–52. https://doi.org/10.1016/j.comppsych.2017.11.006
Tarnopolsky MA (2011) Caffeine and creatine use in sport. Ann Nutr Metab 57:1–8. https://doi.org/10.1159/000322696
Udo T, Grilo CM (2019) Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States. Int J Eat Disord. https://doi.org/10.1002/eat.23004
Nutley SK, Mathews CA, Striley CW (2020) Disordered eating is associated with non-medical use of prescription stimulants among college students. Drug Alcohol Depend 209:107907. https://doi.org/10.1016/j.drugalcdep.2020.107907
Wong CF, Silva K, Kecojevic A et al (2013) Coping and emotion regulation profiles as predictors of nonmedical prescription drug and illicit drug use among high-risk young adults. Drug Alcohol Depend 132:165–171. https://doi.org/10.1016/j.drugalcdep.2013.01.024
Horvath SA, Shorey RC, Racine SE (2020) Emotion dysregulation as a correlate of food and alcohol disturbance in undergraduate students. Eat Behav 38:101409. https://doi.org/10.1016/j.eatbeh.2020.101409
Rancourt D, Ahlich E, Choquette EM et al (2020) A comparison of food and alcohol disturbance (FAD) in sorority and non-sorority women. J Am Coll Heal. https://doi.org/10.1080/07448481.2020.1740233
Lupi M, Martinotti G, Di Giannantonio M (2017) Drunkorexia: an emerging trend in young adults. Eat Weight Disord 22:619–622. https://doi.org/10.1007/s40519-017-0429-2
Kondo T, Nakano Y, Adachi S, Murohara T (2019) Effects of tobacco smoking on cardiovascular disease. Circ J 83:1980–1985. https://doi.org/10.1253/circj.CJ-19-0323
Rice F, Riglin L, Lomax T et al (2019) Adolescent and adult differences in major depression symptom profiles. J Affect Disord 243:175–181. https://doi.org/10.1016/j.jad.2018.09.015
Gratz KL (2003) Risk factors for and functions of deliberate self-harm: an empirical and conceptual review. Clin Psychol Sci Pract 10:192–205. https://doi.org/10.1093/clipsy/bpg022
Nock MK (2010) Self-injury. Annu Rev Clin Psychol 6:339–363. https://doi.org/10.1146/annurev.clinpsy.121208.131258
Gümmer R, Giel KE, Schag K et al (2015) High levels of physical activity in anorexia nervosa: a systematic review. Eur Eat Disord Rev 23:333–344. https://doi.org/10.1002/erv.2377
Taranis L, Meyer C (2011) Associations between specific components of compulsive exercise and eating-disordered cognitions and behaviors among young women. Int J Eat Disord 44:452–458. https://doi.org/10.1002/eat.20838
Oberle CD, Watkins RS, Burkot AJ (2018) Orthorexic eating behaviors related to exercise addiction and internal motivations in a sample of university students. Eat Weight Disord 23:67–74. https://doi.org/10.1007/s40519-017-0470-1
Meyer C, Taranis L, Goodwin H, Haycraft E (2011) Compulsive exercise and eating disorders. Eur Eat Disord Rev 19:174–189. https://doi.org/10.1002/erv.1122
Davern M (2013) Nonresponse rates are a problematic indicator of nonresponse bias in survey research. Health Serv Res 48:905–912. https://doi.org/10.1111/1475-6773.12070
Fosnacht K, Sarraf S, Howe E, Peck LK (2017) How important are high response rates for college surveys? Rev High Educ 40:245–265. https://doi.org/10.1353/rhe.2017.0003
Murray SB, Griffiths S, Mond JM (2016) Evolving eating disorder psychopathology: conceptualising muscularity-oriented disordered eating. Br J Psychiatry 208:414–415. https://doi.org/10.1192/bjp.bp.115.168427
Acknowledgements
We would like to thank Nicole Lisi for providing research assistance and Samuel Benabou for providing editorial assistance.
Funding
No funding was used to support this research.
Author information
Authors and Affiliations
Contributions
KTG and JMN conceptualized the study aims and statistical analysis plan. KTG conducted the statistical analysis and wrote a first draft of the manuscript. All authors provided edits and comments on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Research involving human participants
Healthy Minds Study was approved by the Health Sciences and Behavioral Sciences Institutional Review Board at the University of Michigan and all participating institutions. This study is exempt from research ethics approval given the data are publicly available and unidentifiable.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Ganson, K.T., Mitchison, D., Rodgers, R.F. et al. Compulsive exercise among college students: 5-year time trends in prevalence and demographic, substance use, and mental health correlates. Eat Weight Disord 27, 717–728 (2022). https://doi.org/10.1007/s40519-021-01210-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40519-021-01210-8