
Abstract
Objective
To evaluate factors associated with risk of hospitalization in children with community-acquired pneumonia (CAP).
Design
Prospective cohort study.
Setting
Multi-site hospital based study.
Intervention
A separate acute respiratory tract infection (ARI) treatment unit (ATU) was established. The revised WHO case definition for ARI was used across all the study sites to ensure uniformity in management of ARI patients (2–59 months). Clinical history, examination findings and investigations of enrolled patients were recorded on a predesigned case record form. Children were followed up at 1 week (± 1 day).
Main outcome measure
Risk factors for hospitalization among pneumonia patients.
Results
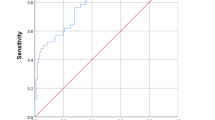
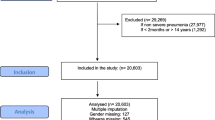
A total of 7026 children with the diagnosis of ARI were enrolled. Pneumonia was diagnosed in 938 (13.4%) patients (median (IQR) age: 15 (8, 25) months; 63.5% boys). Hospitalization was needed in 56.8% of pneumonia patients. On multivariate analysis, factors associated with risk of hospitalization were: Oxygen saturation on pulse oximetry (SpO2) <92% in room air (OR 7.04; 95% CI 1.6, 30.8, >0.5 ng/mL (OR: 7.5, 95% CI: 1.0, 57.7, P=0.05), and lower weight for height z-score (OR 0.8; 95 % CI: 0.6, 0.9, P=0.02).
Conclusion
Present study found SpO2 <92% at room air, serum procalcitonin level >0.5 ng/mL and lower weight for height z-score to be predictors for risk of hospitalization in under-five children presenting with community acquired pneumonia. These factors can be utilized to assess a child with CAP regarding the need of hospitalization.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
World Health Organization. Revised WHO classification and treatment of childhood pneumonia at health facilities: Evidence summaries. World Health Organization; 2014.
Rudan I, Tomaskovic L, Boschi-Pinto C, Campbell H. WHO child health epidemiology reference group. Global estimate of the incidence of clinical pneumonia among children under five years of age. Bull World Health Organ. 2004;356:895–903.
The Inter-Agency Group for Child Mortality Estimation (IGME). Estimates of under-five mortality rates by country, the 2011 release. Accessed on 12 January, 2013. Available at: www.childmortality.org.
Muller B, Harbarth S, Stolz D, et al. Diagnostic and prognostic accuracy of clinical and laboratory parameters in community-acquired pneumonia. BMC Infect Dis. 2007;7:10.
Harris M, Clark J, Coote N, et al. British Thoracic Society Guidelines for the Management of Community Acquired Pneumonia in Children: Update 2011. Thorax. 2011; 356(Suppl 2):ii1–23
Hazir T, Fox LM, Nisar YB, et al. Ambulatory short-course high-dose oral amoxicillin for treatment of severe pneumonia in children: A randomised equivalency trial. Lancet. 2008; 371:49–56.
Smyth A, Carty H, Hart CA. Clinical predictors of hypoxaemia in children with pneumonia. Ann Trop Paediatr. 1998;18:31–40.
Bradley JS, Byington CL, Shah SS, et al. The Management of Community-acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis. 2011;53:e25–76.
Araya S, Lovera D, Zarate C, et al. Application of a prognostic scale to estimate the mortality of children hospitalized with community-acquired pneumonia. Pediatr Infect Dis J. 2016; 35:369–73.
Duke T, Mgone J, Frank D. Hypoxaemia in children with severe pneumonia in Papua New Guinea. Int J Tuberc Lung Dis. 2001;5:511–9.
Subhi R, Adamson M, Campbell H, Weber M, Smith K, Duke T. The prevalence of hypoxemia among ill children in developing countries: A systematic review. Lancet. 2009; 9:219–27.
Graham SM, English M, Hazir T, Enarson P, Duke T. Challenges to improving case management of childhood pneumonia at health facilities in resource-limited settings. Bull World Health Organ. 2008;86:349–55.
Patwari Ak. Risk factors for mortality in children hospitalized with pneumonia. Indian Pediatr. 2016;49:869–70.
Lazzerini M, Sonego M, Pellegrin MC. Hypoxaemia as a mortality risk factor in acute lower respiratory infections in children in low and middle-income countries: Systematic review and meta-analysis. PloS One. 2015;10:e013616610.
Jroundi I, Mahraoui C, Benmessaoud R, et al. Risk factors for a poor outcome among children admitted with clinically severe pneumonia to a university hospital in Rabat, Morocco. Int J Infects Dis. 2014;28:164–70
Yadav K, Awasthi S, Takia L, et al. Procalcitonin and C reactive protein in WHO defined severe and very severe community acquired pneumonia: A hospital based cross sectional study. Clin Epidemiol Global Hlth. 2015;3:S3–S9.
Williams DJ, Zhu Y, Grijalva CG, et al. Predicting severe pneumonia outcomes in children. Pediatrics. 2016;138:e20161019.
Chisti M, Tebruegge M, La Vincente S, Graham S, Duke T. Pneumonia in severely malnourished children in developing countries — mortality risk, aetiology and validity of WHO clinical signs: A systematic review. Trop Med Int Health. 2009;14:1173–89.
Funding
Funding: This work was supported by Bill and Melinda Gates Foundation through the INCLEN Trust International (Grant number: OPP1084307). The funding source had no contribution in study design, implementation, collection and interpretation of data and report writing. Competing interest: None stated.
Author information
Authors and Affiliations
Contributions
JIB, BAC, RA: involved in data collection and manuscript writing; AM,RL: involved in development of protocol, supervision of the study, data analysis; JPG, RRD, VHR, BV: data collection, manuscript review. All authors approved the final version submitted.
Corresponding author
Additional information
Full list of ATU Group provided in Annexure I.
Rights and permissions
About this article

Cite this article
Bhat, J.I., Charoo, B.A., Mukherjee, A. et al. Risk of Hospitalization in Under-five Children With Community-Acquired Pneumonia: A Multicentric Prospective Cohort Study. Indian Pediatr 58, 1019–1023 (2021). https://doi.org/10.1007/s13312-021-2366-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13312-021-2366-4