
Abstract
Purpose
We evaluated the end-users’ satisfaction and the adoption of a technology solution embedding a clinical decision algorithm for screening and counselling individuals with suspicious COVID-19.
Methods
This was a cross-sectional study. Data was collected by the startup company Hi! Healthcare Intelligence. Satisfaction was measured using two questions presenting answer options as Likert scales of eleven points (from 0 to 10), in which 0 indicated low satisfaction and 10 indicated high satisfaction. We measured ‘general satisfaction’ through the average of questions 1 and 2. Descriptive analyses were used to summarize the data.
Results
The average satisfaction regarding the experience in using the technology solution and regarding the ‘recommendation for a friend or family’ was 7.94 (95% confidence interval [CI] 7.60 to 8.28) and 8.14 (95% CI 7.80 to 8.48), respectively. ‘General satisfaction’ was 8.04 (95% CI 7.70 to 8.37). The adoption regarding the implementation of the technology solution was 24.5% (n = 265).
Conclusion
The technology solution embedding a clinical decision algorithm for screening and counselling individuals with suspicious COVID-19 presented high satisfaction. One in four (¼) individuals interested in using the technology solution actually adopted it by following the clinical decision algorithm until the end, when counselling was provided.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
In December 2019, the first human cases of the new coronavirus (SARS-CoV-2/COVID-19) were identified in Wuhan, China [1]. Due to its high transmissibility, the virus spread rapidly to several countries and, after one month, the World Health Organization (WHO) declared the outbreak of COVID-19 to be a ‘public health Emergency of international concern’ [2]. Countries adopted emergency measures to flatten the curve of infection rates, such as contact restriction (e.g., to avoid greetings by shaking hands, hugging or kissing), reducing physical interactions (e.g., avoiding/prohibiting face-to-face meetings and demanding the closing of trade), and also social isolation (e.g., compulsory social isolation such as the so-called ‘lockdown’) [3]. However, even with all emergency measures, in July 2020, the global pandemic of COVID-19 reached 16.341.920 million confirmed cases, affecting 216 countries and territories [4]. In Brazil, in July 2020, the number of confirmed cases reached 2.442.375 with 87.618 confirmed deaths [5].
The diagnosis of COVID-19 in Brazil has been carried out in two stages [6]. The first stage includes the presence of symptoms of the so-called ‘flu syndrome’ (e.g., presence of acute respiratory symptoms, feverish sensation or fever, presence of cough, sore throat, runny nose, and/or breathing difficulty), and the assessment of the presence of symptoms of ‘acute respiratory syndrome’ (i.e., the presence of respiratory distress, persistent pressure in the chest, oxygen saturation less than 95% in room air and/or bluish colorings of the lips or face) [6]. The second stage includes laboratory testing (i.e., molecular biology – reverse transcription polymerase chain reaction (RT-PCR) in real-time, or immunological) and recommendation for social isolation [6]. Due to the large number of cases and the recommendations for social isolation, the Brazilian population has avoided seeking health services while misinformation has grown on the population. Therefore, there was an urgent need to create remote alternatives to screen, advise, provide remote assistance, and to direct the population flow within the health system, when necessary.
In Brazil approximately 81% of the population had Internet access in 2020 [7]. Using of internet-based screening services can reduce healthcare costs by preventing unneeded visits to emergency care and encourage self-care and self-efficacy [8]. Internet-based screening services could provide information to symptoms and possibly guide decisions about health conditions. It is believed that screening, counselling, and health care delivered via the Internet can reach a large part of the population. During the situation of COVID-19, alternative health approaches via the Internet have already been developed and implemented [9, 10]. Among them, a Brazilian startup company named Hi! Healthcare Intelligence developed and implemented, in 2020 during the COVID-19 pandemic in Brazil, a screening and counselling clinical decision algorithm for individuals with suspicion COVID-19.
To reach better outcomes and attempt to contain the dissemination of COVID-19, it is essential to understand the implementation of technology solutions such as the one developed by Hi! Healthcare Intelligence, especially in low- and middle-income countries, once their healthcare systems seem to be less prepared to deal with unforeseen situations. Therefore, the objectives of this study were: (1) to evaluate the end-users’ satisfaction regarding their experience with the screening and counselling clinical decision algorithm implemented during the COVID-19 pandemic in Brazil; and (2) to investigate the adoption of such technology solution.
2 Methods
2.1 Study design and setting
This was a cross-sectional study. Data were previously collected by the startup company Hi! Healthcare Intelligence from March to April 2020, during the COVID-19 pandemic in Brazil. A snowball sampling method was used to recruit any individuals who were interested to use the technology solution, and no incentives were give. The screening and counselling clinical decision algorithm was developed using the Typeform. The screening and counselling clinical decision algorithm was accessible through a link, that could be opened using a smartphone, computer, or tablet. This study was approved by the Research Ethics Committee of the Universidade Cidade de São Paulo (UNICID), CAAE: 33254920.3.0000.0064. This study was reported following the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) for cross-sectional studies [11].
2.2 The COVID-19 triage
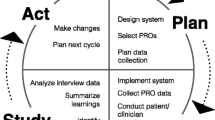
The COVID-19 screening and counselling clinical decision algorithm was developed by the startup company Hi! Healthcare Intelligence, and had three steps based on ‘yes’ or ‘no’ questions: (1) ‘fever’; (2) ‘acute respiratory symptom’; and (3) ‘possible SARS-CoV-2 exposure history’. Based on the answers of steps 1 to 3, the individuals were classified into: (1) ‘Green Flag: not a suspected case of COVID-19’, followed by tailored counselling; (2) ‘Yellow Flag: individual under monitoring for the possible development of COVID-19 symptoms’, followed by tailored counselling; and (3) ‘Red Flag: individual under investigation for COVID-19’, followed by tailored counselling. The COVID-19 screening and counselling clinical decision algorithm is detailed in Fig. 1.

COVID-19 screening and counselling clinical decision algorithm
2.3 Outcomes
The primary outcome of this study was the end-users’ satisfaction regarding their experience in using the technology solution embedding the clinical decision algorithm for screening and counselling individuals with suspicious COVID-19. Satisfaction typically “refers to the general service experience, including such features as waiting times, scheduling, and office environment” [12]. Satisfaction was measured using two questions presenting answer options as Likert scales of eleven points (from 0 to 10) in which 0 indicating low satisfaction and 10 indicating high satisfaction. Question 1 was about experience (On a scale of 0 to 10, how was your experience with the Hi! platform? for Covid-19?) and question 2 was about ‘recommendation for a friend or family’ (On a scale of 0 to 10, how much would you recommend the platform to a friend or family member? ) of the end-users towards the usage of the technology solution. We measure ‘general satisfaction’ through the average of questions 1 and 2.
The secondary outcome of this study was the adoption of using the technology solution embedding the clinical decision algorithm for screening and counselling individuals with suspicious COVID-19. Adoption refers to the representativeness of settings that use a given source, technology solution, intervention, policy or program [12, 13]. Adoption was operationalized in this study by taking the number of individuals who used the technology solution divided by the number of individuals who intended to use the technology solution. Individuals who used the technology solution were those who answered the questions regarding steps 1 to 3 of the clinical decision algorithm. Individuals who did not use the technology solution were those who did not answer the questions regarding steps 1 to 3 of the clinical decision algorithm. Individuals who intended to use the technology solution were all individuals included in this study, that is, those who accessed the technology solution regardless of using it or not.
2.4 Data analysis
All responses were exported from Typeform to a Microsoft Excel sheet. All analyses were performed using R version 3.6.2 [14]. A descriptive analysis was used to summarize the data. The parametric continuous variables were expressed as means and confidence interval (95% CI). The non-parametric continuous or discrete variables were expressed as medians and 25–75% interquartile ranges (IQR). The dichotomous and categorical variables were expressed as percentages (%) and frequency distributions (n). The distribution of the data was assessed by inspection of histograms and density curves.
3 Results
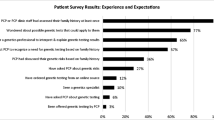
Between March and April 2020, 1500 individuals opened the link of the technology solution. From these 1500 individuals, 1081 individuals (72.1%) had the intention to use the technology solution (i.e., answered question 1 of the questionnaire regarding the ‘terms of use’). From these 1081 individuals, 265 completed steps 1 to 3 of the clinical decision algorithm, which represented an adoption of 24.5%. Individuals from 16 states of Brazil answered the questions regarding steps 1 to 3 of the clinical decision algorithm. Most end-users were from Sao Paulo (56.2%, n = 149) followed by the state of Rio de Janeiro (16.6%, n = 44). Table 1 presents all end-users’ locations. A total of 14.3% (n = 38) reported fever as a symptom. From those who reported fever, 65.8% (n = 25) reported the presence of acute respiratory symptoms. Table 2 presents the proportion of symptoms.
The average satisfaction regarding the experience of end-users towards the usage of the technology solution embedding the clinical decision algorithm for screening and counselling individuals with suspicious COVID-19 was 7.94 (95% confidence interval [CI] 7.60 to 8.28) in a Likert scale ranging from 0 to 10. The average satisfaction related to ‘recommendation for a friend or family’ was 8.14 (95% CI 7.80 to 8.48). The ‘general satisfaction’ (i.e., average of satisfaction regarding the experience and satisfaction related to ‘recommendation for a friend or family’) was 8.04 (95% CI 7.70 to 8.37). Table 3 presents the satisfaction findings.
4 Discussion
4.1 Main findings
The technology solution embedding the clinical decision algorithm for screening and counselling individuals with suspicious COVID-19 developed by the startup company Hi! Healthcare Intelligence presented high satisfaction in experience, recommendation, and general satisfaction. In addition, the adoption of the technology solution was reasonable, since a quarter of the participants who had the intention to use the tool actually used it. Our sample size was mostly composed of individuals from the state of São Paulo, the state was the authors are based at the moment of the data collection.
The high satisfaction of end-users could be explained for: (1) it was a fast and simple technology solution for the end-users; (2) it was based in the main symptoms of the COVID-19; (3) it was accessible via smartphone, tablets and computers; and (4) it was given an instantaneous counselling for end-users. Several online self-triage tools were developed to tackle the COVID-19 pandemic [15,16,17,18]. The satisfaction of end-users was evaluated by one of this tools [17], which also presented a high satisfaction (7.93; SD 1.60 – Likert scale 0 to 10) regarding information on COVID-19 education, self-assessment, and symptom tracking diary [17]. The present findings corroborate a previous systematic review, which showed that patients who used online technology solutions reported high levels of satisfaction [19]. Despite the sudden regulation of telehealth in Brazil [20, 21] and the particular context of public health inequities, individuals present high satisfaction when interacting with a technology solution. A cross-sectional study shows high levels of acceptability (60%, 95% CI 55 to 65%) with telerehabilitation by the general population, a similar implementation outcome to satisfaction [22]. A systematic review shows that 57.14% of internet-based screening of health conditions was offered using an algorithm-based system, and individuals were highly satisfied with internet-based screening services [23].
We considered ‘reasonable’ the adoption of the technology solution herein evaluated due to: (1) the data collection was performed on the onset of the outbreak; (2) the contradictory information disseminated by the federal government to tackle the COVID-19 pandemic, discouraging the population to search for advice and preventive information; [24, 25] (3) until COVID-19 pandemic, the use of telehealth was not integrated into Brazilian healthcare systems and the Brazilian population´s routine, and the Internet access for health was focused on sending instant messages and social media; [26] (4) intense dissemination of fake news about prevention and treatment of COVID-19 [27] discrediting real initiatives aimed at improving the health of the population [28]; (5) poor digital literacy in Brazil [29]; and (6) with the social distancing imposed by the COVID-19 pandemic, the Brazilian population increased the use of telehealth services; however, after two years users still show concerns about the security of personal data [30].
4.2 Strengths and limitations
Our data collection was performed during the onset of the pandemic in Brazil. The technology solution herein evaluated was simple, online, not requiring the creation of an account, and it was free of charge. These characteristics are important to implementation in a large scale. Participants did not have an established relationship with the developers of either the technology solution or the clinical decision algorithm. Therefore, satisfaction measures presented a low risk of detection bias. One the other hand, this was a cross sectional study which does not allow to explore the reasons for adoption, the factors influencing the end-users’ experiences, adherence to the recommendations, and the confirmation of COVID-19 suspicious cases. Additionally, our results could present context bias.
4.3 Implications and future directions
Online algorithms for screening and counselling may be helpful in healthcare. The use of social media to disseminate information about COVID-19, although rapid, it also created an abundance of misinformation, the so called ‘infodemic’, that may cause more harm than good [31]. Hence, having online evidence-based clinical counselling tools based on algorithms may help in disseminating evidence-based information, resulting in more reliable services to the population.
The use of telehealth has increased in the past 20 years [32]. However, the COVID-19 pandemic limited face-to-face contact and the use of telehealth strategies became crucial and increased drastically worldwide [33]. Moreover, ‘Health and Care Professions Councils’ have regulated the use of telehealth for a variety of health conditions [20, 21]. However, it is unknown whether online screening and counselling tools are acceptable for individuals seeking for health management during periods of social restrictions that pandemics and other conditions may employ. Thus, future studies are warranted for the development and/or adaptation of existing tools for health screening and counselling using an online approach. Online approaches may mitigate the community exposure and the saturation of health systems [34]. Future studies are needed to map the determinants (sociodemographic factors, health factors, service factors, and experiences) to patient satisfaction regarding technology solutions.
5 Conclusions
The technology solution embedding a clinical decision algorithm for screening and counselling individuals with suspicious COVID-19 presented high satisfaction regarding experience, recommendation, and general satisfaction. About 25% of the individuals interested in using the technology solution actually adopted it, which means that one in four (¼) followed the algorithm until the end, when counselling was provided towards COVID-19 prevention and/or management.
Data availability
Not applicable.
Code availability
Not applicable.
References
Archived. World Health Organization Timeline - COVID-19, https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (2020).
Novel C. (2019-nCoV) - SITUATION REPORT – 1 21 JANUARY 2020, https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf?sfvrsn=20a99c10_4 (2020, accessed August, 04 2020).
Wang G, Wu C, Zhang Q, Wu F, Yu B, Lv J et al. Epidemiological and Clinical Features of Corona Virus Disease 2019 (COVID-19) in Changsha, China. The LancetPreprint. 2020.
Coronavirus Disease. (COVID-19) Dashboard, https://covid19.who.int (2020, accessed July, 28 2020).
Ministério da saúde. - Painel Coronavírus, https://covid.saude.gov.br (2020, accessed July, 28 2020).
Ministério da Saúde. https://coronavirus.saude.gov.br/sobre-a-doenca#diagnostico (2020, accessed May, 14 2020).
Individuals using the Internet. (% of population) - Brazil, https://data.worldbank.org/indicator/IT.NET.USER.ZS?locations=BR (accessed May, 4 2022).
Boggan JC, Shoup JP, Whited JD, Van Voorhees E, Gordon AM, Rushton S, et al. Effectiveness of Acute Care Remote Triage systems: a systematic review. J Gen Intern Med. 2020;35(7):2136–45. PubMed PMID: 31898116. PMCID: PMC7352001. Epub 2020/01/04.
Governo do Brasil - Coronavírus - SUS. https://www.gov.br/pt-br/apps/coronavirus-sus (accessed May, 8 2020).
Prefeitura da Cidade de Recife. http://www2.recife.pe.gov.br/noticias/26/03/2020/pcr-e-governo-lancam-aplicativo-web-para-populacao-ser-orientada-distancia-por (accessed May, 8 2020).
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The strengthening the reporting of Observational studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–9. PubMed PMID: 18313558. Epub 2008/03/04.
Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76. PubMed PMID: 20957426. PMCID: PMC3068522. Epub 2010/10/20.
Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–7. PubMed PMID: 10474547. PMCID: PMC1508772. Epub 1999/09/04.
Team RC. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; Version 3.5. 0, (2018).
Denis F, Fontanet A, Le Douarin YM, Le Goff F, Jeanneau S, Lescure FXA, Self-Assessment. Web-based app to assess trends of the COVID-19 pandemic in France: Observational Study. J Med Internet Res. 2021;23(3):e26182. PubMed PMID: 33709945. PMCID: PMC7958347. Epub 2021/03/13.
Judson TJ, Odisho AY, Neinstein AB, Chao J, Williams A, Miller C, et al. Rapid design and implementation of an integrated patient self-triage and self-scheduling tool for COVID-19. J Am Med Inf Assoc. 2020;27(6):860–6. PubMed PMID: 32267928. PMCID: PMC7184478. Epub 2020/04/09.
Timmers T, Janssen L, Stohr J, Murk JL, Berrevoets MAH. Using eHealth to support COVID-19 Education, Self-Assessment, and Symptom Monitoring in the Netherlands: Observational Study. JMIR Mhealth Uhealth. 2020;8(6):e19822. PubMed PMID: 32516750. PMCID: PMC7313382. Epub 2020/06/10.
Yu J, Zhang HW, Shao YK, Lei Y, Chen H, Pu ZH et al. A smartphone-based online tool for prehospital self-triage of COVID-19. Chin J Acad Radiol 2020 Nov 16:1–6. PubMed PMID: 33225216. PMCID: PMC7667281. Epub 2020/11/24.
Chambers D, Cantrell AJ, Johnson M, Preston L, Baxter SK, Booth A, et al. Digital and online symptom checkers and health assessment/triage services for urgent health problems: systematic review. BMJ Open. 2019;9(8):e027743. PubMed PMID: 31375610. PMCID: PMC6688675. Epub 2019/08/04.
LEI Nº 13.989, DE 15 DE ABRIL DE. 2020. Dispõe sobre o uso da telemedicina durante a crise causada pelo coronavírus (SARS-CoV-2). (2020, accessed December, 2 2020).
RESOLUÇÃO Nº 516, DE 20 DE MARÇO DE. 2020 – Teleconsulta, Telemonitoramento e Teleconsultoria, https://www.coffito.gov.br/nsite/?p=15825 (2020, accessed December, 2 2020).
Fernandes LG, Oliveira RFF, Barros PM, Fagundes FRC, Soares RJ, Saragiotto BT. Physical therapists and public perceptions of telerehabilitation: an online open survey on acceptability, preferences, and needs. Braz J Phys Ther. 2022 Nov-Dec;26(6):100464. PubMed PMID: 36410257. PMCID: PMC9659283. Epub 2022/11/22.
Farzandipour M, Nabovati E, Sharif R. The effectiveness of tele-triage during the COVID-19 pandemic: a systematic review and narrative synthesis. J Telemed Telecare 2023 Jan 23:1357633X221150278. PubMed PMID: 36683438. PMCID: PMC9892819. Epub 2023/01/24.
Hallal PC. SOS Brazil: science under attack. Lancet. 2021;397(10272):373–4.
COVID-19 in Brazil. So what? Lancet. 2020;395(10235):1461.
Acesso à internet e à televisão. e posse de telefone móvel celular para uso pessoal 2019 / IBGE, Coordenação de Trabalho e Rendimento, https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=2101794 (accessed May, 4 2022).
de Barcelos TDN, Muniz LN, Dantas DM, Cotrim Junior DF, Cavalcante JR, Faerstein E. Analysis of fake news disseminated during the COVID-19 pandemic in Brazil. Rev Panam Salud Publica. 2021;45:e65. PubMed PMID: 34007263. PMCID: PMC8118089. Epub 2021/05/20. Analise de fake news veiculadas durante a pandemia de COVID-19 no Brasil.
Pulido CM, Ruiz-Eugenio L, Redondo-Sama G, Villarejo-Carballido BA. New Application of Social Impact in Social Media for Overcoming Fake News in Health. Int J Environ Res Public Health. 2020;17(7). PubMed PMID: 32260048. PMCID: PMC7177765. Epub 2020/04/09.
Pesquisa TICDomicílios. 2019, https://cetic.br/media/docs/publicacoes/2/20201123121817/tic_dom_2019_livro_eletronico.pdf (accessed May, 6 2022).
Painel TIC, COVID-19. : Pesquisa on-line com usuários de Internet no Brasil – 4ª edição: Cultura, Comércio Eletrônico, Serviços Públicos On-line, Telessaúde, Ensino Remoto e Teletrabalho, https://cetic.br/pt/publicacao/painel-tic-covid-19-pesquisa-online-com-usuarios-de-internet-no-brasil-4edicao/ (2022, accessed May, 6 2022).
The COVID-19 infodemic. Lancet Infect Dis. 2020 August;01(8):875.
Land T. Healthcare’s Present and Future: Consumer Centered, Consumer Driven. Front Health Serv Manage. 2019 Winter;36(2):1–2. PubMed PMID: 31764202. Epub 2019/11/26.
Keesara S, Jonas A, Schulman K. Covid-19 and Health Care’s Digital Revolution. N Engl J Med. 2020;382(23):e82. PubMed PMID: 32240581.
Hollander JE, Carr BG. Virtually Perfect? Telemedicine for Covid-19. N Engl J Med. 2020;382(18):1679–81. PubMed PMID: 32160451. Epub 2020/03/12.
Acknowledgements
Luiz Hespanhol was granted with a Young Investigator Grant from FAPESP, grant 2016/09220-1. Bruno T. Saragiotto was granted with a Young Investigator Grant from FAPESP, grant 2016/24217-7. Pamela Marinelli was granted with a FAPESP Masters scholarship, grant 2019/05805-3, and with a PhD fellowship from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brazil (CAPES) - Finance Code 001.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Contributions
LH and BTS were involved in the conceptualization of the study. PM, BTS, RFFO, LAO and LH were involved in designing the study. FRCF was responsible for the data collection. PM was responsible for cleaning and analyzing the data. PM, BTS, RFFO, LAO and LH were involved in interpreting the results. PM was responsible for writing the first draft of this manuscript. All authors were involved in revising the manuscript for intellectual content. All authors approved the final version of the article. All authors had full access to the data (including statistical reports and tables) and can take responsibility for the integrity of the data and the accuracy of data analysis.
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Research Ethics Committee of the Universidade Cidade de São Paulo (UNICID), CAAE: 33254920.3.0000.0064.
Consent to participate
Not applicable.
Consent for publication
All authors revised the manuscript and agreed with its submission.
Conflict of interest
Felipe R.C. Fagundes is the CEO of the startup Hi! Healthcare Intelligence. Bruno T. Saragiotto is on the scientific advisory board (non-paid) of the startup company Hi! Healthcare Intelligence. Pamela Marinelli, Rafael Felipe Ferreira Oliveira, Lisandra Almeida de Oliveira, and Luiz Hespanhol declare no conflicts of interest of any nature.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Marinelli, P., Saragiotto, B.T., Oliveira, R.F.F. et al. End-users’ satisfaction and adoption regarding the implementation of a technology solution for screening and counselling individuals with suspicious COVID-19: a cross-section study. Health Technol. (2024). https://doi.org/10.1007/s12553-024-00887-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12553-024-00887-y