
Abstract
Purpose of review
There is a known interrelationship between sleep and epilepsy. This review highlights the recent findings regarding interactions between sleep and circadian rhythms and the manifestations of epilepsy and surgical treatments for refractory epilepsy.
Recent findings
CLOCK gene expression may be reduced within the epileptogenic focus in patients with refractory epilepsy. Interictal epileptiform discharges during NREM and especially REM sleep may lateralize to the epileptogenic hemisphere. Intracranial video EEG monitoring and EEG from implanted responsive neurostimulator devices confirm scalp video EEG findings of a nocturnal peak for interictal epileptiform discharges. Successful epilepsy surgery may improve sleep macrostructure and quality.
Summary
Sleep outcomes in people with epilepsy undergoing epilepsy surgery and neurostimulator implantation may provide innovative understandings into the associations between sleep and epilepsy. These associations may then provide novel therapeutic options targeting sleep and circadian pathways to improve seizure control and improve the quality of life for patients with this debilitating disorder.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Epilepsy is a common disease affecting about 1% of the US population [1, 2] with half to nearly two thirds of people with epilepsy reporting sleep disturbances [3, 4]. People with epilepsy have poorer sleep quality and impaired micro- and macrostructure of sleep while the manifestations of epilepsy, including timing and severity seizures, appear to be influenced by endogenous circadian pathways. Understanding of these interactions has led to new strategies in evaluating patients for epilepsy surgery. The impact of epilepsy surgery on sleep outcomes has been recently reported as well. This article highlights studies exploring the association of circadian rhythms and sleep with epilepsy and the surgical evaluation and treatment of refractory epilepsy.
Circadian rhythm and epilepsy
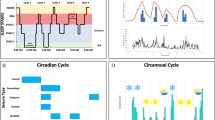
The term circadian rhythm refers to the 24-h cycle of behavioral and physiological activity that we (and other organisms on the planet) experience. Briefly, light entrains our brain to this 24-h cycle through neural pathways from the retina to the pineal gland, via the hypothalamus. Melatonin, produced in the pineal gland, is the circadian hormone in the body, rising during periods of darkness, and suppressed in the light. This hormone has effects in the brain and other tissues as well, timing this rhythmicity.
We have long known that interictal activity and seizures of different types of epilepsy tend to occur in patterns that follow the time of day. Interictal epileptiform discharges (IEDs) associated with multiple types of epilepsy have a nocturnal predominance and are activated by sleep, occurring most often during and with an expanded distribution in NREM sleep, possibly due to enhanced EEG synchronization [5, 6]. IEDs are less frequent and have the most focal field during REM sleep [6,7,8,9,10,11] and may be less frequent in phasic than tonic REM sleep [7, 12, 13]. Quigg et al. found that spontaneous limbic seizures in a rat model of mesial temporal lobe seizures consistently occurred towards the end of the light cycle (12 h light/12 h dark) and persisted at the same time of day when rats were in total darkness for 24 h [14•]. Seizures also occurred more often during inactive (rest) periods compared to active (wake) states, but only with external light exposure, suggesting that zeitgebers and daily patterns may also affect seizure occurrence. In human studies, many types of epilepsy have sleep-activated seizures, with highest seizure preponderance reported in NREM sleep (N1/N2 > N3) and smallest occurrence during REM sleep, based on brain region [9, 15,16,17,18,19]. Mesial temporal lobe seizures have two diurnal peaks, morning and late afternoon (including when evaluated in a non-circadian environment), and are more likely to secondarily generalize during sleep, frontal lobe seizures occur mostly during sleep with an early morning peak, occipital lobe seizures peak in the early evening and rarely occur during sleep, while seizures arising from the parietal lobe have mixed reports, some reporting an early morning peak occurrence and others with rare sleep-related frequency [14•, 17, 18, 20,21,22, 23••]. Clearly, sleep, a physiologic process strongly regulated by the circadian system, plays a role in these patterns. However, there is a greater appreciation of the role of the circadian pathways in epilepsy and the mechanisms underlying this pattern are still being defined.
For example, a link between melatonin and epilepsy has been established over time. Phase shifts of melatonin secretion have been demonstrated in both adults [24] and children [25] with epilepsy, and overall decreases in melatonin levels have been described in patients with epilepsy as well [26]. In an experimental model, rats who underwent pinealectomy, and thus had no melatonin, had an increase in cell loss and neuronal sprouting following drug-induced status epilepticus than controls. This effect was partially reversed by exogenously supplied melatonin, indicating that this hormone and an intact circadian rhythm may be protective for epileptogenesis [27]. As reviewed by Jain and Besag, evidence for the role that melatonin may play in clinical practice is mixed [28] and may be due to the aforementioned difference between the interaction of circadian rhythm with distinct seizure types. Melatonin has been shown to reduce seizure frequency and severity in juveniles with intractable epilepsy [29, 30]. However, a case series reported an increase in seizures in neurologically disabled children [31]. Further research on larger groups of subjects is needed to further identify if melatonin is effective, and if so, for which patients.
Another aspect of the circadian rhythm occurs at the cellular/molecular level, where certain genes are believed to be integral to keeping this clock attuned (e.g., CLOCK, PER1, PER2) as reviewed by Cho [32]. Recently, an examination of human brain tissue revealed decreased CLOCK gene expression within the surgically resected epileptic focus when compared to the surrounding normal brain tissue [33•]. Further studies showed transgenic mice where this protein was eliminated in excitatory neurons demonstrated decreased seizure thresholds and increased spontaneous epileptiform discharges. This work could provide the basis for future therapy using medications targeting circadian pathways in a localized manner to affect these genes within the seizure focus to treat the patient.
Epilepsy surgery and sleep
Knowledge of sleep stage effects on interictal epileptiform discharges (IEDs) has been utilized in patients with refractory epilepsy who are undergoing evaluation for epilepsy surgery. Several case series in patients with focal epilepsy [6, 9, 10, 34, 35] and one in children with generalized discharges but focal neuroimaging changes [8] undergoing video EEG for epilepsy surgery evaluation have investigated the value of lateralized interictal discharges while awake and by sleep stage. While IEDs that occur during NREM sleep tend to lateralize to the epileptogenic hemisphere more often than while awake [34], the unilateral, focal discharges occurring during REM sleep have the greatest concordance with the epileptogenic hemisphere [6, 8,9,10, 35].
Disturbed sleep and daytime sleepiness in people with epilepsy has been attributed to seizures, interictal epileptiform activity, timing of seizures, mood disorders, antiepileptic drugs, and comorbid sleep disorders [36, 37•]. Disturbed sleep patterns include increased transitional light NREM sleep and increased arousals, poor sleep efficiency, and altered percentage of REM sleep [10, 38,39,40,41,42]. Thus, intuitively, patients who become seizure free following epilepsy surgery should transition to a more normalized organization of sleep and improvement in sleep quality.
A few studies in patients with medically refractory epilepsy have evaluated the effects of resective epilepsy surgery on subjective and/or objective sleep measures [43•, 44•, 45••, 46]; most of which are case series or cohort studies performed in patients with medically intractable temporal lobe epilepsy. To help eliminate the impact of changes in antiepileptic drug doses on sleep measures, these investigators report maintaining stable doses of antiepileptic drugs from the preoperative through the postoperative assessment time points. One case series of 21 patients with medically refractory frontal lobe epilepsy with mostly sleep related seizures evaluated excessive daytime sleepiness (Epworth Sleepiness Scale scores > 10) before and at least 12 months after partial frontal lobe resection. Following surgical resection, the nine patients who reported preoperative excessive daytime sleepiness had resolution of excessive daytime sleepiness; seven were seizure free, one had rare disabling seizures, and one had worthwhile seizure reduction following surgery [46]. Carrion and colleagues found that prior to surgery in a cohort of patients with refractory temporal lobe epilepsy, sleep quality was poor (mean global Pittsburgh Sleep Quality Index, PSQI > 5), worse in patients with a predominance of nocturnal seizures (global PSQI = 10.63). Three months following surgical resection, seizure frequency improved and overall sleep quality normalized (global PSQI = 2.25) with persistent improvement at the 1-year postoperative follow-up visit (global PSQI 1.48) [43•].
The effects of epilepsy surgery on objective sleep measures have also been evaluated [44•, 45••]. One study in four patients with symptomatic generalized seizures and large right hemispheric neuroimaging abnormalities who underwent functional or anatomical right hemispherectomy reported seizure freedom postoperatively in all patients with only one patient who required continued antiepileptic drug therapy to control seizures. Although preoperative polysomnography data for the postsurgical patients were not reported, polysomnography in these patients > 2 years following right hemispherectomy demonstrated no IEDs and no significant changes in sleep architecture and objective sleep measures from recordings over the remaining left hemisphere compared to healthy controls [47]. In patients with refractory temporal lobe epilepsy, Serafini and colleagues performed polysomnograms before and after anterior temporal lobectomy while maintaining stable doses of antiepileptic drugs. All seizure-free patients showed reduced interictal epileptiform activity, reduced sleep onset latency, and decreased awakenings as well as increased total sleep time and increased REM sleep 1 year following surgery compared to preoperative baseline [44•]. Zanzmera et al. also found that patients good seizure control after epilepsy surgery had improved subjective daytime sleepiness (on Epworth Sleepiness Scale scores) as well as improved objective measures including reduced IEDs, decreased arousal index, increased total sleep time, and increased total REM sleep. Interestingly, 3 of the 12 patients who became seizure free postoperatively also demonstrated resolution of known comorbid obstructive sleep apnea with apnea-hypopnea index improving from > 5 events per hour to a normal range (< 5 events/h.) Those patients who did not have improved seizure control following surgery did not show improvement in subjective or objective sleep measures [45••]. Another case report demonstrated resolution of obstructive sleep apnea and reduced IEDs and seizures following focal left frontal lobe resection [48]. Although these reports demonstrated improvement in obstructive sleep apnea following epilepsy surgery, further studies are needed to determine the underlying mechanisms.
Neurostimulation treatment for epilepsy
Other treatment options for medically refractory epilepsy not amenable to focal cortical resection include implantation of neurostimulator devices. Deep brain stimulation, Vagus nerve stimulation, and responsive neurostimulation have been shown to improve seizure control. The impact of neurostimulation on sleep quality, sleep architecture, and on certain sleep disorders has been studied most in Vagus nerve stimulation while these interactions remain largely unknown in other forms of neurostimulation for epilepsy.
Vagus nerve stimulation
Vagus nerve stimulation (VNS) was FDA-approved for adjunctive treatment of medically refractory epilepsy in 1997 and since then, several case reports, retrospective and prospective descriptive studies have evaluated its effects on daytime sleepiness and sleep study parameters [49]. Lower VNS stimulus intensity (< 1.5 mA) has been shown to improve daytime sleepiness (decreased Epworth Sleepiness Scale scores [50] or decreased naps on sleep diaries [51]) and vigilance (increased mean sleep latency on Multiple Sleep Latency Test), even without improved seizure frequency from preimplantation baseline [50, 52]. Lower VNS current intensity can also improve visual reaction times which is associated with improved quality of life [52]. These lower current intensity settings may increase sleep-onset REM periods compared to baseline, though, do not appear to change percentages of sleep stages or other sleep parameters on overnight polysomnography in adults [50, 51]; however, increased N3 sleep has been observed in children [53]. Higher VNS stimulus intensities (> 1.5 mA) are associated with disturbed sleep due to increased arousals, NREM stage 1 sleep (N1), increased wake after sleep onset, reduced percentage of REM sleep [51], and increased mean sleep latency on Multiple Sleep Latency Tests [52].
Higher VNS stimulus intensities and rapid cycling on and off have been associated with development of nocturnal stridor, snoring, and development and/or worsening of obstructive and central sleep apnea. Decreasing stimulus intensities and increasing time between stimulation cycles may decrease these detrimental effects, as well as use of continuous positive airway pressure [54,55,56,57], perhaps due to VNS innervated peripheral effects on the upper airway musculature, increased vagal tone, and altered central nervous system modulation of airway patency [48]. Thus, it is important to consider screening for sleep apnea before and after VNS implantation, and to keep in mind that decreasing VNS stimulus intensity may improve VNS-induced sleep apnea.
Deep brain stimulation
Deep brain stimulation of the bilateral anterior nuclei of the thalamus (DBS-ANT) has been utilized to treat refractory epilepsy [49, 58] in Europe. One German study prospectively evaluated nine patients implanted with DBS-ANT and observed that the number of arousals on polysomnography was increased (1.4 to 6.7 times higher) during DBS stimulation compared to non-stimulation periods. Decreasing the DBS voltage reduced arousals and correlated with resolution of neuropsychiatric symptoms without worsening seizure control [59]. Although not yet commercially available in the USA, in May of 2018, the FDA approved deep brain stimulation of the bilateral anterior nuclei of the thalamus for treatment of adults with medically refractory focal epilepsy. There is a paucity of data evaluating the impact of DBS-ANT on sleep in people with epilepsy and due to the importance of thalamic control in sleep-wake processes, further investigation is needed.
Responsive neurostimulation
In 2013, the FDA approved implantation of a closed-loop responsive neurostimulation device within the two epileptogenic foci or single focus of patients with medically refractory focal epilepsy not amenable to resective surgery. The responsive neurostimulator detects and records short and long bursts of interictal epileptiform discharges (IEDs) and seizure activity and then delivers an electrical stimulation therapy to disrupt seizures. Investigations have been performed on these long-term intracranial recordings to determine circadian and ultradian patterns in patients with focal epilepsy. A case report in a patient with type I diabetes and refractory epilepsy s/p bilateral hemispheric responsive neurostimulator implantation, left in the mesial temporal region and right in the neocortical temporal region, found the patient’s right-sided seizures occurred earlier in the morning and at lower glucose levels than the patient’s left-sided seizures. Responsive neurostimulation therapies did not alter glucose levels. This finding encourages further studies evaluating the relationship between glucose levels, seizure activity, and potentially other endogenous circadian processes in patients with responsive neurostimulators [60].
Spencer et al. evaluated 134 refractory focal epilepsy patients with responsive neurostimulators implanted to treat seizures and reported that for all brain regions, IEDs had a nocturnal peak which correlates with prior studies performed with brief (few days) duration of scalp or intracranial video EEG monitoring. Seizures arising from neocortical brain regions had a nocturnal peak while seizures arising from limbic regions peaked during the day with a complex pattern (i.e., not monophasic) [23••]. Further investigations in patients with responsive neurostimulation may help better define circadian and ultradian patterns of ictal and interictal epileptiform activity which may lead to strategies to optimize treatments for epilepsy.
Conclusion
Knowledge of the interaction between sleep and epilepsy has been used to augment seizure localization strategies in patients with medically refractory epilepsy. Epileptiform discharges during REM sleep may have the strongest localizing value, lateralizing to the hemisphere containing the seizure focus. Although people with epilepsy commonly report disturbed sleep, those who undergo epilepsy surgery and achieve good seizure control may have improved subjective and objective sleep outcomes. In addition, seizures of different subtypes appear to have different circadian patterns, and an emerging amount of data implicates circadian rhythm associated genes in epileptogenesis. Focal resective surgery may improve obstructive sleep apnea in a few case reports; however, the underlying mechanisms need to be delineated. While we know that lower Vagus nerve stimulus intensities can positively impact daytime sleepiness, vigilance, and risk for sleep disordered breathing and the clock time peaks of epileptiform activity and seizures, little is known about the impact of other forms of neurostimulation on sleep and other circadian rhythms in people with epilepsy. Expansion of our understanding of the interactions between sleep, circadian rhythms, and epilepsy could provide new therapeutic avenues in the future.
Abbreviations
- ANT:
-
Anterior nucleus of the thalamus
- DBS:
-
Deep brain stimulation
- IED:
-
Interictal epileptiform discharges
- NREM:
-
Non-rapid eye movement sleep
- N1:
-
NREM stage 1 sleep
- N2:
-
NREM stage 2 sleep
- N3:
-
NREM stage 3 sleep or slow wave sleep
- RNS:
-
Responsive neurostimulation
- VNS:
-
Vagus nerve stimulation
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Zach MMaK, R. National and state estimates of the numbers of adults and children with active epilepsy - Unites States, 2015. In: MMWR Morb Mortal Wkly Rep. 2017. 2017.
Leonardi M, Ustun TB. The global burden of epilepsy. Epilepsia. 2002;43(Suppl 6):21–5.
Ismayilova V, Demir AU, Tezer FI. Subjective sleep disturbance in epilepsy patients at an outpatient clinic: a questionnaire-based study on prevalence. Epilepsy Res. 2015;115:119–25. https://doi.org/10.1016/j.eplepsyres.2015.06.009.
Staniszewska A, Maka A, Religioni U, Olejniczak D. Sleep disturbances among patients with epilepsy. Neuropsychiatr Dis Treat. 2017;13:1797–803. https://doi.org/10.2147/ndt.s136868.
Nayak CS, Mariyappa N, Majumdar KK, Ravi GS, Prasad PD, Nagappa M, et al. NREM sleep and antiepileptic medications modulate epileptiform activity by altering cortical synchrony. Clinical EEG and neuroscience. 2018;2017:1550059417747436. https://doi.org/10.1177/1550059417747436.
Malow BA, Aldrich MS. Localizing value of rapid eye movement sleep in temporal lobe epilepsy. Sleep Med. 2000;1(1):57–60.
Busek P, Buskova J, Nevsimalova S. Interictal epileptiform discharges and phasic phenomena of REM sleep. Epileptic disorders : international epilepsy journal with videotape. 2010;12(3):217–21. https://doi.org/10.1684/epd.2010.0319.
Okanari K, Baba S, Otsubo H, Widjaja E, Sakuma S, Go CY, et al. Rapid eye movement sleep reveals epileptogenic spikes for resective surgery in children with generalized interictal discharges. Epilepsia. 2015;56(9):1445–53. https://doi.org/10.1111/epi.13081.
Rocamora R, Andrzejak RG, Jimenez-Conde J, Elger CE. Sleep modulation of epileptic activity in mesial and neocortical temporal lobe epilepsy: a study with depth and subdural electrodes. Epilepsy & behavior : E&B. 2013;28(2):185–90. https://doi.org/10.1016/j.yebeh.2013.04.010.
Scarlatelli-Lima AV, Sukys-Claudino L, Watanabe N, Guarnieri R, Walz R, Lin K. How do people with drug-resistant mesial temporal lobe epilepsy sleep? A clinical and video-EEG with EOG and submental EMG for sleep staging study. eNeurologicalSci. 2016;4:34–41. https://doi.org/10.1016/j.ensci.2016.06.002.
Mendez M, Radtke RA. Interactions between sleep and epilepsy. Journal of clinical neurophysiology : official publication of the American Electroencephalographic Society. 2001;18(2):106–27.
Frauscher B, von Ellenrieder N, Dubeau F, Gotman J. EEG desynchronization during phasic REM sleep suppresses interictal epileptic activity in humans. Epilepsia. 2016;57(6):879–88. https://doi.org/10.1111/epi.13389.
Campana C, Zubler F, Gibbs S, de Carli F, Proserpio P, Rubino A, et al. Suppression of interictal spikes during phasic rapid eye movement sleep: a quantitative stereo-electroencephalography study. J Sleep Res. 2017;26(5):606–13. https://doi.org/10.1111/jsr.12533.
• Quigg M, Clayburn H, Straume M, Menaker M, Bertram EH 3rd. Effects of circadian regulation and rest-activity state on spontaneous seizures in a rat model of limbic epilepsy. Epilepsia. 2000;41(5):502–9 This is an important study that demonstrated that a circadian pattern of seizure occurrence in a rat model of limbic epilepsy.
Minecan D, Natarajan A, Marzec M, Malow B. Relationship of epileptic seizures to sleep stage and sleep depth. Sleep. 2002;25(8):899–904.
Pavlova MK, Shea SA, Scheer FA, Bromfield EB. Is there a circadian variation of epileptiform abnormalities in idiopathic generalized epilepsy? Epilepsy & behavior : E&B. 2009;16(3):461–7. https://doi.org/10.1016/j.yebeh.2009.08.022.
Herman ST, Walczak TS, Bazil CW. Distribution of partial seizures during the sleep--wake cycle: differences by seizure onset site. Neurology. 2001;56(11):1453–9.
Mirzoev A, Bercovici E, Stewart LS, Cortez MA, Snead OC 3rd, Desrocher M. Circadian profiles of focal epileptic seizures: a need for reappraisal. Seizure. 2012;21(6):412–6. https://doi.org/10.1016/j.seizure.2012.03.014.
Bazil CW, Walczak TS. Effects of sleep and sleep stage on epileptic and nonepileptic seizures. Epilepsia. 1997;38(1):56–62.
Durazzo TS, Spencer SS, Duckrow RB, Novotny EJ, Spencer DD, Zaveri HP. Temporal distributions of seizure occurrence from various epileptogenic regions. Neurology. 2008;70(15):1265–71. https://doi.org/10.1212/01.wnl.0000308938.84918.3f.
Karafin M, St Louis EK, Zimmerman MB, Sparks JD, Granner MA. Bimodal ultradian seizure periodicity in human mesial temporal lobe epilepsy. Seizure. 2010;19(6):347–51. https://doi.org/10.1016/j.seizure.2010.05.005.
Quigg M. Circadian rhythms: interactions with seizures and epilepsy. Epilepsy Res. 2000;42(1):43–55.
•• Spencer DC, Sun FT, Brown SN, Jobst BC, Fountain NB, Wong VS, et al. Circadian and ultradian patterns of epileptiform discharges differ by seizure-onset location during long-term ambulatory intracranial monitoring. Epilepsia. 2016;57(9):1495–502. https://doi.org/10.1111/epi.13455This large study carefully characterizes circadian patterns of interictal epileptiform discharges and timing of seizures based on long-term intracranial data from patients with implanted RNS for refractory epilepsy.
Schapel GJ, Beran RG, Kennaway DL, McLoughney J, Matthews CD. Melatonin response in active epilepsy. Epilepsia. 1995;36(1):75–8.
Molina-Carballo A, Acuna-Castroviejo D, Rodriguez-Cabezas T, Munoz-Hoyos A. Effects of febrile and epileptic convulsions on daily variations in plasma melatonin concentration in children. J Pineal Res. 1994;16(1):1–9.
Bazil CW, Short D, Crispin D, Zheng W. Patients with intractable epilepsy have low melatonin, which increases following seizures. Neurology. 2000;55(11):1746–8.
de Lima E, Soares JM Jr, del Carmen Sanabria Garrido Y, Gomes Valente S, Priel MR, Chada Baracat E, et al. Effects of pinealectomy and the treatment with melatonin on the temporal lobe epilepsy in rats. Brain Res. 2005;1043(1–2):24–31. https://doi.org/10.1016/j.brainres.2005.02.027.
Jain S, Besag FM. Does melatonin affect epileptic seizures? Drug Saf. 2013;36(4):207–15. https://doi.org/10.1007/s40264-013-0033-y.
Elkhayat HA, Hassanein SM, Tomoum HY, Abd-Elhamid IA, Asaad T, Elwakkad AS. Melatonin and sleep-related problems in children with intractable epilepsy. Pediatr Neurol. 2010;42(4):249–54. https://doi.org/10.1016/j.pediatrneurol.2009.11.002.
Goldberg-Stern H, Oren H, Peled N, Garty BZ. Effect of melatonin on seizure frequency in intractable epilepsy: a pilot study. J Child Neurol. 2012;27(12):1524–8. https://doi.org/10.1177/0883073811435916.
Sheldon SH. Pro-convulsant effects of oral melatonin in neurologically disabled children. Lancet (London, England). 1998;351(9111):1254. https://doi.org/10.1016/s0140-6736(05)79321-1.
Cho CH. Molecular mechanism of circadian rhythmicity of seizures in temporal lobe epilepsy. Front Cell Neurosci. 2012;6:55. https://doi.org/10.3389/fncel.2012.00055.
• Li P, Fu X, Smith NA, Ziobro J, Curiel J, Tenga MJ, et al. Loss of CLOCK results in dysfunction of brain circuits underlying focal epilepsy. Neuron. 2017;96(2):387–401 e6. https://doi.org/10.1016/j.neuron.2017.09.044 This study demonstrated evidence that CLOCK gene expression may be reduced within the epileptogenic focus in patients with refractory epilepsy.
Adachi N, Alarcon G, Binnie CD, Elwes RD, Polkey CE, Reynolds EH. Predictive value of interictal epileptiform discharges during non-REM sleep on scalp EEG recordings for the lateralization of epileptogenesis. Epilepsia. 1998;39(6):628–32.
Ochi A, Hung R, Weiss S, Widjaja E, To T, Nawa Y, et al. Lateralized interictal epileptiform discharges during rapid eye movement sleep correlate with epileptogenic hemisphere in children with intractable epilepsy secondary to tuberous sclerosis complex. Epilepsia. 2011;52(11):1986–94. https://doi.org/10.1111/j.1528-1167.2011.03198.x.
Legros B, Bazil CW. Effects of antiepileptic drugs on sleep architecture: a pilot study. Sleep Med. 2003;4(1):51–5.
• Jain SV, Glauser TA. Effects of epilepsy treatments on sleep architecture and daytime sleepiness: an evidence-based review of objective sleep metrics. Epilepsia. 2013;55(1):26–37. https://doi.org/10.1111/epi.12478This is an extensive review which critically evaluates the literature evaulating the effects on AEDs on objective sleep measures.
van Golde EG, Gutter T, de Weerd AW. Sleep disturbances in people with epilepsy; prevalence, impact and treatment. Sleep Med Rev. 2011;15(6):357–68. https://doi.org/10.1016/j.smrv.2011.01.002.
Maganti R, Hausman N, Koehn M, Sandok E, Glurich I, Mukesh BN. Excessive daytime sleepiness and sleep complaints among children with epilepsy. Epilepsy & behavior : E&B. 2006;8(1):272–7. https://doi.org/10.1016/j.yebeh.2005.11.002.
Giorelli AS, Passos P, Carnaval T, Gomes Mda M. Excessive daytime sleepiness and epilepsy: a systematic review. Epilepsy research and treatment 2013;2013:629469. doi:https://doi.org/10.1155/2013/629469, 9.
Gutter T, Brouwer OF, de Weerd AW. Subjective sleep disturbances in children with partial epilepsy and their effects on quality of life. Epilepsy & behavior : E&B. 2013;28(3):481–8. https://doi.org/10.1016/j.yebeh.2013.06.022.
Kaleyias J, Cruz M, Goraya JS, Valencia I, Khurana DS, Legido A, et al. Spectrum of polysomnographic abnormalities in children with epilepsy. Pediatr Neurol. 2008;39(3):170–6. https://doi.org/10.1016/j.pediatrneurol.2008.06.002.
• Carrion MJ, Nunes ML, Martinez JV, Portuguez MW, da Costa JC. Evaluation of sleep quality in patients with refractory seizures who undergo epilepsy surgery. Epilepsy & behavior : E&B. 2010;17(1):120–3. https://doi.org/10.1016/j.yebeh.2009.11.008This is prospective study evaluating sleep quality in patients with refractory mesial temporal lobe epilepsy before and after temporal lobectomy.
• Serafini A, Kuate C, Gelisse P, Velizarova R, Gigli GL, Coubes P, et al. Sleep before and after temporal lobe epilepsy surgery. Seizure. 2012;21(4):260–5. https://doi.org/10.1016/j.seizure.2012.01.007This study prospectively evaluated objective sleep parameters before and up to 2 years after temporal lobectomy.
•• Zanzmera P, Shukla G, Gupta A, Goyal V, Srivastava A, Garg A, et al. Effect of successful epilepsy surgery on subjective and objective sleep parameters--a prospective study. Sleep Med. 2013;14(4):333–8. https://doi.org/10.1016/j.sleep.2012.11.017 This is the first study to prospectively measure objective and subjective parameters before and after temporal lobectomy.
Nobili L, Francione S, Mai R, Cardinale F, Castana L, Tassi L, et al. Surgical treatment of drug-resistant nocturnal frontal lobe epilepsy. Brain : a Journal of Neurology. 2007;130(Pt 2):561–73. https://doi.org/10.1093/brain/awl322.
McCormick L, Nielsen T, Ptito M, Ptito A, Villemure JG, Vera C, et al. Sleep in right hemispherectomized patients: evidence of electrophysiological compensation. Clinical Neurophysiology : Official Journal of the International Federation of Clinical Neurophysiology. 2000;111(8):1488–97.
Foldvary-Schaefer N, Stephenson L, Bingaman W. Resolution of obstructive sleep apnea with epilepsy surgery? Expanding the relationship between sleep and epilepsy. Epilepsia. 2008;49(8):1457–9. https://doi.org/10.1111/j.1528-1167.2008.01677.x.
Romero-Osorio O, Gil-Tamayo S, Narino D, Rosselli D. Changes in sleep patterns after vagus nerve stimulation, deep brain stimulation or epilepsy surgery: systematic review of the literature. Seizure. 2018;56:4–8. https://doi.org/10.1016/j.seizure.2018.01.022.
Malow BA, Edwards J, Marzec M, Sagher O, Ross D, Fromes G. Vagus nerve stimulation reduces daytime sleepiness in epilepsy patients. Neurology. 2001;57(5):879–84.
Rizzo P, Beelke M, De Carli F, Canovaro P, Nobili L, Robert A, et al. Chronic vagus nerve stimulation improves alertness and reduces rapid eye movement sleep in patients affected by refractory epilepsy. Sleep. 2003;26(5):607–11.
Galli R, Bonanni E, Pizzanelli C, Maestri M, Lutzemberger L, Giorgi FS, et al. Daytime vigilance and quality of life in epileptic patients treated with vagus nerve stimulation. Epilepsy & Behavior : E&B. 2003;4(2):185–91.
Hallbook T, Lundgren J, Kohler S, Blennow G, Stromblad LG, Rosen I. Beneficial effects on sleep of vagus nerve stimulation in children with therapy resistant epilepsy. European Journal of Paediatric Neurology : EJPN : Official Journal of the European Paediatric Neurology Society. 2005;9(6):399–407. https://doi.org/10.1016/j.ejpn.2005.08.004.
St Louis EK, Faber K. Reversible sleep-related stridor during vagus nerve stimulation. Epileptic Disorders : International Epilepsy Journal With Videotape. 2010;12(1):76–80. https://doi.org/10.1684/epd.2010.0294.
Gschliesser V, Hogl B, Frauscher B, Brandauer E, Poewe W, Luef G. Mode of vagus nerve stimulation differentially affects sleep related breathing in patients with epilepsy. Seizure. 2009;18(5):339–42. https://doi.org/10.1016/j.seizure.2008.12.003.
Malow BA, Edwards J, Marzec M, Sagher O, Fromes G. Effects of vagus nerve stimulation on respiration during sleep: a pilot study. Neurology. 2000;55(10):1450–4.
Marzec M, Edwards J, Sagher O, Fromes G, Malow BA. Effects of vagus nerve stimulation on sleep-related breathing in epilepsy patients. Epilepsia. 2003;44(7):930–5.
Fisher R, Salanova V, Witt T, Worth R, Henry T, Gross R, et al. Electrical stimulation of the anterior nucleus of thalamus for treatment of refractory epilepsy. Epilepsia. 2010;51(5):899–908. https://doi.org/10.1111/j.1528-1167.2010.02536.x.
Voges BR, Schmitt FC, Hamel W, House PM, Kluge C, Moll CK, et al. Deep brain stimulation of anterior nucleus thalami disrupts sleep in epilepsy patients. Epilepsia. 2015;56(8):e99–e103. https://doi.org/10.1111/epi.13045.
Kinnear KM, Warner NM, Haltiner AM, Doherty MJ. Continuous monitoring devices and seizure patterns by glucose, time and lateralized seizure onset. Epilepsy & Behavior Case Reports. 2018;10:65–70. https://doi.org/10.1016/j.ebcr.2018.03.001.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Joseph T. Daley reports no conflicts of interest. Jennifer L. DeWolfe reports grants from Marinus Pharmaceuticals, outside the submitted work.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Take-home points
• Interictal epileptiform discharges have a nocturnal peak in focal and generalized epilepsies
• Interictal epileptiform discharges during REM sleep may help lateralize the hemisphere containing the seizure onset zone in people with intractable epilepsy
• CLOCK gene expression may be reduced within the epileptogenic focus in patients with refractory epilepsy
• Lower intensity settings on Vagus nerve stimulators may improve daytime sleepiness and vigilance in people with refractory epilepsy while higher intensity settings and rapid cycling may increase risk of sleep apnea
• Sleep architecture, daytime sleepiness, and sleep quality may be improved in patients who become seizure free following focal cortical resection
This article is part of the Topical Collection on Epilepsy
Rights and permissions
About this article

Cite this article
Daley, J.T., DeWolfe, J.L. Sleep, Circadian Rhythms, and Epilepsy. Curr Treat Options Neurol 20, 47 (2018). https://doi.org/10.1007/s11940-018-0534-1
Published:
DOI: https://doi.org/10.1007/s11940-018-0534-1