
Abstract
Purpose of Review
The rising suicide rate in the USA will not be reversed without improved risk assessment and prevention practices. To date, the best method for clinicians to assess a patient’s risk for suicide is screening for past suicide attempts in the patient and their family. However, neuroimaging, genomic, and biochemical studies have generated a body of findings that allow description of an initial heuristic biological model for suicidal behavior that may have predictive value.
Recent Findings
We review studies from the past 3 years examining potential biological predictors of suicide attempt behavior. We divide findings into two major categories: (1) structural and functional brain imaging findings and (2) biochemical and genomic findings encompassing several systems, including major neurotransmitters (serotonin, catecholamines, GABA, and glutamate), the hypothalamic pituitary adrenal (HPA) axis, the inflammasome, lipids, and neuroplasticity.
Summary
The biomarkers that appear promising for assessing suicide risk in clinical settings include indices of serotonergic function, inflammation, neuronal plasticity, and lipids.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The World Health Organization estimates that globally over 800,000 people die by suicide each year [1]. The number of nonfatal suicide attempts may be 10–20 times higher [1]. In the USA in 2014, about 43,000 individuals committed suicide [2]—making suicide the tenth leading cause of death [3]—and an estimated 1.3 million attempted suicide [4]. The Centers for Disease Control estimate that, annually, the USA incurs $51 billion worth of healthcare and work loss-related costs due to suicide [4]. Given the immeasurable personal and massive economic impact that suicide has on society, preventing suicide should be a major national health priority.
Suicidal ideation and behavior are on a spectrum. Ideation has a severity that ranges from fleeting, passive thoughts that life is not worth living and not caring if one does not wake up in the morning, to persistent, compelling thoughts of killing oneself with a specific, highly lethal method. Suicide attempts range from impulsive, low lethality attempts to well-planned highly lethal suicide attempts, and finally to suicide death. We recently reviewed biomarkers associated with death by suicide [5•]. Here, we focus on nonfatal suicide attempt behavior because it is linked to suicide more closely than suicidal ideation both in terms of biology and the potential for predicting risk of suicide. At the same time, this avenue of research involves living patients and has potential for detecting markers of higher risk and testing interventions that may prevent suicide. We define suicide attempt, based on Columbia-Classification Algorithm of Suicide Assessment or C-CASA [6], as a deliberate act of self-harm carried out with at least some intent to die. To date, there is no robustly reliable method of assessing suicide risk. Clinicians rely primarily on information offered voluntarily by patients regarding past personal suicidal behavior or a family history of suicidal behavior. Unfortunately, some of the patients who are most determined to die by suicide fear being thwarted in their suicide attempt plans and thus will falsely deny suicidal ideation prior to their suicide [7]. In terms of family history, the stigma associated with suicide may mean the patient is not aware of suicidal behavior that may have involved other family members. Therefore, it is important to develop a risk assessment approach that reduces dependence on subjective patient reports and incorporates information about the neural, genetic, and biochemical underpinnings of suicidal behavior.
In this paper, we review the most recent literature (past 3 years) examining biological markers of nonfatal suicide attempts within the context of psychopathology; studies of suicide attempt stemming from brain injury (e.g., head trauma, stroke, and related neurological disorders) are not considered. We discuss findings from brain imaging, genetic, and molecular studies of nonfatal suicide attempters compared to non-attempters across various diagnoses and to healthy volunteers. Our goal is to highlight biomarkers with potential for predicting risk and thereby guiding prevention or becoming treatment targets in suicide risk management.
Structural and Functional Brain Findings
Brain imaging studies report both structural and functional abnormalities in the brains of suicide attempters. We review suicide attempt studies employing structural magnetic resonance imaging (MRI), diffusion tensor imaging (DTI), resting and task-based functional MRI, and positron emission tomography (PET).
Structural MRI
Gray matter volume (GMV), white matter volume (WMV), and hyperintensities in the brains of suicide attempters have been compared to those of psychiatric and healthy volunteers. Suicide attempters across diagnoses have been shown to have less GMV and density across several brain regions including the prefrontal, temporal [8,9,10], and parietal [9, 10] cortices, occipital cortex [9], putamen, striatum [11], lentiform nucleus [10, 12], insula, midbrain, and cerebellum [10]. Depressed suicide attempters, relative to depressed non-attempters, also have lower WMV in the frontal and parietal regions, external capsule, midbrain, and cerebellum [10], although WMV is greater in the orbital or ventral prefrontal regions of suicide attempters with schizophrenia [13]. Other volumetric changes include a smaller corpus callosum [14] and a larger amygdala [15, 16].
Hyperintensities appear to be more prevalent in suicide attempters relative to both psychiatric and healthy volunteers. Older studies report more subcortical [17, 18], deep white matter [19, 20], and periventricular [18, 21] hyperintensities in suicide attempters relative to non-attempters. In fact, patients who presented with hyperintensities were 4.7 to 8 times more likely to also have a history of suicide attempts than those without hyperintensities [18,19,20,21]. It is unclear, however, if hyperintensities can predict a suicide attempt.
Recent Findings
Most of the studies in the past 3 years have examined brain volumetric changes in depressed suicide attempters relative to non-suicidal patients and healthy controls. The overall direction of findings appears to be similar to that of earlier ones. Studies assessing depressed suicide attempters and depressed non-attempters found lower GMV in the right superior temporal gyrus [22] and cerebellum and in the left angular [23] and cingulate gyri [24] of the attempter group. Smaller hippocampal volume has also been reported [25], particularly in recent suicide attempters (attempts in the past month) compared with non-attempters. Some of these findings are independent of depressed mood—currently, euthymic mood disorder patients with past suicide attempts have smaller left ventrolateral prefrontal cortex (PFC) GMV relative to euthymic mood disorder non-attempters [26]. This independence of mood more strongly links these brain changes to the combination of traits that form the diathesis for suicidal behavior.
Lower GMV has also been reported in suicide attempters with other diagnoses. Lower GMV was observed in the superior temporal, parietal, and frontal cortices; inferior temporal cortex; supramarginal region; and right insula of suicide attempters relative to non-attempters with schizophrenia and schizoaffective disorders [27]. High-lethality attempters had even smaller GMV in the left lingual gyrus and right cuneus; conversely, the GMV of the thalamus, right insula, and left supramarginal gyrus was higher in this group relative to low-lethality attempters. Another study in schizophrenia found suicide attempts associated with cortical thinning in the dorsolateral PFC and right superior temporal, middle temporal, temporopolar, and insular cortices [28]. Other studies—examining suicide attempters with mood disorders [29] and borderline personality disorder [30]—found additional negative correlations between the lethality of suicide attempt and the volume of the nucleus accumbens [29] and several fronto-temporal-limbic regions [30]. However, not all studies agree that GMV [29, 31] is decreased in suicide attempters.
In summary, most MRI studies find smaller GMV in suicide attempters, even in comparison with psychiatric controls, involving primarily prefrontal and temporal cortical sub-regions and insula. However, due to methodological differences related to region of interest selection, magnet strength, sample psychopathology, and perhaps also time since suicide attempt, it is premature to confidently synthesize these findings alone into a meaningful anatomical model of suicide attempt behavior.
Diffusion Tensor Imaging
Older DTI studies of suicide attempters are sparse. The studies reviewed used fractional anisotropy (FA) to measure the integrity and direction of neuronal fibers in the brain. Comparison of attempters to non-attempters in bipolar [32] and depressed samples [33] indicates lower FA or impaired white matter tract integrity in the left orbitofrontal cortex (OFC) and basal ganglia.
Recent Findings
Two recent studies report results that are somewhat convergent with previous findings. Depressed suicide attempters had lower FA in the dorsomedial PFC [34•] and left medial PFC [35•], compared with depressed non-attempters. Reductions in fiber projections from the anterior limb of internal capsule to the left thalamus and left OFC were also noted [35•]. Additionally, attempters had a lower percentage of fibers projecting to cortical regions and thalamus relative to healthy controls [35•]. Euthymic females with a history of bipolar disorder and suicide attempts had lower FA throughout the corpus callosum [36] compared with healthy volunteers. Given the lack of psychiatric controls in some of these studies, one must be cautious in attributing findings in suicide attempters to the diathesis for suicidal behavior or, more generally, psychopathology.
In contrast, two studies of attempters versus non-attempters with primary diagnoses of panic disorder [37], schizophrenia, and schizophreniform disorder [38] reported higher FA values in suicide attempters. In both studies, attempters showed higher FA in areas of the internal capsule, sagittal stratum, posterior thalamic radiation, superior longitudinal fasciculus, and corona radiata [37, 38]. Attempters with panic disorder also had higher FA values in the corpus callosum [37]. Of note, FA values in the posterior thalamic radiation and right retrolenticular part of internal capsule were positively correlated with suicidal ideation scores [37].
White matter abnormalities defined by lower fractional anisotropy have been found in younger suicide attempters, but white matter lesions (WML) that appear progressively with age may represent other pathological processes, including cerebrovascular atherosclerosis. One study of the elderly [39•] found more WML at baseline, and more WML growth over time in depressed attempters compared with depressed non-attempters. This structural change in connectivity may be another pathway to suicidal behavior.
In summary, white matter abnormalities in suicide attempters involve neural networks participating in decision-making and cognitive and emotional processing. However, it is not clear why findings in mood disorders differ from anxiety and psychotic disorders, although modest sample sizes and possible medication effects mean that these disease-related differences in findings may reflect either the effect of the psychiatric diagnosis or residual effects of treatment.
Functional MRI
fMRI uses blood oxygenation levels in the brain as a measure of brain activity at rest or while participants perform cognitive and other tasks. Older fMRI studies of suicide attempters examined emotional vs neutral stimuli [40], decision-making [41], and response inhibition [42]. Relative to depressed non-attempters, suicide attempters showed greater activation in the OFC and anterior cingulate cortex when viewing emotionally expressive faces [40], indicating different processing of emotional stimuli. Moreover, lower occipital and orbitofrontal activation was noted in euthymic attempters compared to non-attempters during risky versus safe choices [41], consistent with altered decision-making. Similarly, depressed adolescent attempters exhibited less activity than non-attempters in the anterior cingulate cortex during response inhibition tasks [42], a possible indicator of impaired impulse control.
Recent Findings
One study [43] partially replicated outcomes from previous studies [40, 41], finding greater OFC and ventrolateral PFC activation in response to angry faces in euthymic suicide attempters compared to non-attempters [43]. No group differences were seen in response to happy faces. However, sad faces (not previously studied) elicited lower activation in the right anterior cingulate cortex (ACC) of attempters [43]. During a decision-making task, attempters, relative to non-attempters, exhibited lower dorsal PFC activation when engaging in risky choices [43]. But, contrary to previous findings of no differences between groups, this study reported higher ACC, dorsal PFC, and OFC response to wins in suicide attempters compared to non-attempters [43].
Emotional processing and decision-making have also been examined in adolescent samples with lifetime MDD. Relative to non-attempters, high-risk decisions in suicide attempters were associated with less right thalamic activation [44] and greater activity in the left dorsal PFC, right ACC, middle temporal gyrus, and sensory cortices when viewing mildly angry faces [45]. In depressed elderly individuals, highly impulsive attempters with histories of poorly planned attempts were more likely to have a dampened paralimbic reward signal [46] and an exaggerated response in the frontal operculum [47]. When reward delay was examined, patients with better planned attempts showed less activation of the lateral PFC [48]. Moreover, longer delays to reward were correlated with less parahippocampal and occipital activation in attempters [48]. There were no differences in activation in depressed attempters and non-attempters performing a response inhibition task [49].
Although there are some inconsistencies that require further research, there seems to be greater prefrontal activation—perhaps as a compensatory mechanism—when engaging in emotional processing tasks, and less activation when assessing risk, evaluating reward, and making decisions carrying some risk, reflecting perhaps impaired top-down control.
Positron Emission Tomography
Most PET studies of suicide attempters have examined indices of the serotonergic system in the brain, because it is the neurotransmitter system most consistently associated with suicide and nonfatal suicidal behavior. Serotonin transporter (5-HTT) binding, measured using the [11C]DASB radioligand [50], was originally reported to be higher in pregenual ACC and midbrain of suicide attempters relative to bipolar non-attempters. Another study [51] compared high and low lethality depressed attempters with respect to relative regional rates of glucose metabolism (rCMRGlu) using [18F]FDG PET in two conditions: a fenfluramine challenge (which causes massive serotonin release) and placebo. High lethality attempters in the placebo condition exhibited lower rCMRGlu in superior and inferior frontal regions and the ACC relative to low lethality attempters; the brain areas of these correlations were roughly doubled during the fenfluramine challenge. These studies indicate prefrontal, cingulate cortical, and brainstem involvement in suicidal behavior.
Recent Findings
Three PET studies report lower serotonin transporter binding in major depression. A [11C]DASB study of depressed patients found lower 5-HTT binding in the midbrain of suicide attempters relative to MDD non-attempters and controls, but no differences in the PFC or ACC [52]. Another study [53], using 4-[18F]ADAM, reported lower binding in the midbrain and thalamus of suicide attempters compared to both non-attempters and healthy controls. Lower 5-HTT binding potential in midbrain and pons of suicide attempters compared to healthy volunteers was also identified by a [11C]ZIENT PET study [54].
An [18F]FDG study examining rCMRGlu in a placebo versus fenfluramine challenge condition, this time in attempters and non-attempters with MDD and bipolar disorder diagnoses [55], reported glucose hypometabolism in the right dorsolateral PFC, including superior, middle, and inferior frontal gyrus, in the placebo condition. During the fenfluramine challenge, the hypometabolic area differences became bilateral. However, contrary to some previous reports, rCMRGlu was higher in ventromedial regions, including ACC, caudate, and putamen.
Two PET studies of the 5-HT1A receptor binding potential with [11C]WAY-100635 [56, 57•] found that past and future higher-lethality depressed attempters had elevated binding potential (BP) in the raphe nuclei autoreceptor, which would favor lower serotonin neuron firing and less serotonin release. This is a novel mechanism for impaired serotonin system transmission. Higher autoreceptor binding can predict the lethality of future suicide attempts, and so, it does not appear to be a consequence of the suicide attempt behavior [57•].
Of the recent PET studies examining the serotonin system, three find brainstem and one finds prefrontal cortex abnormalities in suicide attempters. Most of these studies have been done in patients with mood disorders, and thus, studies of suicidal behavior in other psychiatric conditions are needed to determine if there is a single consistent set of abnormalities across multiple psychiatric diagnostic categories. These abnormalities may predict lethality of future suicidal behavior, and if confirmed, may help calibrate suicide prevention efforts in relation to the risk of more lethal suicide attempts.
Limitations
Most imaging studies involve small samples, raising concerns about statistical power. Furthermore, some studies do not include both healthy and psychiatric control groups, making it impossible to determine which changes are due to the diathesis for suicidal behavior and which are due to the primary psychiatric disorders. Finally, where scanning methods differ, it is harder to compare results across studies.
Biochemical and Genomic Findings
As in our review of neurotransmitter correlates and predictors of suicide [5•], we examine several neurotransmitter systems and major findings from genomic studies in relation to nonfatal suicide attempts.
The Hypothalamic-Pituitary-Adrenal Axis
The hypothalamic-pituitary-adrenal (HPA) axis is a major stress-response system. It has been researched extensively for its role in psychopathology. Older studies show that dexamethasone resistance predicts risk of future suicide in mood disorders implicating HPA axis in suicide attempt behavior. Currier & Mann (2008) provide an overview of the role of the HPA axis in suicidal behavior [58].
Recent Findings
Saliva cortisol levels were lower in suicide attempters relative to non-attempters across diagnoses [59, 60 •] and, interestingly, also in non-attempters with suicide-related behaviors [60•]. Cerebrospinal fluid (CSF) and plasma cortisol levels appeared higher in suicide attempters relative to healthy controls [61], although it is unclear what influence the comparison groups (psychiatric versus healthy controls) and medication status (present versus absent) had on the results. A study of 208 offspring of parents with mood disorders found that familial transmission of suicide attempt behavior was associated with blunted salivary cortisol levels [60•]. We also recently reported that polymorphisms of NR3C1, a glucocorticoid receptor (GR) gene, and FKBP5, a chaperone protein involved in GR function, are associated with suicide attempts in depression [62] confirming and extending findings from some older genetic studies of suicide [63,64,65,66].
Serotonin
The serotonergic system—the main target of selective serotonin-reuptake inhibitors (SSRIs) in depression, associated with the pathogenesis of mood disorders—has been separately implicated in the diathesis (or predisposition) to suicidal behavior. Indices of the serotonergic system of interest in suicidal behavior are serotonin (5-HT), tryptophan hydroxylase (TPH1 and 2, rate-limiting biosynthetic isoenzymes), the 5-HT1A and 5-HT2A serotonin receptors, serotonin transporter (5-HTT), the main metabolite of serotonin (5-HIAA), and associated enzymes, specifically monoamine oxidase A (MAO-A). For reviews of previous findings, please see the following two papers [58, 67].
Recent Findings
Many studies focused on changes in TPH, 5-HTT, or 5-HT receptors, with the majority exploring genetic polymorphisms. Both TPH1 (expressed in the brain during fetal life) and TPH2 (expressed in the brain throughout life) polymorphisms were found to be associated with suicide attempt by some but not all studies [68,69,70].
The rs6295 single nucleotide polymorphism (SNP) in the 5HTR1A promoter region was associated with suicide attempt, psychiatric hospitalizations, and substance use disorder [71]. For 5-HTR2c, the rs6318 C-allele of 5HTR2C conferred greater risk for suicide attempt in Serbian patients with MDD, BD, and schizophrenia [72]. Additionally, methylation pattern changes in the 5-HTR3A gene were associated with suicidal behavior in borderline personality disorder, bipolar disorder, and attention deficit/hyperactivity disorder (ADHD) [73•].
Studies of the serotonin transporter focus mainly on the 5-HTTLPR upstream promotor region polymorphism of the SLC6A4 gene. Most studies find an association between lower expressing variants of the 5-HTTLPR, early life stress, and suicidal behavior [74, 75]. However, the relationship between 5-HTTLPR and suicidal behavior was not confirmed by all studies [76].
Lower CSF 5-HIAA levels were found in female, but not male, suicide attempters with various psychiatric disorders compared to healthy controls [61]. Additionally, loudness-dependence of auditory evoked potentials (LDAEP)—a measure of serotonergic dysfunction—was stronger in depressed attempters relative to non-attempters, pointing to reduced serotonergic activity in the attempter group [77].
In summary, many, but not all, studies report associations between suicide attempt and abnormalities in genes coding for TPH, some 5-HT receptors, and the transporter. In some cases, there appears to be an interaction between childhood stressors and 5-HTT polymorphisms. This interaction may be explained by the stress-diathesis model, in which the diathesis—a genetic vulnerability represented by a variant of 5-HTTLPR combined with childhood trauma—leads to increased lifetime risk for suicidal behavior in the presence of a stressor.
Other Neurotransmitters: Catecholamines, Glutamate, and GABA
Catecholamines, norepinephrine (NE), and dopamine (DA) participate in the body’s stress response and in the reward system, and thus have been investigated for their potential roles in psychopathology and suicidal behavior. Markers of interest in noradrenergic and dopaminergic systems include NE, DA, tyrosine hydroxylase (TH), an enzyme involved in catecholamine synthesis, NE and DA receptors and transporters, monoamine oxidase A (MAO-A) and catecholamine-O-methyltransferase (COMT), two enzymes involved in catecholamine breakdown, and 3-methoxy-4-hydroxyphenylglycol (MHPG) and homovanillic acid (HVA), metabolites of NE and DA, respectively. See Currier and Mann for an overview [58].
Glutamate (Glu) and gamma-aminobutyric acid (GABA) are the main excitatory and inhibitory neurotransmitters in the brain, respectively. In addition to Glu and GABA, other markers of interest in these two systems include the NMDA, AMPA, and kainate glutamatergic receptors, the glutamate metabotropic receptors, as well as GABAA and GABAB receptors. The link between these neurotransmitters and suicidal behavior is less robust than for the serotonin system.
Recent Findings
There have been few additions to literature in this area in recent years. Of these papers, most examined genetic polymorphisms in suicide attempters.
-
Noradrenergic system: Two studies examined the tyrosine hydroxylase gene, TH, and the NE transporter gene, SLC6A2. In patients with schizophrenia, the presence of the TH SNP rs11564717 (A/G) was associated with a history of suicide attempt [78]. Additionally, suicide attempt risk was increased in homozygous carriers of the TCAT(6) repeat [78]. Variants of the SLC6A2 gene have also shown association with suicidal behavior. Presence of either the rs2242446 or rs28836840 SLC6A2 allele type increased the likelihood of a suicide attempt in depressed patients [79].
-
Dopaminergic system: Results of a study [80] examining the dopamine receptor D3 gene (DRD3) and BDNF are reported in the “Neuronal Plasticity” section below.
-
GABAergic and glutamatergic systems: A large genetic study [81] of family trios with offspring who were suicide attempters examined numerous SNPs across several glutamatergic and GABAergic genes. Two genes of interest were detected: GRIN2B, a glutamate NMDA-receptor gene, and ODC1, a gene for an enzyme in the polyamine synthesis pathway [81]. Two SNPs of GRIN2B (rs2268115 and rs220557) and ODC1 (rs1049500 and rs2302614) were associated with suicide attempt. Additionally, a gene-by-environment interaction was noted between another SNP of ODC1 and history of childhood or adolescent physical assault, which increased the risk of suicide attempt [81].
CSF levels of GABA in a sample of mood disorder patients and healthy controls showed no differences between suicide attempters and non-attempters [82]. No association was found between suicide attempts and 119 SNPs in several GABAergic and glutamatergic genes [83], though a link between suicide and GABA receptor G2 gene, GABRG2, was noted. The same gene has been previously linked to suicide attempt in patients with schizophrenia and histories of substance use disorders [84].
More research is needed to further elucidate the relationship between catecholamines, glutamate and GABA, and suicide attempts given the promising but inconclusive findings to date.
Inflammation
Given their connection to the HPA-axis and serotonin precursors, pro-inflammatory cytokines and other markers of inflammation have long been of interest to researchers. The main inflammatory markers studied in suicidal behavior include interleukins (IL-1β, IL-2, IL-4, IL-6, IL-8, IL-10, IL-13), C-reactive protein (CRP), kynurenine (KYN), quinolinic acid (QUIN), picolinic acid (PIC), tumor necrosis factor alpha (TNF-α), transforming growth factor beta (TGF-β), vascular endothelial growth factor (VEGF), interferon alpha (INF-α), and interferon gamma (INF-γ). For an overview of older findings, see the following reviews and meta-analyses [85••, 86••, 87].
Recent Findings
Studies [88••, 89, 90] examining PIC, QUIN, and KYN in suicide attempters with mixed psychopathology relative to healthy controls found higher CSF QUIN in suicide attempters. The differences were most prominent right after a suicide attempt occurred and, although the differences declined over time, they remained statistically significant [88••]. PIC levels were lower in the CSF and plasma of suicide attempters compared to healthy volunteers [90]. Within the attempter group, those with violent attempts had higher QUIN levels than those with non-violent ones [89], but there were no differences in PIC levels in these two groups [90]. QUIN levels were also associated with higher levels of suicide intent [89]. Although lower KYN levels in suicide attempters relative to controls and a negative association between KYN and suicidal ideation or intent scores were reported [88], not all studies found differences between groups [89]. These studies, however, lacked psychiatric control groups, which makes interpretation of findings difficult in terms of separating correlates of the psychiatric disorder from correlates of the diathesis for suicidal behavior. Another study compared plasma KYN and tryptophan (TRP)—a precursor of serotonin—in depressed adolescent suicidal patients (including attempters and patients with active ideation), non-suicidal patients, and healthy controls. Lower TRP and a higher KYN/TRP ratio were found in the suicidal group relative to both healthy and patient control groups [91]. These findings suggest that tryptophan is being shunted away from serotonin and towards KYN, as might result from inflammation activating the responsible enzyme, indoleamine 2, 3-dioxygenase (IDO). Whether this occurs in the brain is uncertain, but more KYN has a further pro-inflammatory effects. It can also be converted to quinolinic acid (QUIN).
In suicide attempters across diagnoses compared to healthy controls, CSF IL-6 levels were positively correlated with QUIN levels [89] and with suicidal ideation scores [88••]. IL-6 levels in suicide attempters were also related to endophenotypes of suicidal behavior [92]. Both CSF and plasma IL-6 levels positively correlated with extraversion in attempters. When extraversion was broken down into two sub-categories—monotony aversion and impulsivity—plasma IL-6 levels correlated with both, whereas CSF IL-6 levels were only correlated with monotony avoidance. Interestingly, higher plasma and CSF IL-6 levels were also reported in association with more violent suicide attempts [92]. Cytokines should increase production of both KYN and QUIN. The downstream effects of inflammation may alter mood, behavior, and risk for suicidal behavior.
Suicide attempters compared to psychiatric controls with only suicidal ideation and non-suicidal patients with mood and psychotic disorders had higher serum CRP levels [93]. A 2.7 time increase in CRP corresponded to a 127% increase in the odds ratio of a suicide attempt. Plasma CRP levels correlated with suicide intent, but not with number of attempts or degree of violence of the index attempt method [94]. Not all studies agreed. One study of attempters, non-attempters with mixed psychopathology, and healthy controls did not find plasma CRP differences between these groups [95]. However, more soluble urokinase-type plasminogen activator receptor (suPAR)—a marker of low-grade inflammation—was observed in suicide attempters relative to controls, but not the patient sample, suggesting a relationship to psychiatric diagnosis but not suicidal behavior.
Oxidative and nitrosative stress has also been linked to suicide attempt. Attempters across diagnoses had higher plasma levels of nitric oxide metabolites and lipid hydroperoxidases (a marker of oxidative damage to lipids) and lowered total antioxidant potential, an index of antioxidant defenses [96]. The same study found no correlation between suicide attempt and inflammatory markers, including CRP, IL-6, and TNF-α.
Only one study examined genetic polymorphisms of genes related to inflammatory markers in suicide attempters. The GG genotype of TNF-α −308 G > A polymorphism was associated with suicide attempt in a sample of depressed patients; no associations were observed for IFN-γ or IL-10 SNPs [97].
In general, findings indicate an association between suicidal behavior and inflammation. Future research in this area could help further delineate how inflammation can affect mood regulation, decision-making, and other components of the diathesis to alter the risk for suicide attempts.
Lipids
Lipids may also play a role in the pathophysiology of suicidal behavior. To date, markers of interest in this area include triglycerides (TGs), total cholesterol (TC), HDL cholesterol (HDL-C), LDL cholesterol (LDL-C), polyunsaturated fatty acids (PUFAs), and apolipoproteins. For a detailed analysis of previous findings, see the meta-analysis by Wu et al. [98••].
Recent Findings
In mood disorders, one study of suicide attempters found lower serum TG levels relative to non-attempters, but no difference in total cholesterol, HDL-C, LDL-C, or leptin levels [99]. Another study found lower serum TG levels in recent attempters compared with non-attempters [100]. Here, however, elevated HDL-C levels were noted in the recent attempter group. Given that depression presents with changes in appetite and weight, it is unclear whether these findings are related to suicidal behavior or the severity of underlying psychopathology.
In contrast to findings discussed above [99], lower plasma TC levels were found in suicide attempters with mixed psychopathology relative to healthy controls [101]. However, because psychiatric controls were absent, it is unclear whether findings represent a marker of suicidal behavior or psychopathology.
Other markers have also been considered. One older study found that omega-3 series PUFAs predict the risk for suicide attempts in bipolar disorder [102]. Since these PUFAs are anti-inflammatory, this observation links findings in lipids and inflammation to suicidal behavior. Apolipoprotein E (ApoE)—a molecule involved in immunity and cognitive function [103]—was elevated in the plasma of those suicide attempters with higher numbers of lifetime suicide attempts, regardless of diagnosis. On the other hand, plasma eicosapentaenoic acid levels did not differentiate attempters from non-attempters in a depressed sample with substance use disorders [104].
One epigenetic study [105] explored polymorphisms affecting the biosynthetic pathway of long-chain PUFAs. Depressed suicide attempters, relative to non-attempters, showed altered methylation patterns in the Elovl5 gene whose products participate in the elongation of very long-chain fatty acids. Higher levels of CpG methylation were noted upstream, whereas lower levels were reported in the downstream TSS region of Elovl5 in attempters. In contrast, no correlation was found between suicide attempts and either SNPs [106] or methylation [105] of fatty acid desaturase genes, Fads1 and Fads2.
Suicidal behavior was also examined within the context of obesity and bariatric surgery. According to two systematic reviews, obesity may be protective with respect to suicide death; the relationship between BMI and suicide attempt, however, was less clear [107, 108]. Bariatric surgery, on the other hand, was shown to increase the risk of self-harm, particularly in patients with a history of depression, but not of death by suicide [109, 110].
Diverse evidence links lipid indices to suicidal behavior. Such indices offer a number of therapeutic targets with prevention potential. Future studies need to explain the mechanistic link between suicidal behavior diathesis and lipids. Lipids could increase risk via effects on neurotransmitter systems like the dopamine system or via the inflammasome.
Neuronal Plasticity
Neuronal plasticity is the process by which the nervous system adapts to changing environmental demands. Given the structural and functional changes observed in the brains of suicide attempters, it is reasonable to investigate the molecular processes by which they may occur. Trophic factors mediate neuronal plasticity. Research has examined brain-derived neurotrophic factor (BDNF)—a growth factor implicated in development, differentiation, and functioning of neurons—and tropomyosin-receptor kinase B (TrkB), a receptor for BDNF [111]. For a summary of older literature, see Dwivedi [112].
Recent Findings
Studies of BDNF in suicide attempters have generated mixed results. A study of an ethnically diverse sample of self-harming patients with unspecified psychopathology found a gene-by-environment interaction between the homozygous Val-Val genotype and childhood emotional environment. Val-Val carriers who reported a less supportive, invalidating emotional environment during childhood were more likely to attempt suicide than Met-carriers or individuals with more supportive emotional environments [113]. Other genetic studies of BDNF also suggest an association between the Val66Met BDNF polymorphism and suicidal ideation or behavior. Carriers of the Val-Val genotype in a Mexican sample of bipolar patients were more likely to have a history of suicide attempt than Val-Met or Met-Met carriers [114], suggesting a potential protective role of the Met allele. Although these findings suggest that the Val-Val genotype confers a vulnerability to suicidal behavior, not all studies agree. A study of patients with schizophrenia found an interaction between the BDNF Met-allele, the dopamine receptor DRD3 Ser9Gly polymorphism, and a history of suicide attempt, although these findings were not replicated in a larger sample [80]. Finally, suicide attempt history in depressed patients was reported to be associated with greater BDNF promoter methylation and presumably less expression [115].
Studies of BDNF serum levels yielded less promising results. Only one study found a correlation between lower serum BDNF levels and suicide attempt in personality and adjustment disorders [116]. These findings could not be replicated in mood disorders [99, 116] or other psychopathology [117]. Serum BDNF levels also did not differentiate between attempters using violent versus non-violent suicide methods [99].
To summarize, the Met allele of the Val66Met BDNF has been reported to be associated with both increased and lower risk of a suicide attempt. More research is needed in this area to further explore this relationship.
Conclusions
Suicide risk assessment currently relies on a patient’s voluntary self-report and a clinician’s judgment. A more objective, biologically based model of suicide risk assessment may yield biomarkers with increased prediction accuracy, facilitate identification of high-risk patients, and focus more intense preventive interventions on that group.
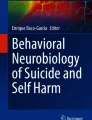
We have reviewed several candidate biomarkers, some showing more promise than others. At present, it appears that the most promising potential biomarkers of suicide attempt may emerge from imaging the serotonergic system and from blood measures of the inflammasome, lipids, and possibly molecules involved in neuronal plasticity. Biochemically, many of these factors are interrelated (see Fig. 1). Early life trauma sensitizes the HPA-axis resulting in higher cortisol levels in response to stress later in life. Cortisol modulates the serotonin system, neuronal survival, and inflammatory processes. Serotonin, on the other hand, shares a common precursor—tryptophan—with inflammatory indices KYN and QUIN. Further research employing a prospective design with larger samples involving several diagnostic groups and multiple biomarkers from different systems is needed to develop a comprehensive biological predictive model of suicidal behavior.

Model of connections between biomarkers associated with suicidal behavior. 5-HT serotonin, ACTH adrenocorticotropic hormone, ApoE apolipiprotein E, BDNF brain-derived neurotrophic factor, CRH corticotropin-releasing hormone, DA dopamine, IDO indoleamine 2,3-dioxygenase, KYN kynurenine, NE norepinephrine, PUFAs polyunsaturated fatty acids, QUIN quinolinic acid, SNS sympathetic nervous system, Trp tryptophan, VTA ventral tegmental area
References
Papers of Particular Interest, Published Recently, Have Been Highlighted as: • Of Importance •• Of Major Importance
World Health Organization. Preventing suicide: A global imperative: World Health Organization; 2014. Available from: http://apps.who.int/iris/bitstream/10665/131056/1/9789241564779_eng.pdf?ua=1&ua=1.
Centers for Disease Control and Prevention. Web-based injury statistics query and reporting system (WISQARS). National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (2014) Retrieved from: http://www.cdc.gov/injury/wisqars/index.html.
Murphy S, Kochanek K, Xu J, Arias E. Mortality in the United States, 2014. NCHS data brief, no 229. Hyattsville, MD: National Center for Health Statistics; 2015.
Centers for Disease Control and Prevention. Suicide: Facts at a Glance 2015. May 28, 2016. Available from: http://www.cdc.gov/violenceprevention/pdf/suicide-datasheet-a.pdf.
• Oquendo MA, Sullivan GM, Sudol K, Baca-Garcia E, Stanley BH, Sublette ME, et al. Toward a biosignature for suicide. Am J Psychiatry. 2014;171(12):1259–77. A review of literature examining biomarkers associated with death by suicide
Posner K, Oquendo MA, Gould M, Stanley B, Davies M. Columbia classification algorithm of suicide assessment (C-CASA): classification of suicidal events in the FDA's pediatric suicidal risk analysis of antidepressants. Am J Psychiatry. 2007;164(7):1035–43.
Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry. 2003;64(1):14–9.
Aguilar EJ, Garcia-Marti G, Marti-Bonmati L, Lull JJ, Moratal D, Escarti MJ, et al. Left orbitofrontal and superior temporal gyrus structural changes associated to suicidal behavior in patients with schizophrenia. Prog Neuro-Psychopharmacol Biol Psychiatry. 2008;32(7):1673–6.
Benedetti F, Radaelli D, Poletti S, Locatelli C, Falini A, Colombo C, et al. Opposite effects of suicidality and lithium on gray matter volumes in bipolar depression. J Affect Disord. 2011;135(1–3):139–47.
Hwang JP, Lee TW, Tsai SJ, Chen TJ, Yang CH, Lirng JF, et al. Cortical and subcortical abnormalities in late-onset depression with history of suicide attempts investigated with MRI and voxel-based morphometry. J Geriatr Psychiatry Neurol. 2010;23(3):171–84.
Dombrovski AY, Siegle GJ, Szanto K, Clark L, Reynolds CF, Aizenstein H. The temptation of suicide: striatal gray matter, discounting of delayed rewards, and suicide attempts in late-life depression. Psychol Med. 2012;42(6):1203–15.
Soloff PH, Pruitt P, Sharma M, Radwan J, White R, Diwadkar VA. Structural brain abnormalities and suicidal behavior in borderline personality disorder. J Psychiatr Res. 2012;46(4):516–25.
Rusch N, Spoletini I, Wilke M, Martinotti G, Bria P, Trequattrini A, et al. Inferior frontal white matter volume and suicidality in schizophrenia. Psychiatry Res. 2008;164(3):206–14.
Cyprien F, Courtet P, Malafosse A, Maller J, Meslin C, Bonafe A, et al. Suicidal behavior is associated with reduced corpus callosum area. Biol Psychiatry. 2011;70(4):320–6.
Spoletini I, Piras F, Fagioli S, Rubino IA, Martinotti G, Siracusano A, et al. Suicidal attempts and increased right amygdala volume in schizophrenia. Schizophr Res. 2011;125(1):30–40.
Monkul ES, Hatch JP, Nicoletti MA, Spence S, Brambilla P, Lacerda AL, et al. Fronto-limbic brain structures in suicidal and non-suicidal female patients with major depressive disorder. Mol Psychiatry. 2007;12(4):360–6.
Ahearn EP, Jamison KR, Steffens DC, Cassidy F, Provenzale JM, Lehman A, et al. MRI correlates of suicide attempt history in unipolar depression. Biol Psychiatry. 2001;50(4):266–70.
Ehrlich S, Breeze JL, Hesdorffer DC, Noam GG, Hong X, Alban RL, et al. White matter hyperintensities and their association with suicidality in depressed young adults. J Affect Disord. 2005;86(2–3):281–7.
Ehrlich S, Noam GG, Lyoo IK, Kwon BJ, Clark MA, Renshaw PF. White matter hyperintensities and their associations with suicidality in psychiatrically hospitalized children and adolescents. J Am Acad Child Adolesc Psychiatry. 2004;43(6):770–6.
Pompili M, Ehrlich S, De Pisa E, Mann JJ, Innamorati M, Cittadini A, et al. White matter hyperintensities and their associations with suicidality in patients with major affective disorders. Eur Arch Psychiatry Clin Neurosci. 2007;257(8):494–9.
Pompili M, Innamorati M, Mann JJ, Oquendo MA, Lester D, Del Casale A, et al. Periventricular white matter hyperintensities as predictors of suicide attempts in bipolar disorders and unipolar depression. Prog Neuro-Psychopharmacol Biol Psychiatry. 2008;32(6):1501–7.
Pan LA, Ramos L, Segreti A, Brent DA, Phillips ML. Right superior temporal gyrus volume in adolescents with a history of suicide attempt. Br J Psychiatry. 2015;206(4):339–40.
Lee YJ, Kim S, Gwak AR, Kim SJ, Kang S-G, Na K-S, et al. Decreased regional gray matter volume in suicide attempters compared to suicide non-attempters with major depressive disorders. Compr Psychiatry. 2016;67:59–65.
Peng H, Wu K, Li J, Qi H, Guo S, Chi M, et al. Increased suicide attempts in young depressed patients with abnormal temporal-parietal-limbic gray matter volume. J Affect Disord. 2014;165:69–73.
Colle R, Chupin M, Cury C, Vandendrie C, Gressier F, Hardy P, et al. Depressed suicide attempters have smaller hippocampus than depressed patients without suicide attempts. J Psychiatr Res. 2015;61:13–8.
Ding Y, Lawrence N, Olie E, Cyprien F, le Bars E, Bonafe A, et al. Prefrontal cortex markers of suicidal vulnerability in mood disorders: a model-based structural neuroimaging study with a translational perspective. Transl Psychiatry. 2015;5(2):e516.
Giakoumatos CI, Tandon N, Shah J, Mathew IT, Brady RO, Clementz BA, et al. Are structural brain abnormalities associated with suicidal behavior in patients with psychotic disorders? J Psychiatr Res. 2013;47(10):1389–95.
Besteher B, Wagner G, Koch K, Schachtzabel C, Reichenbach JR, Schlosser R, et al. Pronounced prefronto-temporal cortical thinning in schizophrenia: neuroanatomical correlate of suicidal behavior? Schizophr Res. 2016;176(2):151–7.
Gifuni AJ, Ding Y, Olié E, Lawrence N, Cyprien F, Le Bars E, et al. Subcortical nuclei volumes in suicidal behavior: nucleus accumbens may modulate the lethality of acts. Brain Imaging Behav. 2016;10(1):96–104.
Soloff P, White R, Diwadkar VA. Impulsivity, aggression and brain structure in high and low lethality suicide attempters with borderline personality disorder. Psychiatry Res. 2014;222(3):131–9.
Lijffijt M, Rourke ED, Swann AC, Zunta-Soares GB, Soares JC. Illness-course modulates suicidality-related prefrontal gray matter reduction in women with bipolar disorder. Acta Psychiatr Scand. 2014;130(5):374–87.
Mahon K, Burdick KE, Wu J, Ardekani BA, Szeszko PR. Relationship between suicidality and impulsivity in bipolar I disorder: a diffusion tensor imaging study. Bipolar Disord. 2012;14(1):80–9.
Jia Z, Huang X, Wu Q, Zhang T, Lui S, Zhang J, et al. High-field magnetic resonance imaging of suicidality in patients with major depressive disorder. Am J Psychiatry. 2010;167(11):1381–90.
• Olvet DM, Peruzzo D, Thapa-Chhetry B, Sublette ME, Sullivan GM, Oquendo MA, et al. A diffusion tensor imaging study of suicide attempters. J Psychiatr Res. 2014;51:60–7. This imaging study of brain white matter tracts identified the dorsomedial PFC as a potential region of interest for understanding the diathesis of suicidal behavior
• Jia Z, Wang Y, Huang X, Kuang W, Wu Q, Lui S, et al. Impaired frontothalamic circuitry in suicidal patients with depression revealed by diffusion tensor imaging at 3.0 T. J Psychiatry Neurosci. 2014;39(3):170–7. This imaging study of brain white matter tracts found abnormalities in the frontothalamic pathways of depressed patients and that these abnormalities are more pronounced in suicide attemtpers compared to non-attempters
Cyprien F, de Champfleur NM, Deverdun J, Olie E, Le Bars E, Bonafe A, et al. Corpus Callosum integrity is affected by mood disorders and also by the suicide attempt history: a diffusion tensor imaging study. J Affect Disord. 2016;206:115–24.
Kim B, Oh J, Kim MK, Lee S, Tae WS, Kim CM, et al. White matter alterations are associated with suicide attempt in patients with panic disorder. J Affect Disord. 2015;175:139–46.
Lee SJ, Kim B, Oh D, Kim MK, Kim KH, Bang SY, et al. White matter alterations associated with suicide in patients with schizophrenia or schizophreniform disorder. Psychiatry Res. 2016;248:23–9.
• Sachs-Ericsson N, Hames JL, Joiner TE, Corsentino E, Rushing NC, Palmer E, et al. Differences between suicide attempters and nonattempters in depressed older patients: depression severity, white-matter lesions, and cognitive functioning. Am J Geriatr Psychiatry. 2014;22(1):75–85. This study showed that white matter lesions differentiated older depressed suicide attempters from non-attempters
Jollant F, Lawrence NS, Giampietro V, Brammer MJ, Fullana MA, Drapier D, et al. Orbitofrontal cortex response to angry faces in men with histories of suicide attempts. Am J Psychiatry. 2008;165(6):740–8.
Jollant F, Lawrence NS, Olie E, O'Daly O, Malafosse A, Courtet P, et al. Decreased activation of lateral orbitofrontal cortex during risky choices under uncertainty is associated with disadvantageous decision-making and suicidal behavior. NeuroImage. 2010;51(3):1275–81.
Pan LA, Batezati-Alves SC, Almeida JR, Segreti A, Akkal D, Hassel S, et al. Dissociable patterns of neural activity during response inhibition in depressed adolescents with and without suicidal behavior. J Am Acad Child Adolesc Psychiatry. 2011;50(6):602–11.
Olie E, Ding Y, Le Bars E, de Champfleur NM, Mura T, Bonafe A, et al. Processing of decision-making and social threat in patients with history of suicidal attempt: a neuroimaging replication study. Psychiatry Res. 2015;234(3):369–77.
Pan L, Segreti A, Almeida J, Jollant F, Lawrence N, Brent D, et al. Preserved hippocampal function during learning in the context of risk in adolescent suicide attempt. Psychiatry Res. 2013;211(2):112–8.
Pan LA, Hassel S, Segreti AM, Nau SA, Brent DA, Phillips ML. Differential patterns of activity and functional connectivity in emotion processing neural circuitry to angry and happy faces in adolescents with and without suicide attempt. Psychol Med. 2013;43(10):2129–42.
Dombrovski AY, Szanto K, Clark L, Reynolds CF, Siegle GJ. Reward signals, attempted suicide, and impulsivity in late-life depression. JAMA Psychiatry. 2013;70(10):1020–30.
Vanyukov PM, Szanto K, Siegle GJ, Hallquist MN, Reynolds 3rd CF, Aizenstein HJ, et al. Impulsive traits and unplanned suicide attempts predict exaggerated prefrontal response to angry faces in the elderly. Am J Geriatr Psychiatry. 2015;23(8):829–39.
Vanyukov PM, Szanto K, Hallquist MN, Siegle GJ, Reynolds 3rd CF, Forman SD, et al. Paralimbic and lateral prefrontal encoding of reward value during intertemporal choice in attempted suicide. Psychol Med. 2016;46(2):381–91.
Richard-Devantoy S, Ding Y, Lepage M, Turecki G, Jollant F. Cognitive inhibition in depression and suicidal behavior: a neuroimaging study. Psychol Med. 2016;46(5):933–44.
Cannon DM, Ichise M, Fromm SJ, Nugent AC, Rollis D, Gandhi SK, et al. Serotonin transporter binding in bipolar disorder assessed using [11C]DASB and positron emission tomography. Biol Psychiatry. 2006;60(3):207–17.
Oquendo MA, Placidi GP, Malone KM, Campbell C, Keilp J, Brodsky B, et al. Positron emission tomography of regional brain metabolic responses to a serotonergic challenge and lethality of suicide attempts in major depression. Arch Gen Psychiatry. 2003;60(1):14–22.
Miller JM, Hesselgrave N, Ogden RT, Sullivan GM, Oquendo MA, Mann JJ, et al. Positron emission tomography quantification of serotonin transporter in suicide attempters with major depressive disorder. Biol Psychiatry. 2013;74(4):287–95.
Yeh Y-W, Ho P-S, Chen C-Y, Kuo S-C, Liang C-S, Ma K-H, et al. Incongruent reduction of serotonin transporter associated with suicide attempts in patients with major depressive disorder: a positron emission tomography study with 4-[18F]-ADAM. Int J Neuropsychopharmacol. 2015;18(3):pyu065.
Nye JA, Purselle D, Plisson C, Voll RJ, Stehouwer JS, Votaw JR, et al. Decreased brainstem and putamen SERT binding potential in depressed suicide attempters using [11C]-zient PET imaging. Depress Anxiety. 2013;30(10):902–7.
Sublette ME, Milak MS, Galfalvy HC, Oquendo MA, Malone KM, Mann JJ. Regional brain glucose uptake distinguishes suicide attempters from non-attempters in major depression. Arch Suicide Res. 2013;17(4):434–47.
Sullivan GM, Oquendo MA, Milak M, Miller JM, Burke A, Ogden RT, et al. Positron emission tomography quantification of serotonin(1A) receptor binding in suicide attempters with major depressive disorder. JAMA Psychiatry. 2015;72(2):169–78.
• Oquendo MA, Galfalvy H, Sullivan GM, Miller JM, Milak MM, Sublette ME, et al. Positron emission tomographic imaging of the serotonergic system and prediction of risk and lethality of future suicidal behavior. JAMA Psychiatry. 2016;73(10):1048–55. This longitudinal prospective observational study of moderately depressed patients showed that higher serotonin 1A autoreceptor binding, which results in less serotonin being released, predicted more severe suicidal ideation up to one year after the brain scan and the lethality of suicide attempts up to two years following the brain scan .
Currier D, Mann JJ. Stress, genes and the biology of suicidal behavior. Psychiatr Clin North Am. 2008;31(2):247–69.
Keilp JG, Stanley BH, Beers SR, Melhem NM, Burke AK, Cooper TB, et al. Further evidence of low baseline cortisol levels in suicide attempters. J Affect Disord. 2016;190:187–92.
• Melhem NM, Keilp JG, Porta G, Oquendo MA, Burke A, Stanley B, et al. Blunted HPA axis activity in suicide attempters compared to those at high risk for suicidal behavior. Neuropsychopharmacology. 2016;41(6):1447–56. This study was able to distinguish suicide attempters from individuals with suicide-related behaviors (but no attempts) using indices of HPA-axis activity. Other studies have reported that HPA axis abnormalities also predict risk of dying by suicide
Chatzittofis A, Nordstrom P, Hellstrom C, Arver S, Asberg M, Jokinen J. CSF 5-HIAA, cortisol and DHEAS levels in suicide attempters. Eur Neuropsychopharmacol. 2013;23(10):1280–7.
Yin H, Galfalvy H, Pantazatos SP, Huang YY, Rosoklija GB, Dwork AJ, et al. Glucocorticoid receptor-related genes: genotype and brain gene expression relationships to suicide and major depressive disorder. Depress Anxiety. 2016;33(6):531–40.
Brent D, Melhem N, Ferrell R, Emslie G, Wagner KD, Ryan N, et al. Association of FKBP5 polymorphisms with suicidal events in the treatment of resistant depression in adolescents (TORDIA) study. Am J Psychiatry. 2009;167(2):190–7.
Roy A, Gorodetsky E, Yuan Q, Goldman D, Enoch MA. Interaction of FKBP5, a stress-related gene, with childhood trauma increases the risk for attempting suicide. Neuropsychopharmacology. 2010;35(8):1674–83.
Roy A, Hodgkinson CA, DeLuca V, Goldman D, Enoch MA. Two HPA axis genes, CRHBP and FKBP5, interact with childhood trauma to increase the risk for suicidal behavior. J Psychiatr Res. 2012;46(1):72–9.
Willour VL, Chen H, Toolan J, Belmonte P, Cutler DJ, Goes FS, et al. Family-based association of FKBP5 in bipolar disorder. Mol Psychiatry. 2009;14(3):261–8.
Mann JJ. The serotonergic system in mood disorders and suicidal behaviour. Philos Trans R Soc Lond Ser B Biol Sci. 2013;368(1615):20120537.
Karanovic J, Ivkovic M, Jovanovic VM, Pantovic M, Pavlovic-Jankovic N, Damjanovic A, et al. Tryptophan hydroxylase 1 variant rs1800532 is associated with suicide attempt in Serbian psychiatric patients but does not moderate the effect of recent stressful life events. Suicide Life Threat Behav. 2016;46(6):664–8.
Lopez-Narvaez ML, Tovilla-Zarate CA, Gonzalez-Castro TB, Juarez-Rojop I, Pool-Garcia S, Genis A, et al. Association analysis of TPH-1 and TPH-2 genes with suicidal behavior in patients with attempted suicide in Mexican population. Compr Psychiatry. 2015;61:72–7.
Zhang Y, Chang Z, Chen J, Ling Y, Liu X, Feng Z, et al. Methylation of the tryptophan hydroxylase2 gene is associated with mRNA expression in patients with major depression with suicide attempts. Mol Med Rep. 2015;12(2):3184–90.
Donaldson ZR, le Francois B, Santos TL, Almli LM, Boldrini M, Champagne FA, et al. The functional serotonin 1a receptor promoter polymorphism, rs6295, is associated with psychiatric illness and differences in transcription. Transl Psychiatry. 2016;6(3):e746.
Karanovic J, Svikovic S, Pantovic M, Durica S, Brajuskovic G, Damjanovic A, et al. Joint effect of ADARB1 gene, HTR2C gene and stressful life events on suicide attempt risk in patients with major psychiatric disorders. World J Biol Psychiatry. 2015;16(4):261–71.
• Perroud N, Zewdie S, Stenz L, Adouan W, Bavamian S, Prada P, et al. Methylation of serotonin receptor 3a in ADHD, borderline personality, and bipolar disorders: link with severity of the disorders and childhood maltreatment. Depress Anxiety. 2016;33(1):45–55. This study shows a link between early childhood maltreatment, epigenetic changes in the serotonin receptor 3A, and suicidal behavior
Benedetti F, Riccaboni R, Poletti S, Radaelli D, Locatelli C, Lorenzi C, et al. The serotonin transporter genotype modulates the relationship between early stress and adult suicidality in bipolar disorder. Bipolar Disord. 2014;16(8):857–66.
Enoch MA, Hodgkinson CA, Gorodetsky E, Goldman D, Roy A. Independent effects of 5′ and 3′ functional variants in the serotonin transporter gene on suicidal behavior in the context of childhood trauma. J Psychiatr Res. 2013;47(7):900–7.
Lee HY, Hong JP, Hwang JA, Lee HJ, Yoon HK, Lee BH, et al. Possible association between serotonin transporter gene polymorphism and suicide behavior in major depressive disorder. Psychiatry Investig. 2015;12(1):136–41.
Kim DH, Park YM. The association between suicidality and serotonergic dysfunction in depressed patients. J Affect Disord. 2013;148(1):72–6.
Hu J, Chan LF, Souza RP, Tampakeras M, Kennedy JL, Zai C, et al. The role of tyrosine hydroxylase gene variants in suicide attempt in schizophrenia. Neurosci Lett. 2014;559:39–43.
Kim YK, Hwang JA, Lee HJ, Yoon HK, Ko YH, Lee BH, et al. Association between norepinephrine transporter gene (SLC6A2) polymorphisms and suicide in patients with major depressive disorder. J Affect Disord. 2014;158:127–32.
Zai CC, Manchia M, Sonderby IE, Yilmaz Z, De Luca V, Tiwari AK, et al. Investigation of the genetic interaction between BDNF and DRD3 genes in suicidical behaviour in psychiatric disorders. World J Biol Psychiatry. 2015;16(3):171–9.
Sokolowski M, Ben-Efraim YJ, Wasserman J, Wasserman D. Glutamatergic GRIN2B and polyaminergic ODC1 genes in suicide attempts: associations and gene-environment interactions with childhood/adolescent physical assault. Mol Psychiatry. 2013;18(9):985–92.
Mann JJ, Oquendo MA, Watson KT, Boldrini M, Malone KM, Ellis SP, et al. Anxiety in major depression and cerebrospinal fluid free gamma-aminobutyric acid. Depress Anxiety. 2014;31(10):814–21.
Yin H, Pantazatos SP, Galfalvy H, Huang YY, Rosoklija GB, Dwork AJ, et al. A pilot integrative genomics study of GABA and glutamate neurotransmitter systems in suicide, suicidal behavior, and major depressive disorder. Am J Med Genet B Neuropsychiatr Genet. 2016;171B(3):414–26.
Zai CC, Zai GC, Tiwari AK, Manchia M, de Luca V, Shaikh SA, et al. Association study of GABRG2 polymorphisms with suicidal behaviour in schizophrenia patients with alcohol use disorder. Neuropsychobiology. 2014;69(3):154–8.
•• Black C, Miller BJ. Meta-analysis of cytokines and chemokines in suicidality: distinguishing suicidal versus nonsuicidal patients. Biol Psychiatry. 2015;78(1):28–37. This meta-analysis showed that certain cytokines may distinguish suicidal patients from nonsuicidal patients across different diagnoses
•• Gananca L, Oquendo MA, Tyrka AR, Cisneros-Trujillo S, Mann JJ, Sublette ME. The role of cytokines in the pathophysiology of suicidal behavior. Psychoneuroendocrinology. 2016;63:296–310. An extensive meta-analysis of the role of cytokines in suicidal behavior
Serafini G, Pompili M, Elena Seretti M, Stefani H, Palermo M, Coryell W, et al. The role of inflammatory cytokines in suicidal behavior: a systematic review. Eur Neuropsychopharmacol. 2013;23(12):1672–86.
•• Bay-Richter C, Linderholm KR, Lim CK, Samuelsson M, Traskman-Bendz L, Guillemin GJ, et al. A role for inflammatory metabolites as modulators of the glutamate N-methyl-D-aspartate receptor in depression and suicidality. Brain Behav Immun. 2015;43:110–7. This study provides longitudinal data demonstrating increased inflammation and abnormal functioning of the kynurenine pathway in the brain of suicide attempters
Erhardt S, Lim CK, Linderholm KR, Janelidze S, Lindqvist D, Samuelsson M, et al. Connecting inflammation with glutamate agonism in suicidality. Neuropsychopharmacology. 2013;38(5):743–52.
Brundin L, Sellgren CM, Lim CK, Grit J, Palsson E, Landen M, et al. An enzyme in the kynurenine pathway that governs vulnerability to suicidal behavior by regulating excitotoxicity and neuroinflammation. Transl Psychiatry. 2016;6(8):e865.
Bradley KA, Case JA, Khan O, Ricart T, Hanna A, Alonso CM, et al. The role of the kynurenine pathway in suicidality in adolescent major depressive disorder. Psychiatry Res. 2015;227(2–3):206–12.
Isung J, Aeinehband S, Mobarrez F, Nordstrom P, Runeson B, Asberg M, et al. High interleukin-6 and impulsivity: determining the role of endophenotypes in attempted suicide. Transl Psychiatry. 2014;4:e470.
Gibbs HM, Davis L, Han X, Clothier J, Eads LA, Caceda R. Association between C-reactive protein and suicidal behavior in an adult inpatient population. J Psychiatr Res. 2016;79:28–33.
Courtet P, Jaussent I, Genty C, Dupuy AM, Guillaume S, Ducasse D, et al. Increased CRP levels may be a trait marker of suicidal attempt. Eur Neuropsychopharmacol. 2015;25(10):1824–31.
Ventorp F, Gustafsson A, Traskman-Bendz L, Westrin A, Ljunggren L. Increased soluble urokinase-type plasminogen activator receptor (suPAR) levels in plasma of suicide attempters. PLoS One. 2015;10(10):e0140052.
Vargas HO, Nunes SO, Pizzo de Castro M, Bortolasci CC, Sabbatini Barbosa D, Kaminami Morimoto H, et al. Oxidative stress and lowered total antioxidant status are associated with a history of suicide attempts. J Affect Disord. 2013;150(3):923–30.
Kim YK, Hong JP, Hwang JA, Lee HJ, Yoon HK, Lee BH, et al. TNF-alpha -308G>a polymorphism is associated with suicide attempts in major depressive disorder. J Affect Disord. 2013;150(2):668–72.
•• Wu S, Ding Y, Wu F, Xie G, Hou J, Mao P. Serum lipid levels and suicidality: a meta-analysis of 65 epidemiological studies. J Psychiatry Neurosci. 2016;41(1):56–69. A meta-analysis emcomassing a large sample, examining the association between suicidal behavior and serum lipid levels .
da Graca CM, Nardin P, Buffon A, Eidt MC, Antonio Godoy L, Fernandes BS, et al. Serum triglycerides, but not cholesterol or leptin, are decreased in suicide attempters with mood disorders. J Affect Disord. 2015;172:403–9.
Baek JH, Kang ES, Fava M, Mischoulon D, Nierenberg AA, Yu BH, et al. Serum lipids, recent suicide attempt and recent suicide status in patients with major depressive disorder. Prog Neuro-Psychopharmacol Biol Psychiatry. 2014;51:113–8.
Papadopoulou A, Markianos M, Christodoulou C, Lykouras L. Plasma total cholesterol in psychiatric patients after a suicide attempt and in follow-up. J Affect Disord. 2013;148(2–3):440–3.
Sublette ME, Hibbeln JR, Galfalvy H, Oquendo MA, Mann JJ. Omega-3 polyunsaturated essential fatty acid status as a predictor of future suicide risk. Am J Psychiatry. 2006;163(6):1100–2.
Asellus P, Nordstrom P, Nordstrom AL, Jokinen J. Plasma apolipoprotein E and severity of suicidal behaviour. J Affect Disord. 2016;190:137–42.
Beier AM, Lauritzen L, Galfalvy HC, Cooper TB, Oquendo MA, Grunebaum MF, et al. Low plasma eicosapentaenoic acid levels are associated with elevated trait aggression and impulsivity in major depressive disorder with a history of comorbid substance use disorder. J Psychiatr Res. 2014;57:133–40.
Haghighi F, Galfalvy H, Chen S, Huang YY, Cooper TB, Burke AK, et al. DNA methylation perturbations in genes involved in polyunsaturated fatty acid biosynthesis associated with depression and suicide risk. Front Neurol. 2015;6:92.
Sublette ME, Vaquero C, Baca-Garcia E, Pachano G, Huang YY, Oquendo MA, et al. Lack of association of SNPs from the FADS1-FADS2 gene cluster with major depression or suicidal behavior. Psychiatr Genet. 2016;26(2):81–6.
Perera S, Eisen RB, Dennis BB, Bawor M, Bhatt M, Bhatnagar N, et al. Body mass index is an important predictor for suicide: results from a systematic review and meta-analysis. Suicide Life Threat Behav. 2016;46(6):697–736.
Klinitzke G, Steinig J, Bluher M, Kersting A, Wagner B. Obesity and suicide risk in adults--a systematic review. J Affect Disord. 2013;145(3):277–84.
Bhatti JA, Nathens AB, Thiruchelvam D, Grantcharov T, Goldstein BI, Redelmeier DA. Self-harm emergencies after bariatric surgery: a population-based cohort study. JAMA Surg. 2016;151(3):226–32.
Kovacs Z, Valentin JB, Nielsen RE. Risk of psychiatric disorders, self-harm behaviour and service use associated with bariatric surgery. Acta Psychiatr Scand. 2017;135(2):149–58.
Huang EJ, Reichardt LF. Neurotrophins: roles in neuronal development and function. Annu Rev Neurosci. 2001;24:677–736.
Dwivedi Y. Brain-derived neurotrophic factor in suicide pathophysiology. In: Dwivedi Y, editor. The neurobiological basis of suicide. Frontiers in neuroscience. 1st ed. Boca Raton, FL: CRC Press; 2012. p. 139–58.
Bresin K, Sima Finy M, Verona E. Childhood emotional environment and self-injurious behaviors: the moderating role of the BDNF Val66Met polymorphism. J Affect Disord. 2013;150(2):594–600.
Gonzalez-Castro TB, Nicolini H, Lanzagorta N, Lopez-Narvaez L, Genis A, Pool Garcia S, et al. The role of brain-derived neurotrophic factor (BDNF) Val66Met genetic polymorphism in bipolar disorder: a case-control study, comorbidities, and meta-analysis of 16,786 subjects. Bipolar Disord. 2015;17(1):27–38.
Kang HJ, Kim JM, Lee JY, Kim SY, Bae KY, Kim SW, et al. BDNF promoter methylation and suicidal behavior in depressive patients. J Affect Disord. 2013;151(2):679–85.
Grah M, Mihanovic M, Ruljancic N, Restek-Petrovic B, Molnar S, Jelavic S. Brain-derived neurotrophic factor as a suicide factor in mental disorders. Acta Neuropsychiatr. 2014;26(6):356–63.
Eisen RB, Perera S, Bawor M, Dennis BB, El-Sheikh W, DeJesus J, et al. Exploring the association between serum BDNF and attempted suicide. Sci Rep. 2016;6:25229.
Acknowledgements
This work was supported by NIMH PHS grant P50MH090964.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Katherin Sudol declares that she has no conflict of interest.
J. John Mann has received royalties from the Research Foundation for Mental Hygiene for commercial use of the C-SSRS.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Mood Disorders
Rights and permissions
About this article

Cite this article
Sudol, K., Mann, J.J. Biomarkers of Suicide Attempt Behavior: Towards a Biological Model of Risk. Curr Psychiatry Rep 19, 31 (2017). https://doi.org/10.1007/s11920-017-0781-y
Published:
DOI: https://doi.org/10.1007/s11920-017-0781-y