
Abstract
Rabies is a zoonotic disease that is usually transmitted to humans by animal bites. Dogs are the most important vector worldwide. There are encephalitic and paralytic forms of the disease. There are differences in the clinical features of the disease acquired from dogs and bats. Neuroimaging is non-specific. Confirmatory diagnostic laboratory tests for rabies include detection of neutralizing anti-rabies virus antibodies in serum or cerebrospinal fluid and rabies virus antigen or RNA in tissues or fluids. Rabies is preventable after recognized exposures with wound cleansing and administration of rabies vaccine and rabies immune globulin. Rabies is virtually always fatal after clinical disease develops, and there have only been rare survivors. The Milwaukee protocol, which includes therapeutic coma, has been shown to be ineffective and should no longer be used. The development of novel therapeutic approaches may depend on a better understanding of basic mechanisms underlying the disease.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rabies is a terrifying infectious disease that has affected humans since antiquity. Currently, there are about 60,000 human rabies deaths worldwide yearly [1], mostly related to the presence of endemic dog rabies in developing countries in Asia and Africa. In North America, rabies is endemic in wildlife [2], and rabies in bats is an especially important threat for transmission to humans. The vast majority of rabies cases are preventable, but bat bites may not be recognized. However, rabies is virtually always fatal once clinical disease develops. The therapy of rabies in humans is an important challenge in medicine, and the development of effective therapy may depend on an improved understanding of basic mechanisms underlying the pathogenesis of rabies.
Pathogenesis
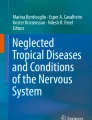
Rabies is a zoonotic infection with rabies virus (RABV) transmission by animal bites. RABV is a negative strand (antisense) RNA virus in the family Rhabdoviridae and genus Lyssavirus. RABV is secreted in the saliva of infected animal vectors and is deposited in the tissues at the bite site. We have learned about the sequential steps involved in rabies pathogenesis from studies in animal models (Fig. 1). After an incubation period, typically lasting weeks or months, in which the virus is known to be close to the site of entry during most of the period, there is viral spread in the peripheral nerves by fast axonal transport to the brainstem or spinal cord (depending on the site of inoculation) followed by dissemination throughout the central nervous system (CNS) along neuroanatomical connections. Subsequently, there is centrifugal spread of the virus from the CNS along the autonomic and sensory nerves to multiple organs (e.g., the heart, adrenal gland, and skin). RABV spreads to the salivary glands in rabies vectors.

Schematic diagram showing the sequential steps in the pathogenesis of rabies after an animal bite/peripheral inoculation of RABV. From [63]
The neuropathology of rabies is characterized by mild inflammatory changes and eosinophilic inclusion bodies in the cytoplasm of infected neurons called Negri bodies. Degenerative neuronal changes are not prominent on routine histopathologic studies. These observations led to the idea that RABV infection causes severe fatal disease by unknown mechanisms producing neuronal dysfunction [3]. In an experimental model of rabies in mice, Jackson and co-workers provided evidence that RABV infection (using a laboratory-adapted RABV strain) selectively injures neuronal processes (dendrites and axons) without producing neuronal death [4]. This injury resulted in few morphologic changes in neurons on routine histopathologic studies in mice inoculated peripherally with RABV, which serves as an excellent model for natural rabies. Further studies of RABV infection in cultured adult rodent dorsal root ganglion (DRG) neurons showed evidence of oxidative stress resulting in axonal swellings and degeneration and impaired axonal growth [5]. Studies of mitochondrial function indicated increased activity of mitochondrial respiratory chain Complex I, a high mitochondrial membrane potential, increased NADH/NAD+ ratio, and reduced ATP content [6]. These studies provide evidence that increased Complex I activity explains reactive oxygen species (ROS) overproduction that was confirmed with measurements of hydrogen peroxide production. RABV P amino acids in the region 139–172 interact with Complex I and increase its activity resulting in increased ROS levels [7].
Clinical Disease
The incubation period after exposure in rabies is variable, typically 20 to 90 days, but ranges from a few days to a year or more. Initially, there are often non-specific prodromal symptoms consisting of fatigue, loss of appetite, headache, insomnia, anxiety, irritability, and fever lasting for up to a period of 10 days. The initial neurological symptoms often include paresthesias, pain, and/or itching at the site of viral entry, which may be a healed bite wound. These symptoms likely reflect infection and associated inflammation in local dorsal root or cranial sensory ganglia. There are two clinical forms of rabies: encephalitic rabies (in ∼80 %) and paralytic rabies (in ∼20 %); fever occurs in both forms. In encephalitic rabies, the burden of infection is thought to involve the brain, whereas in paralytic rabies, it is thought to involve the spinal cord, nerve roots, and peripheral nerves. In encephalitic rabies, there are episodes of generalized arousal or hyperexcitability separated by lucid periods [8]. Autonomic dysfunction may be prominent and include hypersalivation, sweating, and piloerection. This may be caused by direct infection of autonomic nervous system centers or due to involvement of autonomic pathways in the hypothalamus, spinal cord, or ganglia. Hydrophobia occurs in about 50 to 80 % of patients and consists of contractions of the diaphragm and accessory muscles of inspiration with swallowing. Hydrophobia is probably due infection involving brainstem neurons that inhibit inspiratory motor neurons in the vicinity of the nucleus ambiguus [8, 9]. A draft of air on the skin or the breath of an examiner may have the same effect, which has been termed aerophobia. Subsequently, there is progression of the disease with impairment of consciousness and development of quadriparesis. If patients are managed aggressively in a critical care unit, then cardiorespiratory complications and multisystem organ failure commonly develop prior to death. Rabies is virtually always has a fatal outcome within 14 days of the initial symptoms. The duration of survival is strongly influenced by how aggressively the patient is managed and the use of critical care measures.
In paralytic rabies, weakness often initially develops in the bitten limb, and there is progression to quadriparesis with facial weakness. Patients are often alert and are normal mentally when their symptoms first begin. Neurological progression subsequently occurs without the development of hydrophobia, which is followed by death. The development of paralytic rabies is not related to the anatomical site of the bite [10], and survival times are usually longer than for patients with the encephalitic form of the disease [11•]. Rabies may be misdiagnosed as the Guillain-Barré syndrome (acute inflammatory demyelinating polyradiculopathy or the acute motor-sensory neuropathy with predominant axonal involvement (axonal Guillain-Barré syndrome) [12--14]. Sphincter involvement, especially with urinary incontinence, occurs commonly in paralytic rabies, but is not a feature of the Guillain-Barré syndrome [15].
Recently, dog- and bat-acquired rabies were compared in detail based on published case histories [11•]. Specific clinical manifestations are more likely associated with either dog or bat RABV variants. Bat-acquired cases were more likely to be misdiagnosed and to lack a bite history than dog-acquired cases [11•]. Hydrophobia, aerophobia, and encephalopathy are more common in dog-acquired rabies, whereas bat-acquired rabies more frequently has symptoms at the exposure site, tremor, myoclonus, and abnormal cranial nerve, motor, and sensory examinations [11•].
Investigations
Imaging of patients with rabies is mainly performed in order to evaluate for alternative diagnostic conditions that may be considered. In rabies, MR imaging may show lesions involving the gray and/or white matter in the brain or spinal cord, but the lesions are not specific for rabies. Interestingly, MRI findings in the brain and spinal cord are reported to be similar in patients with encephalitic and paralytic rabies [16]. Cerebrospinal fluid (CSF) analysis often is abnormal. A CSF pleocytosis was found in 59 % of cases in the first week of illness and in 87 % after the first week [17]. The white cell count is usually less than 100 cells/μL with predominant mononuclear cells. There may be mild elevation of the CSF protein concentration and CSF glucose is usually normal.
Specific diagnostic laboratory tests for confirming a diagnosis of rabies are for detection of neutralizing anti-rabies virus antibodies in the serum (of a previously unimmunized patient) and CSF, detection of RABV antigen in tissues (typically a nuchal skin biopsy), and/or detection of RABV RNA in saliva, skin biopsy, or CSF. RABV antigen may be detected antemortem by using the immunofluorescent antibody staining of skin biopsies. Skin biopsies containing hair follicles should be obtained by using a full-thickness punch biopsy from the posterior region of the neck at the hairline. Many sections should be taken that include several hair follicles. Fluorescent antibody staining should be performed for RABV antigen, which is present in adjacent small sensory nerves [18, 19]. Corneal impression smears have also been used for rabies antigen detection, but this diagnostic method has low sensitivity and false positive results may occur [17, 19–22]. RABV RNA from saliva, skin biopsies, brain tissue, and CSF can be amplified using the reverse transcriptase polymerase chain reaction. This technique, especially when applied to saliva samples, has proven to be an important advance in the laboratory diagnosis of rabies. RABV RNA was detected in saliva from all of 10 patients with rabies who had this test performed before death in the USA between 1980 and 1996 [20]. However, all of these investigations will only be performed when a rabies diagnosis is seriously considered and the appropriate specimens are sent to the laboratory. A negative test result, except when performed on brain tissues of a symptomatic patient, does not exclude a diagnosis of rabies and additional specimens may need to be evaluated at later time points.
Rabies Due to Non-Rabies Virus Lyssaviruses
In addition to RABV, which is Lyssavirus genotype 1, five of the six other Lyssavirus genotypes have been associated with cases of human rabies, including Mokola virus (genotype 3) [23], Duvenhage virus (genotype 4) [24–26], European bat lyssavirus 1 (genotype 5) [27–30]., European bat lyssavirus 2 (genotype 6) [28, 31–33], and Australian bat lyssavirus (genotype 7) [34–36]. In addition, one human case was reported due to Irkut virus infection (genotype designation is pending) [37]. These viruses are commonly called rabies-like or rabies-related viruses.
Prevention of Rabies
Worldwide, endemic dog rabies in Asia and Africa is responsible for about 99 % of human rabies cases. In Latin America, dog rabies has been eliminated or greatly reduced in most locations due to mass rabies vaccination of dogs so that very few human cases are now due to endemic dog rabies. In Thailand, a very different approach has also been shown to be very effective. Post-exposure rabies prophylaxis of humans with rabies exposures (e.g., dog bites) has greatly the number of human cases to about less than 10 cases per year, despite the continued prevalence of endemic dog rabies in the country.
Rabies post-exposure prophylaxis (PEP) includes wound cleansing, passive immunization with rabies immune globulin, and active immunization with doses of rabies vaccine. A decision to initiate rabies PEP depends on the details of the exposure and a knowledge of the local epidemiological situation. Local public health officials can be very helpful in evaluating the risk and need for prophylactic therapy.
Therapy of Human Rabies
Human rabies almost always has a fatal outcome. Most survivors to date have had severe neurological sequelae and have received one or more doses of rabies vaccine prior to the onset of clinical rabies (Table 1). A group of physicians and basic scientists with expertise in rabies considered the therapeutic options and published a viewpoint article in 2003 [38]. The following year, a young patient recovered from rabies without receiving any post-exposure rabies prophylaxis [39]. She had neutralizing anti-rabies virus antibodies at the time of presentation to hospital. She recovered with mild neurological deficits [40], but it is not at all clear exactly why she had a fairly good outcome [41]. Her therapy included therapeutic coma (midazolam and supplemental phenobarbital), ketamine, ribavirin, and amantadine. Also this therapy, which has been dubbed the Milwaukee protocol, has been relentlessly promoted, and there have been numerous failures and no documented successes despite numerous repetitions of the basic approach with some variations [42•]. There have been many modifications of the protocol, but the scientific foundation of the protocol is very weak, and the approach should be abandoned because of a lack of efficacy and risks associated with the approach [43••]. Instead, novel therapeutic approaches need to be developed. These may come from an improved understanding of basic mechanisms involved in rabies pathogenesis.
Conclusions
Rabies continues to be an important disease, particularly in resource poor countries in Asia and Africa due to presence of endemic dog rabies. Important differences in the clinical features have been noted in human rabies acquired from dogs and bats. Rabies can be very effectively prevented after recognized exposures. Despite aggressive approaches to the therapy of rabies, the disease remains virtually always fatal. The Milwaukee protocol has been shown to be ineffective, and novel approaches need to be taken as we gain an improved understanding of basic mechanisms important that are in rabies pathogenesis.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9:e0003709.
Monroe BP, Yager P, Blanton J, Birhane MG, Wadhwa A, Orciari L, et al. Rabies surveillance in the United States during 2014. J Am Vet Med Assoc. 2016;248:777–88.
Fu ZF, Jackson AC. Neuronal dysfunction and death in rabies virus infection. J Neurovirol. 2005;11:101–6.
Scott CA, Rossiter JP, Andrew RD, Jackson AC. Structural abnormalities in neurons are sufficient to explain the clinical disease and fatal outcome in experimental rabies in yellow fluorescent protein-expressing transgenic mice. J Virol. 2008;82:513–21.
Jackson AC, Kammouni W, Zherebitskaya E, Fernyhough P. Role of oxidative stress in rabies virus infection of adult mouse dorsal root ganglion neurons. J Virol.2010;84:4697--705.
Alandijany T, Kammouni W, Roy Chowdhury SK, Fernyhough P, Jackson AC. Mitochondrial dysfunction in rabies virus infection of neurons. J Neurovirol. 2013;19:537–49.
Kammouni W, Wood H, Saleh A, Appolinario CM, Fernyhough P, Jackson AC. Rabies virus phosphoprotein interacts with mitochondrial complex I and induces mitochondrial dysfunction and oxidative stress. J Neurovirol. 2015;21:370–82.
Warrell DA. The clinical picture of rabies in man. Trans R Soc Trop Med Hyg. 1976;70:188–95.
Warrell DA, Davidson NM, Pope HM, Bailie WE, Lawrie JH, Ormerod LD, et al. Pathophysiologic studies in human rabies. Am J Med. 1976;60:180–90.
Tirawatnpong S, Hemachudha T, Manutsathit S, Shuangshoti S, Phanthumchinda K, Phanuphak P. Regional distribution of rabies viral antigen in central nervous system of human encephalitic and paralytic rabies. J Neurol Sci. 1989;92:91–9.
Udow SJ, Marrie RA, Jackson AC. Clinical features of dog- and bat-acquired rabies in humans. Clin Infect Dis. 2013;57:689–96. This article highlights important differences in the clinical presentation of human rabies acquired from dogs and bats.
Feasby TE, Gilbert JJ, Brown WF, Bolton CF, Hahn AF, Koopman WF, et al. An acute axonal form of Guillain-Barre polyneuropathy. Brain. 1986;109:1115–26.
Griffin JW, Li CY, Ho TW, Tian M, Gao CY, Xue P, et al. Pathology of the motor-sensory axonal Guillain-Barre syndrome. Ann Neurol. 1996;39:17–28.
Sheikh KA, Ramos-Alvarez M, Jackson AC, Li CY, Asbury AK, Griffin JW. Overlap of pathology in paralytic rabies and axonal Guillain-Barré syndrome. Ann Neurol. 2005;57:768–72.
Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain-Barre syndrome. Ann Neurol. 1990;27(Suppl):S21–4.
Laothamatas J, Hemachudha T, Mitrabhakdi E, Wannakrairot P, Tulayadaechanont S. MR imaging in human rabies. A J N R Am J Neuroradiol. 2003;24:1102–9.
Anderson LJ, Nicholson KG, Tauxe RV, Winkler WG. Human rabies in the United States, 1960 to 1979: epidemiology, diagnosis, and prevention. Ann Intern Med. 1984;100:728–35.
Bryceson ADM, Greenwood BM, Warrell DA, Davidson NM, Pope HM, Lawrie JH, et al. Demonstration during life of rabies antigen in humans. J Inf Dis. 1975;131:71–4.
Warrell MJ, Looareesuwan S, Manatsathit S, White NJ, Phuapradit P, Vejjajiva A, et al. Rapid diagnosis of rabies and post-vaccinal encephalitides. Clin Exp Immunol. 1988;71:229–34.
Noah DL, Drenzek CL, Smith JS, Krebs JW, Orciari L, Shaddock J, et al. Epidemiology of human rabies in the United States, 1980 to 1996. Ann Intern Med. 1998;128:922–30.
Mathuranayagam D, Rao PV. Antemortem diagnosis of human rabies by corneal impression smears using immunofluorescent technique. Indian J Med Res. 1984;79:463–7.
Koch FJ, Sagartz JW, Davidson DE, Lawhaswasdi K. Diagnosis of human rabies by the cornea test. Am J Clin Pathol. 1975;63:509–15.
Familusi JB, Osunkoya BO, Moore DL, Kemp GE, Fabiyi A. A fatal human infection with Mokola virus. Am J Trop Med Hyg. 1972;21:959–63.
Meredith CD, Rossouw AP, Koch HP. An unusual case of human rabies thought to be of chiropteran origin. S Afr Med J. 1971;45:767–9.
Paweska JT, Blumberg LH, Liebenberg C, Hewlett RH, Grobbelaar AA, Leman PA, et al. Fatal human infection with rabies-related Duvenhage virus. South Africa Emerg Infect Dis. 2006;12:1965–7.
van Thiel PP, de Bie RM, Eftimov F, Tepaske R, Zaaijer HL, van Doornum GJ, et al. Fatal human rabies due to Duvenhage virus from a bat in Kenya: failure of treatment with coma-induction, ketamine, and antiviral drugs. PLoS Negl Trop Dis. 2009;3:e428.
Selimov MA, Tatarov AG, Botvinkin AD, Klueva EV, Kulikova LG, Khismatullina NA. Rabies-related Yuli virus; Identification with a panel of monoclonal antibodies. Acta Virol. 1989;33:542–6.
Bourhy H, Kissi B, Lafon M, Sacramento D, Tordo N. Antigenic and molecular characterization of bat rabies virus in Europe. J Clin Microbiol. 1992;30:2419–26.
Anonymous. Bat rabies in the Union of Soviet Socialist Republics. Rabies Bull Europe. 1986;10:12–4.
Botvinkin AD, Selnikova OP, Antonova LA, Moiseeva AB, Nesterenko EY, Gromashevsky LV. Human rabies case caused from a bat bite in Ukraine. Rabies Bull Europe. 2005;29:5–7.
Roine RO, Hillbom M, Valle M, Haltia M, Ketonen L, Neuvonen E, et al. Fatal encephalitis caused by a bat-borne rabies-related virus: clinical findings. Brain. 1988;111:1505–16.
Nathwani D, McIntyre PG, White K, Shearer AJ, Reynolds N, Walker D, et al. Fatal human rabies caused by European bat lyssavirus type 2a infection in Scotland. Clin Infect Dis. 2003;37:598–601.
Fooks AR, McElhinney LM, Pounder DJ, Finnegan CJ, Mansfield K, Johnson N, et al. Case report: isolation of a European bat lyssavirus type 2a from a fatal human case of rabies encephalitis. J Med Virol. 2003;71:281–9.
Samaratunga H, Searle JW, Hudson N. Non-rabies lyssavirus human encephalitis from fruit bats: Australian bat lyssavirus (pteropid lyssavirus) infection. Neuropathol Appl Neurobiol. 1998;24:331–5.
Hanna JN, Carney IK, Smith GA, Tannenberg AEG, Deverill JE, Botha JA, et al. Australian bat lyssavius infection: a second human case, with a long incubation period. Med J Aust. 2000;172:597–9.
Francis JR, Nourse C, Vaska VL, Calvert S, Northill JA, McCall B, et al. Australian bat lyssavirus in a child: the first reported case. Pediatrics. 2014;133:e1063–7.
Leonova GN, Belikov SI, Kondratov IG, Krylova NV, Pavlenko EV, Romanova EV, et al. A fatal case of bat lyssavirus infection in Primorye Territory of the Russian Far East. Rabies Bull Europe. 2009;33:5–8.
Jackson AC, Warrell MJ, Rupprecht CE, Ertl HCJ, Dietzschold B, O'Reilly M, et al. Management of rabies in humans. Clin Infect Dis. 2003;36:60–3.
Willoughby Jr RE, Tieves KS, Hoffman GM, Ghanayem NS, Amlie-Lefond CM, Schwabe MJ, et al. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005;352:2508–14.
Hu WT, Willoughby Jr RE, Dhonau H, Mack KJ. Long-term follow-up after treatment of rabies by induction of coma (letter). N Engl J Med. 2007;357:945–6.
Jackson AC. Recovery from rabies (editorial). N Engl J Med. 2005;352:2549–50.
Jackson AC. Current and future approaches to the therapy of human rabies. Antiviral Res. 2013;99:61–7. This review article summarizes current knowledge relevant to treating human patients with rabies and provides important evidence about the failure of the Milwaukee protocol.
Zeiler FA, Jackson AC. Critical appraisal of the Milwaukee protocol for rabies: this failed approach should be abandoned. Can J Neurol Sci. 2016;43:44–51. This article is a detailed evaluation of the Milwaukee protocol that highlights its poor scientific rationale, flaws, and lack of therapeutic efficacy.
Hattwick MAW, Weis TT, Stechschulte CJ, Baer GM, Gregg MB. Recovery from rabies: a case report. Ann Intern Med. 1972;76:931–42.
Porras C, Barboza JJ, Fuenzalida E, Adaros HL, Oviedo AM, Furst J. Recovery from rabies in man. Ann Intern Med. 1976;85:44–8.
Tillotson JR, Axelrod D, Lyman DO. Rabies in a laboratory worker - New York. MMWR.1977; 26:183-4.
Tillotson JR, Axelrod D, Lyman DO. Follow-up on rabies - New York. MMWR.1977; 26:249-50.
Alvarez L, Fajardo R, Lopez E, Pedroza R, Hemachudha T, Kamolvarin N, et al. Partial recovery from rabies in a nine-year-old boy. Pediatr Infect Dis J. 1994;13:1154–5.
Madhusudana SN, Nagaraj D, Uday M, Ratnavalli E, Kumar MV. Partial recovery from rabies in a six-year-old girl (letter). Int J Infect Dis. 2002;6:85–6.
Ministerio da Saude in Brazil. Rabies, human survival, bat - Brazil: (Pernambuco). ProMED-mail 2008; 20081114.3599. Accessed 10 Feb 2009.
Karahocagil MK, Akdeniz H, Aylan O, Sünnetçioglu M, Ün H, Yapici K, et al. Complete recovery from clinical rabies: case report. Turkiye Klinikleri J Med Sci. 2013;33:547–52.
Netravathi M, Udani V, Mani RS, Gadad V, Ashwini MA, Bhat M, et al. Unique clinical and imaging findings in a first ever documented PCR positive rabies survival patient: a case report. J Clin Virol. 2015;70:83–8.
de Souza A, Madhusudana SN. Survival from rabies encephalitis. J Neurol Sci. 2014;339:8–14.
Weyer J, Msimang-Dermaux V, Paweska JT, le Roux K, Govender P, Coertse J, et al. A case of human survival of rabies, South Africa. South Afr J Infect Dis. 2016;31:66–8.
Galvez S, Basque M, Contreras L, Merino C, Ahumada R, Jamett J, et al.: Survivor of rabies encephalitis in Chile. Platform presentation at the XXIVth International Meeting on Research Advances and Rabies Control in the Americas in Toronto, Ontario, Canada on October 27, 2013. Research Advances and Rabies Control in the Americas 2013.
Thakur BS. 2nd rabies survivor in country at P’kula hospital. Hindustan times. Panchkula: HT Media Limited; 2014.
Kumar KV, Ahmad FM, Dutta V. Pituitary cachexia after rabies encephalitis (letter). Neurol India. 2015;63:255–6.
Karande S, Muranjan M, Mani RS, Anand AM, Amoghimath R, Sankhe S, et al. Atypical rabies encephalitis in a six-year-old boy: clinical, radiological and laboratory findings. Int J Infect Dis. 2015;36:1–3.
Manoj S, Mukherjee A, Johri S, Kumar KV. Recovery from rabies, a universally fatal disease. Mil Med Res. 2016;3:21–0089.
Holzmann-Pazgal G, Wanger A, Degaffe G, Rose C, Heresi G, Amaya R, et al. Presumptive abortive human rabies - Texas, 2009. MMWR.2010;59:185-90.
Wiedeman J, Plant J, Glaser C, Messenger S, Wadford D, Sheriff H, et al. Recovery of a patient from clinical rabies - California, 2011. MMWR.2012;61:61-5.
Rawat AK, Rao SK. Survival of a rabies patient (letter). Indian Pediatr. 2011;48:574.
Jackson AC, Fu ZF. Pathogenesis. In: Jackson AC, editor. Rabies: Scientific basis of the disease and its management. 3rd ed. Oxford: Elsevier Academic Press; 2013. p. 299–349.
Jackson AC: Therapy of human rabies, in Rabies: scientific basis of the disease and its management, Third Edition, edited by AC Jackson. Elsevier Academic Press. Oxford: UK; 2013. p. 573–87.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
Dr Jackson declares that he has no conflicts of interests.
Human and Animal Rights and Informed Consent
This article does not contain any reports of new studies with human or animal subjects performed by the author.
Additional information
This article is part of the Topical Collection on Central Nervous System Infections
Rights and permissions
About this article

Cite this article
Jackson, A.C. Human Rabies: a 2016 Update. Curr Infect Dis Rep 18, 38 (2016). https://doi.org/10.1007/s11908-016-0540-y
Published:
DOI: https://doi.org/10.1007/s11908-016-0540-y