
Abstract
Purpose of Review
In this manuscript, the literature published in the past 5 years about BPS/IC biomarkers was reviewed. Topics include BPS/IC biomarkers, the classical BPS/IC diagnostic, clinical outcomes as a new concept of BPS/IC phenotyping biomarkers, BPS/IC urinary biomarkers, BPS/IC bladder tissue biomarkers and BPS/IC biomarkers outside the bladder.
Recent Findings
The importance of patients’ phenotyping and sub-grouping emerged as a way of finding new BPS/IC biomarkers and treatment. Also, the use of non-invasive methodologies and of artificial intelligence approaches has been gaining momentum in BPS/IC biomarkers studies.
Summary
Biomarker research points to the need of following an approach based on a systemic theory instead of a bladder-centred theory. Also, the importance of sample size and the choice of controls to validate BPS/IC biomarkers have been elevated.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Despite significant efforts made in recent years to better understand bladder pain syndrome/interstitial cystitis (BPS/IC), there is still a long road ahead of us. The myriad of symptoms and signs presented by different patients has had a great impact on the management of BPS/IC, starting with the definition of the pathology itself. Different workgroups have presented different definitions, including those stating that BPS and IC are in fact two different pathologies [1]. Nevertheless, in the great majority, it is commonly accepted that the diagnosis is of exclusion and patients should refer pain, pressure or discomfort in the abdomen, and at least one lower urinary symptom [2]. In some cases, further analysis can be performed to characterize the patients, such as cystoscopy and bladder biopsies [2].
Until recently, it was commonly accepted that BPS/IC was a bladder pathology that was associated with the impairment of the urothelial barrier, which allowed urine molecules to diffuse into the bladder wall, triggering an inflammatory cascade that ultimately lead to activation of suburothelial nociceptive fibres, generating pain and bladder symptoms [2]. Hence, the available treatments were directed to overcome pain (e.g. oral analgesics or of local application, anti-inflammatories, anticonvulsants or tricyclics/antidepressants), to overcome lower urinary tract symptoms (e.g. anticholinergics/antimuscarinics), to treat inflammation (e.g. anti-inflammatories and antihistamines) or to reverse urothelial leakage (e.g. pentosan polysulphate sodium) [3,4,5]. However, these treatments have proved to have low efficacy. They are palliative and not curative, particularly because of the unknown cause of the symptoms.
In recent years, the bladder-centred concept has been broadened with the hypothesis that BPS/IC is accompanied by or even results from a systemic imbalance [6]. The black box representing BPS/IC is no longer centred in the bladder but encompasses the whole body. This change of concept was based on different observations, including existence of comorbidities [7], changes in the sympathetic nervous system activity [8] and pain mapping outside the pelvis [9•]. The BPS/IC-related systemic hypothesis broadens the spectrum of signs and symptoms reported by patients that must be clued-in by physicians. Phenotyping and clustering of patients, based on the presence of specific biomarkers, are quickly becoming the road that may lead to a phenotype-specific diagnostic procedure and a more effective treatment aiming to block the causes of pathology rather than simply managing complaints. Here, we will review knowledge of BPS/IC biomarkers, focusing on the past 5 years, and address where the use of these observations can take us.
BPS/IC Biomarkers
A biomarker is a characteristic that serves as an indicator of normal biological activity, of a pathological condition or a response to a procedure/treatment [10]. This characteristic could be something at a subcellular, cellular, tissue, system or organ level. Biomarkers can be used in the diagnostic and monitoring of the disease and the effects of treatment. In addition, biomarkers are useful to predict the outcome of treatments, to help perform a prognostic, to access the safety of a treatment and/or to measure the susceptibility of developing certain phenotype [10].
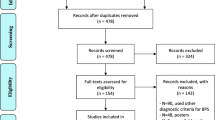
Identifying the precise pathophysiological mechanisms of disease facilitates the identification of putative biomarkers. In BPS/IC, these mechanisms are far from being known. This may be one of the reasons why the BPS/IC biomarkers field per se is still under development. Performing a PUBMED search using the keywords “Bladder pain syndrome” and “biomarker,” restricted to the last 5 years, returned 50 papers, 17 of which were reviews, 2 opinion papers and 2 did not focus on biomarkers. However, the shifting from a bladder-centric theory to a paradigm that accepts BPS/IC is a systemic condition (still considering bladder complaints) and has opened new windows of opportunities to find new BPS/IC biomarkers, to be used to improve patient’s phenotyping.
The Classical BPS/IC Diagnostic
While 2007 ESSIC criteria are used to establish a consensus to diagnose BPS/IC, one must not forget that these criteria still include a large spectrum of possible clinical presentations. Exclusion of organic disorders related to the bladder, urethra and the remaining pelvic structures is paramount [11]. In this context, the basic assessment of the patient should include a thorough collection of the clinical history, with a bladder diary and a careful physical examination. The urinalysis and culture, as well as an ultrasound of the bladder, are also usually performed. In cases of complicated BPS/IC, where the pain is associated with haematuria, incontinence or gynaecological symptoms, further investigation with bladder cystoscopy, endoscopy, urine cytology, urodynamics and further imaging should be made [12].
Although the correct timing to phenotype the patient is different when comparing guidelines, this classification of the patient as BPS, without Hunner lesions, or IC, with Hunner lesions, is important [13]. These are the only presently known phenotypes and the available treatments are chosen based on these two phenotypes. Only after the exclusion of potential confounders, the diagnostic could be confirmed.
Clinical Outcomes as a New Concept of BPS/IC Phenotyping Biomarkers
Clinical outcomes may be used as phenotyping biomarkers for some sub-groups of BPS/IC patients. Walker and co-workers have demonstrated that low bladder capacity (inferior to 400 mL) was positively correlated with age, higher urinary frequency and higher scores on Interstitial Cystitis Symptom Index, Interstitial Cystitis Problem Index and Pelvic Pain and Urgency/Frequency Patient Symptom Scale [14]. This was quite promising as these findings were not present in confoundable diseases such as depression and other systemic pain problems. Furthermore, Schachar and co-workers showed that BPS/IC patients with low bladder capacity were older and exhibited higher levels of both acute and chronic bladder inflammation [15]. In another study, Mazeaud verified that BPS/IC patients with low bladder capacity had higher frequency and nocturia, earlier onset of painful urge during bladder filling and lower compliance. These patients also present more often the IC phenotype [16].
BPS/IC Urinary Biomarkers
A good biomarker is associated with non-invasive techniques, without any significant bothers to the patients. Hence, because urine can be collected in significant amounts and without bothersome procedures, it has been the source of choice to identify putative biomarkers. However, one of the limitations in the use of urine is the number of samples, normally restricted to the number of patients that researchers have access to. This low number of samples may not be representative of the disease. To overcome this, Chancellor and co-workers have recently presented a new method to overcome such problem [17••, 18]. They have performed a national crowdsourcing study in cooperation with the Interstitial Cystitis Association to recruit patients [17••, 18]. In addition to listing a large list of phenotyping biomarkers, such as symptom severity and urinary frequency questionnaires, urine samples were collected at home, stabilized and sent to the research institution [17••, 18]. This increased the number of patients participating in the study, and therefore, the number of the sample became more representative of the disease. This study shows that it was possible to use urine samples to assess phenotyping biomarkers, complementing clinical outcomes. Moreover, investigators were able to standardize the process [17••], which will positively impact future studies. Chancellor et al. used a machine learning algorithm, in which urinary cytokines GRO/CXCL-1, interleukin 6 and interleukin 8 were used as biomarkers to phenotype previously diagnosed groups of patients with BPS/IC (who presented Hunner lesions), patients with BPS/IC but without Hunner lesions and controls. The accuracy in phenotype outcome was 95.1% accuracy [17••]. To further refine patients’ phenotyping, Chancellor and co-workers have validated the results to predict Bladder Permeability Defect Risk Score and had an 88.7% accuracy in their phenotype outcome [17••].
Another putative urinary biomarker to phenotype BPS/IC patients is the macrophage migration inhibitory factor (MIF). Vera and co-workers showed that this molecule is increased in the urine of female BPS/IC patients with Hunner lesion when compared to BPS/IC patients without Hunner lesion or healthy subjects [19]. However, the urinary values of MIF of female BPS/IC patients with Hunner lesion were similar to values observed in male patients with bacterial and radiation cystitis [19]. As a chronic pain condition, BPS/IC may show gender-specific pathways [20] but no values from BPS/IC male patients were reported. Therefore, it would have been important to demonstrate differences between urinary MIF concentration between affected men and women to validate urinary MIF as a biomarker.
One of the most studied molecules as a BPS/IC biomarker is nerve growth factor (NGF). Recently, Tonyali and co-workers have demonstrated that urinary NGF normalized to creatinine levels is significantly correlated with the O’Leary-Sant IC Symptom and Problem Index scores in BPS/IC patients [21]. However, Regauer and co-workers did not observe differences in urinary NGF levels of BPS/IC, with and without Hunner lesions, from patients with overactive bladder syndrome (OAB) and healthy subjects [22]. This discrepancy of outcomes may be due to differences in the BPS/IC population, which would indicate that NGF may be a phenotyping or a predictive biomarker only for a subset of patients. The same may be true for other molecules. In fact, in a recent study of the Multidisciplinary Approach to the Study of Chronic Pelvic Pain (MAPP) Research Network using 40 independent urinary samples from BPS/IC patients, investigators showed that it was not possible to define a single urinary profile accommodating all samples [23]. Hence, it is expectable that different BPS/IC patient’s clusters likely present a specific urinary profile. In fact, in the MAPP Research Network study, two sub-groups of BPS/IC patients based on urinary etiocholan-3α-ol-17-one sulphate levels were identified [23]. Likewise, Jiang and co-workers have analysed the urine of 127 BPS/IC patients to study the levels of different cytokines [24]. Although the authors have clustered the patients according to the ESSIC definition, it was possible to infer the existence of sub-groups inside the clusters.
The chemical composition of the urine may also be used as a phenotyping biomarker. Capua-Sacoto and co-workers showed that exposure of neoplastic cell lines to different samples of urine from BPS/IC patients induced apoptosis in a manner dependent on the severity of symptoms reported by patients [25]. However, the investigators did not differentiate the effects of urine samples collected from patients with Hunner lesions [25]. Importantly, the apoptosis-inducing properties of urine from patients with chronic pelvic pain of gynaecological origin did not correlate with symptom severity [25], suggesting that the urine apoptotic ability could be used to differentiate BPS/IC from chronic pelvic pain of gynaecological origin.
Urinary cations have been proposed as BPS/IC biomarkers. Argade and co-workers showed that in a population of 51 male patients with BPS/I the urinary higher levels of cationic metabolites with higher cytotoxicity were significantly higher compared to controls [26]. However, when these patients were treated with heparinoid therapy, despite symptom improvement, cationic metabolites remain elevated [26]. This may indicate that cationic metabolites may be used in the future as a diagnostic biomarker but not as a predictive biomarker. One should note that predictive biomarkers must correlate with clinical outcomes, defined to assess symptomatic improvement. When such a correlation does not exist or only exists partially, it mines the confidence in treatment efficacy. Jiang and co-workers presented urinary NGF, platelet-derived growth factor AB, matrix metallopeptidase 13 (MMP-13), vascular endothelial growth factor (VEGF) and tumour necrosis factor-alpha (TNF-α) levels as predictive biomarkers for repeated intravesical injections of platelet-rich plasma treatment of BPS/IC patients, as these molecule levels vary with treatment [27]. However, when correlated with the different clinical outcomes, there was not a pan correlation of all markers with all clinical outcomes. In fact, in the case of VEGF and MMP-13, their urinary levels changed even when no changes occurred in clinical outcomes. These results prompted different questions such as whether these molecules are in fact predictive biomarkers, whether the clinical outcomes were appropriated chosen for this specific study or whether platelet-rich plasma treatment was ineffective.
Urine has also been shown to be a viable source to evaluate DNA methylation as a BPS/IC diagnostic biomarker. Bradley and co-workers have analysed the urine of 19 BPS/IC patients and 17 controls to assess quantitative DNA methylation in the pelleted urine sediment. Samples were age and ethnic group matched and had adequate DNA for methylation analysis [28]. The authors observed that genes within or downstream of the mitogen-activated protein kinase (MAPK) pathway exhibit altered methylation in BPS/IC [28], suggesting that analysis of levels of DNA methylation of key genes, including the pro-survival MAPPK pathway, in cells found in the sediment may serve as a urinary biomarker.
BPS/IC Bladder Tissue Biomarkers
Bladder tissue may also be used to assess BPS/IC biomarkers. Regauer and co-workers have analysed innervation in bladder biopsies from small groups of BPS/IC patients with Hunner lesions, BPS/IC patients without Hunner lesion, patients with OAB and healthy subjects [22]. They have performed immunohistochemistry using the pan-neuronal marker protein gene product 9.5 (PGP9.5) and determined that BPS/IC patients, with and without Hunner lesion, but not OAB or healthy controls, presented nerve sprouting in the bladder subepithelial layer [22]. Curiously, this sprouting was associated with B lymphocyte marker cluster of differentiation 20 (CD20) overexpression [22]. Since OAB is one of the BPS/IC confounding diseases, markers related to this nerve sprouting and lymphocytic infiltration may be useful in the future as diagnostic biomarkers.
More recently, artificial intelligence/bioinformatics approaches have been used to identify BPS/IC biomarkers. Saha and co-workers have performed a gene expression analysis using bladder wall samples of BPS/IC patients with Hunner lesion and compared with non-malignant bladder wall samples of the patient that underwent radical cystectomy or transurethral resection of bladder tumours [29]. The authors performed an integrated analysis of Gene Expression Omnibus datasets, followed by the construction of a protein-protein interaction network using cytoHubba v0.1, and determined a total of 53 common differentially expressed genes in the BPS/IC samples [29]. This analysis showed that haematopoietic cell lineage, immune system and T cell receptor (TCR) signalling in naïve cluster of differentiation 4+ (CD 4+) T cell signalling pathways were prominently involved with 51 upregulated genes. The two downregulated genes were involved in linoleic acid metabolism and synthesis of epoxy and dihydroxy eicosatrienoic acid signalling pathways. Although complex and requiring validation by classical molecular biology techniques, this type of approach seems to allow the identification of putative biomarkers and the identification of altered signalling pathways which could point to new key targets for the treatment of BPS/IC. Arai and co-workers also analysed gene expression in bladder tissue samples. They compared the levels of miRNA in samples from control, BPS/IC with and without Hunner lesions and samples from bladder cancer patients; identifying three transcription factors, E2F-1, E2F-2 and TUB, the expression of which was altered only in BPS/IC patients, without specifying which had Hunner lesions or not [30••]. It is, however, important to stress the origin of control samples. A recent study showed that the bladder tissue from cadaveric donors does not routinely yield high-quality RNA needed for downstream gene expression applications and, therefore, cannot be used as a reliable control samples [31]. The confirmation of these results is important, especially when an increase in expression of genes is expected in the tissue of the pathological group. Although the origin of control samples is not clear in Arai and co-workers’ work, these authors have confirmed their gene expression analysis through the immunohistochemistry technique [30••]. Other authors have used bladder samples obtained from other bladder pathologies as control tissue to perform gene analysis. Choi and co-workers used as controls bladder tissue from patients submitted to sling operation for stress urinary incontinence to study WNT pathway involvement in BPS/IC but proper validation was not performed [32], although observations were in agreement with data obtained with animal models of disease [33]. Results seem to indicate that decreased expression of WNT11 may be used to differentiate BPS/IC patients with and without Hunner lesion [32]. In another study, Cho and co-workers have evaluated changes in uroplakin expression in the urothelium of BPS/IC patients with Hunner lesion, using as control bladder tissue from bladder cancer patients submitted to radical cystectomy [34]. Despite observations showing that uroplakin-III protein was significantly upregulated in the urothelium of BPS/IC with Hunner lesion, the results are not fully conclusive as proper validation of control tissue was not performed. In fact, the lack of validations of control tissues might be the major drawback of bladder tissue analysis. While the ideal control tissue would be samples obtained from healthy individuals, without any bladder complaints, this would never be ethically acceptable.
Nevertheless, tissue biomarkers are still valuable tools to understand the pathophysiological mechanisms involved in symptom development in the different subtypes of BPS/IC patients. Furuta and co-workers have demonstrated that the bladder wall of BPS/IC patients (with and without Hunner lesion) had higher expression of TNF-α, VEGF, cluster of differentiation 31 (CD31), transforming growth factor-beta (TGF-β) and snail family transcriptional repressor 2 (SLUG) [35], clear indicators of tissue inflammation and angiogenesis. In fact, CD31 expression was shown to be correlated with O’Leary-Sant symptom indexes, O’Leary-Sant problem indexes and visual analogue scale pain scores [35]. Curiously, only BPS/IC patients with Hunner lesions showed increased expression of mast cell tryptase and collagen and decrease expression of E-cadherin [35]. The latter is involved in cell-to-cell adhesion, raising the hypothesis that impaired E-cadherin expression might be involved in Hunner lesion appearance. Moreover, mast cell tryptase and collagen are both involved in the fibrotic mechanism, suggesting their increase could represent a tissue healing response to the lesions.
BPS/IC Biomarkers Outside the Bladder
In order to identify other putative BPS/IC biomarkers, researchers have looked for sources other than the bladder. Plasmatic proteins are thought to be good candidates for BPS/IC diagnostic or, at least, useful to exclude confounding diseases. Accordingly, Ma and co-workers showed that plasmatic TNF-α and macrophage inflammatory protein 1 beta (MIP-1β) levels were significantly higher in OAB patients compared with BPS/IC patients, prompting these two molecules as putative biomarkers for disease exclusion [36].
Other studies have focused on the microbiome, as recent studies demonstrated that changes in the faecal microbiome are linked to pelvic pain in BPS/IC [37]. Braundmeier-Fleming and co-workers used faecal samples of BPS/IC patients and healthy controls and performed machine learning by extended random forest to identify operational taxonomic units by 16S rDNA sequence analysis [38]. This analysis was complemented by analysis of the clinical outcome obtained with a questionnaire assessing symptom severity and by metabolomic pathway analysis [38]. They observed that the severity of symptoms was linked to a reduced presence of some bacterial species in stool from BPS/IC patients, supporting that analysis of the faecal microbiome could be used as a biomarker [38]. Further studies are needed but, considering that stool collection and analysis are non-invasive routine procedures, we anticipate in the near future that, like urine, the stool will become a relevant source of putative biomarkers.
Autonomic responses and peripheral catecholamines have also been investigated as biomarkers as sympathetic hyperactivity is common among BPS/IC patients and though to be a contributing pathophysiological factor [39]. Kim and co-workers have evaluated the correlation between symptom severity in BPS/IC patients and autonomic nervous system activity. They found exaggerated autonomic responses to bladder hydrodistention in BPS/IC patients, which correlated with the severity of symptoms [40]. This study reinforced the idea that catecholamines may be useful as a follow-up or predictive biomarkers.
Conclusions: Where Can We Go from Here?
Grouping of BPS/IC patients according to their phenotype is now seen as the best practice to choose the most adequate therapeutic approach (Fig. 1). To produce such phenotyping, specific BPS/IC biomarkers need to be identified and properly validated. In the past 5 years, an effort has been made towards this goal. However, there is still a long path to walk. The design of standard procedures of analyses, with appropriate controls (negative or positive, as patients with confounding diseases), is essential for the success of such a complex process. To determine which clinical outcomes to analyse, which samples to use (urine, saliva, blood/plasma, among others), which complementary analysis should be performed (functional magnetic resonance imaging, for example) will help to find the best diagnostic, predictive or excluding biomarkers. Only then it will be possible to study the pathophysiological mechanisms of the diseases that may lead us, in the future, to specific effective treatments.

General diagram depicting how the use of biomarkers could contribute to better management of BPS/IC patients. While urine has been widely studied as a source of BPS/IC biomarkers, other sources could be considered. Preference should be given to non-invasive techniques to avoid bothering patients. Data should be properly validated so it can be used to design effective tailor-made therapeutic approaches for improved BPS/IC treatment
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Fall M, Nordling J, Cervigni M, Dinis Oliveira P, Fariello J, Hanno P, et al. Hunner lesion disease differs in diagnosis, treatment and outcome from bladder pain syndrome: an ESSIC working group report. Scand J Urol. 2020;54(2):91–8.
Malde S, Palmisani S, Al-Kaisy A, Sahai A. Guideline of guidelines: bladder pain syndrome. BJU Int. 2018 [cited 2020 Feb 18];122(5):729–43. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29777618.
Jhang J-F, Hsu Y-H, Jiang Y-H, Ho H-C, Kuo H-C. Clinical relevance of bladder histopathological findings and their impact on treatment outcomes among patients with interstitial cystitis/bladder pain syndrome: an investigation of the European Society for the Study of Interstitial Cystitis Histopatholog. J Urol. 2020. https://doi.org/10.1097/JU.0000000000001334.
Taneja R. Current status of oral pentosan polysulphate in bladder pain syndrome/interstitial cystitis. Int Urogynecol J. 2020. https://doi.org/10.1007/s00192-020-04517-9.
Garzon S, Laganà AS, Casarin J, Raffaelli R, Cromi A, Sturla D, et al. An update on treatment options for interstitial cystitis. Prz Menopauzalny. 2020;19(1):35–43.
Colemeadow J, Sahai A, Malde S. Clinical management of bladder pain syndrome/interstitial cystitis: a review on current recommendations and emerging treatment options. Res Rep Urol. 2020;12:331–43.
Marcu I, Campian EC, Tu FF. Interstitial cystitis/bladder pain syndrome. Semin Reprod Med. 2018;36(2):123–35.
Charrua A, Pinto R, Birder LA, Cruz F. Sympathetic nervous system and chronic bladder pain: a new tune for an old song. Transl Androl Urol. 2015;4(5):534–42. https://doi.org/10.3978/j.issn.2223-4683.2015.09.06.
• Tripp DA, Nickel JC, Wong J, Pontari M, Moldwin R, Mayer R, et al. Mapping of pain phenotypes in female patients with bladder pain syndrome/interstitial cystitis and controls. Eur Urol. 2012;62(6):1188–94. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22633363This work reported numerous systemic pain symptoms outside the areas associated with the bladder/pelvic region. It was, possible, the turning point from a bladder centric theory to a systemic centred theory.
Califf RM. Biomarker definitions and their applications. Exp Biol Med (Maywood). 2018;243(3):213–21 Available from: https://pubmed.ncbi.nlm.nih.gov/29405771.
van de Merwe JP, Nordling J, Bouchelouche P, Bouchelouche K, Cervigni M, Daha LK, et al. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: an ESSIC proposal. Eur Urol. 2008;53(1):60–7 Available from: http://www.ncbi.nlm.nih.gov/pubmed/17900797.
Engeler Baranowski AP, Borovicka J, Dinis-Oliveira P, Elneil S, Hughes J, Messelink EJ, van Ophoven A, Reisman Y, Williams AC de CD. Guidelines on chronic pelvic pain. Urology EA of, editor. 2013. p. 132. Available from: http://www.uroweb.org/gls/pdf/25_Chronic_Pelvic_Pain_LR.pdf.
Whitmore KE, Fall M, Sengiku A, Tomoe H, Logadottir Y, Kim YH. Hunner lesion versus non-Hunner lesion interstitial cystitis/bladder pain syndrome. Int J Urol. 2019;26 Suppl 1:26–34.
Walker SJ, Zambon J, Andersson K-E, Langefeld CD, Matthews CA, Badlani G, et al. Bladder capacity is a biomarker for a bladder centric versus systemic manifestation in interstitial cystitis/bladder pain syndrome. J Urol. 2017;198(2):369–75.
Schachar JS, Evans RJ, Parks GE, Zambon J, Badlani G, Walker SJ. Histological evidence supports low anesthetic bladder capacity as a marker of a bladder-centric disease subtype in interstitial cystitis/bladder pain syndrome. Int Urogynecol J. 2019;30(11):1863–70.
Mazeaud C, Rigaud J, Levesque A, Madec F-X, Le Clerc Q-C, Wack M, et al. Stratification of patients with interstitial cystitis/bladder pain syndrome according to the anatomical bladder capacity. Urology. 2019;123:87–92.
•• Chancellor MB, Bartolone SN, Veerecke A, Lamb LE. Crowdsourcing disease biomarker discovery research: The IP4IC study. J Urol. 2018;199(5):1344–50 This work presents crowdsourcing as a way to overcome the problem of low sample number presented by different studies. Also, it presents machine learning algorithm as a tool to study BPS/IC biomarkers.
Lamb LE, Janicki JJ, Bartolone SN, Peters KM, Chancellor MB. Development of an interstitial cystitis risk score for bladder permeability. PLoS One. 2017;12(10):e0185686.
Vera PL, Preston DM, Moldwin RM, Erickson DR, Mowlazadeh B, Ma F, et al. Elevated urine levels of macrophage migration inhibitory factor in inflammatory bladder conditions: a potential biomarker for a subgroup of interstitial cystitis/bladder pain syndrome patients. Urology. 2018;116:55–62.
Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. 2013;111(1):52–8.
Tonyali S, Ates D, Akbiyik F, Kankaya D, Baydar D, Ergen A. Urine nerve growth factor (NGF) level, bladder nerve staining and symptom/problem scores in patients with interstitial cystitis. Adv Clin Exp Med. 2018;27(2):159–63.
Regauer S, Gamper M, Fehr MK, Viereck V. Sensory hyperinnervation distinguishes bladder pain syndrome/interstitial cystitis from overactive bladder syndrome. J Urol. 2017;197(1):159–66.
•• Parker KS, Crowley JR, Stephens-Shields AJ, van Bokhoven A, Lucia MS, Lai HH, et al. Urinary metabolomics identifies a molecular correlate of interstitial cystitis/bladder pain syndrome in a multidisciplinary approach to the study of Chronic Pelvic Pain (MAPP) Research Network Cohort. EBioMedicine. 2016;7:167–74 This work excels the existence of multiple BPS/IC patients phenotype. Although they have focused on etiocholan-3α-ol-17-one sulphate (Etio-S), they lift the veil to other molecules/BPS/IC phenotypes.
Jiang Y-H, Jhang J-F, Hsu Y-H, Ho H-C, Wu Y-H, Kuo H-C. Urine cytokines as biomarkers for diagnosing interstitial cystitis/bladder pain syndrome and mapping its clinical characteristics. Am J Physiol Ren Physiol. 2020;318(6):F1391–9.
Di Capua-Sacoto C, Sanchez-Llopis A, Oconnor JE, Martinez-Romero A, Ruiz-Cerdá JL. Apoptotic effect as biomarker of disease, severity and follow-up in interstitial cystitis. Actas Urol Esp. 2018;42(4):262–6.
Argade S, Berecz Z, Su Y, Parsons CL. Increased toxic urinary cations in males with interstitial cystitis: a possible cause of bladder symptoms. World J Urol. 2016;34(12):1685–91.
Jiang Y-H, Kuo Y-C, Jhang J-F, Lee C-L, Hsu Y-H, Ho H-C, et al. Repeated intravesical injections of platelet-rich plasma improve symptoms and alter urinary functional proteins in patients with refractory interstitial cystitis. Sci Rep. 2020;10(1):15218. https://doi.org/10.1038/s41598-020-72292-0.
Bradley MS, Burke EE, Grenier C, Amundsen CL, Murphy SK, Siddiqui NY. A genome-scale DNA methylation study in women with interstitial cystitis/bladder pain syndrome. Neurourol Urodyn. 2018;37(4):1485–93.
Saha SK, Jeon T-I, Bin JS, Kim SJ, Lim KM, Choi YJ, et al. Bioinformatics approach for identifying novel biomarkers and their signaling pathways involved in interstitial cystitis/bladder pain syndrome with Hunner lesion. J Clin Med. 2020;9(6):1935. https://doi.org/10.3390/jcm9061935.
•• Arai T, Fuse M, Goto Y, Kaga K, Kurozumi A, Yamada Y, et al. Molecular pathogenesis of interstitial cystitis based on microRNA expression signature: miR-320 family-regulated molecular pathways and targets. J Hum Genet. 2018;63(5):543–54 This work approaches the importance of using appropriated controls to validate putative biomarkers. In this case, it demonstrated that bladder tissue from cadaveric donors should not be used (or used with extremely caution) as controls for the validation of RNA-related biomarkers.
Matthews CA, Eschenroeder A, Badlani G, Evans R, Walker SJ. Evaluation of the efficacy of postmortem human bladder tissue as a normal comparator for case-controlled gene expression studies in urology. Neurourol Urodyn. 2017;36(4):1076–80.
Choi D, Han J-Y, Shin JH, Ryu C-M, Yu HY, Kim A, et al. Downregulation of WNT11 is associated with bladder tissue fibrosis in patients with interstitial cystitis/bladder pain syndrome without Hunner lesion. Sci Rep. 2018;8(1):9782.
Song M, Lim J, Yu HY, Park J, Chun J-Y, Jeong J, et al. Mesenchymal stem cell therapy alleviates interstitial cystitis by activating Wnt signaling pathway. Stem Cells Dev. 2015;24(14):1648–57.
Cho KJ, Lee K-S, Choi JB, Koh JS, Kim JC. Changes in uroplakin expression in the urothelium of patients with ulcerative interstitial cystitis/bladder pain syndrome. Investig Clin Urol. 2020;61(3):304–9.
Furuta A, Suzuki Y, Igarashi T, Koike Y, Kimura T, Egawa S, et al. Angiogenesis in bladder tissues is strongly correlated with urinary frequency and bladder pain in patients with interstitial cystitis/bladder pain syndrome. Int J Urol. 2019;26 Suppl 1:35–40.
Ma E, Vetter J, Bliss L, Lai HH, Mysorekar IU, Jain S. A multiplexed analysis approach identifies new association of inflammatory proteins in patients with overactive bladder. Am J Physiol Ren Physiol. 2016;311(1):F28–34.
Nickel JC, Stephens-Shields AJ, Landis JR, Mullins C, van Bokhoven A, Lucia MS, et al. A culture-independent analysis of the microbiota of female interstitial cystitis/bladder pain syndrome participants in the MAPP Research Network. J Clin Med. 2019;8(3):415. https://doi.org/10.3390/jcm8030415.
Braundmeier-Fleming A, Russell NT, Yang W, Nas MY, Yaggie RE, Berry M, et al. Stool-based biomarkers of interstitial cystitis/bladder pain syndrome. Sci Rep. 2016;6:26083.
Charrua A, Pinto R, Taylor A, Canelas A, Ribeiro-da-Silva A, Cruz CD, et al. Can the adrenergic system be implicated in the pathophysiology of bladder pain syndrome/interstitial cystitis? A clinical and experimental study. Neurourol Urodyn. 2015;34(5):489–96. https://doi.org/10.1002/nau.22542.
Kim SW, Son HS, Troya IS, Kim JY, Kim MJ, Fraser MO, et al. Autonomic response during bladder hydrodistention reflects the severity of symptoms in patients with bladder pain syndrome/interstitial cystitis. Neurourol Urodyn. 2017;36(3):677–82.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on BPS/Interstitial Cystitis
Rights and permissions
About this article

Cite this article
Charrua, A., Mendes, P. & Cruz, C. Biomarkers for Bladder Pain Syndrome/Interstitial Cystitis. Curr Bladder Dysfunct Rep 16, 12–18 (2021). https://doi.org/10.1007/s11884-020-00626-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11884-020-00626-9