
Abstract
Purpose
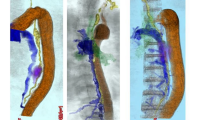
We describe the optimal protocol of magnetic resonance-thoracic ductography (MRTD) and provide examples of thoracic ducts (TD) and various anomalies. The anatomical pathway of the TD was analyzed based on embryological considerations.
Methods
A total of 78 subjects, consisting of noncancer adults and patients with esophageal cancer and lung cancer, were enrolled. The MRTD protocol included a long echo time and was based on emphasizing signals from the liquid fraction and suppressing other signals, based on the principle that lymph flow through the TD appears hyperintense on T2-weighted images. The TD configuration was classified into nine types based on location [right and/or left side(s) of the descending aorta] and outflow [right and/or left venous angle(s)].
Results
MRTD was conducted in 78 patients, and the three-dimensional reconstruction was considered to provide excellent view of the TD in 69 patients, segmentalization of TD in 4, and a poor view of the TD in 5. MRTD achieved a visualization rate of 94%. Most of the patients had a right-side TD that flowed into the left venous angle. Major configuration variations were noted in 14% of cases. Minor anomalies, such as divergence and meandering, were frequently seen.
Conclusion
MRTD allows noninvasive evaluation of TD and can be used to identify TD configuration. Thus, this technique is considered to contribute positively to safer performance of thoracic surgery.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Williams KR, Burford TH. The management of chylothorax. Ann Surg 1964;160:131–140.
Udagawa H, Akiyama H, Kirk RM. Oesophageal cancer. In: Kirk RM, editor. General surgical operation. 5th edn. Edinburgh: Elsevier; 2006. p. 139–157.
Clouse ME. Technique. In: Clouse ME, editor. Clinical lymphography (Golden’s diagnostic radiology). 1st edn. Baltimore: Williams & Wilkins; 1977. p. 61–75.
Adachi B. Der Ductus Thoracicus der Japaner. In: Kihara T, editor. Das Lymphgefässsystem der Japaner. Tokyo: Kenkyusha; 1953. p. 1–83.
Kotani M. The lymphatics and lymphoreticular tissues in relation to the action of sex hormones. Arch Histol Cytol 1990;53:1–76.
Van der Putte SCJ, van Limborgh J. The embryonic development of the main lymphatics in man. Acta Morphol Neerl Scand 1980;18:323–335.
Wirth W, Frommhold H. Der ductus thoracicus und seine variationen: lymphographische studie. Fortschr Geb Rontgenstr Nuklearmed 1970;112:450–459.
Gabella G. Cardiovascular system. In: Williams PL, editor. Gray’s anatomy. 38th edn. New York: Churchill Livingstone; 1995. p. 1451–1626.
McVay CB. Thoracic cavity and its contents. In: McVay CB, editor. Anson & McVay Surgical anatomy. Vol. 1. 6th edn. Philadelphia: Saunders; 1984. p. 385–482.
Hayashi S, Miyazaki M. Thoracic duct: visualization at nonenhanced MR lymphography: initial experience. Radiology 1999;212:598–600.
Davis HK. A statistical study of the thoracic duct in man. Am J Anat 1914;17:211–242.
Kausel HW, Reeve TS, Stein AA, Alley RD, Steranahan A. Anatomic and pathologic studies of the thoracic duct. J Thorac Surg 1957;34:631–641.
Nair SK, Petko M, Hayward MP. Aetiology and management of chylothorax in adults. Eur J Cardiothorac Surg 2007;32:362–369.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okuda, I., Udagawa, H., Takahashi, J. et al. Magnetic resonance-thoracic ductography: imaging aid for thoracic surgery and thoracic duct depiction based on embryological considerations. Gen Thorac Cardiovasc Surg 57, 640–646 (2009). https://doi.org/10.1007/s11748-009-0483-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-009-0483-4