
Abstract
Background
Gastric leak is a severe complication of gastric bypass that is associated with significant morbidity and mortality. Anastomosis dehiscence usually occurs at gastrojejunal anastomosis and can appear simultaneously with gastric leak, for which treatment can be a challenge. Fistula may have several clinical impacts, depending on patient-related factors, fistula characteristics, onset time, and therapy proposal. Abdominal toilet, drainage, gastrostomy, and revisional surgery constitute the traditional approaches to dehiscence and fistula closure, with variable results. Currently, endoscopic stents are gaining space, promoting fistula sealing, secretion deviation, treating gastric stricture, and allowing early oral diet. Herein, we present a case of severe gastrojejunal anastomosis dehiscence treated with partially covered stent.
Materials and Methods
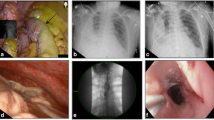
We present a video of a 39-year-old man with a body mass index of 40 Kg/m2 who underwent a Roux-en-Y gastric bypass and presented fever and leukocytosis. Gastric leak was diagnosed 7 days after the bariatric surgery. At first, he was submitted to three reoperations: laparotomy with abdominal toilet, abdominal drain, and gastrostomy. Sepsis was controlled, but drain output maintained the same debit. On the 22nd POD, it was decided to place a metallic stent. As the first step, an endoscopist looked at the lesser curvature. There was no continuity to the alimentary limb, and the anastomosis was disrupted. Careful inflation and washing was done, allowing identification of the alimentary limb, followed by guidewire passage, with radioscopic control. Once the guidewire was positioned, stent placement was possible and safe. Upper edge of stent was placed in the lower third of the esophagus.
Results
Patient progressed uneventfully. After 4 weeks, stent removal was attempted. However, it was not possible due to endoluminal tissue hyperplasia. Argon plasma was used three times to promote proliferative mucosa ablation. Stent was removed after 53 days, with no migration. The abdominal drain was removed 1 week later. After 6-months follow-up, the patient remains asymptomatic.
Conclusion
Early dehiscence closure was observed, without recurrence. The use of partially covered self-expandable metallic stent is associated with lower migration rates; however, removal can be technically difficult due to tissue hyperplasia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
ᅟ
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from the individual participant included in the study.
Electronic supplementary material
ESM 1
(MP4 38157 kb)
Rights and permissions
About this article

Cite this article
Alhinho, H.C.A.W., Ferreira, F.C., Medeiros, R.C.L. et al. Severe Dehiscence of Gastrojejunal Anastomosis after Gastric Bypass: Its Cure by Using Partially Covered Stent and Avoiding Migration. OBES SURG 28, 594 (2018). https://doi.org/10.1007/s11695-017-3016-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-3016-8