
Abstract
Purpose
Myopic foveoschisis (MF), a major cause of visual loss in highly myopic patients, shows varied foveal anatomic characteristics. We determined how the foveal status is related to surgical results in MF.
Methods
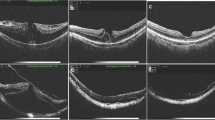
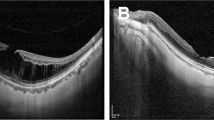
Forty-four eyes underwent vitrectomy for MF, including internal limiting membrane (ILM) peeling and gas tamponade. The eyes were divided into three groups depending on the preoperative foveal anatomy: foveal detachment (FD, n = 17), retinoschisis (RS, n = 16), and macular hole (MH, n = 11). Best-corrected visual acuity (BCVA) and optical coherence tomographic findings preoperatively and 3, 6, and 12 months postoperatively were obtained and compared.
Results
BCVA improved two lines or more in 81% of the FD group, 50% of the RS group, and 45% of the MH group 12 months postoperatively. The FD group had significantly improved vision (P < 0.01). Visual improvement was borderline in the RS group (P = 0.057) and not significant in the MH group. Visual improvement was significantly better in FD eyes than in RS (P < 0.05) or MH (P < 0.01) eyes. In FD and RS eyes, the postoperative BCVA was significantly correlated with age (P < 0.05) and preoperative BCVA (P < 0.01), whereas visual improvement was correlated with symptom duration (P < 0.05) and preoperative BCVA (P < 0.01).
Conclusions
Vitrectomy including ILM peeling and gas tamponade is safe and effective for MF. Patients with FD showed the most visual improvement postoperatively and therefore can obtain the most benefit from the surgery. Surgery also benefits RS and MH patients by preserving vision. The foveal status, age, duration of symptoms, and preoperative BCVA are key factors determining postoperative visual outcome in MF.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Phillips CI. Retinal detachment at the posterior pole. Br J Ophthalmol 1958;42:749–753.
Takano M, Kishi S. Foveal retinoschisis and retinal detachment in severely myopic eyes with posterior staphyloma. Am J Ophthalmol 1999;128:472–476.
Baba T, Ohno-Matsui K, Futagami S, et al. Prevalence and characteristics of foveal retinal detachment without macular hole in high myopia. Am J Ophthalmol 2003;135:338–342.
Kuhn F. Internal limiting membrane removal for macular detachment in highly myopic eyes. Am J Ophthalmol 2003;135:547–549.
Sayanagi K, Ikuno Y, Tano Y. Tractional internal limiting membrane detachment in highly myopic eyes. Am J Ophthalmol 2006;142:850–852.
Ikuno Y, Gomi F, Tano Y. Potent retinal arteriolar traction as a possible cause of myopic foveoschisis. Am J Ophthalmol 2005;139:462–467.
Bando H, Ikuno Y, Choi JS, Tano Y, Yamanaka I, Ishibashi T. Ultrastructure of internal limiting membrane in myopic foveoschisis. Am J Ophthalmol 2005;139:197–199.
Ishikawa F, Ogino N, Okita K, et al. Vitrectomy for macular detachment without macular hole in highly myopic eyes. Atarashii Ganka (J Eye) 2001;18:953–956.
Kanda S, Uemura A, Sakamoto Y, Kita H. Vitrectomy with internal limiting membrane peeling for macular retinoschisis and retinal detachment without macular hole in highly myopic eyes. Am J Ophthalmol 2003;136:177–180.
Kobayashi H, Kishi S. Vitreous surgery for highly myopic eyes with foveal detachment and retinoschisis. Ophthalmology 2003;110:1702–1707.
Ikuno Y, Sayanagi K, Ohji M, et al. Vitrectomy and internal limiting membrane peeling for myopic foveoschisis. Am J Ophthalmol 2004;137:719–724.
Hirakata A, Hida T. Vitrectomy for myopic posterior retinoschisis or foveal detachment. Jpn J Ophthalmol 2006;50:53–61.
Kwok AK, Lai TY, Yip WW. Vitrectomy and gas tamponade without internal limiting membrane peeling for myopic foveoschisis. Br J Ophthalmol 2005;89:1180–1183.
Spaide RF, Fisher Y. Removal of adherent cortical vitreous plaques without removing the internal limiting membrane in the repair of macular detachments in highly myopic eyes. Retina 2005;25:290–295.
Panozzo G, Mercanti A. Optical coherence tomography findings in myopic traction maculopathy. Arch Ophthalmol 2004;122:1455–1460.
Benhamou N, Massin P, Haouchine B, Erginay A, Gaudric A. Macular retinoschisis in highly myopic eyes. Am J Ophthalmol 2002;133:794–800.
Ikuno Y, Tano Y. Vitrectomy for macular holes associated with myopic foveoschisis. Am J Ophthalmol 2006;141:774–776.
Sayanagi K, Ikuno Y, Gomi F, Tano Y. Retinal vascular microfolds in highly myopic eyes. Am J Ophthalmol 2005;139:658–663.
Gandorfer A, Haritoglou C, Gandorfer A, Kampik A. Retinal damage from indocyanine green in experimental macular surgery. Invest Ophthalmol Vis Sci 2003;44:316–323.
Sippy BD, Engelbrecht NE, Hubbard GB, et al. Indocyanine green effect on cultured human retinal pigment epithelial cells: implication for macular hole surgery. Am J Ophthalmol 2001;132:433–435.
Kimura H, Kuroda S, Nagata M. Triamcinolone acetonide-assisted peeling of the internal limiting membrane. Am J Ophthalmol 2004;137:172–173.
Ikuno Y, Sayanagi K, Oshima T, et al. Optical coherence tomographic findings of macular holes and retinal detachment after vitrectomy in highly myopic eyes. Am J Ophthalmol 2003;136:477–481.
Polito A, Lanzetta P, Del Borrello M, et al. Spontaneous resolution of a shallow detachment of the macula in a highly myopic eye. Am J Ophthalmol 2003;135:546–547.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Ikuno, Y., Sayanagi, K., Soga, K. et al. Foveal anatomical status and surgical results in vitrectomy for myopic foveoschisis. Jpn J Ophthalmol 52, 269–276 (2008). https://doi.org/10.1007/s10384-008-0544-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10384-008-0544-8