
Abstract
Purpose
The first-pass effect during mechanical thrombectomy improves clinical outcomes regardless of first-line treatment approach, but current success rates for complete clot capture with one attempt are still less than 40%. We hypothesize that the ThrombX retriever (ThrombX Medical Inc.) can better engage challenging clot models during retrieval throughout tortuous vasculature in comparison with a standard stent retriever without increasing distal emboli.
Materials and Methods
Thrombectomy testing with the new retriever as compared to the Solitaire stent retriever was simulated in a vascular replica with hard and soft clot analogs to create a challenging occlusive burden. Parameters included analysis of distal emboli generated per clot type, along with the degree of recanalization (complete, partial or none) by retrieval device verified by angiography.
Results
The ThrombX device exhibited significantly higher rates of first-pass efficacy (90%) during hard clot retrieval in comparison with the control device (20%) (p < 0.009), while use of both techniques during soft clot retrieval resulted in equivalent recanalization. The soft clot model generated higher numbers of large emboli (>200 μm) across both device groups (p = 0.0147), and no significant differences in numbers of distal emboli were noted between the ThrombX and Solitaire techniques.
Conclusions
Irrespective of clot composition, use of the ThrombX retriever demonstrated high rates of complete recanalization at first pass in comparison with a state-of-the-art stent retriever and proved to be superior in the hard clot model. Preliminary data suggest that risk of distal embolization associated with the ThrombX system is comparable to that of the control device.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Advancements in endovascular treatment options have significantly improved functional outcome of patients suffering from acute ischemic stroke (AIS) due to a large vessel occlusion.
However, consistent rates of successful recanalization may be compromised by the inability of most thrombectomy devices to completely remove the clot with one attempt. First-pass effect (FPE) is defined as achieving a complete (TICI 3) or near complete (TICI 2C) recanalization with a single thrombectomy pass. Patients with FPE show a higher rate of good clinical outcomes at 90 days as well as a lower rate of mortality when compared to those with failed FPE [1].
FPE may be affected by a variety of factors, including the composition of the clot. Clot composition and pre-interventional CT attenuation have been shown to be associated with the recanalization outcomes [2, 3]. Previous results suggested that fibrin-rich clots have a lower clot density in Hounsfield units (HU) on non-contrast CT images when compared to red blood cell-rich clots. The clot HU values (absolute HU or HU ratio) can be used to describe the clot characteristics and also predict clot length and volume [4]. Clots with high amounts of red blood cells have lower stiffness and elasticity. As a result, they are associated with shorter intervention times and fewer thrombectomy attempts when compared to clots with high percentage of fibrin [5].
In addition to recanalization rates, the development of distal emboli may also be an important factor influencing outcome. The use of clot retrievers can cause clot fragmentation with the release of distal emboli or emboli to new territory [6,7,8]. The presence of fragmented clots is a predictor of poor outcome [9], as disrupted clots can cause distal embolization in the previously unaffected area or blockage of collateral flow to the potentially salvageable tissue [10,11,12,13,14]. Procedural release of embolic particulate represents an opportunity to improve the design of thrombectomy systems.
The ThrombX Retriever (TXR; ThrombX Medical Inc., Santa Clara, CA) is a novel device composed of two nitinol baskets that act as an engaging compartment that has recently received CE mark. This engaging compartment is composed of a distal expandable and proximal element with the intent to clasp or hold the thrombus in the device. We hypothesize that a thrombectomy system, such as the ThrombX retriever can improve the rate of first-pass success by enhancing the clot-device interaction. This is especially critical when dealing with the hard clot such as the fibrin-rich clot. The objective of this study was to evaluate the recanalization rates of hard and soft clot occlusions as well as the generation of distal emboli liberated after a thrombectomy procedure using the TXR in comparison with the Solitaire Revascularization Device (Medtronic Neurovascular, Irvine, CA) in an in vitro, simulated use experiment.
Materials and Methods
Vascular Occlusion Model
A silicone vascular replica mimicking the geometry of the human complete circle of Willis, middle cerebral artery (MCA), anterior cerebral artery (ACA), intracranial internal carotid artery (ICA) with challenging anatomy was selected. Magnetic resonance angiograms from 20 patients were used to produce a population-representative anatomical model of severe ICA-siphon curvature with an average curvature of 0.64 mm−1 (Fig. 1A), since it is often the most challenging segment for access to the intracranial vasculature. The model was constructed using a small-batch manufacturing process for device testing as previously described [15]. In order to augment the anatomical challenge, a tortuous segment of extracranial internal carotid artery (Fig. 1B) was attached to the model acquired from a patient case where significant difficulty advancing the distal access catheter was encountered during ICA navigation.

(A) Mechanical thrombectomy was simulated with the tortuous ICA siphon (square outline). (B) Model of internal carotid artery with redundant loop in cervical segment (square outline) attached to the circle of Willis model
The silicone replica was connected to a flow loop which contains a peristaltic roller pump used to deliver an oscillatory flow of saline solution 0.9%, adjustable clamps to control distal resistance, flow and pressure sensors with continuous monitoring of carotid and MCA flow and pressure, respectively. Peripheral resistance was adjusted to achieve human physiologic representative flow rates and pressures (common carotid ~340 ml/min, MCA ~130 ml/min) [16].
Clot Characteristics
Two types of clot models, a stiff elastic clot and a soft friable clot, were prepared for device testing [17]. The friable clot (diameter: 4.3 mm) was generated by thrombin-induced clotting of bovine blood (2.5 NIHU thrombin/ml blood) with the addition of fibrinogen and barium sulfate (1 g/10 ml blood), the latter making the clot radiopaque. The stiffness of this clot under low strain (0–45%) is 130 Pa and is similar to clinical specimens [17]. This type of clot was prone to fragmentation during mechanical thrombectomy and chosen to mimic the worst-case scenario with respect to clot fragmentation. The stiffer but more elastic clot (diameter: 4 mm) was derived from bovine blood with the addition of fibrinogen and calcium-phosphate apatite [18], and the absence of barium sulfate or other radiopaque additive makes this clot analog radiolucent. Fibrin-rich, challenging clots are estimated to be encountered in 20–50% of thrombectomy cases [19, 20]. This clot analog was more challenging for thrombectomy since the stiffness (280 Pa) at low strain (0–45%) is more than twofold greater than the soft clot [18]. Clot diameters were chosen according to the diameter of the target vessel in our model and ability to reliably create a large vessel occlusion. Consistency regarding percentage of red blood cells and fibrin has been shown to be reproducible and realistic through histologic testing of our clot specimens.
Clots were cut into 10 mm lengths, injected into the internal carotid artery through a syringe filled with normal saline and lodged in the middle cerebral artery (MCA) M1 segment reaching the MCA bifurcation to cause occlusion. The occlusion as well as the consistency of clot positioning was verified by angiography in all experiments. Clot length inside the silicone model elongated when lodged in the smaller M1 segment and ranged between 12 and 17 mm.
Flow Restoration Procedure
Devices were alternated using block randomization by coin flip to reduce bias. All soft clot procedures were performed consecutively, followed by hard clot experiments on subsequent days.
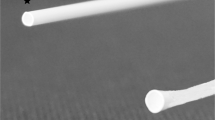
The ThrombX Retriever consists of two self-expanding nitinol baskets independently attached to a hypotube (proximal) and a core wire (distal). Platinum markers on the proximal and distal baskets allow fluoroscopic visualization. A handle on the proximal end of the device keeps the baskets locked in position while advancing the device in the microcatheter. Once the device is deployed, the handle is used to control the distance between baskets by pulling the distal basket toward the proximal basket. The TXR nitinol baskets were both 4.5 mm diameter, with a distal basket 20 mm long and a 9 mm proximal basket (Fig. 2).

The ThrombX device consists of two baskets that can articulate to trap the clot
ThrombX or the Solitaire devices were deployed under fluoroscopy to achieve recanalization per the manufacturer’s instructions for use and with common, standard-of-care techniques. The Solitaire was 4 mm in diameter and 40 mm in length. We selected a longer device since recent data suggest that longer stent retrievers are associated with improved first-pass effect [21]. In brief, a 0.088-in. long sheath (8F) was placed in the proximal ICA and was connected to a continuous drip infusion of normal saline.
A microcatheter (Headway 0.021 in., Microvention, Tustin, CA) was navigated over an 0.014-in. microwire distal beyond the end of the occlusive clot with its distal tip in the proximal superior division of the MCA bifurcation. The microwire was withdrawn followed by device delivery for thrombectomy. For positioning of the TRX device, the markers of the proximal and distal baskets were used so as the main clot burden would lie in the area in between. When the Solitaire device was used deployment was performed with the thrombus at the mid-proximal end of the device.
Following deployment, each device was left in place for 3 min prior to withdrawal. The devices were withdrawn under continuous slow retraction and without flow arrest or flow reversal during the initial part of the retrieval. Aspiration was applied via a pump when the device was in the proximal petrous segment of the carotid to avoid any effect from stripping the clot off the device as it was withdrawn into the 8F sheath. Angiography was performed at the end of the thrombectomy procedure to determine the recanalization. Since the deployed vascular phantom does not mimic the human distal cerebrovasculature beyond the M2 vessels, we have modified the clinical version of the TICI score specific to this model. Specifically, recanalization was rated as complete (fully re-opened), partial (retained clot in cerebral circulation, typically in one of the M2 branches) or none (continued occlusion of M1). Ten retrievals were carried out for each group. All retrievals were performed under fluoroscopy by the same operator (MGM, >10 years of experience). Only one thrombectomy attempt was allowed for each experiment, with 40 total experiments performed. Importantly, all effluent from both the MCA and ACA vascular territories was captured and clot fragments in the effluent larger than 200 μm were measured with a Coulter counter and recorded.
Statistical Analysis
All statistical calculations were performed using R3.5.2 using publicly available packages. For continuous data that were normally distributed, a Welch’s t test was used to determine if a factor was significantly followed by a Tukey’s post hoc test. Categorical data (recanalization rates) for a given clot type were compared with a Fisher’s exact test. An alpha of 0.05 was significant for all tests.
Results
Both devices either fully re-opened the circulation or left the M1 segment completely occluded, with no passes resulting in partial recanalization. The TXR demonstrated equivalent first-pass recanalization for the soft clot and significantly higher first-pass complete recanalization for the hard clot (p < 0.009, Fisher’s exact test) as compared to the gold-standard stent retriever. First-pass complete recanalization rates for soft and hard clot thrombectomies, respectively, are depicted in Fig. 3. It is shown that both devices achieved complete recanalization in nine out of ten soft clot thrombectomies. For the hard clot model, TXR achieved recanalization in nine out of ten while the Solitaire stent only in two out of ten thrombectomies performed.

Complete recanalization rates at first pass with soft clot and hard clot
In the soft clot cases, with barium impregnated clot, it was possible to see the relationship between the embolus and the device. The clot was observed to be held in the same location relative to the device throughout the retrieval in the cases where the TXR achieved reperfusion (Fig. 4). When the Solitaire achieved reperfusion, the clot was observed to be engaged by the device and mobilized as the device was pulled, but gradually it moved or rolled down the length of device and was not observed to be firmly held by the device struts. During some recanalization passes, the thrombus fully disengaged from the Solitaire; however, it was pulled out of the circulation by the aspiration applied at the end of the procedure (Fig. 5). These were counted as full recanalization and the Solitaire was able to show equivalent recanalization with soft clot in this test model.

Barium impregnated soft clot (arrow) retrieval with TXR demonstrating clot is maintained between proximal and distal basket markers throughout the retrieval process (arrows) with no clot migration relative to the device. The clot takes a u-shape as it is pinned between the baskets of the retriever (arrowhead)

Full recanalization during soft clot retrieval with the Solitaire device. During the extraction in the petrous segment of internal carotid artery, the clot (arrows) rolls along the surface of the device migrating to the distal markers (arrowheads) and is even hanging off of the end of the device as it is removed into the guide catheter
Soft clot generated more distal fragments than hard clot with both devices in sizes which were 200–1000 μm (p = 0.0147) and >1000 μm (p < 0.05). Figure 6 shows the average rates of distal emboli for soft and hard clot in the two size ranges over 10 retrieval attempts for the TXR and Solitaire. There was no significant difference in number of emboli between the TXR and Solitaire for either hard or soft clot.

Mean number of emboli with a single pass for each device with soft clot (A) and hard clot (B)
Eight and six total soft clot fragments >1000 μm were obtained from 5 TXR retrievals and 6 Solitaire retrievals, respectively. Solitaire generated 23 soft clot fragments 200–1000 μm versus 15 for the TXR. Two hard clot fragments >1000 μm were generated from one of ten TXR retrievals and two clot fragments were collected from two of ten Solitaire retrievals. Ten 200–1000-μm hard clot fragments were seen with Solitaire versus 14 for TXR.
Discussion
The design of the ThrombX retriever enabled the device to achieve a significantly higher rate of first-pass success with the hard clot model in comparison with the Solitaire retriever in an extremely challenging occlusion model. This is likely due to the phenomenon in which fibrin-rich clots tend to roll off of stent retrievers since with stiffer clots there is less integration of the clot into the stent cells [22, 23], whereas the articulating baskets of the TXR effectively trap the stiff clot for more efficient extraction. In addition, the performance of the thrombectomy system was tested in a vascular model with a nearly 360° turn at the proximal ICA and a severely tortuous ICA siphon. In this study, neither proximal flow control with a balloon guide catheter or combined use of distal aspiration with retrievers was modeled, which have been shown in similar in vitro modeling to provide a benefit [6, 7] since the goal of the study was to understand differences in retriever performance. The TXR device is conceptually different than thrombectomy assist devices, such as the Lazarus Cover [24,25,26] which is a braided structure proximal to a retriever that inverts over the retriever in the ICA in an effort to retain the clot. The TXR device is a contained system with two laser-cut nitinol baskets that when approximated by the operator effectively pin the clot between the baskets, perhaps explaining the improvement in first-pass complete recanalization with fibrin-rich clots that have a tendency to roll along the surface of standard stent retrievers.
The results also show in this model that the efficacy of the TXR did not vary with clot type. Clot composition has been shown to influence the recanalization rate. The clots used in this study show similar bulk mechanical properties as compared to clinical specimens [17]. Thrombi higher in erythrocyte content have shown higher rates of recanalization and reperfusion takes fewer retrieval attempts [2]. In contradistinction, fibrin-rich thrombi have been shown to be more difficult to remove and require more passes [27]. In vitro studies have shown that thrombus with high fibrin content is more difficult for stent retrievers to mobilize and remove [28, 29]. A recent report analyzed the thrombus composition with each pass using both stent retrievers and aspiration catheters alone or together [30]. It found that in the first two passes performed there was a high red cell content in the retrieved clot. However, when three or more passes were needed, sequential thrombus fragments retrieved following two or more passes had a much higher fibrin content compared to those recovered in earlier passes. This suggests there can be variation in the composition of the thrombus with some regions having higher fibrin content and being more resistant to retrieval. A device able to more efficiently retrieve the full spectrum of thrombus would clearly have a benefit in these circumstances.
The clot models used in this study have similar physical characteristics to specimens retrieved clinically from patients having acute ischemic strokes [17]. While the soft clot used in this study is easier to retrieve it is also more prone to fragmentation. The soft clot demonstrated more emboli with either device. The test circumstances were potentially designed to show more emboli without the use of proximal flow control, performing the retrieval in a tortuous model and use of aspiration only when the thrombus was close to the being withdrawn into the sheath. One concern was that the handling of the thrombus by the TXR, with an inherently different method of securing the clot, where the clot is clasped between two baskets rather than being wrapped around as with stent retrievers like the Solitaire, might result in more emboli due to different mechanical forces applied on the clot causing eventually fragmentation of the material, but this did not prove to be the case.
This study has limitations. An in vitro model does not replicate the true forces experienced by arterial wall–thrombus interaction. Clots of only a single uniform length were tested in the model. As this was a study of first-pass efficacy, distal emboli were only quantified from a single pass, potentially reducing the opportunity to detect more significant embolization with multiple passes when recanalization attempts had failed with the first pass. We used a single operator who could not be blinded to the device type since it appears differently on fluoroscopy, which could have introduced bias in the outcome.
Conclusion
This study evaluated a new retriever design, the TXR, in a tortuous anatomic model of the anterior cerebral circulation with challenging clot models. The TXR showed similar rates of first-pass recanalization with soft clot and significantly higher rates of recanalization for hard clot when compared to the control device. The rates of distal embolization for both hard and soft clot were the same for both devices. These results suggest that the ability of the TXR to recanalize a large vessel occlusion is not dependent on clot type like the first-generation stent retriever when used without any adjunctive devices. On-going clinical evaluation is required to confirm these observations in patients.
References
Zaidat OO, et al. First pass effect: a new measure for stroke thrombectomy devices. Stroke. 2018;49(3):660–6.
Maekawa K, et al. Erythrocyte-rich thrombus is associated with reduced number of maneuvers and procedure time in patients with acute ischemic stroke undergoing mechanical thrombectomy. Cerebrovasc Dis Extra. 2018;8(1):39–49.
Sporns PB, et al. Ischemic stroke: histological thrombus composition and pre-interventional CT attenuation are associated with intervention time and rate of secondary embolism. Cerebrovasc Dis. 2017;44(5–6):344–50.
Mokin M, et al. Thrombus density predicts successful recanalization with Solitaire stent retriever thrombectomy in acute ischemic stroke. J Neurointerv Surg. 2015;7(2):104–7.
Hashimoto T, et al. Histopathologic analysis of retrieved thrombi associated with successful reperfusion after acute stroke thrombectomy. Stroke. 2016;47(12):3035–7.
Chueh JY, et al. Reduction in distal emboli with proximal flow control during mechanical thrombectomy: a quantitative in vitro study. Stroke. 2013;44(5):1396–401.
Chueh JY, et al. Risk of distal embolization with stent retriever thrombectomy and ADAPT. J Neurointerv Surg. 2016;8(2):197–202.
Mordasini P, et al. In vivo evaluation of the first dedicated combined flow-restoration and mechanical thrombectomy device in a swine model of acute vessel occlusion. AJNR Am J Neuroradiol. 2011;32(2):294–300.
Gratz PP, et al. Whole-brain susceptibility-weighted thrombus imaging in stroke: fragmented thrombi predict worse outcome. AJNR Am J Neuroradiol. 2015;36:1277–82.
Akins PT, et al. Complications of endovascular treatment for acute stroke in the SWIFT trial with Solitaire and Merci devices. AJNR Am J Neuroradiol. 2014;35:524–8.
Kurre W, et al. Frequency and relevance of anterior cerebral artery embolism caused by mechanical thrombectomy of middle cerebral artery occlusion. AJNR Am J Neuroradiol. 2013;34(8):1606–11.
Soize S, et al. Predictive factors of outcome and hemorrhage after acute ischemic stroke treated by mechanical thrombectomy with a stent-retriever. Neuroradiology. 2013;55(8):977–87.
Todo A, et al. Incidence and outcome of procedural distal emboli using the Penumbra thrombectomy for acute stroke. J Neurointerv Surg. 2012;5(2):135–8.
Zhu L, et al. Thrombus branching and vessel curvature are important determinants of middle cerebral artery trunk recanalization with Merci thrombectomy devices. Stroke. 2012;43(3):787–92.
Chueh JY, Wakhloo AK, Gounis MJ. Neurovascular modeling: small-batch manufacturing of silicone vascular replicas. AJNR Am J Neuroradiol. 2009;30(6):1159–64.
Blankensteijn JD, et al. Flow volume changes in the major cerebral arteries before and after carotid endarterectomy: an MR angiography study. Eur J Vasc Endovasc Surg. 1997;14(6):446–50.
Chueh JY, et al. Mechanical characterization of thromboemboli in acute ischemic stroke and laboratory embolus analogs. AJNR Am J Neuroradiol. 2011;32(7):1237–44.
Chueh J-Y, et al. Characteristics of clots from acute ischemic stroke and laboratory analogs. In: Summer biomechanics, bioengineering, and biotransport conference, Tucson, AZ, 2017.
Liebeskind DS, et al. CT and MRI early vessel signs reflect clot composition in acute stroke. Stroke. 2011;42(5):1237–43.
Fennell VS, et al. What to do about fibrin rich ‘tough clots’? Comparing the Solitaire stent retriever with a novel geometric clot extractor in an in vitro stroke model. J Neurointerv Surg. 2018;10(9):907–10.
Zaidat OO, et al. Impact of stent retriever size on clinical and angiographic outcomes in the STRATIS Stroke Thrombectomy Registry. Stroke. 2019;50(2):441–7.
van der Marel K, et al. Quantitative assessment of device-clot interaction for stent retriever thrombectomy. J Neurointerv Surg. 2016;8(12):1278–82.
Weafer FM, et al. Characterization of strut indentation during mechanical thrombectomy in acute ischemic stroke clot analogs. J Neurointerv Surg. 2019;11(9):891–7.
Chueh JY, Puri AS, Gounis MJ. An in vitro evaluation of distal emboli following Lazarus Cover-assisted stent retriever thrombectomy. J Neurointerv Surg. 2017;9(2):183–7.
Fargen KM, Mocco J, Gobin YP. The Lazarus Funnel: a blinded prospective randomized in vitro trial of a novel CE-marked thrombectomy assist device. J Neurointerv Surg. 2016;8(1):66–8.
Mokin M, et al. Stent retriever thrombectomy with the Cover accessory device versus proximal protection with a balloon guide catheter: in vitro stroke model comparison. J Neurointerv Surg. 2016;8(4):413–7.
Yuki I, et al. The impact of thromboemboli histology on the performance of a mechanical thrombectomy device. AJNR Am J Neuroradiol. 2012;33(4):643–8.
Machi P, et al. Experimental evaluation of stent retrievers’ mechanical properties and effectiveness. J Neurointerv Surg. 2017;9(3):257–63.
Boeckh-Behrens T, et al. Thrombus histology suggests cardioembolic cause in cryptogenic stroke. Stroke. 2016;47(7):1864–71.
Duffy S, et al. Per-pass analysis of thrombus composition in patients with acute ischemic stroke undergoing mechanical thrombectomy. Stroke. 2019;50(5):1156–63.
Funding
This study was funded by a sponsored research contract by ThrombX Medical.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Chueh: Fee-for-service consulting for Stryker Neurovascular and InNeuroCo Inc.
Marosfoi: Fee-for-service consulting for Stryker Neurovascular, ThrombX and InNeuroCo Inc.
Anagnostakou: The author declares no conflict of interest.
Arslanian: The author declares no conflict of interest.
Marks: Founder and shareholder in ThrombX.
MJG: Has been a consultant on a fee-per-hour basis for Cerenovus, Imperative Care, Medtronic Neurovascular, Mivi Neurosciences, Phenox, Route 92 Medical, Stryker Neurovascular; holds stock in Imperative Care, InNeuroCo and Neurogami; and has received research support from the National Institutes of Health (NIH), the United States – Israel Binational Science Foundation, Anaconda, Apic Bio, Axovant, Cerenovus, Ceretrieve, Cook Medical, Gentuity, Imperative Care, InNeuroCo, Magneto, Microvention, Medtronic Neurovascular, MIVI Neurosciences, Neuravi, Neurogami, Philips Healthcare, Rapid Medical, Route 92 Medical, Stryker Neurovascular, Syntheon and the Wyss Institute.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
Not applicable.
Consent for Publication
For this type of study, consent for publication is not required.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chueh, JY., Marosfoi, M.G., Anagnostakou, V. et al. Quantitative Characterization of Recanalization and Distal Emboli with a Novel Thrombectomy Device. Cardiovasc Intervent Radiol 44, 318–324 (2021). https://doi.org/10.1007/s00270-020-02683-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-020-02683-3