
Abstract
The Spanish version of the Wisconsin Stone Quality of Life (WISQOL) questionnaire was developed and validated. A double-back translation of the WISQOL was conducted and syntactic amendments were made, resulting in the Spanish version of the WISQOL (S-WISQOL) which then went through a readability analysis. Stone formers from two hospitals in Mexico (Merida and Monterrey) filled in the S-WISQOL and the Short Form 36 (SF36). Convergent validity was assessed by the correlation of both questionnaires. Internal consistency was evaluated by Cronbach’s α, and external validity by comparing between centers. The impact of clinical settings on patients’ health-related quality of life (HRQOL) scores was tested. Each hospital’s institutional review board approved the project and informed consent was obtained from all participants. A total of 87 Spanish-speakers patients completed the S-WISQOL and SF36 and a good correlation was found between both (r = 0.75, p < 0.001). S-WISQOL readability was rated as “easy”. Patients from Merida had longer median duration (years) with stones, more stone-related procedures, and hospitalizations, and scored lower on WISQOL (p = 0.006). Internal consistency was good as Cronbach’s α coefficients ranged between acceptable and excellent. Stone-related admissions and duration of stones were inversely correlated with S-WISQOL score (− 0.254 and − 0.283, respectively; p < 0.005) but not to SF36. The S-WISQOL is an internally consistent, reliable, and valid instrument to assess HRQOL in Spanish-speaking patients with kidney stones. The S-WISQOL is generalizable as demonstrated by good external validity among centers. S-WISQOL scores can be added as an outcome for kidney stone treatments.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The prevalence of kidney stones (KS) has been rising worldwide but is more noticeable in developing countries. Moreover, KS has a high recurrence rate of 30% at 10 years and often triggers the need for invasive procedures [1,2,3]. Despite Spanish language ranks among the three most spoken languages around the world, the impact of KS over Spanish-speaking patients’ lives has not been widely reported. In 2002, Medina-Escobedo et al., found a self-reported KS prevalence of 5.5% in southeast Mexico. Furthermore, KS was the leading indication for a nephrectomy (~ 60%) in the health system database [4, 5].
Patients with KS have a lower health-related quality of life (HRQOL) when compared to non-stone formers. Likewise, patients with stones and/or stone-related symptoms have lower HRQOL than patients who are free from stones and/or symptoms. KS affects patients’ quality of life (QoL) in several spheres, including work, financial expense, and lifestyle. Therefore, it has been suggested that HRQOL should be an important outcome of KS management [7, 8]. When evaluating the impact of KS disease, related complications, and the procedures performed for its diagnosis and treatment, urologists usually rely on several outcomes or markers to determine the success of treatment. (i.e., stone-free rate). However, the patient’s own perception of his/her illness as an indicator of success should be considered, and the HRQOL assessment is an objective and accurate way to do it.
Several tools to assess patients’ HRQOL have been validated in Spanish, such as the widely used Short Form (SF36) health survey, but some particularities among diseases can interfere in how HRQOL is measured [9]. Therefore, a disease-specific evaluation of HRQOL is a better approach. Recently, the Wisconsin Stone Quality of Life Questionnaire (WISQOL), which contains 28 items grouped into 4 domains, was developed and validated to assess HRQOL in patients with KS. This questionnaire has proven to be a better assessment tool measuring HRQOL associated with KS than the SF36.[10, 11]. Our objective was to develop and internally and externally validate a Spanish version of the WISQOL (S-WISQOL) in a Mexican population. A secondary objective was to assess the HRQOL of patients with different profiles of KS at two medical centers using the validated instrument.
Methods
Translation
After approval from authors of the original WISQOL, a double-back translation was performed by two different certified translators. Then a panel of urologists (MBM, DOP, CMP, JPFT) discussed wording discrepancies between the two translated versions and a first draft was obtained. It was administrated to 5 subjects for feedback. Writing and syntactic corrections were made resulting in the final version of the S-WISQOL (Online Resource 1). The Fernández-Huerta method was used to assess the readability of both questionnaires, the S-WISQOL and SF36 [12].
Inclusion criteria and data selection
All participants prospectively included were native Spanish-speakers and stone formers living in Mexico. Participants with at least elementary school education (6 years of schooling), without any visual or cognitive impairment, and without acute illness were invited to enroll at the 2 medical centers involved in the study (Merida and Monterrey). Patients who did not complete the questionnaire were excluded.
Additionally, sociodemographic and clinical data were obtained through an interview. Stone-related issues such as years with KS, hospitalizations and procedures due to KS, JJ status, and single kidney status, were documented to evaluate the overall impact of KS. Every participant signed an informed consent, and the study protocol was approved by the ethics and research committee from each of the institutions that recruited subjects.
Statistical analysis
Internal consistency of the S-WISQOL was obtained with Cronbach’s α overall and between centers. External validity was assessed by comparing S-WISQOL results between both centers. The Spearman test was used for item and domain correlations and for S-WISQOL total score. Correlation of total scores of the S-WISQOL and SF36 was assessed to determine convergent validity. Correlations between clinical variables and results from the S-WISQOL and SF36 were analyzed to assess the effects of these on results. In addition, S-WISQOL total scores were compared between subjects from different clinical settings to determine any impact on HRQOL.
For categorical variables the χ2 test was used. The U Mann–Whitney or T test were used for quantitative data, according to its distribution as assessed by the Kolmogorov–Smirnov normality test. Data were analyzed with IBM® SPSS™v.21, p values < 0.05 were considered statistically significant. Cronbach’s α and correlation coefficients results were interpreted as in the original WISQOL development study [11].
Results
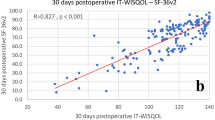
A total of 87 subjects completed the S-WISQOL and SF36. Subject’s baseline characteristics are summarized in Table 1. The Fernandez–Huerta readability test found the S-WISQOL as “easy”, and the SF36 as “fairy easy”, which means that 6 and 5 years of schooling, respectively, are needed for understanding. A good correlation between SF36 and S-WISQOL total scores was observed (r = 0.75, p < 0.001) as shown in Fig. 1.

Correlation between S-WISQOL and SF36 total scores in stone-formers
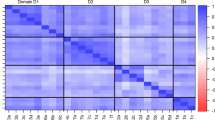
S-WISQOL internal consistency overall and at each center is presented in Table 2. Spearman correlation coefficients ranged from 0.60 to 0.89 (mean 0.73) and were, thus, considered as good. Interdomain and domain–total score Cronbach’s α coefficient went from acceptable to excellent. In the Merida sample, domain 1–2 and 2–4 coefficients were lower, confirming that they are measuring different constructs.
Domains comparison between centers is presented in Table 3.
A weak correlation of years with KS and S-WISQOL score (− 0.283, p = 0.008) was found, but this was not true for the SF36 (p = 0.058). Similarly, the number of hospitalizations due to KS and S-WISQOL total score (− 0.254, p = 0.018) were correlated, but neither was correlated with the SF36 (p = 0.153).
There were no differences for S-WISQOL total scores between subjects with and without an indwelling JJ-stent at enrollment (p = 0.255). Other comparisons were also not significant, such as between those receiving renal replacement therapy and not (p = 0.787), those with and without type 2 diabetes mellitus (p = 0.788), those with and without hypertension (p = 0.818), or subjects with single-kidney status and those with both kidneys intact (p = 0.314).
Discussion
This comprehensive study shows that the S-WISQOL is a valid tool to assess the HRQOL of Spanish-speaking patients with KS. Spanish is the second most spoken language worldwide; thereby, this work provides a reliable and easy-to-read instrument to assess the disease-specific HRQOL in Spanish-speaking countries or Spanish-speaking immigrants.
Convergent validity was shown by a good correlation between S-WISQOL and SF36 total scores (Fig. 1). The SF36 can be influenced by other comorbidities; whereas, the S-WISQOL focuses solely on the effects of KS on HRQOL. Similar results were found in the original WISQOL and in a recently validated Turkish version, showing a moderate and acceptable correlation, respectively. Moreover, we found that readability between both tests was similar and all subjects enrolled in this study met the required years of schooling for proper comprehension; hence, the differences found between the S-WISQOL and SF36 questionnaires are not attributable to its understanding [9, 13].
We found that internal consistency was comparable between centers. In addition, interdomain correlations were all acceptable, and total score–domain measures ranged from good to excellent. Spearman correlation coefficients were considered good (Table 2). These results show the strong impact of each domain on S-WISQOL scores. Correlations between domains 1 (social) and 2 (emotional), and between domains 2 and 4 (vitality) were moderate. Likewise, psychometric analysis of the Turkish version of the WISQOL found a moderate correlation between domains 2 and 4, and so did the analysis of the original WISQOL. In agreement with authors, it is considered that higher correlations would have suggested insufficient differences between subscales [9, 13].
External validity analysis showed that S-WISQOL scores were different between centers (Table 3). This finding supports that HRQOL impairment is different for each patient, as subjects from Merida had a longer duration of time with KS, and higher numbers of procedures and hospitalizations due to KS. All these features showed a correlation with total S-WISQOL scores. Thus, the lower scores of the S-WISQOL among these patients are reasonable. Nevertheless, these variables did not affect SF36 results, indicating that the S-WISQOL is better at detecting stone-related conditions affecting HRQOL than the SF36. These findings, altogether with the easy readability results, confirm the external validity and reliability of the S-WISQOL. Likewise, S-WISQOL score was not influenced by other medical conditions that are prone to affect HRQOL, like the presence of a JJ-stent, renal replacement therapy, type 2 diabetes mellitus, and hypertension, enhancing further the fact that the S-WISQOL is an effective instrument to assess disease-specific HRQOL of patients with KS. In fact, evidence supports that HRQOL is impaired in asymptomatic stone patients, suggesting that the WISQOL may be sensitive to underlying effects of KS that patients may not sense or report as “symptoms” [14].
Domain score comparisons between centers showed differences in all domains but 3 (stone-related symptoms). This suggests that baseline differences between patients from each center, as previously mentioned (Table 1), may have impacted the social, emotional, and vitality domains and might explain the differences found for S-WISQOL scores.
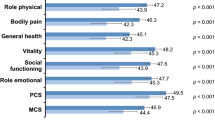
This observation is supported by a recent review showing that most patients with KS have worse HRQOL, as assessed by the SF36, the most affected domains were bodily pain and general health, concluding that the way KS affects HRQOL might have a role in the decision-making for treatment [8].
Contrary to the development of the original WISQOL, in this work, all patients had stones at enrollment. There is evidence supporting that the stone itself may cause worst HRQOL. A recent publication found that asymptomatic stone formers with current stones, whether they were aware or not, had lower HRQOL than asymptomatic patients without stones at the time they were surveyed [10].
Donnally et al., conducted a follow-up study to assess changes in HRQOL over time using the SF36. Although low scores were obtained, no changes between baseline and follow-up were found. This is perhaps because the SF36 was not the most suitable tool for detecting changes in KS status at follow-up [15]. We believe that S-WISQOL is a better tool for assessing follow-up changes in HRQOL among stone formers. Other studies have demonstrated the impact on HRQOL of certain treatments for KS; Pérez-Fentes et al., found an improvement in the bodily pain domain of the SF36 after stone treatment [16]. Using the EQ-SD index, also a generic HRQOL instrument, Eryildirimir et al., found that patients who received medical expulsive therapy had better HRQOL than those treated for colic [17]. The Turkish WISQOL found an improvement in WISQOL total score and within the four WISQOL domains four weeks after percutaneous nephrolithotomy (p < 0.001). Likewise, using the WISQOL, Jiang et al., found that using a nephrostomy tube rather than a JJ-stent after a percutaneous nephrolithotomy leads to better HRQOL; and de Sousa Morais et al., supported this finding, as they reported a higher negative impact on HRQOL in patients undergoing retrograde JJ-stent placement than those treated with percutaneous nephrostomy placement for urgent urinary diversion due to KS [18, 19]. Other studies have showed that stone formers who use potassium citrate or thiazides, and stone formers with cystinuria undergoing tiopronin, scored better in all WISQOL domains vs. those who were not prescribed these medications [20, 21].
Further studies assessing HRQOL in KS patients using the S-WISQOL are warranted in the next few years, and the resulting data could lead to better and yet more informed decision-making. The self-reported perceptions of patients about their own disease is a tangible and objective way to assess HRQOL. This is important as everything that is measured might be improved.
Some limitations are identified. First, the validation was conducted in patients from northeast and southeast Mexico. To assess the broader generalizability of the S-WISQOL within a Spanish-speaking population, further studies with wider cultural backgrounds and involving patients from diverse regions are needed. Second, a relatively small number of patients was included. Finally, larger-scale external validations are needed as are assessments of the predictability of the S-WISQOL in capturing changes over time in a patient’s stone and/or stone-related symptom status.
Conclusions
KS impairs patients’ HRQOL. The recently developed S-WISQOL is a valid and reliable instrument for assessing disease-specific HRQOL. With this instrument, the impact of KS overall and of related diagnostic and therapeutic procedures can be objectively assessed. Here, we provide a valid, reliable, and easy-to-read Spanish version of the WISQOL questionnaire which will be useful to both urologists and patients in Spanish-speaking settings as we move forward to improving our patients’ HRQOL.
References
Sorokin I, Mamoulakis C, Miyazawa K, Rodgers A, Talati J, Lotan Y (2017) Epidemiology of stone disease across the world. World J Urol 35(9):1301–1320. https://doi.org/10.1007/s00345-017-2008-6
Alatab S, Pourmand G, El Howairis MEF, Buchholz N, Najafi I, Pourmand MR et al (2016) National profiles of urinary calculi: A comparison between developing and developed worlds. Iran J Kidney Dis 10(2):51–61
Saigal CS, Joyce G, Timilsina AR, Urologic Disease in America Project (2005) Direct and indirect costs of nephrolithiasis in an employed population: opportunity for disease management? Kidney Int 68(4):1808–1814. https://doi.org/10.1111/j.1523-1755.2005.00599.x
Medina-Escobedo M, Zaidi M, Real-de-León E, Orozco-Rivadeneyra S (2002) Prevalencia y factores de riesgo en Yucatán, México, para litiasis urinaria. Salud Pública Mex 44(6):541–545
Medina-Escobedo M, Martín-Soberanis G (2009) Nefrolitiasis como indicación de nefrectomía. Estudio multicéntrico. Rev Med Inst Mex Seguro Soc 74(1):29–32
Bryant M, Angell J, Tu H, Goodman M, Pattaras J, Ogan K (2012) Health related quality of life for stone formers. J Urol 188(2):436–440. https://doi.org/10.1016/j.juro.2012.04.015
Romero V, Akpinar H, Assimos DG (2010) Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Rev Urol 12(2–3):86–96
New F, Somani BK (2016) A Complete world literature review of quality of life (QOL) in patients with kidney stone disease (KSD). Curr Urol Rep 17(12):88. https://doi.org/10.1007/s11934-016-0647-6
Vilagut G, Ferrer M, Rajmil L, Rebollo P, Permanyer-Miralda G, Quintana JM et al (2005) The Spanish version of the Short Form 36 Health Survey: a decade of experience and new developments. Gac Sanit 19(2):135–150. https://doi.org/10.1157/13074369
Penniston KL, Nakada SY (2013) Development of an instrument to assess the health-related quality of life of kidney stone formers. J Urol 189(3):921–930. https://doi.org/10.1016/j.juro.2012.08.247
Penniston KL, Antonelli JA, Viprakasit DP, Averch TD, Sivalingam S, Sur RL et al (2017) Validation and reliability of the wisconsin stone quality of life questionnaire. J Urol 197(5):1280–1288. https://doi.org/10.1016/j.juro.2016.11.097
Fernández-Huerta J (1959) Medidas sencillas de lecturabilidad. Consigna (214):29–32 https://legible.es/blog/lecturabilidad-fernandez-huerta/#id1. Accessed 6 Mar 2018
Atalay HA, Ulker V, Canat L, Ozer M, Can O, Penniston KL (2018) Validation of the Turkish version of the Wisconsin stone-quality of life questionnaire. Turkish J Urol 16:1–6. https://doi.org/10.5152/tud.2018.35305
Penniston KL, Sninsky BC, Nakada SY (2016) Preliminary Evidence of Decreased Disease-Specific Health-Related Quality of Life in Asymptomatic Stone Patients. J Endourol 30(Suppl 1(S1)):S42–45. https://doi.org/10.1089/end.2016.0074
Donnally CJ, Gupta A, Bensalah K, Tuncel A, Raman J, Pearle MS et al (2011) Longitudinal evaluation of the SF-36 quality of life questionnaire in patients with kidney stones. Urol Res 39(2):141–146. https://doi.org/10.1007/s00240-010-0313-2
Pérez-Fentes DA, Gude F, Blanco B, Freire CG (2015) Percutaneous nephrolithotomy: short- and long-term effects on health-related quality of life. J Endourol 29(1):13–17. https://doi.org/10.1089/end.2014.0081
Eryildirim B, Sahin C, Tuncer M, Sabuncu K, Cetinel C, Tarhan F et al (2015) Effect of medical expulsive therapy on the health-related quality of life of patients with ureteral stones: a critical evaluation. Int Urol Nephrol 47(8):1271–1275. https://doi.org/10.1007/s11255-015-1036-7
Jiang H, Huang D, Yao S, Liu S (2017) Improving drainage after percutaneous nephrolithotomy based on health-related quality of life: a prospective randomized study. J Endourol 31(11):1131–1138. https://doi.org/10.1089/end.2017.0444
de Sousa MN, Pereira JP, Mota P, Carvalho-Dias E, Torres NJ, Lima E (2018) Percutaneous nephrostomy vs ureteral stent for hydronephrosis secondary to ureteric calculi: impact on spontaneous stone passage and health-related quality of life—a prospective study. Urolithiasis 47:567–573. https://doi.org/10.1007/s00240-018-1078-2
Raffin EP, Penniston KL, Antonelli JA, Viprakasit DP, Averch TD, Bird VG et al (2018) The effect of thiazide and potassium citrate use on the health-related quality of life of patients with urolithiasis. J Urol 200(6):1290–1294. https://doi.org/10.1016/j.juro.2018.06.023
Modersitzki F, Goldfarb DS, Goldstein RL, Sur RL, Penniston KL (2019) Assessment of health-related quality of life in patients with cystinuria on tiopronin therapy. Urolithiasis. https://doi.org/10.1007/s00240-019-01174-6
Acknowledgements
No competing financial interests exist. Partial results of this paper were presented in the 36th World Congress of Endourology in Paris in 2018.
Author information
Authors and Affiliations
Contributions
MB-M: protocol/project development, data collection or management, data analysis and manuscript writing/editing. JPF-T: protocol/project development and data collection or management. MDG-P: protocol/project development and data collection or management. AH: protocol/project development and data analysis. CM-P: protocol/project development, and data analysis. DO-P: protocol/project development, data collection or management, data analysis and manuscript writing/editing. KP: protocol/project development, data analysis and manuscript writing/editing. IAV-M: protocol/project development and data collection or management.
Corresponding author
Ethics declarations
Conflicts of interest
All authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Research and Ethics Committee (Reference Number: 2017–012) of the HRAEPY and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Basulto-Martínez, M., Olvera-Posada, D., Velueta-Martínez, I.A. et al. Quality of life in patients with kidney stones: translation and validation of the Spanish Wisconsin Stone Quality of Life Questionnaire. Urolithiasis 48, 419–424 (2020). https://doi.org/10.1007/s00240-020-01192-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-020-01192-9