
Abstract
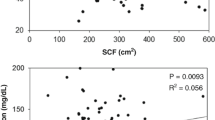
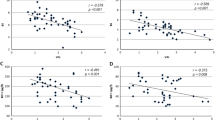
The aim of the present study was to investigate the association between the serum lipid profile and components of the metabolic syndrome, such as central obesity (anthropometric, computed tomography and fat cell data), insulin, sex-hormonebinding-globulin (SHBG) and different hormones influencing this important syndrome, e.g. sex steroids, leptin and tumor necrosis factor-alpha (TNF-α). The sample consisted of 85 obese patients (30 men and 55 women) who had undergone abdominal surgery. Fasting serum lipids were analysed, as well as anthropometric and computed tomography data, perivisceral and subcutaneous fat cell size and serum glucose and hormones. Abdominal fat revealed itself as an important correlator of the adverse changes in plasma lipoprotein levels, the waist-to-hip-ratio and waist-to-thigh-ratio being the best morphological correlators in men and women, respectively. Intra-abdominal fat (VA) correlated significantly and positively to perivisceral fat cell size in women, while no correlation was found between subcutaneous fat accumulation (SA) and adipocyte size in both genders. Perivisceral fat cell size showed the greatest number of correlations with the adverse plasma lipid profile compared to that in the subcutaneous depot. SHBG and sex steroids showed a negative correlation with serum lipids considered a cardiovascular risk. In contrast, TNF-α and C-peptide were inversely correlated with potential protector lipids. In conclusion, abdominal obesity, adipocyte hypertrophy from visceral fat, serum TNF-α and C-peptide seem to be the best correlators of the lipoprotein disturbance characteristic of the metabolic syndrome, whereas SHBG and sex steroids could play a protective role regarding the lipid profile associated to this syndrome.
Resumen
Se investiga la asociación entre el perfil lipídico del plasma y algunos componentes del síndrome metabólico, tales como la obesidad central, y los niveles de insulina, proteína transportadora de hormonas sexuales (SHBG), esteroides sexuales, leptina y factor de necrosis tumoral alfa TNFα. La muestra incluye 85 pacientes obesos (30 hombres y 55 mujeres) sometidos a cirugía abdominal. Analizados los lípidos plasmáticos en ayunas, datos antropométricosy de tomografía computerizada, tamaño del adipocito en grasa subcutánea y perivisceral y los valores plasmáticos de glucosa y hormonas, se observa correlación entre grasa abdominal y alteraciones de los valores plasmáticos de lipoproteínas, siendo los índices cintura-cadera y cintura-muslo los parámetros morfológicos que mejor correlación presenta en hombres y mujeres, respectivamente. La grasa intraabdominal (VA) se correlaciona significativa y positivamente con el tamaño del adipocito perivisceral en mujeres, mientras que no se encuentra correlación entre el tamaño adipocitario y la grasa subcutánea (SA) para ningún género. El tamaño adipocitario perivisceral presenta mayor número de correlaciones con el perfil lipídico desfavorable del plasma, comparado con el subcutáneo. Los esteroides sexuales y SHBG se correlacionan negativamente con los lípidos plasmáticos considerados de riesgo cardiovascular. Por el contrario, el péptido C y el TNFα lo hacen con lípidos potencialmente protectores. En conclusión, la obesidad abdominal y la hipertrofia de los adipocitos de la grasa visceral, junto con el péptido C y el TNFα plasmáticos se asocian positivamente con la alteración de las lipoproteínas característica del síndrome metabólico, mientras que los esteroides sexuales y SHBG parecen desempeñar un papel protector respecto del perfil lipídico.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Abate, N., Garg, A., Peshock, R. M., Stray-Gundersen, J. and Grundy, S. M. (1995):J. Clin. Inv.,96, 88–98.
Björntorp, P. (1993):Obes. Res.,1, 216–222.
Björntorp, P. (1998): In “Handbook of Obesity” (Bray, G. A., Bouchard, C. and James, W. P. T., eds.), Marcel Dekker, New York, pp. 573–600.
B. M. D. P. (1985): “Statistical software”, University of California Press, London.
Castelo-Branco, C., Casals, E., Martínez de Osaba, M. J., Shanllehy, C. and Fortuny, A. (1996):Acta Obstet. Gynecol. Scand.,75, 261–265.
Davis, S. R., McCloud, P., Strauss, B. J. and Burger, H. (1995):Maturitas,21, 227–236.
Dobbelsteyn, C. J., Joffres, M. R., MacLean, D. R., Flowerdew, G. and the Canadian Heart Health Surveys Research Group. (2001):Int. J. Obes.,25, 652–661.
Durnin, J. V. G. A. and Rahaman, M. M. (1967):Br. J. Nut.,21, 681–689.
Faust, T. (1981): In: “Recent advances in obesity research” (Björntorp, P., Cairella, M. and Howard, A. N., eds.), John Libbey, London.
Garaulet, M., Pérez-Llamas, F., Fuente, T., Zamora, S. and Tébar, F. J. (2000):Eur. J. Endoc.,143, 657–666.
Goodpaster, B. H., Leland-Thaete, F., Simoneau, J. A. and Kelley, D. E. (1997):Diabetes,46, 1579–1585.
Grundy, S. M. (1980): In “Atherosclerosis-V” (Gotto, A. M., Smith, L. C. and Allen, B., eds.), Springer, New York, pp. 586–589.
Haffner, S. M., Valdez, R. A., Stern, M. P. and Katz, M. S. (1993):Int. J. Obes.,17, 643–649.
Haffnet, S. M. and Valdez, R. A. (1995):Am. J. Med.,98, 40S-47S.
Haluzik, M., Fiedler, J., Nedvidkova, J. and Ceska, R. (1999):Physiol. Res.,48, 363–368.
Haluzik, M., Fiedler, J., Nedvidkova, J. and Ceska, R. (2000):Nutrition,16, 429–433.
Hautanen, A. (2000):Int. J. Obes.,24, Suppl. 2, S64-S70.
Horsten, M., Mittleman, M. A., Wamala, S. P., Schenck-Gustafsson, K. and Orth-Gomer, K. (1999):J. Cardiovascular Risk,6, 391–397.
Larsson, B., Svärdsudd, K., Welin, L., Wihelmsen, L., Björntorp, P. and Tibblin, G. (1984):Br. Med. J.,288, 1401–1404.
Levy, R. I. (1981):Clinical Chem.,27, 653–662.
Megnien, J. L., Denarie, N., Cocaul, M., Simon, A. and Levenson, J. (1999):Int. J. Obes.,23, 90–97.
Öhrvall, M., Berglund, L. and Vessby, B. (2000):Int. J. Obes.,24, 497–501.
Pollare, T., Vessby, B. and Lithell, H. (1991):Arterioscler. Thromb.,11, 1192–1203.
Pouliot, M. C., Deprés, J. P., Lemieux, S., Moorjani, S., Bouchard, C., Tremblay, A.et al. (1994):Am. J. Cardiol.,73, 460–468.
Reaven, G. M. and Chen, Y. D. I. (1988):Diabetes Metab.,4, 639–652.
Sarrel, P. M. (1998):Semin. Reprod. Endocrinol.,16, 121–128.
Shono, N., Kumagai, S., Higaki, Y., Nishizumi, M. and Sasaki, H. (1998):J. Ather. Thromb.,3, 41–51.
Simon, D., Charles, M. A., Nahoul, K., Orssaud, G., Kremski, J., Hully, V., Joubert, E., Papoz, L. and Eschwege, E. (1997):J. Clin. Endoc. Metab.,82, 682–685.
Sjöström, L., Björntorp, P. and Vrana, J. (1972):J. L. Res.,12, 521–530.
Sjöström, L. (1991):Int. J. Obes.,15, 19–30.
Spiegelman, B. M. and Flier, J. S. (2001):Cell,23, 531–543.
Tai, E. S., Lau, T. N., Ho, S. C., Fok, A. C. and Tan, C. E. (2000):Int. J. Obes.,24, 751–757.
Tauri, S., Tokunaga, K., Fujioka, S. and Matsuzawa, Y. (1991):Int. J. Obes.,15, 1–8.
Tchernof, A., Toth, M. J. and Poehlman, E. T. (1999):Diabetes Care,22, 1875–1881.
Terry, R. B., Stefanick, M. L., Haskell, W. L. and Wood, P. D. (1991):Metabolism,40, 733–740.
Valdez, R., Seidell, J. C., Ahn, Y. I. and Weiss, K. M. (1993):Int. J. Obes.,17, 77–82.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Garaulet, M., Pérez-Llamas, F., Zamora, S. et al. Interrelationship between serum lipid profile, serum hormones and other components of the metabolic syndrome. J. Physiol. Biochem. 58, 151–160 (2002). https://doi.org/10.1007/BF03179852
Received:
Issue Date:
DOI: https://doi.org/10.1007/BF03179852