
Abstract
Purpose: To evaluate the accuracy and precision of “deep-forehead” temperature with rectal, esophageal, and tympanic membrane temperatures, compared with blood temperature.
Methods: We studied 41 ASA physical status 1 or 2 patients undergoing abdominal and thoracic surgery scheduled to require at least three hours. “Deep-forehead” temperature was measured using a Coretemp® thermometer (Terumo, Tokyo, Japan). Blood temperature was measured with a thermistor of a pulmonary artery. Rectal, tympanic membrane, and distal esophageal temperatures were measured with thermocouples. All temperatures were recorded at 20 min intervals after the induction of anesthesia. We considered blood temperature as the reference value. Temperatures at the other four sites were compared with blood temperature using correlation, regression, and Bland and Altman analyses. We determined accuracy (mean difference between reference and test temperatures) and precision (standard deviation of the difference) of 0.5°C to be clinically acceptable.
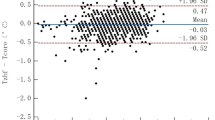
Results: “Deep-forehead” temperature correlated well with blood temperature as well as other temperatures, the determination coefficients (r2) being 0.85 in each case. The bias for the “deep-forehead” temperature was 0.0°C which was the same as tympanic membrane temperature and was smaller than rectal and esophageal temperatures. The standard deviation of the differences for the “deep-forehead” temperature was 0.3°C, which was the same as rectal temperature.
Conclusions: We have demonstrated that the “deep-forehead” temperature has excellent accuracy and clinically sufficient precision as well as other three core temperatures, compared with blood temperature.
Résumé
Objectif: Évaluer l’exactitude et la précision de la température frontale «cutanée profonde» et les températures rectale, œsophagienne et tympanique, comparées à la température du sang.
Méthode: L’étude a porté sur 41 patients d’état physique ASA I ou II devant subir une intervention chirurgicale abdominale et thoracique d’au moins deux heurs. La température «cutanée profonde» a été mesurée à l’aide du thermomètre Coretemp® (Terumo, Tokyo, Japon). Celle du sang a été prise avec une thermistance d’une artère pulmonaire et les températures rectale, tympanique et œsophagienne distale, avec des thermocouples. Elles ont toutes été enregistrées à 20 min d’intervalle après l’induction de l’anesthésie. La température du sang a servi de référence. Les températures des quatre autres sites ont été comparées avec celle du sang à l’aide d’analyses de corrélation, de régression et des analyses de Bland et Altman. Nous avons reconnu une exactitude (différence moyenne entre la température de référence et les autres) et une précision (écart type de la différence) de 0,5 °C près comme une différence acceptable en clinique.
Résultats: La température «cutanée profonde» était en corrélation avec celle du sang, et avec celle des autres sites, le cofficient de détermination (r2) étant de 0,85 dans chaque cas. Le biais de la température «cutanée profonde» était de 0,0 °C, comme celui de la température tympanique, et plus faible que ceux des températures rectale et œsophagienne. L’écart type de la différence pour la température «cutanée profonde» était de 0,3 °C, comme pour la température rectale.
Conclusion: Nous avons démontré que la température frontale pronfonde présentait une grande exactitude et une précision utile suffisante, autant que les trois autres températures centrales, comparée à la température du sang.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Sessler DI. Mild perioperative hypothermia. N Engl J Med 1997; 336: 1730–7.
Matsukawa T, Sessler DI, Sessler AM, et al. Heat flow and distribution during induction of general anesthesia. Anesthesiology 1995; 82: 662–73.
Frank SM, Beattie C, Christopherson R, et al. Epiduralversus general anesthesia, ambient operating room temperature, and patient age as predictors of inadvertent hypothermia. Anesthesiology 1992; 77: 252–7.
Heier T, Caldwell JE, Sessler DI, Miller RD. Mild intra-operative hypothermia increases duration of action and spontaneous recovery of vecuronium blockade during nitrous oxide-isoflurane anesthesia in humans. Anesthesiology 1991; 74: 815–9.
Valeri CR, Khabbaz K, Khuri SF, et al. Effect of skin temperature on platelet function in patients undergoing extracorporeal bypass. J Thorac Cardiovasc Surg 1992; 104: 108–16.
Just B, Delva E, Camus Y, Lienhart A Oxygen uptake during recovery following naloxone. Relationship with intraoperative heat loss. Anesthesiology 1992; 76: 60–4.
Kurz A, Sessler DI, Lenhardt R Perioperative nor-mothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. N Engl J Med 1996; 334: 1209–15.
Frank SM, Fleisher LA, Breslow MJ, et al. Perioperative maintenance of normothermia reduces the incidence of morbid cardiac events. A randomized clinical trial. JAMA 1997; 277: 1127–34.
Ikeda T, Sessler DI, Marder D, Xiong J. Influence of thermoregulatory vasomotion and ambient temperature variation on the accuracy of core-temperature estimates by cutaneous liquid-crystal thermometers. Anesthesiology 1997; 86: 603–12.
Sessler DI. A Proposal for new temperature monitoring and thermal management guidelines (Letter). Anesthesiology 1998; 89: 1298–300.
Fox RH, Solman AJ. A new technique for monitoring the deep body temperature in man from the intact skin surface. J Physiol (Lond) 1970; 212: 8–10.
Togawa T, Nemoto T, Yamazaki T, Kobayashi T. A modified internal temperature measurement device. Med Biol Eng 1976; 14: 361–4.
Matsukawa T, Kashimoto S, Ozaki M, Shindo S, Kumazawa T. Temperatures measured by a deep body thermometer (Coretemp®) compared with tissue temperatures measured at various depths using needles placed into the sole of the foot. Eur J Anaesthesiol 1996; 13: 340–5.
Matsukawa T, Sessler DI, Ozaki M, Hanagata K, Iwashita H, Kumazawa T. Comparison of distal oesophageal temperature with “deep” and tracheal temperatures. Can J Anaesth 1997; 44: 433–8.
Matsukawa T, Ozaki M, Sessler DI, Nishiyama T, Imamura M, Kumazawa T. Accuracy and precision of “deep sternal” and tracheal temperatures at high- and low-fresh-gas flows. Br J Anaesth 1998; 81: 171–5.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–10.
Harioka T, Sone T, Nomura K, Kakuyama M Relative accuracy and precision of two non-invasive thermometry systems. Masui 1993; 42: 856–61.
Sessler DI. Temperature monitoring and management during neuraxial anesthesia (Editorial). Anesth Analg 1999; 88: 243–5.
Dorsch JA, Dorsch SE. Temperature monitoring.In: Understanding Anesthesia Equipment, 4th ed. Baltimore: Williams & Wilkins, 1999; 879–93.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Harioka, T., Matsukawa, T., Ozaki, M. et al. “Deep-forehead” temperature correlates well with blood temperature. Can J Anesth 47, 980–983 (2000). https://doi.org/10.1007/BF03024869
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03024869