
Abstract
Purpose
Despite the well-documented impairment of pulmonary function after cardiopulmonary bypass, effective precautions and ideal management strategies for this problem are still under debate. This study aimed to evaluate the effects of continuous positive airway pressure (CPAP) applied during cardiopulmonary bypass on respiratory and hemodynamic variables.
Methods
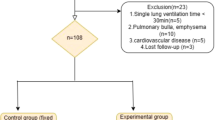
In this randomized, prospective, controlled trial, 120 male patients, aged 45 to 70 yr undergoing first-time elective bypass surgery, were randomly assigned to receive either 10 cm H2O of CPAP (Group I; n = 60) during cardiopulmonary bypass, or serve as control (Group II; n = 60), where the patient’s lungs were vented to atmosphere during the bypass period.
Results
Alveolar-arterial oxygen partial pressure difference and shunt fraction were significantly higher in the control group compared with the CPAP group after cardiopulmonary bypass (T2) and after closure of sternum (T3), (P < 0.05). No differences between groups with respect to hemodynamic variables were observed at any time. Postoperative pulmonary function variables were lower in both groups compared to baseline values.
Conclusions
Continuous positive airway pressure administered during cardiopulmonary bypass decreased shunt fraction and alveolar-arterial oxygen partial pressure difference during surgery, but had no sustained effect on either variable postoperatively. We conclude that, in patients with normal preoperative pulmonary function, application of 10 cm H2O CPAP does not improve lung function after cardiac surgery.
Résumé
Objectif
Malgré les connaissances acquises sur l’atteinte de la fonction pulmonaire après la circulation extracorporelle, les précautions efficaces et le traitement idéal touchant ce problème font toujours l’objet de débats. Nous voulions évaluer les effets d’une ventilation en pression positive continue (CPAP pour «continuous positive airway pressure») pendant la circulation extracorporelle sur les variables respiratoires et hémodynamiques.
Méthode
Dans notre étude randomisée, prospective et contrôlée, 120 hommes de 45 à 70 ans devant subir un premier pontage électif, ont reçu soit 10 cm H2O de CPAP (Groupe I; n = 60) pendant la circulation extracorporelle, soit ont servi de témoins (Groupe II; n = 60) et les poumons ont été ventilés à la pression atmosphérique pendant le pontage.
Résultats
La différence alvéolaire-artérielle de pression partielle en oxygène et la fraction de shunt ont été significativement plus élevées chez les témoins que chez les patients sous CPAP après la circulation extracorporelle (T2) et après la fermeture du sternum (T3), (P < 0,05). Les variables hémodynamiques ont toujours été similaires dans les deux groupes. Dans les deux groupes aussi, les variables de la fonction pulmonaire postopératoire étaient plus basses que les valeurs de départ.
Conclusion
La ventilation à pression positive continue pendant la circulation extracorporelle a réduit la fraction de shunt et la différence alvéolaire-artérielle de pression partielle en oxygène pendant l’opération, mais n’a pas eu d’effet postopératoire prolongé sur chacune des variables. Donc, chez les patients dont la fonction pulmonaire préopératoire est normale, une CPAP de 10 cm H2O n’améliore pas la fonction pulmonaire après la cardiochirurgie.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Fowler AA, Hamman RF, Good JT, et al. Adult respiratory distress syndrome: risk with common predispositions. Ann Intern Med 1983; 98: 593–7.
Andrejaitiene J, Sirvinkas E, Bolys R. The influence of cardiopulmonary bypass on respiratory dysfunction in early postoperative epriod. Medicina 2004; 40(Suppl 1): 7–12.
Boldt J, King D, Scheld HH, Hempellmann G. Lung management during cardiopulmonary bypass: influence on extravascular lung water. J Cardiothorac Anesth 1990; 4: 73–9.
Berry CB, Butler PJ, Myles PS. Lung management during cardiopulmonary bypass: is continuous positive airways pressure beneficial? Br J Anaesth 1993; 71: 864–8.
Loeckinger A, Kleinasser A, Lindner KH, Margreiter J, Keller C, Hoermann C. Continuous positive airway pressure at 10 cm H20 during cardiopulmonary bypass improves postoperative gas exchange. Anesth Analg 2000; 91: 522–7.
Brasil LA, Gomes WJ, Salamao R, Buffolo E. Inflammatory response after myocardial revascularization with or without cardiopulmonary bypass. Ann Thorac Surg 1998; 66: 56–9.
Anyanwu E, Dittrich H, Giesenking R, Enders HJ. Ultrastructural changes in the human lung following cardiopulmonary bypass. Basic Res Cardiol 1982; 77: 309–22.
Parker DJ. Some changes in the lungs associated with cardiopulmonary bypass,In:Junod F (Ed.). Lung Metabolism. San Diego, CA: Academic; 1974: 459–79.
Menasche P, Edmunds LH Jr. The inflammatory response.In: Cohn LH, Edmunds LH (Eds). Cardiac Surgery in the Adult, 2nd ed. McGraw Hill; 2003: 349–60.
Hewson JR, Shaw M. Continuous airway pressure with oxygen minimizes the metabolic lesion of pump-lung. Can Anaesth Soc J 1983; 30: 37–47.
Pavelkova M, Kubala L, Ciz M, et al. Blood phagocyte activation during open heart surgery with cardiopulmonary bypass. Physiol Res 2005; 24 (Epub ahead of print).
Ishikawa S, Ohtaki A, Takahashi T, et al. PEEP therapy for patients with pleurotomy during coronary artery bypass grafting. J Card Surg 2000; 15: 175–8.
Magnusson L, Zemgulis V, Tenling A, et al. Use of vital capacity maneuver to prevent atelectasis after cardiopulmonary bypass: an experimental study. Anesthesiology 1998; 88: 134–42.
Magnusson L, Zemgulis V, Wicky S, Tyden H, Hedenstierna G. Effect of CPAP during cardiopulmonary bypass on postoperative lung function. An experimental study. Acta Anaesthesiol Scand 1998; 42: 1133–8.
Stanley TH, Liu WS, Gentry S. Effects of ventilatory techniques during cardiopulmonary bypass on postbypass and postoperative pulmonary compliance and shunt. Anesthesiology 1977; 46: 391–5.
Magnusson L, Zemgulis V, Wicky S, Tyden H, Thelin S, Hedenstierna G. Atelectasis is a major cause of hypoxemia and shunt after cardiopulmonary bypass. An experimental study. Anesthesiology 1996; 87: 1153–63.
Lindberg H, Svennevig JL, Lilleaasen P, Vatne K. Pulsatile vs. non-pulsatile flow during cardiopulmonary bypass. A comparison of early postoperative changes. Scand J Thorac Cardiovasc Surg 1984; 18: 195–201.
Taggart DP, El Fiky M, Carter R, Bowman A, Wheatley DJ. Respiratory dysfunction after uncomplicated cardiopulmonary bypass. Ann Thorac Surg 1993; 56: 1123–8.
Westerdahl E, Lindmark B, Eriksson T, Friberg Ö, Hedenstierna G, Tenling A. Deep-breathing exercises reduce atelectasis and improve pulmonary function after coronary artery bypass surgery. Chest 2005; 128: 3482–8.
Vargas F, Cukier A, Terra-Filho M, Hueb W, Teixeira LR, Light RW. Relationship between pleural changes after myocardial revascularization and pulmonary mechanics. Chest 1992; 102: 1333–6.
Shapira N, Zabatino SM, Ahmed S, Murphy DM, Sullivan D, Lemole GM. Determinants of pulmonary function in patients undergoing coronary bypass operations. Ann Thorac Surg 1990; 50: 268–73.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests: None declared.
Rights and permissions
About this article
Cite this article
Altmay, E., Karaca, P., Yurtseven, N. et al. Continuous positive airway pressure does not improve lung function after cardiac surgery. Can J Anesth 53, 919–925 (2006). https://doi.org/10.1007/BF03022835
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03022835